Is Your Fat Aging Faster Than You? How Adipose Tissue Controls Lifespan and Disease
Adipose tissue isn’t just fat—it may control how fast you age. Explore biomarkers, inflammation, and proven strategies for healthier aging.
AGINGMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/2/202612 min read
Adipose tissue aging refers to the progressive decline in fat tissue function, characterised by increased inflammation, accumulation of senescent cells, impaired mitochondrial function, and disrupted hormone signalling (Wang et al., 2025). As fat ages, it releases harmful molecules through the senescence-associated secretory phenotype (SASP), contributing to insulin resistance, cardiovascular disease, frailty, and systemic aging (Liu et al., 2025).
Emerging research in geroscience suggests adipose tissue may act as a “pace-maker” of biological aging by dictating metabolic health, immune function, and organ performance (Liu et al., 2025). Key biomarkers such as ELN, MXD1, FGF21, and recently HDAC9 are being studied to measure fat tissue aging and guide future therapies (Xie et al., 2025; Goo et al., 2026).
In simple terms: healthy fat supports longevity, while dysfunctional fat accelerates aging and disease risk.
Clinician’s Perspective: Adipose Tissue as a Central Metabolic Organ
Adipose tissue is a central metabolic organ—not a passive depot
Modern evidence firmly establishes adipose tissue as an endocrine and immunologically active organ regulating systemic metabolism, inflammation, and energy homeostasis (Corvera et al., 2026). Its dysfunction is a primary driver, not merely a consequence, of cardiometabolic disease (Wang et al., 2025).
Adipose aging is clinically visible long before disease onset
Subtle shifts—central fat redistribution, rising triglycerides, declining insulin sensitivity—often precede overt diagnoses by years (Wang et al., 2025). These changes reflect early adipose dysfunction and should be treated as actionable warning signals rather than benign age-related changes.
Visceral fat is the most clinically relevant compartment
Expansion of visceral adipose tissue correlates strongly with insulin resistance, hepatic steatosis, and systemic inflammation (Wang et al., 2025). Waist-to-height ratio >0.5 and imaging-based fat quantification provide more meaningful risk assessment than BMI alone.
Chronic low-grade inflammation (“inflammaging”) is adipose-driven
Aging fat becomes enriched with senescent cells exhibiting the SASP, releasing IL-6, TNF-α, and MCP-1 that amplify metabolic and vascular risk (Liu et al., 2025). New data from 2026 show that white adipose atrophy during aging also exacerbates cold intolerance and accelerates systemic decline, indicating that both excess and loss of fat function are harmful (Liu et al., 2026).
Biomarkers are transitioning from research to clinical relevance
Emerging markers such as FGF21, adiponectin-to-leptin ratio, and now HDAC9 expression offer early insight into adipose health (Xie et al., 2025; Goo et al., 2026). While not yet routine, they are likely to become part of precision metabolic care (Aging Biomarker Consortium et al., 2025).
Therapeutic focus should shift from weight loss to fat quality
The goal is not simply to reduce fat mass but to improve adipose function—enhancing insulin sensitivity, reducing inflammation, preserving mitochondrial flexibility, and restoring beige/brown fat activity (Luo et al., 2026).
Exercise remains the most potent intervention
Combined aerobic and resistance training improves adipokine signaling, promotes mitochondrial biogenesis via PGC-1α, reduces senescent cell burden, and may partially reverse adverse adipose remodeling (Luo et al., 2026; Goo et al., 2026).
Metabolic health must be managed proactively and longitudinally
Early control of glucose, lipids, and blood pressure slows adipose aging and reduces downstream organ damage (Wang et al., 2025).
Future therapies are promising, but adjunctive
Targets such as FGF21 analogues, senolytics, and HDAC9 inhibitors may complement—but not replace—lifestyle interventions (Xie et al., 2025; Goo et al., 2026).
Clinical takeaway
Healthy aging is not defined by the absence of fat, but by functionally resilient adipose tissue—a modifiable determinant of long-term metabolic and systemic health (Wang et al., 2025).
Why Your Fat Tissue Deserves More Respect
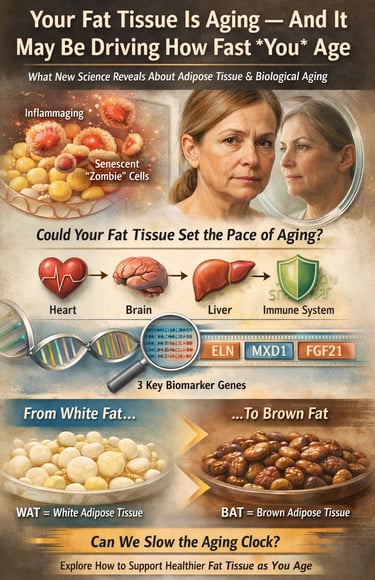
What if the pace at which you age is not primarily determined by your heart, your brain, or even your DNA—but by your fat?
For decades, adipose tissue was dismissed as little more than passive energy storage. Today, that view has been decisively overturned. A growing body of research in geroscience and metabolic medicine now positions adipose tissue as a central regulator of systemic aging—an active endocrine organ capable of influencing inflammation, insulin sensitivity, immune function, and even brain health (Wang et al., 2025; Liu et al., 2025; Corvera et al., 2026).
As fat tissue ages, it becomes more inflamed, less metabolically flexible, increasingly fibrotic, and populated by senescent “zombie” cells that secrete harmful signaling molecules (Wang et al., 2025). These signals circulate throughout the body, subtly reshaping the biological environment in which every organ operates.
This has led to a provocative hypothesis: adipose tissue may act as a “pace-maker” of biological aging, influencing how quickly—or slowly—multiple organ systems decline (Liu et al., 2025). Advances in bioinformatics have identified measurable signatures of this process. Recent work highlights ELN, MXD1, FGF21 and HDAC9 as key genes that track the aging trajectory of fat tissue with remarkable precision (Xie et al., 2025; Goo et al., 2026).
A 2026 Nature Communications study showed that age-related white adipose atrophy impairs thermogenesis and stress resilience, accelerating aging in male mice (Liu et al., 2026). This suggests preserving healthy adipose mass and function—not just preventing obesity—is critical for longevity.
Understanding this hidden biology may be one of the most important steps toward slowing the aging process itself.
What Is Adipose Tissue, and Why Does It Age Differently?
Adipose tissue comes in several forms. White adipose tissue (WAT) stores energy. Brown adipose tissue (BAT) burns energy to generate heat via UCP1-dependent thermogenesis. Beige adipose tissue can shift between the two (Villarreal & Baranova, 2026).
A landmark review in Nature Reviews Endocrinology described how adipose tissue undergoes striking structural and functional changes as we age (Wang et al., 2025). These include:
1. Redistribution of fat from subcutaneous to visceral depots
2. Decline in brown and beige fat activity
3. Increase in chronic low-grade inflammation—“inflammaging” (Liu et al., 2025)
4. Reduced regenerative capacity of fat-resident stem cells
5. Impaired secretion of beneficial hormones, including adiponectin and leptin
6. Mitochondrial dysfunction and loss of metabolic flexibility (Goo et al., 2026)
New comparative anatomy data show human BAT is more dispersed and less UCP1-dense than rodent BAT, but retains significant metabolic potential through UCP1-independent pathways like creatine and calcium cycling (Villarreal & Baranova, 2026). This may explain why some adults retain “metabolically healthy” aging despite low classical BAT mass.
Because adipose tissue is a major endocrine organ, its aging disrupts metabolic regulation body-wide. The consequence is a cascade that raises risk for type 2 diabetes, cardiovascular disease, neurodegenerative conditions, and some cancers (Wang et al., 2025; Ou et al., 2022).
A comprehensive review spanning 2,527 documents found that interest in adipose tissue browning and aging has accelerated since 2015, with bioinformatics now enabling researchers to map the aging process within fat tissue at unprecedented detail (Luo et al., 2026).
What Are Aging Biomarkers, and Why Do We Need Them?
A biomarker is a measurable biological signal that reliably indicates a particular biological state. In aging, biomarkers help answer: How old is this tissue, really?
Your chronological age tells only part of the story. Your biological age can diverge significantly based on genetics, lifestyle, and metabolic health.
Identifying reliable adipose tissue aging biomarkers is crucial for early detection, therapeutic targeting, and tracking interventions (Aging Biomarker Consortium et al., 2025). The Consortium’s 2025 framework established agreed standards for what counts as a valid adipose aging biomarker, enabling more consistent research globally.
The Four Breakthrough Biomarker Genes: ELN, MXD1, FGF21, and HDAC9
A 2025 study in Frontiers in Endocrinology used integrative bioinformatics and machine learning to identify genes most consistently associated with adipose tissue aging (Xie et al., 2025). Three stood out: ELN, MXD1, and FGF21. New 2026 research adds HDAC9 to this list (Goo et al., 2026).
ELN (Elastin)
Elastin maintains the extracellular matrix of fat depots. As adipose tissue ages, reduced ELN expression causes stiffening and fibrosis (Xie et al., 2025). This limits healthy adipocyte expansion, triggering cellular stress and early senescence. Elastin fragments also act as pro-inflammatory “matrikines.”
MXD1 (MAX Dimerization Protein 1)
MXD1 balances cell turnover versus senescence. Dysregulation in aging fat shifts toward increased senescent cell accumulation and SASP (Xie et al., 2025). Targeting MXD1 could slow “zombie cell” buildup.
FGF21 (Fibroblast Growth Factor 21)
FGF21 improves insulin sensitivity and promotes fat oxidation. But chronic elevation signals “FGF21 resistance”—a marker of metabolic stress (Xie et al., 2025). FGF21 analogues are now in Phase 3 trials for NASH and obesity.
HDAC9 (Histone Deacetylase 9)
A 2026 Aging Cell study found HDAC9 gene deletion in mice ameliorates aging-related adipose senescence and restores mitochondrial function (Goo et al., 2026). HDAC9 appears to repress PGC-1α and mitochondrial biogenesis. Inhibiting HDAC9 may be a future strategy to rejuvenate aged fat.
How Does Adipose Tissue "Talk" to the Rest of Your Body?
Aging fat shifts from a “youthful secretome” to an “aged secretome” (Wang et al., 2025). Adiponectin falls. Leptin resistance rises. SASP factors increase.
The adipose-brain axis is bidirectional. Aged adipose tissue impairs hypothalamic function via inflammatory exosomes, while hypothalamic aging accelerates white adipose atrophy (Liu et al., 2025; Liu et al., 2026). This creates a vicious cycle linking metabolic and cognitive decline.
Transplanting young adipose tissue into aged animals improves metabolism and lifespan, proving fat health is causal, not correlative (Wang et al., 2025).
The Browning Connection: A Metabolic Lifeline Against Aging
Browning capacity declines with age but is not lost (Luo et al., 2026).
New mechanisms (2025-2026):
1. UCP1-independent thermogenesis via creatine futile cycling and SERCA2b calcium cycling can compensate for lost BAT (Villarreal & Baranova, 2026).
2. Cold exposure, exercise, and polyphenols like resveratrol and EGCG activate these pathways (Luo et al., 2026).
3. HDAC9 inhibition promotes beige adipocyte formation (Goo et al., 2026).
This plasticity means adipose aging is partially reversible.
Practical Applications: What You Can Do Right Now
1. Prioritize Exercise: Aerobic + resistance training reduces senescent cell burden, lowers HDAC9, and increases FGF21 sensitivity (Goo et al., 2026; Luo et al., 2026). Aim for 150 min of moderate aerobic + 2 strength sessions weekly.
2. Manage Inflammation Through Diet: The Mediterranean diet reduces SASP and improves ELN expression (Wang et al., 2025). Add omega-3s, polyphenols, and fermented foods.
3. Protect Sleep: Sleep loss raises cortisol, increases visceral fat, and induces FGF21 resistance. 7–9 hours nightly is metabolic medicine.
4. Avoid Prolonged Sitting: Break sedentary time every 60 min. Inactivity specifically atrophies gluteofemoral fat, worsening metabolic risk (Liu et al., 2026).
5. Cold Exposure: 2-3x weekly cold showers or 15 min at 14-17°C can activate beige fat and UCP1-independent thermogenesis (Luo et al., 2026).
6. Monitor Waist-to-Height Ratio: Keep <0.5. This outperforms BMI for tracking visceral adipose aging (Wang et al., 2025).
7. Stay Updated on Therapeutics: FGF21 analogues, senolytics, and HDAC9 inhibitors are in trials (Xie et al., 2025; Goo et al., 2026).
Frequently Asked Questions (FAQs)
Q1: What exactly does "adipose tissue aging" mean in practical terms?
It refers to functional changes in fat cells—shifts toward visceral depots, increased inflammation, reduced metabolic flexibility, and altered hormone secretion (Wang et al., 2025). These changes contribute to metabolic disease risk and accelerated systemic aging.
Q2: Can I measure my adipose tissue's biological age?
Not yet at the consumer level. The Aging Biomarker Consortium's 2025 framework is establishing the foundation for validated clinical tools (Aging Biomarker Consortium et al., 2025). Blood-based markers like FGF21 levels and adiponectin-to-leptin ratios offer partial windows into adipose health (Xie et al., 2025).
Q3: Are ELN, MXD1, FGF21, and HDAC9 the only important biomarkers?
No—they are among the most robust candidates identified using machine-learning methods (Xie et al., 2025; Goo et al., 2026). Dozens of candidate biomarkers exist, but these show strong convergence across analytical approaches.
Q4: Does losing weight improve adipose tissue aging?
Reduction of visceral fat generally improves adipose function, reduces inflammatory markers, and shifts adipokine profiles favorably (Wang et al., 2025). However, quality matters: rapid extreme restriction can impair adipose health. Gradual fat loss through lifestyle is preferred.
Q5: Is adipose tissue aging reversible?
Partially, yes. Research into browning, senescence clearance, and metabolic reprogramming suggests meaningful reversibility (Luo et al., 2026; Corvera et al., 2026; Goo et al., 2026). Exercise, diet, and emerging drugs can shift fat toward a more youthful state.
Q6: How does adipose tissue aging relate to Alzheimer's disease?
Adipokines and inflammatory signals from aged fat cross the blood-brain barrier and influence neuroinflammation and amyloid metabolism (Liu et al., 2025). Maintaining adipose health is a modifiable factor in neurodegenerative risk.
Q7: Should I be concerned about having too little body fat as I age?
Yes. Both excess and insufficient body fat are associated with accelerated adipose aging (Liu et al., 2026). Subcutaneous fat, especially gluteofemoral, has protective metabolic properties. Age-related lipoatrophy drives ectopic lipid deposition and worsens insulin sensitivity.
Q8: What is white adipose atrophy and why does it matter?
New 2026 research shows that losing white fat with age impairs cold tolerance, increases stress hormones, and accelerates aging (Liu et al., 2026). Healthy aging requires preserving functional fat, not eliminating it.
Q9: What does HDAC9 do in fat aging?
HDAC9 suppresses mitochondrial genes. Mice lacking HDAC9 have less adipose senescence and better metabolic health (Goo et al., 2026). Drugs targeting HDAC9 are in preclinical development.
Q10: Can I activate brown fat if I’m older?
Yes. While classical BAT declines, UCP1-independent beige fat pathways remain responsive to exercise, cold, and nutrition into older age (Villarreal & Baranova, 2026; Luo et al., 2026).
Clinical Pearls: The Aging Adipose Organ
1. The "Adipose-Brain Axis" Connection
Aging adipose tissue undergoes a "secretome shift," increasing systemic release of pro-inflammatory cytokines (SASP) that can breach the blood-brain barrier (Liu et al., 2025). This contributes to neuroinflammation and may accelerate neurodegenerative pathologies.
2. The Lipoatrophy Paradox
Age-related subcutaneous lipoatrophy—particularly in the gluteofemoral region—leads to ectopic lipid deposition in liver and muscle, significantly worsening insulin resistance (Liu et al., 2026). Not all fat is bad; losing protective subcutaneous fat can be risky.
3. Structural Integrity and the ELN Biomarker
Downregulation of ELN leads to fibrosis and stiffening of the extracellular matrix within fat depots (Xie et al., 2025). This mechanical rigidity limits healthy expansion of adipocytes, triggering cellular stress and early senescence.
4. Therapeutic Potential of Adipose "Browning"
Interventions such as cold thermogenesis and aerobic exercise can induce "browning" of WAT, enhancing mitochondrial biogenesis and increasing systemic metabolic rate via UCP1-mediated and UCP1-independent thermogenesis (Luo et al., 2026; Villarreal & Baranova, 2026).
5. FGF21: The Metabolic Stress Signal
While FGF21 is a potent insulin sensitizer, chronic elevation in aging often indicates "FGF21 resistance" (Xie et al., 2025). Monitoring this biomarker can serve as an early warning system for metabolic dysfunction.
6. The Atrophy Paradox
While visceral excess is harmful, age-related subcutaneous white adipose atrophy drives ectopic lipid deposition and cold intolerance (Liu et al., 2026). Preserving gluteofemoral fat mass is metabolically protective.
7. HDAC9 as a Master Regulator
HDAC9 links epigenetic aging to mitochondrial dysfunction in adipocytes (Goo et al., 2026). Its inhibition restores PGC-1α and reduces SASP.
Take the Next Step: From Reading to Action
✅ Right Now (Today)
Share this article with a friend, family member, or healthcare provider who cares about healthy aging. Write down one lifestyle habit from the Practical Applications section you will commit to this week.
✅ This Week
Speak with your doctor about visceral fat levels—a DEXA scan or waist-to-height ratio can offer a useful starting point. Ask whether an FGF21 blood test is appropriate for your health context.
✅ This Month
Start or upgrade an exercise routine that includes both aerobic and resistance components. Begin a 4-week Mediterranean diet trial and track energy, sleep quality, and waist measurement.
Author’s Note
This article bridges rapidly evolving molecular science and real-world clinical understanding. The biology of adipose tissue has advanced from a “energy storage” model to a systems-level view of fat as a dynamic regulator of aging (Wang et al., 2025; Corvera et al., 2026). Findings around ELN, MXD1, FGF21, and HDAC9 are promising but represent a developing field (Xie et al., 2025; Goo et al., 2026). For clinicians, the goal is earlier recognition of adipose dysfunction. For readers, the aim is to reframe fat not as an adversary, but as a biologically active partner in health.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Aging Biomarker Consortium, Yu, J., Zhang, Y., et al. (2025). A framework of biomarkers for adipose tissue aging: a consensus statement by the Aging Biomarker Consortium. Life Medicine, 4(5), lnaf027. https://doi.org/10.1093/lifemedi/lnaf027
Corvera, S., Rajan, A., Townsend, K. L., et al. (2026). Advances in adipose tissue biology. Endocrine Reviews, 47(1), 75–92. https://doi.org/10.1210/endrev/bnaf032
Goo, B., Ahmadieh, S., Veerapaneni, P., et al. (2026). Histone Deacetylase 9 Gene Deletion Ameliorates Aging-Related Adipose Tissue Senescence and Mitochondrial Dysfunction in Mice. Aging Cell, 25(5), e70519. https://doi.org/10.1111/acel.70519
Liu, J., Huang, Q., & Liu, F. (2025). Fat talks first: how adipose tissue sets the pace of aging? Life Medicine, 4(5), lnaf028. https://doi.org/10.1093/lifemedi/lnaf028
Liu, Z., Hu, W., Tan, X., et al. (2026). White adipose atrophy exacerbates cold stress and accelerates aging in male mice. Nat Commun, 17, 1821542. https://doi.org/10.1038/s41467-026-71857-3
Luo, Y., Song, Y., Zeng, M., et al. (2026). The past, present, and future of adipose tissue browning and aging: A review combined with bibliometrics and bioinformatics of 2527 documents published over the past four decades. Ageing Research Reviews, 114, 102959. https://doi.org/10.1016/j.arr.2025.102959
Ou, MY., Zhang, H., Tan, PC., et al. (2022). Adipose tissue aging: mechanisms and therapeutic implications. Cell Death Dis, 13, 300. https://doi.org/10.1038/s41419-022-04752-6
Villarreal J & Baranova A. (2026). Comparative anatomy and metabolic profiles of brown and white adipose tissue in humans. Front. Endocrinol, 17, 1821542. doi: 10.3389/fendo.2026.1821542
Wang, G., Song, A., & Wang, Q. A. (2025). Adipose tissue ageing: implications for metabolic health and lifespan. Nature Reviews Endocrinology, 21, 623–637. https://doi.org/10.1038/s41574-025-01142-8
Xie, X., Wang, H., Xiao, F., et al. (2025). Identifying aging-related biomarkers in adipose tissue using integrative bioinformatics and machine-learning approaches: discovery of ELN, MXD1, and FGF21 as key genes. Frontiers in Endocrinology, 16, 1638343. https://doi.org/10.3389/fendo.2025.1638343