GLP-1s and Muscle Loss: What’s Normal, What’s Not, and How to Protect Lean Mass
GLP-1 drugs like semaglutide can lead to some lean mass loss during weight reduction. Learn what’s physiologically expected, what raises concern for true muscle loss, and evidence-based strategies to preserve skeletal muscle during therapy.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/21/202623 min read
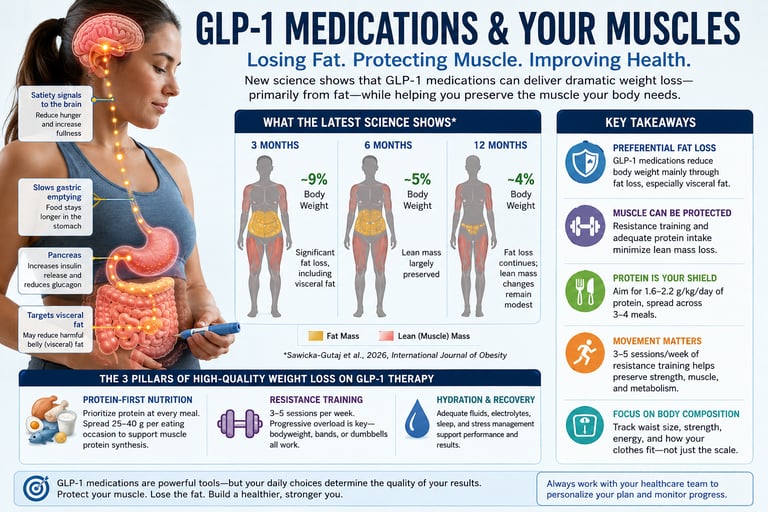
GLP-1 medications such as semaglutide and tirzepatide cause a measurable reduction in lean mass during weight loss, but most evidence suggests fat loss exceeds lean mass loss. Current studies show preserved muscle strength in most patients, particularly when resistance training and adequate protein intake are maintained.
GLP-1 Medications and Muscle Loss: Key Takeaways
While GLP-1 medications like semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) cause lean mass reduction, it is a natural byproduct of rapid weight loss, not a drug-specific side effect. Clinical trials show that body composition shifts on GLP-1s closely mirror those of traditional caloric restriction and bariatric surgery.
Fat Loss Dominates the Scale: In major clinical trials, fat mass accounts for 60% to 75% of total weight lost. The vast majority of weight dropped is adipose tissue, not skeletal muscle.
Lean Mass Loss is Standard, Not Catastrophic: A total weight loss of 10–15 kg typically includes 3–5 kg of lean mass (which includes water, connective tissue, and muscle). This ratio is identical to traditional dieting; GLP-1s do not uniquely "eat" muscle.
Physical Strength Holds Steady: Multiple mobility studies demonstrate that metrics like grip strength and real-world physical performance remain stable or improve, as improved muscle quality and reduced joint load compensate for minor size reductions.
Resistance Training is Non-Negotiable: Engaging in progressive resistance training 2 to 3 times per week acts as a powerful stimulus to preserve skeletal muscle and maximize metabolic rate during active weight loss.
Protein Intake Sets the Retention Floor: Patients should target 1.6 to 2.2 grams of protein per kilogram of ideal body weight daily. Because GLP-1s induce severe appetite suppression, intentional protein pacing via lean meats and shakes is a clinical priority.
Baseline Demographics Dictate Risk: Adults over the age of 60, sarcopenic patients, and individuals starting with low baseline muscle mass face the highest functional risks and require immediate, proactive strength and nutritional interventions.
Tirzepatide vs. Semaglutide Patterns: Dual GIP/GLP-1 receptor agonists (tirzepatide) induce greater absolute weight loss than GLP-1-only agents (semaglutide). This results in higher absolute lean mass loss, but the favorable fat-to-lean loss ratio remains virtually identical.
Real-World Function Matters Most: Medicine is shifting focus from DXA scan metrics to functional outcomes. The ultimate measure of success is maintaining daily vitality—such as climbing stairs, carrying groceries, and preserving long-term mobility.
The Clinical Verdict: GLP-1 medications are powerful tools for profound weight loss. While some lean mass loss is inevitable, pairing the medication with structured resistance training and high protein intake ensures that the weight lost is overwhelmingly body fat.
Introduction
If you've started a GLP-1 receptor agonist like semaglutide (Wegovy, Ozempic), liraglutide (Saxenda), or tirzepatide (Zepbound, Mounjaro) — or you're thinking about it — you've probably seen the headlines: these drugs melt away muscle along with fat.
It's a real concern, and it deserves a real answer instead of a scary headline or a dismissive one.
So here's what this article does differently: instead of citing "studies show," we pulled the actual numbers from the most clinically relevant evidence on GLP-1 and muscle loss published through mid-2026 — including a brand-new dose-specific meta-analysis of seven randomized trials (821 patients) and a separate systematic review focused on people with fatty liver disease. We'll walk through the exact effect sizes, what they mean in practice, where the data is strong, and where it's genuinely shaky.
By the end, you'll know:
How much lean mass GLP-1 drugs actually cause you to lose, in real kilograms
Why "lean mass" is not the same thing as "muscle," and why that distinction matters enormously
Which drug (semaglutide, liraglutide, or tirzepatide) has the largest effect, and why
Whether losing muscle on these drugs is dangerous, or just a normal — even favorable — part of weight loss
A practical, evidence-aligned protocol to protect your muscle while losing fat
1. The Short Answer
Yes, GLP-1 receptor agonists at obesity-treatment doses cause a measurable, statistically significant loss of absolute lean mass. The best current dose-specific evidence — a 2026 meta-analysis of seven RCTs in 821 patients — puts the average loss at −1.74 kg (95% CI: −3.04 to −0.45 kg) compared with placebo.
But here's the part that headlines tend to skip: the proportion of your body that is lean mass actually goes up during treatment, by an average of 1.81 percentage points (95% CI: 1.1–2.52). That's because fat loss outpaces muscle loss by a wide margin. You're losing some muscle in absolute terms, but your overall body composition is shifting toward a healthier ratio.
The researchers who ran this analysis put it plainly in their own conclusion: lean mass loss "should not be considered a limitation" to using these drugs for obesity — provided it's paired with resistance training and adequate protein intake.
2. What "Lean Mass" Actually Measures (and Why It's Not "Muscle")
This is the single most important distinction in this entire topic, and it's the one most consumer health articles get wrong.
Lean mass (also called fat-free mass) is not the same as skeletal muscle. It includes:
Skeletal muscle (the tissue you build with resistance training)
Internal organs, including the liver
Bone
Body water and fluid
Connective tissue
Most of the studies on GLP-1 drugs and "muscle loss" actually measured lean mass using DXA scans (dual-energy X-ray absorptiometry) or bioelectrical impedance — neither of which can isolate skeletal muscle from everything else in that category.
This matters more than it sounds like. If you have obesity, your liver is often enlarged with excess fat and glycogen — a hallmark of metabolic dysfunction-associated steatotic liver disease (MASLD), which affects a large share of people who qualify for GLP-1 therapy. When a GLP-1 drug reduces liver fat and shrinks the organ back toward a normal size, that entire reduction gets counted as "lean mass loss" on a DXA scan — even though no muscle tissue was lost at all.
A small but illuminating 2026 animal study illustrates the scale of this effect: in mice treated with a GLP-1 agonist, liver mass change accounted for roughly 71% of the early body-weight-change signal, while muscle mass in the untreated leg accounted for only about 9%. The liver was doing the great majority of the apparent "lean mass" shrinking.
The implication: a meaningful share of what gets reported as "muscle loss" in body-composition studies is very likely organ shrinkage, fluid shifts, and fat-mass reclassification — not the loss of contractile, force-generating muscle tissue.
This is exactly why the gold-standard outcome to track isn't lean mass on a scan. It's muscle strength and function — and as you'll see below, that's where the picture looks considerably more reassuring.
3. The Core Evidence: A Dose-Specific Meta-Analysis of 821 Patients
Most of the meta-analyses published before 2026 had a significant blind spot: they pooled data from people taking GLP-1 drugs at the lower doses used for diabetes, not the higher doses actually prescribed for obesity. Since these drugs work in a dose-dependent way, that likely understated the real effect on muscle.
A 2026 systematic review and meta-analysis published in the International Journal of Obesity (Laverde et al.) closed that gap. The researchers searched PubMed, Embase, and LILACS through March 2025 and included only randomized, placebo-controlled trials using doses specifically approved for obesity treatment: liraglutide 3 mg/day, semaglutide 2.4 mg/week, and tirzepatide 5–15 mg/week. Seven trials met that bar, covering 821 adults with obesity.
Here's exactly what they found, outcome by outcome.
Lean mass as a proportion of total body weight (the body-composition signal)
Combined effect: +1.81% (95% CI: 1.1–2.52; p < 0.00001)
Heterogeneity between studies was low (I² = 7%), meaning this result was highly consistent across trials
The certainty of evidence for this outcome was rated high using the GRADE framework
In plain terms: as a percentage of your total body weight, you end up with more lean tissue after treatment, not less — because fat mass drops faster than lean mass does.
Absolute lean mass lost, in kilograms (the number everyone actually wants)
Combined effect: −1.74 kg (95% CI: −3.04 to −0.45 kg; p < 0.00001)
Heterogeneity was very high (I² = 98%), meaning the result varied enormously depending on which drug and which follow-up duration you're looking at — this is a critical caveat, explained in the next section
Certainty of evidence: high
Percentage change in lean mass from baseline
Combined effect: −3.06% (95% CI: −5.10 to −1.02%; p < 0.00001)
Again, very high heterogeneity (I² = 98%), driven mainly by which medication was used
The authors' own interpretation is worth quoting carefully because it's more nuanced than a headline number suggests: even though the statistically significant changes in lean mass proportion were real, the authors note this "may not be clinically significant" — and could instead be read as "no net deterioration" in overall body composition.
That's an important admission from the researchers themselves. Statistical significance (a real, non-random effect) and clinical significance (an effect large enough to matter for your health or function) are two different things, and this study explicitly says the former doesn't guarantee the latter here.
4. Semaglutide vs. Liraglutide vs. Tirzepatide: Head-to-Head Numbers
This is where the high heterogeneity (I² = 98%) mentioned above actually resolves into something useful: the "combined" number above is an average across three very different drugs. Breaking it apart by medication tells a much clearer story.
Liraglutide (3 mg/day)
Short-Term Use (<52 weeks):
Absolute Lean Mass: Decreased by 0.41 kg (95% CI: −0.82 to 0.00).
Lean Mass Change (%): Decreased by 1.05% (95% CI: −1.58 to −0.52).
Proportion of Total Weight: Lean mass increased by 1.51% as a proportion of total body weight (95% CI: 0.81–2.22).
Long-Term Use (>52 weeks):
Absolute Lean Mass: Decreased by 2.65 kg (95% CI: −3.14 to −2.16).
Lean Mass Change (%): Decreased by 4.27% (95% CI: −5.08 to −3.46).
Proportion of Total Weight: Lean mass increased by 2.53% as a proportion of total body weight, though this result was not statistically significant ($p=0.15$).
Semaglutide (2.4 mg/week)
Duration: ~68 weeks
Absolute Lean Mass: Decreased by 5.44 kg (95% CI: −7.07 to −3.81).
Lean Mass Change (%): Decreased by 9.9% (95% CI: −14.26 to −6.42).
Proportion of Total Weight: Lean mass increased by 2.95% as a proportion of total body weight (95% CI: 1.42–4.48).
Tirzepatide (5–15 mg/week)
Duration: 72 weeks
Lean Mass Change (%): Decreased by 10.9% compared to a 2.0% decrease in the placebo group (Estimated treatment difference: −8.3%).
Fat-to-Lean Ratio: Fat mass loss was roughly 3× greater than lean mass loss.
Data Limitation: Absolute lean mass change was not poolable in the meta-analysis because the SURMOUNT-1 trial did not report standalone results for its DXA-measured subgroup.The clearest pattern in the data: effect size tracks with total weight loss. Semaglutide and tirzepatide produce more total weight loss than liraglutide, and they also produce more absolute lean mass loss. This is consistent with what you'd expect physiologically — when you lose a larger fraction of your total body mass, some of that loss will be lean tissue, regardless of which drug got you there.
A complementary 2026 meta-analysis (Beavers et al., cited within the Laverde study) helps interpret these numbers in context: it found that lean mass typically accounts for around 30% of total weight lost on GLP-1 therapy — comparable to the proportion lost after bariatric surgery. Within Laverde's own dataset, that proportion ranged from 14–22% with liraglutide up to roughly 45% with semaglutide and about 26% with tirzepatide.
In other words, semaglutide's higher percentage may partly reflect that the people in that trial simply lost more total weight, not that the drug is uniquely "muscle-toxic" compared with the others at matched amounts of weight loss.
5. Is the Muscle Loss Clinically Significant, or Just Statistically Significant?
This is the question that actually matters for your decision-making, and it's where most coverage of this topic stops short.
Three things from the data support a measured, non-alarmist read:
1. None of the included trials measured muscle strength or physical function. The Laverde meta-analysis is explicit about this limitation: the included RCTs did not assess grip strength, walking speed, or any functional outcome. The authors note that functional decline is known to occur earlier and progress faster than measurable changes in muscle mass — meaning a drop in lean mass on a scan doesn't necessarily translate into weaker muscles or reduced function. Without that data, "clinically significant muscle loss" can't actually be confirmed from this trial set; only "statistically significant lean mass loss" can.
2. Placebo groups lost muscle too. Even patients getting a placebo plus lifestyle counseling lost some lean mass over the study periods — consistent with the expected 0.3–1% per year of age-related muscle decline. This tells you that not all of the lean-mass loss in the drug groups is necessarily abnormal or drug-specific; some of it is the ordinary trajectory of aging, which the drug groups simply experienced on top of much larger total weight changes.
3. The studied populations were young, healthy, and short-term. Average participant age across the included trials ranged from 31 to 51 years, with a low burden of comorbidities, and most trials ran less than a year. The authors flag this directly: results may not generalize to older adults, people with diabetes, or those with multiple chronic conditions — precisely the groups most vulnerable to sarcopenia (age-related muscle loss) in the first place. If you're 65+, or already have low muscle mass, this evidence base has very little to say about your specific risk.
What does have function data: MRI substudies
One dataset did look beyond simple lean mass: the SURPASS-3 MRI substudy of tirzepatide in type 2 diabetes, which used actual muscle-volume imaging rather than DXA. It found a real reduction in muscle volume (−0.64 L) and a small drop in an MRI-derived muscle "z-score" (−0.22) relative to insulin therapy. This is more specific evidence of a measurable, if modest, effect on the muscle compartment itself — and it reinforces that "lean mass" results, while imperfect, are pointing at something real, not solely a methodological artifact.
The honest synthesis: there is a real signal of muscle-compartment shrinkage with these drugs, proportional to overall weight loss, but the current evidence cannot tell you whether that translates into weaker muscles or worse physical function — because almost nobody has measured it directly in the trials that matter most.
6. A Different Lens: What Happens in Fatty Liver Disease (MASLD)?
Because so much of "lean mass" interpretation hinges on liver-fat changes, a 2026 systematic review in Liver International (Iorra et al.) specifically asked: what happens to muscle in people who have metabolic dysfunction-associated steatotic liver disease (MASLD), a population where this confound is most relevant?
This review took a different, arguably more clinically rigorous approach. Across 12 studies (810 patients), it didn't just track lean mass — it separately evaluated muscle mass, muscle strength, and muscle quality (the degree of fat infiltration within muscle tissue, called myosteatosis).
The findings, read carefully, are genuinely reassuring on the functional side:
Muscle mass: A numerical reduction was seen in most cohorts, but it reached statistical significance in only 3 of 11 studies. Where lean mass loss did happen, it was generally proportional to overall weight loss (in one trial, about 27% of weight lost was lean mass — in line with general weight-loss expectations, not an outlier).
Muscle strength: Across the available data (handgrip strength and sit-to-stand testing), strength was largely preserved despite meaningful weight loss. One study even showed modest improvement in sit-to-stand performance — a functional gain, not a loss.
Muscle quality: Multiple studies showed a reduction in intramuscular fat (myosteatosis), suggesting the muscle tissue that remained was, if anything, higher quality after treatment.
The review's own conclusion states it directly: "Current evidence suggests that GLP-1RA therapy is not associated with clinically meaningful loss of muscle mass or strength in adults with MASLD, with early data indicating possible improvements in muscle quality."
Why does this review reach a more reassuring tone than the obesity-dose meta-analysis? A few honest reasons:
It measured strength directly in some studies, rather than relying solely on lean-mass proxies.
Most of the included studies used lower, diabetes-range doses, not the higher obesity doses — which, consistent with the dose-dependency seen elsewhere, would be expected to show a smaller effect.
It draws heavily on non-randomized, observational studies (9 of 12), which carry a higher risk of bias (rated high-risk in over 75% by the ROBINS-I tool) — a real weakness when interpreting the strength of this reassurance.
The included strength data itself was sparse: just three studies, 477 people total, with relatively short follow-up.
So the fair conclusion isn't "one study is right and the other is wrong." It's that the obesity-dose RCT evidence shows a real, measurable absolute lean-mass loss, while the function-focused MASLD evidence — albeit from weaker study designs — suggests that strength holds up. Both can be true simultaneously, and that's actually the most likely real-world picture: some tissue change, with the body's functional capacity largely intact, at least over the time periods studied so far.
7. The Mechanism: Why Do GLP-1 Drugs Affect Muscle At All?
You don't need a biochemistry degree to understand the core mechanism, and understanding it clarifies why "some lean mass loss" is expected rather than alarming.
1. Caloric restriction, not drug toxicity, is the primary driver. GLP-1 receptor agonists work mainly by increasing satiety and slowing gastric emptying, leading people to eat significantly less. Any time the body is in a sustained calorie deficit — whether from a GLP-1 drug, a diet, or bariatric surgery — some lean tissue loss is essentially universal. The reviewed literature places this at roughly 15–45% of total weight lost, depending on the population and method, which lines up closely with what's been reported after bariatric surgery for decades. GLP-1 drugs are not uniquely catabolic; they're simply a very effective way to create a large, sustained calorie deficit.
2. Lower amino acid and physical-activity stimulus. When you eat less — especially less protein — and your overall energy intake drops, your body has fewer of the raw materials and hormonal signals (like insulin and amino acid availability) that normally support muscle protein synthesis. Without a compensating stimulus (resistance training, adequate protein), some muscle loss alongside fat loss is the default physiological response to almost any form of weight loss.
3. There's no confirmed direct toxic effect on muscle tissue. This is worth stating clearly because it's often implied otherwise: the MASLD review notes explicitly that no direct catabolic effect of GLP-1 receptor agonists on skeletal muscle has been demonstrated. If anything, preclinical (animal) research suggests these drugs may have some protective effects on muscle tissue in the context of metabolic disease, by reducing local inflammation and supporting muscle-regulating factors. The mechanism of lean-mass loss appears to be "weight loss happening," not "this drug attacks muscle."
4. Organ and fluid shifts inflate the apparent effect. As covered in Section 2, especially in people with fatty liver disease, a portion of "lean mass" loss reflects liver shrinkage and fluid changes rather than muscle tissue loss specifically.
8. Evidence Summary Table
Laverde et al. 2026 (International Journal of Obesity)
Study Design & Population: Meta-analysis of 7 Randomized Controlled Trials (RCTs) involving 821 participants with obesity taking obesity-approved doses.
Absolute Lean Mass Result: Decreased by −1.74 kg (95% CI: −3.04 to −0.45).
Lean Mass as % of Total Weight Result: Increased by +1.81% (95% CI: 1.1 to 2.52).
Certainty & Bias: High certainty (GRADE framework) with a low risk of bias across the included RCTs.
Iorra et al. 2026 (Liver International)
Study Design & Population: Systematic review of 12 studies (3 RCTs and 9 observational studies) involving 810 participants with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD).
Muscle Strength Result: Largely preserved across handgrip and sit-to-stand tests, with one outcome showing improvement.
Muscle Quality Result: Myosteatosis (fat accumulation in muscle) was improved or preserved in most studies.
Certainty & Bias: High risk of bias in the observational studies (ROBINS-I tool), "some concerns" in the RCTs (RoB 2 tool), and a small overall sample size ($n=139$) specifically evaluating muscle quality.
SURPASS-3 MRI Substudy (Cited in Laverde et al.)
Study Design & Population: Post-hoc randomized controlled trial analysis evaluating participants with Type 2 Diabetes (T2D) taking tirzepatide versus insulin.
Muscle Volume Result: MRI-measured muscle volume decreased by −0.64 L (95% CI: −0.74 to −0.54).
Certainty & Bias: Limited by its post-hoc nature; participants were not originally randomized specifically for this muscle volume outcome.
Jalleh et al. 2026 (Journal of Clinical Investigation)
Study Design & Population: Narrative safety review (not a systematic review); no specific participant count ($N/A$).
Adverse-Effect Profile Result: Gastrointestinal (GI) side effects remain the most common. Concerns regarding pancreatitis and cancer have been largely dispelled by long-term clinical trials.
9. How to Protect Your Muscle on a GLP-1: The Practical Protocol
The research consensus across every source reviewed here — the obesity-dose meta-analysis, the MASLD review, and the broader literature they both cite — converges on the same two interventions: resistance exercise and adequate protein intake. Neither is optional if preserving muscle is a priority; both are explicitly called out by the trial authors as necessary companions to drug therapy, not optional extras.
Step 1: Prioritize protein at every meal
With appetite substantially suppressed, total food volume drops — so the quality of what you do eat matters more, not less.
Aim for protein at each meal/snack opportunity rather than back-loading it into one meal
Lean proteins (poultry, fish, eggs, dairy, legumes, tofu) tend to sit better with the slowed digestion these drugs cause than very fatty or fried protein sources
If nausea limits solid food, protein shakes, Greek yogurt, or cottage cheese can be easier to tolerate than a full meal
This article does not provide specific gram-per-kilogram targets, since individual protein needs vary substantially by kidney function, age, and other health factors — talk to a doctor or registered dietitian for a number tailored to you.
Step 2: Make resistance training non-negotiable
Cardio alone does not send the "preserve this tissue" signal to muscle the way mechanical loading does.
2–3 resistance sessions per week, covering the major muscle groups, is the pattern most consistently associated with preserved lean mass during weight loss in the broader literature
You do not need a gym: bodyweight training, resistance bands, or a basic dumbbell set are sufficient if used consistently
Progressive overload (gradually increasing difficulty over time) matters more than the specific exercises chosen
Step 3: Monitor more than the scale
Body weight alone can't tell you whether you're losing fat, muscle, or both.
If accessible, a DXA scan or bioelectrical impedance device at baseline and periodically thereafter can track the composition of weight lost
A simpler proxy: track strength on a couple of key lifts or movements. If you're getting weaker as the weight comes off, that's a more direct signal of muscle loss than the scale alone
Grip strength (measurable with an inexpensive hand dynamometer) is the metric used in several of the studies reviewed here and correlates with broader physical function
Step 4: Don't under-eat on top of the drug's appetite suppression
GLP-1 drugs already create a significant calorie deficit on their own. Deliberately restricting further, on top of the drug's effect, increases the relative proportion of weight lost from lean tissue rather than fat. This is a common and avoidable mistake — more in Section 10.
Step 5: Loop in your care team
Especially relevant if you're over 65, have pre-existing low muscle mass, kidney disease, or multiple chronic conditions — populations the underlying trials explicitly did not study in depth. A clinician can help individualize monitoring and may suggest baseline functional testing (grip strength, chair-stand test) to track over time.
10. Common Myths and Mistakes
Myth: "GLP-1 drugs eat away your muscle directly." Not supported by current evidence. No study reviewed here demonstrates a direct catabolic (muscle-destroying) action of these drugs on muscle tissue. The lean-mass loss observed appears to be a downstream consequence of the calorie deficit they create — the same mechanism behind muscle loss from any major weight-loss method, including diet alone or bariatric surgery.
Myth: "Lean mass loss on a scan equals muscle loss." As covered in Section 2, "lean mass" includes organs, bone, and fluid — not just muscle. In people with fatty liver disease specifically, a meaningful portion of measured "lean mass" loss may reflect a shrinking, healthier liver rather than weaker muscles.
Mistake: Stacking aggressive calorie restriction on top of the drug. Because appetite is already suppressed, some people add a strict diet on top, assuming "more deficit = better results." This is precisely the scenario most likely to maximize lean-mass loss relative to fat loss, since severe caloric restriction without adequate protein and resistance training disproportionately taxes muscle tissue.
Mistake: Skipping resistance training because "the weight is coming off anyway." The weight loss happening doesn't mean it's happening from the right places. Every source in this review treats resistance training as the primary lever for ensuring weight loss comes preferentially from fat.
Myth: "If I'm losing weight fast, it must mostly be fat." Faster, more aggressive weight loss is generally associated with a larger absolute lean-mass loss in the comparative data above (semaglutide and tirzepatide vs. liraglutide). Total amount of weight lost, not the drug per se, appears to be the main driver of how much lean tissue goes with it.
Myth: "Once I stop the drug, I'll just get my muscle back automatically." Muscle regrowth after a period of loss requires the same inputs that prevent loss in the first place — protein and mechanical loading — it doesn't happen passively just because the drug is discontinued. Weight regain after stopping a GLP-1 (which is common) without resistance training tends to come back disproportionately as fat, not muscle, which can worsen body composition over the long run.
11. Safety Snapshot: Where Muscle Loss Fits Among Other Side Effects
To keep muscle-related concerns in proportion, it's worth a brief look at the broader adverse-effect picture, drawn from a 2026 review in the Journal of Clinical Investigation dedicated specifically to GLP-1 safety.
Gastrointestinal effects (nausea, vomiting, diarrhea, constipation) are by far the most common adverse events and the leading cause of discontinuation. In the obesity-dose trials reviewed above, GI side effects occurred in roughly 47–82% of treated patients depending on the drug, versus 8–72% on placebo.
Pancreatitis and pancreatic cancer concerns, which circulated heavily in earlier years, have been substantially addressed by long-term trial data, according to this safety review.
Thyroid cancer risk may be modestly increased and remains an area of ongoing monitoring — this is a recognized contraindication area, particularly for anyone with a personal or family history of medullary thyroid carcinoma.
Gallbladder disease (cholelithiasis) occurred in up to 2.6% of patients in the obesity-dose trials — a known, dose-related effect linked to rapid weight loss generally, not unique to GLP-1 drugs.
Discontinuation due to any adverse event occurred in roughly 7–9% of patients across the major obesity trials reviewed here.
Muscle/lean-mass loss did not appear as a discontinuation-driving adverse event in any of the trials reviewed — it was identified through planned body-composition substudies, not through patients reporting it as a problem severe enough to stop treatment.
This is not medical advice. GLP-1 receptor agonists are prescription medications with real risks and contraindications. Talk to your doctor about whether one is appropriate for you, and don't start, stop, or adjust a dose without medical guidance.
12. FAQs
Does Ozempic or Wegovy cause muscle loss? Semaglutide (the active ingredient in both) is associated with a statistically significant average loss of absolute lean mass — about 5.44 kg over roughly 68 weeks in the largest dose-specific analysis available. However, fat loss occurs at a substantially greater rate, so overall body composition (the proportion of lean vs. fat mass) tends to improve. Whether this translates into weaker muscles specifically hasn't been directly tested in these trials.
Is the muscle loss from GLP-1 drugs permanent? The available trials don't follow patients long enough after stopping the drug to answer this directly. In general, muscle tissue responds to the inputs you give it — protein and resistance training rebuild it; inactivity and under-eating do not. There's no evidence the muscle loss observed is irreversible by mechanism.
Which GLP-1 drug causes the least muscle loss? In the dose-specific meta-analysis covered above, liraglutide (3 mg/day) under 52 weeks showed the smallest absolute lean-mass loss (−0.41 kg) compared with semaglutide (−5.44 kg). However, liraglutide also produces less total weight loss, so this isn't necessarily evidence that it's "gentler" on muscle specifically — it may simply reflect a smaller overall effect size.
Can I prevent muscle loss while taking a GLP-1? You can't fully eliminate lean-mass loss during any significant weight-loss process, but you can substantially shift the ratio of fat to muscle lost in your favor. The two interventions with the most consistent support across this literature are resistance training (2-3x weekly) and adequate dietary protein at each meal.
Should I take creatine while on a GLP-1? None of the trials reviewed here tested creatine supplementation specifically in this population, so there's no direct evidence to cite either way. Creatine is generally well-studied for supporting resistance-training adaptations in other contexts; ask your doctor or a dietitian whether it's appropriate for your individual situation.
Does tirzepatide (Mounjaro/Zepbound) cause more muscle loss than semaglutide? The SURMOUNT-1 trial reported a −10.9% lean mass change with tirzepatide vs. −9.9% with semaglutide in the respective trials — similar in magnitude, though these come from different trials with different populations, not a head-to-head comparison, so a direct ranking isn't statistically supportable from this data alone.
Is "lean mass loss" the same as "sarcopenia"? No. Sarcopenia is a specific clinical diagnosis requiring documented loss of muscle strength as a primary criterion, with low muscle quantity/quality as a secondary confirming factor. None of the obesity-dose RCTs reviewed measured strength, so none can actually diagnose treatment-induced sarcopenia — they measured a body-composition proxy, not the clinical syndrome.
I have fatty liver disease (MASLD/NAFLD) — does that change the muscle-loss risk? The MASLD-specific systematic review found muscle strength was largely preserved in this population despite meaningful weight loss, and some markers of muscle quality even improved. Because MASLD patients often have an enlarged, fatty liver, some of their "lean mass" loss on scans may specifically reflect liver shrinkage rather than muscle loss — an effect particularly relevant to this group.
Are older adults at higher risk of muscle loss on GLP-1 drugs? This is a genuine evidence gap. The major obesity-dose trials studied relatively young, healthy populations (average age 31–51) with few comorbidities. Older adults — who have less muscle reserve to begin with — were not well represented, and the original researchers explicitly flag this as a priority for future study.
Do GLP-1 drugs affect bone density too? This wasn't a primary focus of the trials reviewed here, though it's a related and active area of research given that bone, like muscle, is part of "lean mass" on a DXA scan. If bone health is a specific concern for you, raise it directly with your prescribing physician.
Conclusion: What Should You Actually Do With This Information?
The honest, evidence-grounded summary looks like this:
GLP-1 receptor agonists at obesity doses cause a real, statistically robust reduction in absolute lean mass — roughly 1.7 kg on average across drugs, more with semaglutide specifically. At the same time, your overall body composition improves, because fat loss outpaces that lean-mass loss by a wide margin. Whether this measurable lean-mass change actually translates into weaker, less functional muscle is the one question the strongest trials in this space did not directly test — and where the available function-focused data (largely from weaker observational designs) is more reassuring than alarming.
Your action steps:
If you're on, or considering, a GLP-1 drug — don't let lean-mass headlines alone drive your decision. Discuss your individual risk factors (age, baseline muscle mass, comorbidities) with your prescriber.
Build resistance training into your routine before or as soon as you start treatment — not as an afterthought once you notice changes.
Prioritize protein at each meal, especially as appetite drops.
Track strength, not just weight, if you want a real signal of whether your muscle is holding up.
If you're older, have existing low muscle mass, or multiple health conditions, ask your doctor about baseline functional testing — this population is underrepresented in the current trial evidence, which is reason for individualized caution, not avoidance.
This is an active, fast-moving area of research. As longer-term studies with direct strength and function measurements are published, this guidance may be refined — we'll update this article as that evidence matures.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals. That it's not personalized medical advice. If you're implementing changes, consult a doctor/dietitian as emphasized
Explore related reads on this site:
Your Cholesterol Isn’t the Whole Story: The Hormone Imbalances Driving Heart Disease
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Remnant Cholesterol: The Hidden Link Between Insulin Resistance, Type 2 Diabetes, and Heart Disease
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
References
Laverde, L. P., Muñoz-Velandia, O. M., Alfonso, D., & Gómez Medina, A. M. (2026). Effect of GLP-1 receptor agonists at doses for obesity management on muscle health: systematic review and meta-analysis of randomized controlled trials (RCTs). International Journal of Obesity. https://doi.org/10.1038/s41366-026-02118-y
Iorra, F., Jayakar, T., Yee, M., Thursz, M. R., Schaan, B. D., & Manousou, P. (2026). Effects of GLP-1 Receptor Agonists on Muscle Mass, Strength, and Quality in MASLD: A Systematic Review. Liver International, 46(5), e70643. https://doi.org/10.1111/liv.70643
Jalleh, R. J., Talley, N. J., Horowitz, M., & Nauck, M. A. (2026). The science of safety: Adverse effects of GLP-1 receptor agonists as glucose-lowering and obesity medications. Journal of Clinical Investigation, 136(4), e194740. https://doi.org/10.1172/JCI194740
Ceasovschih, A., Asaftei, A., Lupo, M. G., et al. (2025). Glucagon-like peptide-1 receptor agonists and muscle mass effects. Pharmacological Research, 220, 107927. https://doi.org/10.1016/j.phrs.2025.107927
Pantazopoulos, D., Gouveri, E., Papazoglou, D., & Papanas, N. (2025). GLP-1 receptor agonists and sarcopenia: Weight loss at a cost? A brief narrative review. Diabetes Research and Clinical Practice, 229, 112924. https://doi.org/10.1016/j.diabres.2025.112924
Karakasis, P., Patoulias, D., Fragakis, N., & Mantzoros, C. S. (2024). Effect of glucagon-like peptide-1 receptor agonists and co-agonists on body composition: systematic review and network meta-analysis. Metabolism, 156113.
Jiao, R., Lin, C., Cai, X., et al. (2024). Characterizing body composition modifying effects of a glucagon-like peptide 1 receptor-based agonist: a meta-analysis. Diabetes, Obesity and Metabolism, 27, 259-267.
Linge, J., Birkenfeld, A. L., & Neeland, I. J. (2024). Muscle mass and glucagon-like peptide-1 receptor agonists: adaptive or maladaptive response to weight loss? Circulation, 150(16), 1288-1298.
Sattar, N., Neeland, I. J., Dahlqvist Leinhard, O., et al. (2025). Tirzepatide and muscle composition changes in people with type 2 diabetes (SURPASS-3 MRI): a post-hoc analysis. Lancet Diabetes & Endocrinology, 13, 482-493.
Wilding, J. P. H., Batterham, R. L., Calanna, S., et al. (2021). Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine, 384, 989-1002.
Jastreboff, A. M., Aronne, L. J., Ahmad, N. N., et al. (2022). Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine, 387, 205-216.
Lundgren, J. R., Janus, C., Jensen, S. B. K., et al. (2021). Healthy weight loss maintenance with exercise, liraglutide, or both combined. New England Journal of Medicine, 384, 1719-1730.
Beavers, K. M., Cortes, T. M., Foy, C. M., et al. (2025). GLP1Ra-based therapies and DXA-acquired musculoskeletal health outcomes: a focused meta-analysis of placebo-controlled trials. Obesity, 33, 225-237.
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., et al. (2019). Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age and Ageing, 48(1), 16-31.
Wei, S., Nguyen, T. T., Zhang, Y., et al. (2023). Sarcopenic obesity: epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Frontiers in Endocrinology, 14, 1185221.
Neeland, I. J., Linge, J., & Birkenfeld, A. L. (2024). Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies. Diabetes, Obesity and Metabolism, 26(4), 16-27.
Marjot, T., Armstrong, M. J., & Stine, J. G. (2025). Skeletal Muscle and MASLD: Mechanistic and Clinical Insights. Hepatology Communications, 9(6), 1-21.
Moolla, A., Poolman, T., Othonos, N., et al. (2025). Randomised trial comparing weight loss through lifestyle and GLP-1 receptor agonist therapy in people with MASLD. JHEP Reports, 7(5), 101363.
Ditzenberger, G. L., Lake, J. E., Kitch, D. W., et al. (2025). Effects of Semaglutide on Muscle Structure and Function in the SLIM LIVER Study. Clinical Infectious Diseases, 80(2), 389-396.
Mitchell, W. K., Williams, J., Atherton, P., et al. (2012). Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Frontiers in Physiology, 3, 260.
Note: This reference list includes the primary studies discussed in depth above plus the key supporting citations drawn directly from their reference lists. It is not an exhaustive bibliography of the GLP-1/muscle literature