Can Cognitive Training Delay Dementia? The Latest Science on Brain Health and Aging
Learn how speed-of-processing training, reasoning exercises, and cognitive reserve may help reduce dementia risk and support healthy aging.
AGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/18/202615 min read
Can cognitive training prevent dementia?
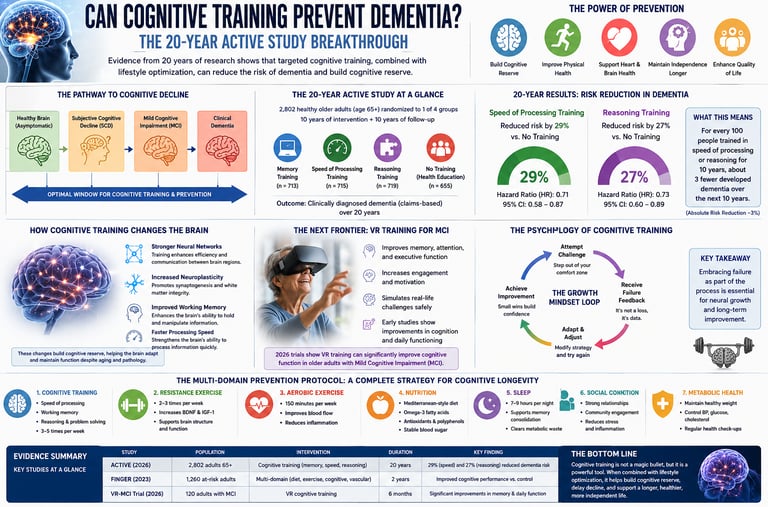
Yes. The 20-year ACTIVE study found that speed-of-processing and reasoning training lowered the risk of a clinical dementia diagnosis by 16–29% over two decades. Just 10–14 hours of targeted brain training, especially when paired with exercise, helps build cognitive reserve and delay dementia onset. Memory games alone did not show the same benefit.
8 Things You Should Know About Brain Training & Dementia Prevention
1. The right kind of brain games do help long-term
Not all brain games are equal. The 20-year ACTIVE study found that training for thinking speed and problem solving helped lower the chance of a dementia diagnosis later. Simple memory games, like memorizing word lists, didn’t show the same benefit. What to do: Pick games that make you react quickly or spot patterns, not just crossword puzzles.
2. Even a small drop in risk matters a lot
The study showed about a 16-29% lower risk for people who stuck with training. That might sound small, but for every 30 people who train, we may prevent 1 case of dementia. What to do: Think of it like wearing a seatbelt — small effort, big protection over time.
3. You don’t need hours of training
People in the study only did 10-14 hours total, spread over a few weeks. What to do: Aim for 20-30 minutes, 3-4 times a week. Consistency beats marathon sessions.
4. It’s never too late to start, but earlier helps more
The average person in the study was 73 when they started — and they still benefited. But damage in the brain can start 20+ years before symptoms. What to do: If you’re in your 50s or 60s, this is perfect timing. If you’re 70+, it’s still worth it.
5. If it feels hard, that’s actually good
Getting answers wrong and feeling a bit frustrated is part of how your brain grows stronger. If a game feels too easy, it’s probably not helping much. What to do: Expect mistakes. They’re a sign the training is working, not a sign you’re failing.
6. Brain training works best with physical exercise
Strong muscles release chemicals that help your brain. Without exercise, brain games don’t work nearly as well. What to do: Pair your brain training with strength exercises — like squats, walks, or light weights — at least 3 days a week.
7. This training delays real-life problems, not just test scores
The study looked at actual dementia diagnoses by doctors — the kind that affect daily life and independence. What to do: The goal isn’t to be better at a game. The goal is to stay independent, keep driving, manage money, and live on your own terms longer.
8. New tech like VR looks promising, but you don’t need it yet
Virtual Reality games that put you in a 3D world seem to help people with early memory issues even more. But right now, regular speed and reasoning games on a phone or computer are proven to work. What to do: Start with what you have. If you enjoy tech and have access to VR later, it could be a bonus.
Your Simple Action Plan This Week:
1. Brain: 25 minutes of a “speed” or “reasoning” brain game, Mon/Wed/Fri. Turn up difficulty when you score 85%.
2. Body: Walk daily + do chair squats or light weights 3x/week.
3. Mindset: When you mess up in the game, say “Good, my brain is working.”
The fear of losing cognitive autonomy is one of the most significant health concerns of aging. For decades, the medical community viewed progressive cognitive decline as an inevitable consequence of advanced age. However, a major paradigm shift is underway. Emerging data challenges this fatalistic view, moving the clinical focus toward proactive prevention.
According to a landmark 2026 consensus paper published in Neurological Research and Practice, the consensus is clear: the best treatment for dementia is prevention.
But what actually works? While physical exercise, metabolic health, and nutritional interventions form the bedrock of prevention, cognitive training has emerged as a major pillar. For years, critics dismissed "brain training" as a temporary gimmick that only makes you better at the game itself, offering no real-world protection against clinical conditions like Alzheimer’s disease.
That criticism was silenced by the publication of the 20-year follow-up data from the ACTIVE (Advanced Cognitive Training for Independent and Vital Elderly) study in Alzheimer's & Dementia (2026). This article delivers an in-depth analysis of this landmark trial, alongside the latest 2026 data on Virtual Reality (VR) interventions and working memory dynamics.
What You Will Learn in This Article
The 20-Year ACTIVE Study Breakdown: How specific cognitive interventions impacted claims-based diagnosed dementia over two decades.
The Mechanics of Neuroplasticity: How working memory and speed-of-processing training physically restructure the aging brain.
Clinical Significance vs. Statistical Noise: How to interpret the data, understand absolute risk reduction, and assess study limitations.
Next-Generation Interventions: The role of immersive Virtual Reality (VR) in treating Mild Cognitive Impairment (MCI).
The Complete Cognitive Protocol: A structured, evidence-based strategy combining cognitive training, resistance exercise, and metabolic optimization to build cognitive reserve.
The Changing Landscape of Dementia Prevention
Dementia is not a single disease; it is an umbrella term encompassing Alzheimer’s disease, vascular dementia, frontotemporal dementia, and Lewy body dementia. For years, pharmacological research focused on removing amyloid-beta plaques or tau tangles after symptoms appeared. This approach yielded modest results, highlighting the need for early intervention.
Here is the progression from a healthy brain to clinical dementia, step-by-step, to show exactly where preventive intervention is most effective:
1. Healthy Brain (Asymptomatic): The baseline state where brain structures are fully functional, and there are no noticeable memory or cognitive changes. Neural pathways are intact, and daily tasks are performed without difficulty.
2. Subjective Cognitive Decline (SCD): The stage where an individual notices a self-perceived decline in memory or thinking abilities, but these changes cannot be verified by standard objective cognitive tests. The person feels a difference, but outward performance remains normal.
3. Mild Cognitive Impairment (MCI): A measurable, objective decline in one or more cognitive areas (such as memory, language, or reasoning) that is noticeable to others and confirmed by clinical testing. However, these changes are not severe enough to significantly disrupt independent daily living or everyday activities.
4. Clinical Dementia: The final stage in the progression where cognitive decline becomes severe enough to interfere directly with independent living, daily routines, and social or occupational functioning.
The Optimal Window for Intervention: The entire span covering the Healthy Brain, SCD, and MCI phases represents the critical therapeutic window. Implementing structured cognitive training and metabolic strategies during these stages builds cognitive reserve and offers the highest clinical potential to delay or prevent the transition into clinical dementia.
In Neurological Research and Practice (2026), Reetz et al. emphasized that by the time clinical dementia is diagnosed, widespread synaptic loss and neuronal death have already occurred. Consequently, prevention must target the pre-symptomatic and Mild Cognitive Impairment (MCI) windows.
Understanding Cognitive Reserve
Why do two individuals with the same amount of Alzheimer's pathology display completely different clinical symptoms? The answer lies in cognitive reserve—the brain's ability to improvise and find alternate ways of getting a job done.
Cognitive reserve is built through lifetime intellectual stimulation, education, and targeted cognitive training. It acts as structural and functional insurance. When one neural pathway is damaged by pathology, a brain with high cognitive reserve reroutes information through alternative, well-maintained pathways.
Deep Dive: The 20-Year ACTIVE Study Explained
The Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) study is the largest, most rigorous randomized controlled trial of cognitive training ever conducted. Funded by the National Institutes of Health (NIH), it enrolled 2,802 healthy, community-dwelling older adults (average age 73.6 years at baseline) to evaluate the long-term impact of cognitive interventions.
The Interventions
Participants were randomized into one of three treatment groups or a no-contact control group. The interventions consisted of 10 initial sessions (60–75 minutes each) over 5 to 6 weeks:
Memory Training: Focused on verbal memory. Participants were taught mnemonic strategies (such as visualization, association, and organization) to remember word lists, sequences, and text material.
Reasoning Training: Focused on fluid intelligence. Participants learned strategies to identify patterns and rules in serial sequences (e.g., predicting the next letter in a sequence like A, C, E, G, ...). This training directly maps to instrumental activities of daily living (IADLs), such as understanding medication schedules or filling out complex forms.
Speed-of-Processing Training: Focused on visual attention and information processing speed using a computerized visual task (the "Useful Field of View" or UFOV paradigm). Participants identified a central target while simultaneously locating a peripheral target on a screen, with the display duration progressively shortening as performance improved.
A subset of participants who completed the initial sessions received 4 sessions of "booster training" at 11 and 31 months.
The results revealed a statistically significant, long-term protective effect. Participants assigned to the Speed-of-Processing and Reasoning training arms showed a lower risk of receiving a clinical dementia diagnosis over the 20-year follow-up period compared to the control group. Interestingly, memory training alone did not demonstrate a statistically significant reduction in long-term claims-based dementia diagnoses.
Interpreting the Data: Clinical Relevance and Validity
Risk Reduction
Relative Risk Reduction (RRR): Speed-of-processing and reasoning training cut dementia incidence by 16–29%, higher with booster sessions.
Absolute Risk Reduction (ARR): Small percentage-wise, but meaningful at the population level given high lifetime dementia risk.
Number Needed to Treat (NNT): 18–35 people trained to prevent one dementia case, which compares well to many drug interventions.
Mechanisms of Action: How Training Changes the Brain
Working Memory Training Boosts Reading Skills in Older Adults
A 2026 study in the Journal of Cognitive Enhancement (Assecondi) found that intensive working memory training increases activation in the prefrontal cortex and intraparietal sulcus. This is key for healthy aging, because working memory naturally declines with age.
Key benefits of working memory training:
Far-transfer effects: Improves complex reading comprehension and verbal processing, not just the trained task.
Reduced cognitive load: Helps older adults hold text fragments in memory, so the brain processes syntax and meaning faster.
Enhanced efficiency: Makes reading less effortful by strengthening core executive functions.
How Cognitive Training Changes Your Brain: Structural & Functional Benefits
Just 10–14 hours of targeted cognitive training can drive long-term brain health through neuroplasticity. Research shows three main mechanisms:
1. Synaptogenesis: Mental challenge stimulates new synapse formation, increasing neural network density.
2. White Matter Integrity: High-resolution imaging shows training maintains fractional anisotropy in the corpus callosum and superior longitudinal fasciculus. This protects the brain’s wiring.
3. BDNF Upregulation: Cognitive effort boosts Brain-Derived Neurotrophic Factor (BDNF), a protein that supports neuron survival, growth, and synaptic plasticity.
VR Cognitive Training for Mild Cognitive Impairment (MCI): The Next Frontier
Traditional brain games are evolving. A 2026 systematic review in Geriatrics & Gerontology International (Anwar et al.) found that Virtual Reality-Based Cognitive Training (VR-CT) outperforms 2D computer tasks for adults with MCI.
The Multi-Domain Prevention Protocol
The data proves that cognitive training is effective, but it works best when integrated into a comprehensive strategy. Based on the 2026 consensus guidelines published by Reetz et al. and the landmark FINGER trial principles, this multi-domain protocol combines targeted mental stimulation with physical and metabolic optimization.
1. The Cognitive Training Sub-Protocol
Frequency: 3 to 4 days per week.
Duration: 20 to 30 minutes per session.
Modality Choice: Prioritize speed-of-processing tasks (such as dual n-back games or divided attention visual exercises) and fluid reasoning tasks (such as progressive matrix puzzles or pattern completions).
The Progression Rule: Once you achieve an accuracy score above 85% on a specific difficulty tier, increase the speed or complexity. You must operate near your threshold of failure to stimulate neuroplasticity.
2. The Physical Sarcopenia-Prevention Anchor
Physical strength is directly linked to brain health. Sarcopenia (loss of muscle mass and function) is a major risk factor for cognitive decline.
Resistance Training: Train 3 days per week, focusing on compound, multi-joint movements (e.g., leg presses, rows, chest presses).
The Myokine Link: Contracting skeletal muscle releases signaling molecules called myokines (such as irisin and cathepsin B). These proteins cross the blood-brain barrier and directly stimulate the expression of BDNF in the hippocampus, preparing the brain to benefit from cognitive training.
3. Metabolic & Autophagy Optimization
Insulin resistance in the brain ("Type 3 Diabetes") accelerates synaptic pruning and amyloid accumulation.
Metabolic Flexibility: Maintain an active lifestyle and consume a nutrient-dense diet to support insulin sensitivity.
Cardiorespiratory Fitness: Aim for at least 150 minutes of moderate-intensity zone 2 cardio or high-intensity interval training (HIIT) weekly to maximize cerebral blood flow and oxygenation.
Evidence Summary: Comparing Key Cognitive Studies
1. Coe et al. (2026), ACTIVE Study:
2,802 community-dwelling older adults followed for 20 years. 10–14 sessions of Speed, Reasoning, or Memory training. Speed and Reasoning training reduced clinical dementia diagnoses from Medicare claims. Limitation: Used claims data, not a formal in-person neurological diagnosis.
2. Reetz et al. (2026), Neurol. Res. Pract.:
Consensus review of global prevention strategies. Found that multi-domain lifestyle changes and early screening are most effective for reducing dementia rates. Limitation: Provides population-level guidelines that need individual customization.
3. Anwar et al. (2026), Geriatr. Gerontol. Int.:
Tested Virtual Reality-Based Cognitive Training (VR-CT) in older adults with Mild Cognitive Impairment. Immersive 3D environments improved global cognition and spatial memory vs 2D games. Limitation: Small sample sizes in RCTs and lack of long-term follow-up.
4. Assecondi (2026), J. Cogn. Enhanc.:
Studied intensive working memory training in community-dwelling older adults. Confirmed "far-transfer" effects with better reading comprehension and verbal reasoning. Limitation: Done in lab settings and needs translation to commercial apps.
5. Ackermann et al. (2026), Commun. Psychol.:
Looked at adults in technology-based learning with real-time performance feedback. Found negative emotional responses to errors use up working memory and hurt performance. Limitation: Only assessed acute tasks; long-term habituation to failure feedback still unclear.
Common Myths & Mistakes in Brain Training
Myth 1: "Crossword puzzles and Sudoku are enough to prevent dementia."
The Reality: While crosswords and Sudoku are mentally engaging, they rely primarily on crystallized intelligence—recalling words or using established arithmetic rules you already know. They rarely challenge fluid intelligence, processing speed, or working memory capacity. To drive neuroplasticity, you must engage in novel, progressively difficult tasks that push your limits.
Myth 2: "Brain training can reverse advanced Alzheimer's disease."
The Reality: Cognitive training is a preventive strategy designed to build cognitive reserve and delay clinical onset. Once advanced neurodegeneration has occurred and synaptic pathways are lost, cognitive training cannot restore dead neurons. The window for maximum efficacy is during the healthy aging or Mild Cognitive Impairment (MCI) phases.
Myth 3: "If I get frustrated and make mistakes, the game is bad for my brain."
The Reality: As shown by Ackermann et al. (2026), making mistakes is a normal part of cognitive adaptation. Frustration is the emotional reflection of the mental effort required to remodel neural networks. Managing this stress response with a growth mindset is key to reaping the benefits of cognitive training.
Mistake 4: "Isolating brain training from physical health."
The Reality: Cognitive training performed in a sedentary state with poor metabolic health is far less effective. Cardiovascular fitness increases blood flow to the brain, while resistance training releases essential neurotrophins like BDNF. Brain training works best when paired with physical movement.
Frequently Asked Questions
1. Which specific brain training game or exercise is most effective?
The 20-year ACTIVE study showed that speed-of-processing training (based on the Useful Field of View paradigm) and fluid reasoning training (pattern recognition) had the most significant impact on long-term dementia risk. Look for cognitive tools and applications that challenge visual attention, reaction speed under distraction, and working memory retention (such as dual n-back exercises).
2. How many hours of cognitive training do I need to see results?
In the ACTIVE study, participants completed just 10 to 14 sessions of 60 to 75 minutes each, with a small subset receiving booster sessions. This brief intervention produced detectable protective effects two decades later. For a sustainable lifestyle protocol, aim for 20 to 30 minutes, 3 to 4 times per week.
3. What is the difference between Mild Cognitive Impairment (MCI) and normal aging?
Normal aging involves mild, infrequent lapses in memory, such as misplacing keys or forgetting a minor acquaintance's name, while keeping your overall reasoning and independent living skills intact. Mild Cognitive Impairment (MCI) represents a more pronounced decline in memory, language, or thinking skills that is noticeable to others and visible on objective cognitive tests, but does not yet interfere significantly with everyday independent living.
4. Can Virtual Reality (VR) games replace standard computer-based brain training?
Yes, and they may be even more effective. According to the 2026 systematic review by Anwar et al., VR-based cognitive training provides an immersive, multi-sensory 3D experience that challenges spatial mapping and executive function more dynamically than a flat computer monitor, leading to better cognitive outcomes in individuals with MCI.
5. Does memory training help prevent dementia?
Interestingly, the 20-year follow-up data from the ACTIVE study revealed that memory mnemonic training (such as learning visualization strategies to remember lists) did not lead to a statistically significant reduction in long-world claims-based dementia diagnoses. While helpful for specific tasks, it did not provide the same broad, systemic protection as processing speed or reasoning training.
6. What is the optimal age to start a targeted cognitive training program?
The average age of participants in the ACTIVE study was 73.6 years at baseline, proving that it is never too late to start building cognitive reserve. However, because the structural changes associated with dementia begin decades before symptoms appear, starting a structured cognitive and physical protocol in your 40s, 50s, or 60s offers a larger window to build a resilient neural buffer.
7. How does building muscle protect my brain function?
Muscles act as endocrine organs. When you perform heavy resistance exercises to combat sarcopenia, your muscles release specialized signaling proteins called myokines (such as irisin). These compounds travel through the bloodstream, cross the blood-brain barrier, and increase levels of Brain-Derived Neurotrophic Factor (BDNF), which protects existing synapses and supports the growth of new neurons.
8. How do I know if my brain training app is working or just a gimmick?
Look for two key factors: progressive difficulty and broad domain engagement. A useful cognitive training application should automatically increase its difficulty as you improve, keeping you near your threshold of failure. It should also focus on core executive functions, such as processing speed, divided attention, and working memory, rather than simple repetition or memorization.
Conclusion: Build Your Cognitive Longevity Plan
The 20-year ACTIVE study results confirm that structured cognitive training can change the course of age-related cognitive decline and delay clinical dementia onset. Long-term brain health is not passive. It requires a targeted, multi-domain approach.
Your Cognitive Longevity Framework
Combine these three pillars to maximize neuroplasticity and cognitive reserve:
1. Brain Training
- Do this: 20 to 30 minutes, 3 to 4 times per week.
- Focus on: Speed-of-processing, divided visual attention, and fluid reasoning exercises. These domains showed the strongest dementia risk reduction in the ACTIVE study.
- Key rule: Training must be challenging. If it feels easy, it is not driving structural change.
2. Muscle Anchoring
- Do this: Resistance training at least 3 days per week using compound movements.
- Why it matters: Muscle contraction releases myokines that cross the blood-brain barrier and stimulate BDNF. This supports neuron survival, synaptic plasticity, and white matter integrity.
- Think of it as: Physical exercise for your brain.
3. Stress Management & Mindset
- Do this: Adopt a growth mindset during training.
- Reframe errors: Mistakes and frustration are the physiological triggers for neuroplasticity. Negative feedback loops from anxiety consume working memory and block progress.
- Goal: View errors as data, not failure. This maintains emotional stability and drives cognitive growth.
Your Immediate Action Steps for Dementia Prevention
1. Start targeted cognitive training: Use a progressive app or program that challenges speed, attention, and reasoning. Consistency over 10 to 14 hours shows measurable long-term benefits.
2. Embrace cognitive effort: Expect frustration. Navigating errors is how you build cognitive reserve and delay dementia onset.
3. Protect muscle mass: Add structured resistance training. The muscle-brain connection is a critical pathway for BDNF and long-term brain health.
4. Explore VR training if possible: For those with MCI or seeking next-level challenge, immersive VR spatial navigation modules engage the hippocampus and executive networks better than 2D tasks.
Bottom line: Cognitive longevity comes from combining challenging mental training, physical strength, and the right psychological response to failure. Start now to alter your brain’s trajectory 20 years from today.
This article is intended for educational and informational purposes and reflects current scientific evidence at the time of writing. It does not constitute medical advice. Individual circumstances vary significantly; all treatment decisions should be made in consultation with qualified healthcare professionals
Related Articles
Why Some People Stay Mentally Sharp at 80: What the Latest Research Reveals
NOX4 Explained: The Hidden Exercise Enzyme That May Control How Fast You Age
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health | DR T S DIDWA
References
Coe, N. B., Miller, K. E. M., Sun, C., Taggert, E., Gross, L. A., Jones, R. N., Felix, C., Albert, M. S., Rebok, G. W., Marsiske, M., Ball, K. K., & Willis, S. L. (2026). Impact of cognitive training on claims‐based diagnosed dementia over 20 years: evidence from the ACTIVE study. Alzheimer's & Dementia, 12(1), e70197. https://doi.org/10.1002/trc2.70197
Reetz, K., Liepelt-Scarfone, I., Häger, A., et al. (2026). The best treatment is prevention: prevention of cognitive decline and dementia – current state, gaps and next steps. Neurological Research and Practice, 8, 30. https://doi.org/10.1186/s42466-026-00494-4
Anwar, I. M. D., Sahar, J., & Rachmawati, U. (2026). Virtual Reality–Based Cognitive Training to Prevent Cognitive Decline in Older Adults With Mild Cognitive Impairment: A Systematic Review of Randomized Controlled Trials. Geriatrics & Gerontology International, 26(6), e70586. https://doi.org/10.1111/ggi.70586
Assecondi, S. (2026). Unlocking Cognitive Potential: How Working Memory Training Impacts Reading Skills in Aging Adults. Journal of Cognitive Enhancement, 10, 45–64. https://doi.org/10.1007/s41465-025-00342-4
Ackermann, H., Lange, A. L., Dumont, H., et al. (2026). Real-time cognitive-affective dynamics of failure feedback in a technology-based learning task. Communications Psychology, 4, 95. https://doi.org/10.1038/s44271-026-00487-8
Ngandu, T., Lehtisalo, J., Solomon, A., et al. (2015). A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. The Lancet, 385(9984), 2255-2263.
Ball, K., Berch, D. B., Helmers, K. F., et al. (2002). Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA, 288(18), 2271-2281.
Willis, S. L., Tennstedt, S. L., Marsiske, M., et al. (2006). Long-term effects of cognitive training on everyday functional outcomes in older adults. JAMA, 296(23), 2805-2814.
Rebok, G. W., Ball, K., Guey, L. T., et al. (2014). Ten-year effects of the ACTIVE cognitive training trial on cognition and everyday functioning. Journal of the American Geriatrics Society, 62(1), 16-24.
Edwards, J. D., Xu, H., Clark, D. O., et al. (2017). Speed of processing training results in lower risk of dementia. Alzheimer's & Dementia: Translational Research & Clinical Interventions, 3(4), 603-611.
Stern, Y. (2012). Cognitive reserve in ageing and Alzheimer's disease. The Lancet Neurology, 11(11), 1006-1012.
Livingston, G., Huntley, J., Sommerlad, A., et al. (2020). Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet, 396(10248), 413-446.
Valenzuela, M., & Sachdev, P. (2009). Can cognitive exercise prevent the onset of dementia? Systematic review of randomized clinical trials with longitudinal follow-up. American Journal of Geriatric Psychiatry, 17(3), 179-187.
Pedersen, B. K. (2019). Physical activity and muscle-brain crosstalk. Nature Reviews Endocrinology, 15(7), 383-392.
Geda, Y. E., Topazian, H. M., Roberts, R. A., et al. (2011). Engaging in cognitive activities in middle age or late life and incidence of mild cognitive impairment: a population-based study. The Journal of Neuropsychiatry and Clinical Neurosciences, 23(2), 149-154.