Why Some People Stay Mentally Sharp at 80: What the Latest Research Reveals
Cognitive aging varies dramatically between individuals. Learn how exercise, sleep, and lifelong learning influence brain health.
AGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/19/202621 min read
Can your brain stay younger than your actual age?
Yes. New 2026 research shows your brain’s age doesn’t have to match your birthday. Some people stay mentally sharp at 80 because of factors like exercise, sleep, social engagement, and biology. Cognitive decline is not automatic with age. You can influence how your brain ages.
Key takeaways,
1. Your "Brain Age" Matters More Than Your Chronological Age
Aging affects everyone differently. While some individuals experience early memory lapses, others maintain laser-sharp focus deep into their senior years. Your cognitive health isn't dictated by your birthday; instead, it is driven by a combination of daily lifestyle choices, metabolic health, and genetics.
2. Neurogenesis Continues Long Past Age 80
For decades, scientists believed the brain stopped producing new cells in adulthood. However, a landmark 2026 study published in Nature shattered this myth. Researchers discovered that healthy brains continue neurogenesis—the creation of new memory cells in the hippocampus—even after age 80. Interestingly, this cellular growth only drops off significantly in those with Alzheimer’s disease, proving that the steep decline is not a normal part of aging.
3. Exercise Triggers a Brain "Clean-Up Service"
We all know that physical activity is good for the body, but 2026 clinical research shows it acts as a literal detox for your mind. When you engage in aerobic exercise, your muscles release tiny extracellular packages. These packages travel to the brain and signal your microglial cells (the brain's immune system) to clear out harmful, memory-blocking proteins.
4. Subtle Cognitive Changes Start Earlier Than Realized
Waiting until severe memory loss occurs to take action is a mistake. A recent Japanese study tracking 343 adults revealed that subtle drops in processing speed and focus often begin quietly in your 60s—even when standard clinical tests flag your memory as "perfectly normal."
SEO Pro Tip / Key Takeaway: Single-snapshot cognitive tests can miss the early signs of decline. Routine, annual cognitive checkups are essential for tracking changes over time.
5. "SuperAgers" Maintain Youthful Brain Structures
"SuperAgers" are individuals over the age of 80 who possess the memory, recall, and cognitive stamina of a 50-year-old. Neuroimaging shows that these individuals have highly active neuron growth and greater volume in the hippocampus. While genetics provide a baseline, data shows that lifelong learning, complex problem-solving, and deep social connections are what keep these brain centers firing.
6. Deep Sleep Flushes Out Toxic Waste
Think of deep sleep as your brain’s nightly garbage disposal. During the deepest stages of sleep, your glymphatic system opens up, flushing out metabolic waste and toxic proteins (like beta-amyloid) that are linked to dementia. Prioritizing seven or more hours of uninterrupted sleep—and treating conditions like sleep apnea—is non-negotiable for long-term brain health.
7. Cardiovascular Health Dictates Brain Power
What is good for your heart is directly tied to your head. Midlife chronic conditions like hypertension (high blood pressure), Type 2 diabetes, and high cholesterol are leading accelerators of vascular dementia. Aggressively managing these metabolic factors in your 40s and 50s creates a defensive shield for your brain tissue later in life.
8. You Can Build "Cognitive Reserve" at Any Age
Your brain is highly plastic, a concept known as neuroplasticity. Every time you learn a difficult new skill (like speaking a new language or playing an instrument) or engage in complex social interactions, you build "cognitive reserve." This creates an alternate network of neural pathways, providing a structural buffer that resists cognitive decline. It is truly never too late to start.
Introduction: Why Your Brain's Age Doesn't Have to Match Your Birthday
If you've watched a parent or grandparent stay razor-sharp into their 80s while a peer of the same age struggles to find words mid-sentence, you've already seen the central fact of modern aging science up close: chronological age is a remarkably weak predictor of cognitive health.
For decades, the dominant story about brain aging was simple and, frankly, a little fatalistic — neurons die, networks shrink, and memory fades on a fixed schedule. That story is now outdated. A wave of research published in 2025 and 2026, including a major review in Ageing Research Reviews and a landmark Nature study on so-called "SuperAgers," has replaced it with something more useful and more hopeful: cognitive aging is highly individualized, driven by specific, measurable biological processes that differ from person to person — and several of those processes respond to what you do.
This guide pulls together the most current, peer-reviewed evidence on healthy cognitive aging and translates it into something you can actually act on. You'll learn:
What "healthy cognitive aging" means clinically, and how it's measured
The biological hallmarks that separate resilient brains from declining ones
What large longitudinal studies actually show about the timing and pattern of decline
The mechanisms connecting exercise, sleep, and social engagement to brain resilience
How clinicians use neuropsychological testing to catch problems early — and what the data says about how predictive these tools really are
A practical, evidence-graded protocol you can start this week
Common myths that are quietly wasting your time and money
What Is Healthy Cognitive Aging?
"Healthy cognitive aging" doesn't mean your brain at 70 performs identically to your brain at 30. Processing speed and certain types of working memory do slow gradually for almost everyone. It means your cognitive trajectory stays on a stable, gently sloping curve rather than dropping off a cliff — and that you remain free of dementia and significant functional impairment.
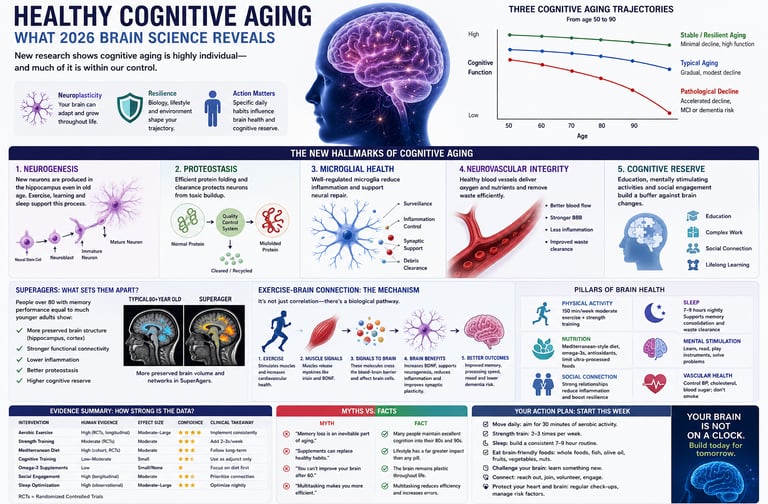
Clinically, researchers distinguish three broad trajectories:
Stable/resilient aging — minimal decline across decades, sometimes called "successful aging"
Typical aging — gradual, modest decline in speed and some memory domains, without dementia
Pathological decline — accelerated decline progressing toward mild cognitive impairment (MCI) or dementia
A comprehensive 2026 review in Ageing Research Reviews, authored by a multinational team spanning institutions in France, Sweden, Portugal, Germany, and the Netherlands, frames this clearly: cognitive aging is a highly heterogeneous process in which some people preserve stable cognitive performance across the lifespan while others show pronounced decline, and this variability means chronological age alone is a poor predictor of cognitive health. The authors argue that rather than reflecting one uniform degenerative process, healthy and unhealthy aging trajectories diverge at the molecular, cellular, and brain-network level — which is exactly why two 75-year-olds can look so different.
Why this distinction matters clinically: if cognitive aging were uniform, prevention would be pointless — you'd simply be waiting out the clock. Because it isn't uniform, the biological drivers of resilience become legitimate targets for intervention, and that reframes the entire conversation from "managing decline" to "actively building reserve."
The New Hallmarks of Cognitive Aging: What the Science Actually Shows
Hallmark 1: Adult Hippocampal Neurogenesis (and Why It May Matter More Than We Thought)
For years, scientists debated whether the adult human brain produces new neurons at all. The hippocampus — your brain's memory-indexing hub — was the focus of this debate because, in rodents, newly born neurons there are essential for certain forms of learning and memory.
A landmark February 2026 Nature study resolved much of this uncertainty using single-cell genomic profiling of postmortem human hippocampi from five groups: young adults, cognitively normal older adults, "SuperAgers" (adults over 80 with memory performance matching people decades younger), people with preclinical Alzheimer's pathology, and people with diagnosed Alzheimer's disease. The researchers analyzed the molecular profiles of 355,997 individual cell nuclei and identified neural stem cells, neuroblasts, and immature granule neurons across all these groups, providing some of the strongest direct evidence yet that neurogenesis persists into very old age in healthy individuals — and that it specifically fails in Alzheimer's disease.
Clinical interpretation: This is postmortem tissue data, not a living biomarker you can currently get tested for. Its real-world relevance right now is mechanistic insight, not a diagnostic tool. But it strongly reframes what's biologically plausible: declining neurogenesis isn't an inevitable feature of "getting older" — it's a feature that tracks specifically with disease, which is an important and encouraging distinction.
Hallmark 2: Protein Quality Control (Proteostasis)
Every cell in your body constantly builds, repairs, and recycles proteins. In aging neurons, this system slows down — and the consequences appear to concentrate at synapses, the junctions where neurons communicate.
A January 2026 Nature study from Stanford, using a novel protein-tagging method, found that in old age, synaptic proteins break down much more slowly, become more likely to clump into the tangled aggregates characteristic of neurodegenerative disease, and are increasingly taken up by microglia — the immune cells responsible for pruning damaged synapses. A separate but related 2025 Science study using killifish (a short-lived vertebrate model) traced this further upstream, showing that aging reduces the fidelity of protein production itself, via ribosome dysfunction — offering a possible root-cause explanation for why multiple aging processes start to fail together.
Clinical interpretation: This is animal and cell-level mechanistic research, several steps removed from a clinical intervention. Its main value today is generating testable biomarker candidates — for example, the Stanford team has suggested tracking neuron-derived proteins in blood as an early warning signal. Don't expect a "proteostasis supplement" to be validated any time soon; be skeptical of anyone marketing one right now.
Hallmark 3: Neurovascular and Neuroinflammatory Health
Your brain consumes about 20% of your body's oxygen and glucose despite being only 2% of body weight, which makes it acutely dependent on healthy blood flow. Chronic low-grade neuroinflammation and reduced cerebral blood flow are increasingly recognized as core drivers — not just side effects — of cognitive aging, with effects that depend heavily on timing: protective in acute injury, damaging when sustained for years.
Hallmark 4: Cognitive Reserve
"Cognitive reserve" describes the brain's capacity to maintain function despite accumulating pathology — essentially, a buffer built from education, occupational complexity, bilingualism, and sustained mental and social engagement. A 2026 editorial in Frontiers in Neuroscience on mechanisms for enhancing cognitive reserve underscores that this isn't a fixed trait fixed in youth; it's a target for intervention across the lifespan, particularly through cognitively demanding activity and social engagement.
Clinical interpretation: Cognitive reserve is one of the few hallmarks with genuinely strong human epidemiological support, because it's been studied across large populations for over 30 years. It is also one of the more actionable: lifelong learning, social complexity, and occupational demand are all measurable contributors.
How Much Decline Is "Normal"? What Longitudinal Data Reveals {#how-much-decline}
It's one thing to talk about molecular hallmarks; it's another to know what actual decline looks like in real people over real time. This is where a 2025/2026 study from Nagoya University in Japan is genuinely useful, because it directly tackles a question most aging research dodges: has cognitive decline in "normal" older adults gotten better or worse over the past decade?
Study Design (and Why It Matters for Interpreting the Results)
The researchers recruited 343 adults aged 60 and older who visited a memory clinic with various complaints — including subjective or objective memory problems — but who were classified as cognitively normal after comprehensive specialist evaluation, with assessments spanning 2013 to 2022. Participants were split into four age bands (60s, early 70s, late 70s, 80s), and the team used both cross-sectional comparison across age groups and a separate analysis tracking whether scores from a given age group shifted over the ten-year window — including across the COVID-19 pandemic.
Why the design matters: This is a clinic-based sample (people who proactively sought evaluation for memory concerns), not a random community sample. That means the findings likely don't fully generalize to the broader population of older adults who never visit a memory clinic — a key validity caveat. It also means the "cognitively normal" label reflects a comprehensive specialist workup, which is a methodological strength: misclassification of early dementia as "normal aging" is less likely than in studies relying on brief screening tools alone.
Key Findings
Certain cognitive domains — particularly processing speed and some executive function measures — showed measurable decline starting earlier than commonly assumed, even within groups still classified as cognitively normal.
The linear regression analysis examining test scores by year of assessment found patterns suggesting some test performances differed across the decade studied, raising questions about whether generational, educational, or pandemic-related factors are shifting the baseline of "normal" cognitive aging.
Clinical relevance: This study reinforces a point clinicians increasingly emphasize: a "normal" label on a screening test at one point in time doesn't mean cognition is static. It supports the case for repeated, longitudinal testing rather than single-snapshot assessment, especially in patients who present with subjective complaints — even when an initial workup is reassuring.
SuperAgers: What Their Brains Do Differently
"SuperAgers" are a small, well-studied group — fewer than 10% of older adults — defined by episodic memory performance matching people 20–30 years younger, despite being over 80. The 2026 Nature hippocampal study described above specifically included this group, and the comparison is illuminating.
Researchers found that markers of active neurogenesis — proliferating neural stem cells and immature neurons — were better preserved in SuperAgers than in typically aging adults of the same age, while these markers were sharply reduced in people with Alzheimer's pathology. As the study's lead author put it in coverage of the findings, the takeaway is that the aging brain is not fixed or doomed to decline, and understanding how some people naturally maintain neurogenesis could open the door to strategies helping more adults preserve memory and cognitive health.
A necessary caveat on validity: SuperAgers are also more likely to have larger hippocampal volumes and possibly favorable genetics from the outset. This is an observational comparison, not a randomized trial — it tells us neurogenesis preservation is associated with exceptional memory, not that boosting neurogenesis in an average ager would replicate SuperAger status. Mechanistic plausibility is strong; proof of a causal, modifiable pathway in living humans is not yet established.
The Exercise-Brain Connection: Mechanism, Not Just Correlation
Exercise is the single most consistently recommended intervention for brain health — but "exercise is good for your brain" has been repeated so often it risks sounding like a slogan rather than science. Recent mechanistic work changes that.
A 2026 Mechanism Study Worth Knowing About
A Nature Aging paper (with a 2026 author correction clarifying figure details, underscoring that even high-impact journals require post-publication scientific scrutiny) investigated how exercise helps in Alzheimer's disease mouse models — not just whether it helps.
The researchers found that swimming exercise promotes secretion of skeletal muscle-derived extracellular vesicles, which are taken up by microglia and, through gain- and loss-of-function experiments, were shown to drive a shift in disease-associated microglia that enhances clearance of amyloid-beta plaques. They further identified a specific microRNA, miR-378a-3p, as a key cargo molecule in these vesicles that regulates lipid metabolism in disease-related microglia by targeting a protein called p110α. Critically, when researchers administered vesicles engineered to overexpress this microRNA directly to AD mice — bypassing the need to actually exercise — cognitive impairment was alleviated, demonstrating a causal link rather than mere correlation.
Clinical interpretation: This is mouse data using a genetic Alzheimer's model, not a clinical trial in humans. You cannot extrapolate "exercise cures Alzheimer's" from it. What you can responsibly take from it is mechanistic plausibility for a specific, testable pathway — exercise-induced muscle signaling molecules reaching the brain and modulating immune cell behavior around amyloid plaques. This adds biological weight to the well-established human epidemiological link between physical activity and lower dementia risk; it doesn't replace the need for human trials testing this specific pathway.
A related but independently conducted study using treadmill exercise in a different Alzheimer's mouse model reinforces the theme from another angle: exercise shifted microglial energy metabolism away from a dysfunctional, glycolysis-dominant state toward a healthier balance with oxidative phosphorylation, alongside reduced amyloid-beta levels and improved spatial memory performance in maze testing. Multiple independent mechanistic pathways converging on "exercise improves microglial function and amyloid clearance" strengthens confidence in the broader phenomenon, even though each individual pathway remains preclinical.
Why This Matters for You, Practically
You don't need to wait for human trials of specific microRNA pathways to benefit from what's already well-established: large human cohort studies and meta-analyses consistently link regular aerobic activity with slower cognitive decline and reduced dementia risk. The newer mechanistic work explains why that correlation likely exists — which matters for confidence, motivation, and for guiding future drug development, even if today's actionable takeaway (move your body regularly) hasn't fundamentally changed.
Practical Application: A Step-by-Step Brain Health Protocol
This protocol organizes interventions by the strength of human evidence behind them, not by trendiness.
Step 1: Build an Aerobic Exercise Base (Strongest Human Evidence)
Target: 150 minutes per week of moderate-intensity aerobic activity (brisk walking, cycling, swimming), per general physical activity guidelines from major health bodies.
Add: 2 sessions per week of resistance training. Grip strength and overall muscular strength have been linked to cognitive trajectory in several aging cohorts, likely partly via the muscle-brain signaling pathways described above.
Why it works (mechanistically): improved cerebral blood flow, reduced neuroinflammation, and — per the newest mechanistic data — muscle-derived signals that influence microglial behavior around amyloid pathology.
Step 2: Protect Sleep Architecture
Deep slow-wave sleep is when the brain's glymphatic clearance system is most active, flushing metabolic waste — including amyloid-beta — from brain tissue. Prioritize a consistent sleep-wake schedule and address sleep apnea if present, since untreated apnea has been independently linked to accelerated cognitive decline.
Step 3: Build Cognitive Reserve Deliberately
Engage in novel, effortful learning — a new language, instrument, or skill — rather than passive familiar activities. Novelty and difficulty appear to matter more than simply "staying busy."
Maintain socially complex engagement: conversation, group activities, and relationships with cognitive demands (negotiating, planning, remembering details about others) appear to contribute more to reserve than solitary screen time.
Step 4: Manage Vascular Risk Factors Aggressively
Hypertension, type 2 diabetes, and dyslipidemia in midlife are among the most consistently replicated modifiable dementia risk factors across large epidemiological studies (including the Lancet Commission on dementia prevention). Treat these as brain health interventions, not just cardiovascular ones — work with your physician on individualized targets.
Step 5: Get a Baseline Cognitive Assessment — and Repeat It
Given the Nagoya findings that decline can begin subtly even in people clinically labeled "cognitively normal," consider a baseline neuropsychological assessment in your 50s or 60s, especially if there's a family history of dementia, and repeat testing periodically rather than relying on a single evaluation.
Safety note: Always consult your physician before starting a new exercise program, particularly if you have cardiovascular disease, uncontrolled hypertension, or other chronic conditions. This article is educational and does not replace personalized medical advice.
Evidence Summary Table:
🌟 Strongest Evidence (First-Line Clinical Strategies)
Vascular Risk Factor Control
Evidence Strength: Strong
Type of Evidence: Large Randomized Controlled Trials (RCTs) and extensive cohort studies.
Key Source: Lancet Commission on dementia prevention.
Clinical Takeaway: Strongly recommended. Managing blood pressure, cholesterol, and diabetes should be treated as a first-line strategy for protecting brain health.
Aerobic Exercise
Evidence Strength: Strong for general health data (epidemiology); preclinical for specific cellular pathways.
Type of Evidence: Human cohort studies combined with animal mechanism studies.
Key Source: Nature Aging (2026 mouse study) and decades of human tracking data.
Clinical Takeaway: Broadly recommended. While the exact biological pathways are still being mapped out in humans, the cognitive benefits are highly proven.
Cognitive Reserve Building (Novel Learning & Socializing)
Evidence Strength: Strong
Type of Evidence: Large human epidemiological studies.
Key Source: Frontiers in Neuroscience (2026 editorial) alongside decades of cognitive reserve literature.
Clinical Takeaway: Strongly recommended. Learning difficult new skills and staying socially active carries zero risk and has a highly plausible protective effect on the brain.
📈 Moderate to Strong Evidence (Recommended Routine Practices)
Repeated Neuropsychological Screening
Evidence Strength: Moderate to Strong
Type of Evidence: Longitudinal human clinical cohorts.
Key Source: European Geriatric Medicine, 2026 (Matsui et al.).
Clinical Takeaway: Recommended. Doctors should use periodic, ongoing cognitive reassessments rather than relying on a one-time test to spot decline.
Resistance Training
Evidence Strength: Moderate to Strong
Type of Evidence: Human cohort and observational studies.
Key Source: Multiple cohort studies linking physical grip strength directly to cognitive function.
Clinical Takeaway: Recommended as an excellent addition to your routine alongside aerobic exercise.
🔍 Moderate Evidence (Targeted Support & Risk Evaluation)
Sleep Optimization
Evidence Strength: Moderate
Type of Evidence: Mechanistic and observational human studies.
Key Source: Ongoing research into the glymphatic system (the brain's waste clearance process).
Clinical Takeaway: Recommended. It is highly beneficial to prioritize deep sleep and actively treat sleep disorders like sleep apnea.
Composite Neuropsychological Scores for Prediction
Evidence Strength: Moderate
Type of Evidence: Longitudinal human clinical cohort tracking 349 patients over a 3-year follow-up period.
Key Source: Frontiers in Aging Neuroscience, 2026 (Padilla et al.).
Clinical Takeaway: Highly useful for categorizing a patient's risk of progressing from Mild Cognitive Impairment (MCI) to dementia, but should not be used as a standalone diagnostic tool.
🧪 Preliminary & Preclinical Evidence (Watch This Space)
Hippocampal Neurogenesis-Targeted Therapy
Evidence Strength: Preliminary / Mechanistic
Type of Evidence: Postmortem human brain tissue and animal models.
Key Source: Nature, 2026 (Disouky et al.).
Clinical Takeaway: Not yet ready for medical use. This is a fascinating area of research to keep an eye on, but it has no immediate clinical application.
Proteostasis-Targeted Therapy & Supplements
Evidence Strength: Early Preclinical (Laboratory stage)
Type of Evidence: Animal models focusing on short-lived killifish and mice.
Key Source: Science (2025) and Nature / Stanford University (2026).
Clinical Takeaway: View with extreme skepticism. Consumers should be highly wary of memory supplements currently marketed on this basis, as human trials are still severely lacking.
Common Myths & Mistakes About Brain Aging {#myths}
Myth 1: "Memory loss is just a normal part of getting older — nothing can be done." Reality: Some slowing in processing speed is typical, but pronounced memory decline is not an inevitable consequence of aging itself — it's far more closely tied to specific pathological processes (like impaired neurogenesis and amyloid accumulation) that don't affect everyone equally.
Myth 2: "Brain-training apps will meaningfully prevent dementia." Reality: Most commercial brain-training programs improve performance on the specific trained task with limited evidence of transfer to broader cognitive function or dementia risk reduction. Real-world novel learning and socially engaging activities have stronger support.
Myth 3: "If a screening test says I'm cognitively normal, I'm in the clear." Reality: As the Nagoya longitudinal data shows, decline can be underway even within a "normal" classification. One clean test result is reassuring, not definitive — periodic reassessment matters.
Myth 4: "Supplements that target amyloid or 'cellular cleanup' are proven brain protectors." Reality: Much of the proteostasis and neurogenesis research is still in cell and animal models. Be wary of any product claiming to leverage these specific 2025–2026 discoveries — that's marketing running far ahead of the clinical evidence.
Myth 5: "Only intense cognitive specialists' tests can detect early decline." Reality: While comprehensive neuropsychological batteries are the gold standard, even composite scores from accessible measures have demonstrated meaningful predictive value for dementia conversion risk in MCI patients in recent cohort research — making early evaluation more accessible than many assume.
Frequently Asked Questions
1. At what age does cognitive decline typically begin? Subtle changes in processing speed can begin as early as the 30s-40s for some measures, but clinically meaningful decline in memory and executive function typically becomes more apparent from the 60s onward — and even then, trajectories vary enormously between individuals.
2. Can exercise actually reverse cognitive decline, or just slow it? Current human evidence supports exercise primarily as a way to slow decline and reduce dementia risk, rather than reverse established damage. Animal mechanism studies suggest plausible biological pathways (like enhanced amyloid clearance via muscle-to-microglia signaling) that could eventually support more targeted interventions, but reversal in humans isn't established yet.
3. Is memory loss with age always a sign of Alzheimer's disease? No. Many causes of memory complaints in older adults are non-Alzheimer's — including normal aging, depression, sleep disorders, thyroid dysfunction, medication side effects, and other medical conditions. A comprehensive evaluation is the only way to distinguish these.
4. What is "cognitive reserve" and can I build it later in life? Cognitive reserve is the brain's capacity to maintain function despite accumulating pathology, built through education, occupational complexity, and engagement. Evidence suggests it remains buildable later in life through sustained novel learning and socially complex activity, not just early-life education.
5. Are SuperAgers just genetically lucky, or can their traits be cultivated? Likely both. SuperAgers show distinct biological features (like preserved hippocampal neurogenesis markers), and while genetics likely play a role, the lifestyle and cognitive engagement patterns common in this group are largely replicable behaviors.
6. How predictive are memory tests for future dementia risk? A 2026 study following 349 MCI patients for three years found that composite neuropsychological scores carried meaningful predictive value for who would progress to dementia, though no single test is perfectly predictive — risk stratification works best combining multiple measures over time.
7. Does the COVID-19 pandemic appear to have affected cognitive aging trends? Researchers examining a decade of clinic data (2013–2022) specifically built pandemic-era assessment into their analysis given concerns about isolation and reduced activity during that period; this remains an active area of investigation rather than a fully settled question.
8. Should I take supplements marketed for "neurogenesis" or "brain cell renewal"? Be cautious. The neurogenesis and proteostasis research generating these marketing claims is largely based on postmortem tissue analysis or animal models, not clinical trials proving a supplement restores these processes in living humans.
9. What's the single most evidence-backed action for brain health? If forced to choose one, regular aerobic exercise has the broadest, most consistent human evidence base across decades of cohort studies, now reinforced by emerging mechanistic data explaining plausible biological pathways.
10. How often should I get cognitive function tested as I age? There's no universal protocol, but given evidence that decline can occur even within "normal" classifications, many clinicians now favor a baseline assessment in the 50s–60s with periodic reassessment every few years, more frequently if risk factors or symptoms emerge.
11. Does bilingualism or learning a new language really help? Substantial epidemiological evidence links bilingualism and active language learning to greater cognitive reserve and, in several studies, delayed dementia symptom onset, likely through the sustained cognitive demand involved.
12. Is there a genetic test that tells me my dementia risk? APOE4 genotype testing can indicate elevated statistical risk for Alzheimer's disease, but it is not diagnostic — many APOE4 carriers never develop dementia, and many non-carriers do. Genetic counseling is recommended before pursuing this testing.
Conclusion: Your Action Plan
The clearest message from the 2025–2026 wave of cognitive aging research is this: your brain's future is not predetermined by your birth year. Hallmarks like hippocampal neurogenesis, protein quality control, neurovascular health, and cognitive reserve diverge sharply between individuals — and several of them respond, at least partially, to what you do consistently over years and decades.
Here's where to start this week:
Schedule a baseline cognitive check-in with your physician, especially if you're over 55 or have a family history of dementia.
Add two structured aerobic sessions to your weekly routine if you don't already have them — even brisk 20-minute walks count.
Pick one genuinely new, effortful skill to start learning this month — not something you're already comfortable with.
Get your blood pressure, blood sugar, and cholesterol checked if it's been over a year, and treat any abnormalities as brain health priorities, not just heart health ones.
Protect your sleep — treat seven-plus consistent hours as non-negotiable, and get evaluated for sleep apnea if you snore heavily or wake unrefreshed.
None of this guarantees SuperAger status. But the evidence is genuinely clear that these are the levers most strongly associated with staying on the resilient end of the cognitive aging spectrum — and unlike the molecular mechanisms still being mapped in labs, you can act on every one of them today.
You can place this immediately before the conclusion section.
Author's Note: A Clinician's Perspective
As a physician, one of the most common concerns I hear from older adults is, “Doctor, am I developing dementia?” Often, the trigger is a forgotten name, a misplaced set of keys, or difficulty recalling a recent conversation. While these experiences can be unsettling, they do not automatically indicate Alzheimer's disease or another neurodegenerative condition.
What I have learned from both clinical practice and the scientific literature is that cognitive aging is far more individualized than most people realize. I have cared for patients in their 80s who remain intellectually active, socially engaged, physically independent, and cognitively sharp, while others develop significant impairment decades earlier. The difference is rarely explained by age alone.
Many of the factors that influence brain health—physical activity, sleep quality, blood pressure control, diabetes management, social engagement, and lifelong learning—are modifiable. The emerging science reviewed in this article reinforces what clinicians increasingly observe in practice: the brain remains adaptable throughout life, and healthy habits appear to strengthen resilience against age-related cognitive decline.
Perhaps the most important message is this: occasional forgetfulness is common, but progressive decline is not an inevitable consequence of aging. Early evaluation, attention to cardiovascular and metabolic health, and proactive lifestyle measures can make a meaningful difference in maintaining cognitive function and quality of life.
A Patient Example
Consider a 69-year-old retired schoolteacher who came to clinic concerned about worsening memory. She frequently misplaced household items, occasionally forgot appointments, and worried that she was developing Alzheimer's disease because her mother had dementia.
A comprehensive evaluation revealed that her cognitive testing was within the normal range for her age. However, she also had poorly controlled hypertension, untreated obstructive sleep apnea, physical inactivity, and chronic sleep deprivation.
Rather than focusing solely on memory symptoms, we addressed these underlying contributors. Over the next year, she began a structured walking program, improved her sleep habits, received treatment for sleep apnea, and achieved better blood pressure control.
At follow-up, her subjective memory complaints had significantly improved. More importantly, repeat cognitive assessments remained stable, and she reported greater confidence in her daily functioning.
While not every patient experiences such improvement, this case illustrates an important principle: many factors that affect brain performance are treatable, and preserving cognitive health often begins by addressing the foundations of overall health.
This article is for educational purposes and does not constitute medical advice. Please consult a qualified healthcare professional regarding your individual cognitive health, especially before starting new exercise programs or if you have concerns about memory or cognitive function.
Related Articles
Mitochondria, Motor Units, and Muscle Aging: A Complete Guide | DR T S DIDWAL
Can Aging Cells Cause Diabetes? The Science Behind SASP and Blood Sugar Dysfunction
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
The Science of Healthy Brain Aging: Microglia, Metabolism & Cognitive Fitness | DR T S DIDWAL
References
Abrous, D. N., Blin, N., Boraxbekk, C.-J., & Wolbers, T., et al. (2026). Hallmarks of healthy cognitive aging: Inter-individual differences in aging trajectories. Ageing Research Reviews, 119, Article 102345. https://doi.org/10.1016/j.arr.2026.102345
Lin, J., Shao, X., Shi, T., et al. (2026). Exercise alleviates cognitive dysfunction in Alzheimer's disease mice via skeletal muscle-derived extracellular vesicles that enhance plaque clearance by microglia. Nature Aging. https://doi.org/10.1038/s43587-026-01075-5
Matsui, Y., Fujisawa, C., Minakami, M., et al. (2026). The decline in cognitive function with age and its changes over time in cognitively normal older adults. European Geriatric Medicine, 17, 299–308. https://doi.org/10.1007/s41999-025-01377-8
Stanford Report / Knight Initiative for Brain Resilience (2026). Aging slows breakdown of synaptic proteins, raising disease risk. https://news.stanford.edu/stories/2026/02/aging-brains-proteins-cognitive-decline-alzheimers-research
Silva-Pereyra, J., Fernández, T., & Rodríguez-Rodríguez, V. (2026). Editorial: Mechanisms and interventions for enhancing cognitive reserve in aging populations. Frontiers in Neuroscience, 20:1830725. https://doi.org/10.3389/fnins.2026.1830725
Prince, J. B., et al. (2024). Cognitive and neuroscientific perspectives of healthy ageing. Neuroscience & Biobehavioral Reviews, Article 105649. https://doi.org/10.1016/j.neubiorev.2024.105649
Disouky, A., Sanborn, M. A., Sabitha, K. R., et al. (2026). Human hippocampal neurogenesis in adulthood, ageing and Alzheimer's disease. Nature, 652, 1264–1273. https://doi.org/10.1038/s41586-026-10169-4
Padilla, C., Zsadanyi, S. E., Aragón, I., et al. (2026). The predictive power of neuropsychological measures in MCI: early detection of dementia conversion. Frontiers in Aging Neuroscience, 18:1740033. https://doi.org/10.3389/fnagi.2026.1740033
Di Fraia, D., Marino, A., Lee, J. H., et al. (2025). Altered translation elongation contributes to key hallmarks of aging in the killifish brain. Science, 389(6759). https://doi.org/10.1126/science.adk3079
Frontiers in Aging Neuroscience (2025). Treadmill exercise alleviates Alzheimer's disease pathologies in APP/PS1 mice through modulation of microglial glucose metabolic reprogramming.
Wisdom, N. M., Mignogna, J., & Collins, R. L. (2012). Variability in Wechsler Adult Intelligence Scale-IV subtest performance across age. Archives of Clinical Neuropsychology, 27(4), 389–397.
Harada, C. N., Natelson Love, M. C., & Triebel, K. (2013). Normal cognitive aging. Clinics in Geriatric Medicine, 29, 737–752.
Livingston, G., et al. (Lancet Commission). Dementia prevention, intervention, and care. The Lancet.
World Health Organization. Physical activity guidelines for adults and older adults.
Alzheimer's Association. Mild cognitive impairment (MCI) overview and diagnostic criteria.
National Institute on Aging. Cognitive health and older adults.
Stern, Y. (2012). Cognitive reserve in ageing and Alzheimer's disease. The Lancet Neurology.
Petersen, R. C. (2016). Mild cognitive impairment. Continuum (Minneapolis, Minn.), 22(2 Dementia), 404–418.
Moreno-Jiménez, E. P., et al. (2019). Adult hippocampal neurogenesis is abundant in neurologically healthy subjects and drops sharply in patients with Alzheimer's disease. Nature Medicine, 25, 554–560.
Schmauck-Medina, T., Molière, A., Lautrup, S., et al. (2022). New hallmarks of ageing: a 2022 Copenhagen ageing meeting summary. Aging (Albany NY). https://doi.org/10.18632/aging.204248