Your Body Clock Could Be Increasing Your Heart Disease Risk—Here's What Research Shows
Scientists now believe circadian rhythm may be one of the most overlooked factors in heart health. Learn how your body's internal clock influences cardiovascular disease risk.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/25/202624 min read
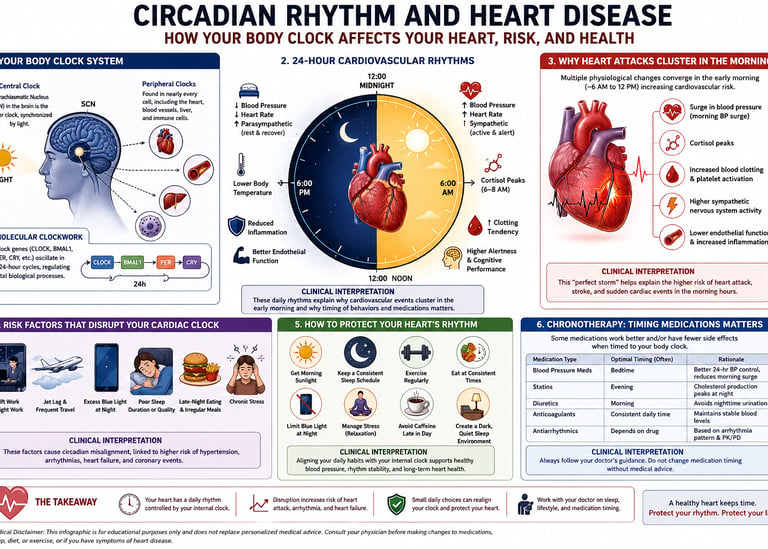
Heart attacks occur roughly three times more often between 6:00 AM and noon than in the late evening. This dangerous window is driven by your body’s circadian rhythm (internal clock), which triggers a sharp morning surge of cortisol and adrenaline. This natural transition causes blood pressure and heart rate to spike while simultaneously increasing platelet aggregation (blood clotting tendency), putting maximum stress on the cardiovascular system immediately after waking.
Key Takeaways
The Morning Surge is a Physiological Reality: Heart attacks are roughly three times more common between 6:00 AM and noon than in the late evening. This is driven by a coordinated, master-clock-controlled morning surge of cortisol and adrenaline that simultaneously spikes blood pressure, heart rate, and platelet stickiness (clotting tendency).
The Midnight-to-Dawn Window Amplifies Tissue Damage: While fewer heart attacks occur in the dead of night, those starting between midnight and 6:00 AM frequently result in the largest structural damage (infarct size). Underlying heart tissue is less tolerant to oxygen deprivation overnight, increasing the 1-year risk of heart failure rehospitalization by 30% to 50% if blood flow isn't restored within 120 minutes.
Animal Models Prove Structure, Not Function: A rigorous 2026 meta-analysis reveals that chronic circadian disruption definitely causes structural heart enlargement (cardiac hypertrophy, rated high certainty). However, claims that it directly destroys heart pumping function (ejection fraction) or ruins blood vessel dilation remain directionally concerning but are still graded as low-certainty science.
"Non-Dipping" Hypertension Wreckages the Heart: A healthy circadian clock forces blood pressure to drop by 10% to 20% overnight to allow the vascular system to rest. If your blood pressure stays flat at night ("non-dipping") or rises ("reversed dipping"), this unremitting mechanical stress significantly worsens the prognosis for hypertension and heart failure.
Arrhythmias Have Unique Day vs. Night Profiles: The time your heart goes out of rhythm points directly to different triggers. Atrial Fibrillation (AF) that strikes at night is usually "vagally mediated" (driven by the rest-and-digest system and highly linked to sleep apnea), whereas daytime AF is typically "adrenergic" (triggered by stress, exertion, and adrenaline surges).
Shift Work Carries a Quantified Cardiovascular Toll: Chronic nighttime shift work is not just an inconvenience; it is a major independent cardiovascular risk factor. The data associates routine night shifts with a 15% increased risk of cardiovascular mortality, a 23% increase in heart attacks, and a 31% higher risk of developing high blood pressure.
Cardiovascular Resilience is an Active Asset: Sleep and circadian alignment are no longer viewed merely as passive recovery phases. Landmark roadmaps position a well-regulated internal clock as an active engine of cardiovascular resilience—a modifiable defense mechanism that helps the heart withstand and bounce back from acute physical stress.
Chronotherapy Requires Precise Physician Guidance: Timing medications (like taking blood pressure pills at night or beta-blockers to blunt the morning surge) can drastically improve their efficacy. However, you should never alter your dosing schedule on your own; incorrect timing can leave you completely unprotected during peak-risk morning hours.
1. What Is the Circadian Rhythm? A Quick Primer
Your circadian rhythm is an internally generated, roughly 24-hour cycle that governs nearly every biological process in your body — sleep, hormone release, body temperature, digestion, and, critically, your cardiovascular function.
This system has two levels:
The central clock: Located in the suprachiasmatic nucleus (SCN), a tiny region of your brain's hypothalamus, this "master clock" takes its cues primarily from light hitting your retina.
Peripheral clocks: Nearly every cell in your body — including heart muscle cells, blood vessel walls, and immune cells — contains its own molecular clock. The SCN keeps these peripheral clocks synchronized using nerve signals, hormones, and behavioral cues like sleep, meal timing, and physical activity.
At the molecular level, this rhythm is generated by a feedback loop of "clock genes" — proteins with names like CLOCK, BMAL1, PER, and CRY — that switch each other on and off in a roughly 24-hour cycle, according to the foundational biology described in the European Heart Journal review. This oscillation drives daily fluctuations in things like myocardial contractility (how forcefully your heart squeezes) and endothelial function (how well your blood vessels dilate and constrict).
Key terms you'll see throughout this article:
Circadian Rhythm: A foundational ~24-hour internal biological cycle calibrated by light and dark cues. It dictates the daily peaks and drops in your blood pressure, heart rate, and clotting factors.
Central Clock (SCN): The brain’s master pacemaker, located in the hypothalamus and synchronized by daylight. It acts as the primary conductor, sending hormonal and neural signals to keep all bodily systems on the same schedule.
Peripheral Clocks: Local cellular timekeepers embedded directly inside organs like the heart, liver, and blood vessels. They dictate local organ functions, such as how forcefully your heart muscle squeezes across the 24-hour day.
Chronotype: Your natural, genetically influenced preference for morning activity ("morning lark") or evening activity ("night owl"). Night owls often suffer higher rates of cardiovascular stress due to early morning social and work schedules.
Circadian Misalignment: A state where your internal clock is forced out of sync with your actual behavior, such as during shift work or erratic eating patterns. This mismatch acts as a chronic physiological stressor, raising your risk for heart failure and stroke.
Chronotherapy: The clinical practice of timing medical treatments to match your natural biological peaks. Strategic timing of specific heart or blood pressure medications can maximize their effectiveness and shield you during high-risk morning hours.
2. How Your Internal Clock Controls Your Cardiovascular System
Here's the part most people never learn: your autonomic nervous system flips a daily switch that directly drives cardiovascular risk patterns.
During sleep, your parasympathetic ("rest and digest") nervous system dominates. This lowers your heart rate and blood pressure and reduces vascular resistance, allowing your cardiovascular system genuine recovery time. Come morning, the sympathetic ("fight or flight") system takes over — heart rate climbs, blood pressure rises, and your body gears up for the demands of being awake and active.
This transition from sleep to wakefulness is exactly when trouble tends to start. According to the European Heart Journal review, the early-morning sympathetic surge coincides with measurable jumps in:
Blood pressure
Platelet aggregation (clotting tendency)
Catecholamine levels (adrenaline-type stress hormones)
Myocardial oxygen demand
Why this matters clinically: This isn't a minor statistical quirk — it's the physiological explanation for one of cardiology's most replicated findings. Multiple studies cited in the review found that heart attacks occur roughly three times more often in the morning than in the late evening, and ST-elevation myocardial infarction (STEMI, the most severe type of heart attack) was about 10% more common in the morning than in the afternoon or night.
Heart rate variability (HRV) — a measure doctors use to assess how well your autonomic nervous system is balancing these two branches — follows this same daily rhythm, shaped by both the central SCN clock and local peripheral clocks in your heart and vessels.
3. The Evidence: Circadian Rhythms and Specific Heart Conditions
This is where the science gets clinically actionable. Let's break it down by condition.
3.1 Heart Attacks (Myocardial Infarction)
The pattern: Heart attacks cluster in the morning hours, driven by the convergence of higher blood pressure, increased platelet aggregation, and elevated sympathetic tone right after waking.
What affects severity, not just timing:
A pooled analysis of four randomized trials found the largest heart attack damage (infarct size) occurred in people whose symptoms began between midnight and 6 a.m.
A separate study using cardiac imaging found the worst outcomes — biggest infarcts and weakest heart pumping function — in heart attacks starting between 6 a.m. and noon, a finding later confirmed in an analysis of 1,031 STEMI patients.
Late evening or early morning symptom onset increased the one-year risk of being re-hospitalized for heart failure by 30–50%, particularly when the period of reduced blood flow (ischemia) lasted longer than 120 minutes.
Night-onset STEMI was linked to higher mortality in at least one study, and early-morning symptom onset was associated with larger infarcts and higher 30-day mortality.
Clinical interpretation: These findings matter because time of symptom onset is a piece of prognostic information your care team can use — alongside standard risk markers — when assessing how aggressively to monitor and treat a patient. They also strengthen the case for why minimizing ischemic time (time from symptom onset to treatment) is especially critical during overnight and early-morning hours, when underlying tissue tolerance to oxygen deprivation may already be working against the patient.
An important caveat: Not every study agrees on the exact time window of worst risk, and the EHJ review's authors note explicitly that these differences "may reflect variations in study design, population characteristics, or definitions of time windows." The general direction — overnight/early-morning onset is worse — is consistent, but precise hour-by-hour conclusions should be interpreted cautiously.
3.2 Daylight Saving Time Transitions
One of the clearest natural experiments in circadian cardiology: the spring "spring forward" time change.
MI incidence rises in the week following the spring transition, with an increase specifically in non-STEMI cases.
This elevated risk persists for up to three weeks after the clock change, with a more pronounced effect in women, a finding a subsequent meta-analysis supported.
The autumn "fall back" transition shows no consistent increase or decrease in MI incidence.
Clinical interpretation: This is a textbook demonstration of acute circadian misalignment translating into measurable cardiovascular harm in a real-world population — not a lab mouse, not a hypothesis, but documented hospital admission data. If you have existing cardiovascular risk factors, treating the week of a clock change like a higher-vigilance period (prioritizing sleep, moderating stimulants, not skipping medications) is a reasonable, low-cost precaution.
3.3 Heart Failure
In heart failure, the circadian system doesn't shut off — it gets dampened but stays partially intact, according to the EHJ review's analysis of melatonin and cortisol rhythms in heart failure patients. This is clinically important: a damped rhythm is still a rhythm doctors can potentially work with therapeutically.
Key findings:
Reduced ability of the time-of-day fluctuations normally seen in cardiac contractility and electrical activity, linked to altered neurohormonal rhythms.
Elevated nighttime heart rate and blood pressure (a "non-dipping" pattern) increases arrhythmia risk.
Sleep deprivation — common in heart failure patients — worsens the condition through increased sympathetic activity and inflammation.
Insomnia, obstructive sleep apnea, shift work, and non-dipping hypertension all independently worsen heart failure outcomes.
A genuinely useful diagnostic advance: A deep learning model analyzing 24-hour ECG heart rate variability data achieved 92.6% accuracy, 90.7% sensitivity, and 95.2% specificity for diagnosing heart failure with preserved ejection fraction (HFpEF) — a notoriously hard-to-diagnose condition. This shows that the daily pattern itself — not just a single snapshot measurement — carries diagnostic value.
Clinical interpretation: This is the strongest argument in the entire body of evidence for moving away from single-point measurements (one blood pressure reading, one ejection fraction) toward 24-hour monitoring approaches in heart failure care. Persistent circadian misalignment — a blunted day-night variation in BP and HR — "significantly worsens prognosis" according to the EHJ review, meaning the pattern of your numbers across the day may carry as much prognostic weight as the numbers themselves.
3.4 Arrhythmias: Ventricular Arrhythmias and Atrial Fibrillation
This is where the morning/night split becomes most dramatic — and most useful for understanding your personal risk pattern.
Ventricular arrhythmias and sudden cardiac death:
Peak incidence occurs in the morning, between 7 a.m. and noon, mirroring sudden cardiac death patterns.
The mechanism involves the morning cortisol surge increasing expression of specific ion channel proteins (Scn5a, Kcnh2) that alter the heart's electrical properties, making arrhythmias more likely during the active phase.
Beta-blockers, which blunt the morning sympathetic surge, attenuate this pattern — one of the clearest examples of circadian biology directly informing why a specific drug class works.
People with chronic kidney disease or diabetes show an attenuated version of this morning pattern, an important nuance for risk-stratifying patients with these comorbidities.
Conditions like obstructive sleep apnea, Brugada syndrome, and early repolarization syndrome flip the pattern: their dangerous ventricular arrhythmias tend to occur at night, linked to the elevated nighttime sympathetic activity these conditions paradoxically produce.
Atrial fibrillation (AF):
AF is more biologically complex than ventricular arrhythmias — it can be triggered from either direction of the autonomic nervous system:
A subset of patients have AF that comes on almost exclusively at night, likely driven by vagal (parasympathetic) tone shortening the heart's electrical refractory period.
AF during the day is more often triggered by adrenergic surges — physical exertion or emotional stress.
A periodicity analysis of 2,080 patients with 11,886 AF onset events across 14 studies confirmed a statistically significant 24-hour rhythm to AF onset (cosine-fit R² = 0.77, p = 0.03).
Sleep apnea independently worsens nighttime AF risk through intermittent oxygen drops and sympathetic bursts.
Clinical interpretation: Because AF can be triggered by both nighttime vagal surges and daytime sympathetic surges, the time your AF episodes occur is a genuinely useful piece of clinical information. If your AF consistently strikes at night, your physician may consider vagally-mediated triggers (and ask about sleep apnea); if it consistently strikes during exertion or stress, an adrenergic mechanism is more likely — and these can call for different management approaches.
3.5 Cardiac Diagnostics: Why Time-of-Day Matters for Your Lab Results
This is an underappreciated but practically important finding: not every cardiac biomarker behaves the same way across the clock.
Troponin-I (used to diagnose heart attacks) shows no significant diurnal fluctuation — its diagnostic accuracy is stable no matter what time you're tested.
Troponin-T, by contrast, gradually declines through the day and rises overnight, peaking in the early morning. While this doesn't change its accuracy for diagnosing a heart attack, it can affect how doctors interpret the size of a change in troponin level within the first hour of presentation, especially outside of suspected-MI settings.
Clinical interpretation: This is a clear example of why "interpreting the result" matters as much as the number itself. The same troponin-T value might mean something different at 6 a.m. versus 6 p.m. — a nuance your lab and clinician should already be factoring into urgent decision-making, and one more reason not to self-interpret lab values without clinical context.
4. Mechanistic Evidence From Animal Models: What We Actually Know (and How Confident We Can Be)
Most of what's described above comes from observational human data — it tells us what happens and when, but not always why at the cellular level. To understand mechanism, researchers turn to animal models, where genes and environmental exposures can be manipulated directly.
A rigorous 2026 systematic review and meta-analysis in BMC Medicine pooled data from 34 studies (32 retained after quality screening) using genetic clock-gene knockout models and environmental disruption models (light phase shifts, sleep deprivation/fragmentation) in rodents and other mammals. This is the most methodologically careful synthesis of mechanistic circadian-cardiovascular evidence to date, using GRADE-style certainty ratings — the same framework used to grade evidence in major clinical guidelines.
Here's what the evidence actually supports
High-certainty finding: Cardiac hypertrophy
Circadian disruption significantly increased the left ventricular mass-to-body-weight ratio (a marker of pathological heart enlargement),
Moderate-certainty finding: Cardiomyocyte enlargement
Individual heart muscle cells were larger following circadian disruption across multiple independent model types (genetic knockouts and environmental jet-lag models), supported by elevated natriuretic peptides (ANP, BNP) and pro-fibrotic markers — biological signatures consistent with the heart trying (and struggling) to compensate for an abnormal workload.
Low-certainty findings (real signal, but interpret cautiously)
Reduced systolic function: Ejection fraction dropped significantly
Impaired blood vessel dilation (endothelium-dependent vasorelaxation):
Elevated triglycerides:
What this graded approach tells you, clinically
This is the single most important interpretive point in the entire mechanistic literature: not all circadian-cardiovascular claims are equally well-supported. Cardiac hypertrophy is a robust, well-replicated, low-heterogeneity finding you can treat as solid science. Effects on contractile function and vascular relaxation are directionally concerning but statistically noisier — promising leads for future research, not settled facts to build clinical decisions on yet.
5. Clinical Interpretation: What This Means For You and Your Doctor
Pulling the threads together, here's how clinicians and researchers are translating circadian biology into practice — and what questions are still open.
What's already changing in clinical recommendations
The European Heart Journal review proposes a specific set of clinical care recommendations, including:
Recording the time of day for interventions, drug administration, and lab measurements — not just the result itself.
Using 24-hour ambulatory blood pressure and heart rate monitoring for cardiovascular risk assessment, rather than relying solely on single clinic readings.
Minimizing disruption of sleep and daily rhythms for hospitalized patients — an often-overlooked aspect of inpatient care.
Considering nocturnal blood pressure "dipping" patterns (whether BP normally falls at night) as a prognostic marker, since abnormal patterns — "non-dippers" and "risers" — are associated with worse outcomes in both young hypertensive patients and acute heart failure.
What is genuinely uncertain or still being established
Being transparent about limitations is part of good evidence-based guidance:
Clinical evidence on circadian biology in heart attacks remains observational, not mechanistic. The EHJ review notes directly that most human MI studies describe time-of-day patterns rather than proving the underlying circadian mechanism driving them — an important distinction for interpreting causality.
The optimal time for elective cardiac surgery is unresolved: one randomized study found that afternoon aortic valve surgery caused less myocardial injury, but several other studies found no timing effect for either aortic valve replacement or coronary bypass surgery.
Donor heart procurement timing in transplantation shows an association (early-morning procurement linked to better long-term survival) but is heavily confounded by surgeon fatigue, logistics, and scheduling factors that are nearly impossible to fully separate from biology.
Time-of-day-adjusted "normal ranges" for cardiac biomarkers don't yet exist in routine clinical practice — the EHJ authors list this explicitly as a future research priority, not a current standard.
The bigger picture: cardiovascular resilience
A parallel and complementary framework comes from a National Heart, Lung, and Blood Institute workshop, published as a 2025 roadmap in Nature Reviews Cardiology. Rather than only asking how circadian disruption causes disease, this roadmap reframes the question: how does healthy, well-aligned sleep and circadian function actively build cardiovascular resilience — the capacity to withstand and recover from cardiovascular stress?
This is a meaningful shift in framing. It positions circadian and sleep health not just as a risk factor to manage, but as a protective resource you can actively build, alongside traditional pillars like diet, exercise, and not smoking — echoed in the American Heart Association's "Life's Essential 8" framework for cardiovascular health.
Clinical interpretation, in plain terms: Your cardiologist isn't going to start prescribing "go to bed earlier" as a substitute for your statin or blood pressure medication. But circadian health is increasingly being recognized as a legitimate, modifiable contributor to cardiovascular risk — one that sits alongside, not beneath, the traditional risk factors you already know about.
6. Risk Factors That Disrupt Your Cardiac Clock
Several overlapping factors interact with your circadian system to elevate cardiovascular risk:
Shift work
This is the most extensively studied real-world circadian disruptor, and the data is sobering:
Night shift work is associated with a 15% increased risk of cardiovascular mortality, per a meta-analysis of cohort studies referenced in the BMC Medicine review.
Shift workers show a 23% increased risk of myocardial infarction and a 24% increased risk of coronary events compared to non-shift workers.
Shift work is linked to a 31% greater risk of hypertension in cohort studies (10% higher risk in cross-sectional studies).
Chronotype (morning vs. evening preference)
Evening chronotypes — people who naturally prefer staying up late and waking late — show greater susceptibility to sleep-related issues, unhealthy lifestyle habits, and metabolic disturbances linked to cardiovascular risk. Notably, women with an evening chronotype appear especially susceptible to sleep disruption and its downstream health consequences.
Obstructive sleep apnea (OSAS)
OSAS creates a uniquely disruptive nighttime physiology: intermittent oxygen drops paired with sympathetic nervous system bursts. This combination independently worsens heart failure, increases nighttime ventricular arrhythmia risk, and raises AF susceptibility during sleep.
Comorbidities that blunt protective rhythms
Chronic kidney disease and diabetes mellitus both attenuate the normal morning peak in ventricular arrhythmia risk — not necessarily a good thing, since it suggests these conditions disrupt the body's underlying circadian regulation of cardiac electrical stability rather than simply shifting it to a safer time.
Light exposure and irregular meal timing
Both are flagged repeatedly across the literature as circadian disruptors that impair "molecular clock pathways," increasing risk of hypertension, atherosclerosis, and arrhythmias.
7. Practical Application: How to Protect Your Heart's Rhythm
Translating the evidence into action. None of this replaces medical treatment for existing heart disease — think of it as the modifiable layer underneath your medical care.
A Daily Circadian Heart-Health Checklist
[ ] Get bright light exposure within an hour of waking — outdoor light if possible, even on cloudy days. This is the strongest signal your SCN uses to anchor your daily rhythm.
[ ] Keep a consistent wake time, including weekends. Variable wake times are a form of self-imposed jet lag.
[ ] Dim lights and avoid bright screens for 1–2 hours before bed. Evening light exposure delays your internal clock and pushes back the protective parasympathetic shift that should happen at sleep onset.
[ ] Eat your meals within a consistent daily window. Irregular meal timing is repeatedly flagged as a circadian disruptor in the cardiovascular literature.
[ ] Prioritize 7–9 hours of sleep, not just "enough to function." Sleep deprivation directly increases sympathetic activity and inflammation — two pathways implicated throughout this article.
[ ] If you take morning blood pressure or heart medications, take them at a consistent time daily. Consistency itself supports the chronotherapy principle discussed below.
[ ] Be cautious during daylight saving transitions. Prioritize sleep and avoid scheduling elective stressful events in the week after the spring "spring forward" shift.
[ ] If you work night shifts, ask your physician about more frequent cardiovascular risk screening — shift work carries a measurable, quantified increase in cardiovascular risk, not a hypothetical one.
[ ] Get evaluated for sleep apnea if you snore heavily, wake gasping, or have unexplained daytime fatigue — especially if you also have nighttime arrhythmias or treatment-resistant hypertension.
[ ] Ask your doctor about 24-hour ambulatory blood pressure monitoring if you have hypertension, rather than relying solely on single clinic readings — this is one of the clearest practical applications of circadian cardiology already available today.
For Shift Workers Specifically
Shift work is one of the few circadian disruptors with hard quantified cardiovascular risk data behind it, so it deserves dedicated strategy:
Anchor sleep, even if total hours are reduced, rather than sleeping in fragmented, unpredictable blocks.
Use bright light strategically during night shifts (to support alertness) and wear sunglasses on the commute home (to avoid signaling "daytime" to your brain right before you try to sleep).
Discuss cardiovascular screening frequency with your doctor, given the documented 15–24% relative risk increases in cardiovascular mortality, MI, and coronary events associated with shift work.
Don't ignore new palpitations, chest discomfort, or unusual fatigue — given the measurable excess risk, a lower threshold for medical evaluation is reasonable.
8. Chronotherapy: Timing Medications for Maximum Benefit
Chronotherapy is the practice of timing medical treatments to align with the body's circadian rhythms, with the goal of improving effectiveness, reducing side effects, or both. This is one of the more clinically exciting and directly actionable areas of circadian cardiology.
Where the evidence currently points
Beta-blockers enhance heart rate variability by suppressing sympathetic activity, providing the most benefit during the high-risk early morning hours when sympathetic surges would otherwise spike arrhythmia risk.
ACE inhibitors have been shown to restore circadian blood pressure variability, improving clinical status in congestive heart failure.
SGLT2 inhibitors (a newer heart failure drug class) improve cardiac autonomic function, reducing both daytime and nighttime heart rate while enhancing parasympathetic modulation — potentially helping normalize circadian rhythm itself, not just treating a single number.
Digoxin reduces sympathetic activity specifically during sleep, modulating nighttime blood pressure and parasympathetic function.
Anticoagulation and antihypertensive chronotherapy more broadly "has shown promise in improving the effectiveness" of these drug classes, according to the EHJ review — though the strength of evidence varies by drug and condition.
An important caution
Beta-blockers may suppress melatonin production. While melatonin supplementation has been explored for sleep quality in patients taking beta-blockers, the EHJ review is explicit that there is currently limited evidence on its clinical cardiovascular benefit in this specific population. This is a good example of where popular supplement advice outpaces actual clinical evidence — don't start melatonin to counteract a medication side effect without discussing it with your prescriber first.
Bottom line on chronotherapy: This is a genuinely promising and partly already-implemented area of cardiology, but it is not a green light for self-adjusting when you take prescribed medications. The timing effects described above were studied under specific protocols; changing your own medication schedule without medical guidance could affect both efficacy and safety. Talk to your prescriber about whether timing adjustments are appropriate for your specific regimen.
9. Evidence Summary Tables
1. Circadian Patterns in Major Cardiovascular Conditions (Human Data)
General Heart Attacks (Myocardial Infarction): Occur roughly three times more often in the morning than in the late evening, driven by a simultaneous spike in blood pressure, heart rate (sympathetic surge), and blood stickiness (platelet aggregation).
Severe Heart Attacks (STEMI): Approximately 10% more common during the morning hours than during the afternoon or night.
Maximum Heart Damage (Infarct Size): Clusters between midnight and noon, driven by a natural biological drop in the heart tissue's ability to tolerate oxygen deprivation (ischemic tolerance) during overnight hours.
Sudden Cardiac Death & Ventricular Arrhythmias (VA): Peak sharply between 7:00 AM and noon due to early-morning cortisol surges that directly alter the heart's electrical ion channels.
Specialized Ventricular Arrhythmias: Conditions like Sleep Apnea (OSAS), Brugada syndrome, and early repolarization reverse the standard pattern, causing dangerous rhythms primarily at night due to abnormal nighttime sympathetic spikes.
Atrial Fibrillation (Vagally-Mediated): Strikes primarily at night when the rest-and-digest (parasympathetic) system dominates, which shortens the heart's electrical recovery period.
Atrial Fibrillation (Adrenergic): Strikes primarily during the day, triggered directly by stress, physical exertion, and adrenaline surges.
2. Mechanistic Evidence Certainty (What Animal Models Prove)
Heart Enlargement (Hypertrophy): High Certainty. Circadian disruption significantly increases the left ventricular mass-to-body-weight ratio
Heart Cell Size (Cardiomyocytes): Moderate Certainty. Individual heart muscle cells consistently enlarge across both genetic and jet-lag environmental models.
Pumping Performance (Ejection Fraction): Low Certainty. Data shows a downward trend but this finding is statistically noisy and highly dependent on removing outlier studies.
Heart Squeezing Ability (Fractional Shortening): Low Certainty. Shows a directional decrease but requires more consistent replication.
Vessel Dilation (Endothelial Function): Low Certainty. While data signals a large impairment in blood vessel relaxation (SMD: -2.72), it is based on very few, highly inconsistent studies.
Triglycerides: Low Certainty. Shows an upward trend (SMD: 1.64) but remains statistically unconfirmed as a definitive direct consequence.
3. Shift Work and Cardiovascular Risk (Human Epidemiological Data)
Cardiovascular Mortality: Chronic night shift work is associated with a 15% relative risk increase in death from cardiovascular disease.
Heart Attacks: Routine shift workers experience a 23% higher risk of acute myocardial infarction compared to standard daytime workers.
Coronary Events: Shift work drives a 24% increase in the risk of overall adverse coronary artery events.
Chronic Hypertension (Long-Term Studies): Long-term tracking data reveals a 31% relative risk increase in developing high blood pressure among shift workers.
Hypertension (Snapshot Studies): Cross-sectional data shows a more modest but highly consistent 10% increase in prevalent high blood pressure across shift-working populations.
10. Myths & Mistakes
Myth 1: "Circadian rhythm disruption is just about feeling tired."
Reality: It's a measurable, mechanistic contributor to cardiac hypertrophy, arrhythmia risk, and altered cardiovascular biomarker patterns — not simply a fatigue or mood issue.
Myth 2: "If I take melatonin, I'll protect my heart from circadian disruption."
Reality: The evidence on melatonin's clinical cardiovascular benefit — especially in patients on beta-blockers — is explicitly described in the literature as limited. Melatonin is not a validated cardioprotective intervention; treat it as a sleep aid to discuss with your doctor, not a heart-protection supplement.
Myth 3: "Heart attacks happening more in the morning means I should worry every morning."
Reality: The morning peak is a population-level statistical pattern, not a personal daily alarm. It's most relevant for understanding why certain medications (like beta-blockers) are timed the way they are, and for recognizing symptoms promptly if they occur — not for generating daily anxiety.
Myth 4: "Animal studies on clock genes directly translate to human treatment advice."
Reality: The BMC Medicine meta-analysis is explicit that genetic knockout models and environmental (shift-work-like) models don't always show the same effects — and most humans experience the environmental type. High-certainty findings (like cardiac hypertrophy) are more trustworthy than low-certainty ones (like vascular relaxation effects), and none of this evidence currently changes individual treatment without a doctor's involvement.
Myth 5: "Daylight saving time is a minor inconvenience, not a real health issue."
Reality: Multiple independent studies, plus a supporting meta-analysis, document increased MI incidence for up to three weeks after the spring transition. This is one of the better-replicated findings in the entire field.
Myth 6: "My single blood pressure reading at the doctor's office tells my doctor everything they need to know."
Reality: Non-dipping or "riser" blood pressure patterns (where BP doesn't fall normally at night) are independently associated with worse cardiovascular outcomes — information a single daytime reading cannot capture. This is part of why 24-hour ambulatory monitoring is increasingly emphasized.
11. Frequently Asked Questions
1. What is the circadian rhythm's effect on the heart? The circadian rhythm controls daily fluctuations in blood pressure, heart rate, clotting tendency, and electrical stability of the heart. It explains why heart attacks, dangerous arrhythmias, and sudden cardiac death cluster in the early morning hours, while certain types of atrial fibrillation cluster at night.
2. Why do heart attacks happen more in the morning? The transition from sleep to wakefulness triggers a surge in sympathetic nervous system activity, raising blood pressure, increasing platelet aggregation (clotting tendency), and elevating catecholamine (stress hormone) levels — a combination that increases the likelihood of a blood clot blocking a coronary artery. Studies show heart attacks occur about three times more often in the morning than in the late evening.
3. Can poor sleep cause heart disease? Poor sleep and circadian disruption are associated with increased cardiovascular risk through several mechanisms, including increased sympathetic nervous system activity, inflammation, and — in heart failure patients specifically — worsening of existing disease. Shift work, which severely disrupts circadian alignment, is associated with measurably higher rates of cardiovascular mortality, myocardial infarction, and hypertension in large meta-analyses.
4. Does shift work really increase heart attack risk? Yes, according to published meta-analyses of cohort studies. Shift workers show a 23% increased risk of myocardial infarction and a 24% increased risk of coronary events compared to non-shift workers, along with a 15% increase in cardiovascular mortality risk.
5. What is chronotherapy, and should I time my medications differently? Chronotherapy is the practice of timing treatments to align with circadian biology — for example, taking certain blood pressure medications to coincide with periods of highest cardiovascular risk. Some evidence supports this approach for beta-blockers, ACE inhibitors, and anticoagulants. However, you should never change your medication timing without first discussing it with your prescribing physician, since studies tested specific protocols that may not generalize to your situation.
6. Is atrial fibrillation linked to time of day? Yes, but in a more complex way than heart attacks. Some patients have AF that occurs almost exclusively at night, likely driven by nighttime vagal (parasympathetic) nervous system tone. Other patients experience AF during the day, often triggered by physical exertion or emotional stress through adrenergic (sympathetic) pathways.
7. Does daylight saving time actually affect heart attack rates? Multiple studies and a supporting meta-analysis found increased heart attack incidence — specifically non-STEMI heart attacks — in the weeks following the spring "spring forward" transition, with effects lasting up to three weeks and a more pronounced impact in women. The autumn "fall back" transition has not shown the same consistent effect.
8. What is a "non-dipping" blood pressure pattern, and why does it matter? Normally, blood pressure drops at night during sleep (called "dipping"). A "non-dipper" or "riser" pattern — where blood pressure stays elevated or even rises at night — is associated with worse cardiovascular outcomes, including in heart failure and in young hypertensive patients. This is part of why doctors increasingly use 24-hour ambulatory blood pressure monitoring rather than single office readings.
9. Can circadian rhythm disruption cause heart failure, or does it just make existing heart failure worse? Current evidence suggests both. Circadian clocks regulate processes relevant to heart failure development, including heart rate, blood pressure, contractility, and inflammation. In animal models, circadian disruption produces cardiac hypertrophy and structural remodeling consistent with early heart failure development. In people who already have heart failure, circadian misalignment — including sleep deprivation, sleep apnea, and abnormal blood pressure patterns — independently worsens the condition and prognosis.
10. Is melatonin good for heart health? Melatonin plays a role in regulating circadian rhythms, but current clinical evidence for its direct cardiovascular benefit is limited — particularly in patients taking beta-blockers, where it's been studied mainly for sleep quality rather than proven cardiac outcomes. Don't substitute melatonin for prescribed cardiovascular medication or treat it as a validated heart-protective supplement without medical guidance.
11. What's the difference between a "morning person" and "evening person" in terms of heart disease risk? Evening chronotypes (people who naturally prefer later sleep and wake times) show greater susceptibility to sleep-related issues, unhealthy lifestyle patterns, and metabolic disturbances linked to cardiovascular risk, with women showing particular susceptibility to related sleep disruption. This doesn't mean being a night owl guarantees heart problems — it's a risk modifier, not a diagnosis.
12. How confident are scientists that circadian disruption actually causes cardiovascular disease, rather than just correlating with it? Confidence varies by specific outcome. A 2026 systematic review grades cardiac hypertrophy from animal studies as high-certainty evidence — a well-replicated, low-heterogeneity finding. Other outcomes, like impaired blood vessel relaxation, are rated low-certainty due to limited studies and high variability between them. In humans, most heart attack timing data is observational, meaning it shows a strong association but hasn't fully proven the precise underlying circadian mechanism in each case.
12. Conclusion & Action Steps
Your heart runs on a 24-hour clock just as much as your sleep does — and the clinical evidence now makes that connection impossible to ignore. Heart attacks cluster in the morning. Certain arrhythmias prefer the night. Heart failure prognosis tracks with how well your blood pressure and heart rate rhythms hold their normal daily shape. And in animal models, disrupting the circadian clock reliably produces real, measurable cardiac hypertrophy — one of the most consistent, high-certainty findings in this entire field.
None of this means your daily schedule is destiny. It means circadian health belongs on the same list as diet, exercise, and not smoking — a modifiable contributor to your cardiovascular risk, not a fixed sentence.
Your next steps:
Anchor your sleep and light exposure using the daily checklist above — this is the lowest-cost, evidence-backed intervention available to everyone.
If you work night shifts, talk to your doctor about more frequent cardiovascular screening, given the documented relative risk increases.
If you have hypertension or heart failure, ask whether 24-hour ambulatory blood pressure monitoring is appropriate for you — it captures circadian patterns a single office reading cannot.
Never adjust medication timing on your own based on chronotherapy research — bring it up with your prescriber as a conversation, not a self-directed change.
Pay attention to symptom timing. If you notice your palpitations, chest discomfort, or other symptoms cluster at a particular time of day, mention this specifically to your doctor — it's clinically meaningful information, not a coincidence to dismiss.
If you found this guide useful, consider sharing it with someone who works night shifts, has been recently diagnosed with a heart condition, or simply needs a science-backed reason to take their sleep schedule seriously.
Related Articles
How Many Hours of Sleep Are Best for Your Heart? New Research Says Timing Matters Too
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWA
References
Kelters, I. R., Koop, Y., Young, M. E., Daiber, A., & van Laake, L. W. (2025). Circadian rhythms in cardiovascular disease. European Heart Journal, 46(36), 3532–3545. https://doi.org/10.1093/eurheartj/ehaf367
Das, M. K., De Ryck, E., Jorgensen, I. L., Zienolddiny-Narui, S., & Erdem, J. S. (2026). Circadian rhythm disruption in cardiovascular disease: a systematic review and meta-analysis of mechanistic evidence from animal models. BMC Medicine, 24(1), 73. https://doi.org/10.1186/s12916-025-04572-3
Aggarwal, B., Gao, Y., Alfini, A., et al. (2026). Sleep and circadian rhythms in cardiovascular resilience: mechanisms, implications, and a Roadmap for research and interventions. Nature Reviews Cardiology, 23, 116–130. https://doi.org/10.1038/s41569-025-01188-1
Liu, L., Cai, Y., Zhu, M., Liu, Y., & Liu, Y. (2026). Circadian rhythms in cardiovascular disease: A new perspective on inter-organ crosstalk. Medicine Plus. https://doi.org/10.1016/j.medp.2026.100140
Su, F., Huang, D., Wang, H., & Yang, Z. (2021). Associations of shift work and night work with risk of all-cause, cardiovascular and cancer mortality: a meta-analysis of cohort studies. Sleep Medicine, 86, 90–98.
Vyas, M. V., Garg, A. X., Iansavichus, A. V., et al. (2012). Shift work and vascular events: systematic review and meta-analysis. BMJ, 345, e4800.
Manohar, S., Thongprayoon, C., Cheungpasitporn, W., Mao, M. A., & Herrmann, S. M. (2017). Associations of rotational shift work and night shift status with hypertension: a systematic review and meta-analysis. Journal of Hypertension, 35(10), 1929–1937.
Crnko, S., Du Pré, B. C., Sluijter, J. P. G., & Van Laake, L. W. (2019). Circadian rhythms and the molecular clock in cardiovascular biology and disease. Nature Reviews Cardiology, 16(7), 437–447.
Lloyd-Jones, D. M., et al. (2022). Life's Essential 8: updating and enhancing the American Heart Association's construct of cardiovascular health. Circulation, 146, e18–e43.
Scheer, F. A., Hilton, M. F., Mantzoros, C. S., & Shea, S. A. (2009). Adverse metabolic and cardiovascular consequences of circadian misalignment. PNAS, 106(12), 4453–4458.
Morris, C. J., Purvis, T. E., Hu, K., & Scheer, F. A. (2016). Circadian misalignment increases cardiovascular disease risk factors in humans. PNAS, 113(10), E1402–E1411.
Cappuccio, F. P., Cooper, D., D'Elia, L., Strazzullo, P., & Miller, M. A. (2011). Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European Heart Journal, 32(12), 1484–1492.
Chaput, J. P., et al. (2023). The role of insufficient sleep and circadian misalignment in obesity. Nature Reviews Endocrinology, 19, 82–97.
Tsao, C. W., et al. (2023). Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation, 147, e93–e621.
World Health Organization. Cardiovascular diseases (CVDs). https://www.who.int/health-topics/cardiovascular-diseases
This article synthesizes peer-reviewed research current as of mid-2026. Cardiovascular science evolves continuously — always confirm current best practice with your physician.