How Many Hours of Sleep Are Best for Your Heart? New Research Says Timing Matters Too
Explore the latest evidence on the ideal sleep duration for heart health, why both too little and too much sleep increase risk, and how bedtime consistency fits into the picture.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/27/202618 min read
Sleep affects heart health through both duration and consistency. Current research shows that sleeping 7–8 hours per night and maintaining a regular bedtime are associated with the lowest cardiovascular risk. Short sleep, long sleep, and irregular sleep schedules can increase the risk of hypertension, inflammation, atherosclerosis, heart attack, and strok
Key Takeaways
Sleep Is More Than a Number
Modern cardiovascular science shows that heart health depends not only on how long you sleep but also when you sleep. Sleep duration and sleep regularity are complementary pillars of cardiovascular protection.The Heart Thrives on Consistency
Emerging 2025–2026 research suggests that maintaining a consistent bedtime may be nearly as important as achieving 7–8 hours of sleep. Large night-to-night shifts in bedtime are increasingly recognized as an independent cardiovascular risk factor.Both Too Little and Too Much Sleep Carry Risk
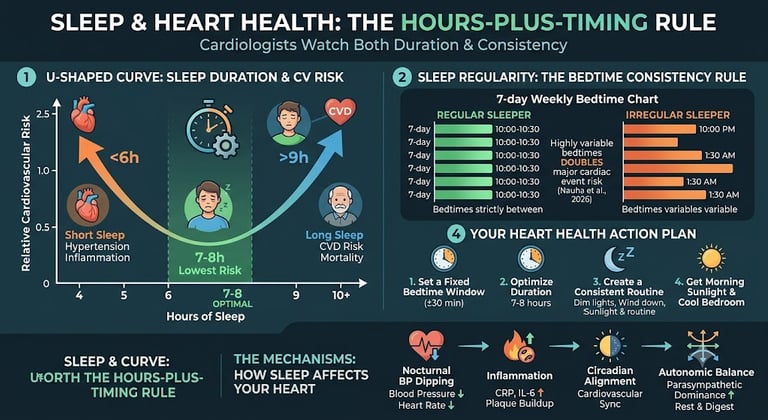
The relationship between sleep duration and heart disease follows a U-shaped pattern. Sleeping substantially less than 7 hours or consistently more than 8–9 hours is associated with higher cardiovascular risk, emphasizing that more sleep is not always better.Sleep Shapes Cardiovascular Biology Every Night
Healthy sleep supports nocturnal blood pressure dipping, reduces chronic inflammation, stabilizes autonomic nervous system function, synchronizes circadian rhythms, and improves metabolic health—all fundamental mechanisms that protect the heart over time.Sleep Should Be Treated Like Exercise and Nutrition
The latest evidence supports viewing sleep as a core lifestyle intervention, not simply a recovery period. Optimizing sleep is now a cornerstone of comprehensive cardiovascular prevention alongside physical activity, diet, and blood pressure control.Personalized Sleep Matters in Cardiovascular Disease
Individuals with hypertension, diabetes, or established heart disease may have a narrower "optimal" sleep range and may be more vulnerable to the adverse effects of prolonged sleep, highlighting the importance of individualized medical guidance.Small Behavioral Changes Can Produce Meaningful Long-Term Benefits
Maintaining a consistent bedtime, obtaining morning daylight exposure, limiting late-night alcohol and heavy meals, and seeking evaluation for symptoms of sleep apnea are practical, evidence-based strategies that can improve long-term cardiovascular health.The Future of Heart Prevention Includes Circadian Health
As wearable technology and objective sleep monitoring become more widespread, cardiology is shifting beyond measuring sleep duration alone. Protecting the heart increasingly means protecting the body's internal clock through regular, restorative sleep habits.
If you've ever Googled "how many hours of sleep do I need for my heart," you've probably landed on the same answer a hundred times: seven to nine hours. Get your number, problem solved.
Except it isn't that simple — and the newest cardiovascular research makes that clear.
A 2026 study from the University of Oulu followed 3,231 adults for more than a decade and found something that duration-only advice misses entirely: people with highly variable bedtimes had roughly double the risk of a major cardiac event compared to people with consistent bedtimes — even after accounting for how many hours they slept overall. Irregular wake-up times, interestingly, didn't carry the same risk. It was bedtime that mattered.
That's not a fluke finding. It sits alongside a growing stack of large cohort studies — some following tens of thousands of people, one following nearly half a million — all pointing toward the same two-part conclusion: your heart cares about how long you sleep, and it separately cares about how consistent that sleep is, night to night.
This guide walks through both halves of that picture using the most current peer-reviewed evidence available, explains the biological mechanisms connecting sleep to your cardiovascular system, and gives you a practical, doctor-informed framework for protecting your heart through better sleep — without resorting to extreme schedules or unrealistic perfectionism.
1. The Big Picture: What the Latest Research Actually Shows
Cardiovascular disease remains the leading cause of death worldwide, and over the past three years, sleep has moved from a "nice to have" wellness footnote to a recognized, independent modifiable risk factor — one taken seriously enough that the American Heart Association's "Life's Essential 8" cardiovascular health checklist now includes sleep duration alongside diet, exercise, and blood pressure.
But the research has evolved fast, and most consumer health content hasn't caught up. Here's the shift:
Old framework: Sleep less than 7 hours → higher heart disease risk → fix it by sleeping more.
Current framework: Heart risk rises at both ends of the sleep duration spectrum, AND separately rises when sleep timing is irregular, AND the size of these effects depends on your existing cardiovascular health, AND duration and irregularity appear to combine multiplicatively rather than just adding together.
This matters practically. If you sleep 7.5 hours a night but your bedtime swings between 10 PM and 2 AM depending on the day, duration-only advice would tell you you're doing great. The regularity research suggests you might not be.
2. Sleep Duration and Heart Disease: The U-Shaped Curve
Short Sleep: The Risk You Expected
Most people intuitively understand that not sleeping enough is bad for the heart, and the data backs that up consistently across populations and study designs.
A large Chinese cohort study following 33,883 adults over a median of five years found that night sleep duration had a meaningful relationship with incident cardiovascular disease, with the researchers specifically noting that underlying chronic health conditions needed to be accounted for to get an accurate picture — a reminder that sleep and heart disease often travel together with other risk factors rather than existing in isolation.
A cross-sectional study of over 8,300 adults in the Hoveyzeh Cohort (Iran) used the well-established Framingham Risk Score to test this more directly, comparing short sleepers (≤5 hours), standard sleepers (6–8 hours), and long sleepers (≥9 hours) against their ten-year cardiovascular risk.
Long Sleep: The Risk Most People Don't Expect
Here's where it gets counterintuitive: sleeping too much appears to be its own independent risk factor, not just a marker of being sick or sedentary (though researchers do work hard to rule that out statistically).
The Korean Ansung-Ansan cohort study, tracking 9,641 adults for over 15 years, found that sleeping more than 8 hours per night was associated with a 27% increase in all-cause mortality risk compared to the reference group. When researchers combined sleep duration with sleep regularity, the picture sharpened further: long sleep duration plus regular sleep timing was associated with a similarly elevated mortality risk as short sleep combined with irregular timing.
A 2026 analysis published in the Journal of Affective Disorders, using NHANES data, found something that helps explain why duration recommendations can't be one-size-fits-all: the shape of the risk curve itself changes depending on your cardiovascular health status. In healthy individuals and those with elevated cardiovascular risk factors, the relationship between sleep time and mortality was U-shaped — both too little and too much sleep raised risk, with a clear low-risk zone in the middle. But in people who already had cardiovascular disease, the relationship was J-shaped instead — meaning long sleep carried a steeper, more linear risk increase, without the same forgiving middle zone.
What "Optimal" Actually Looks Like
A 2026 prospective cohort study from the Eastern Mediterranean Region, following over 5,400 adults free of cardiovascular disease at baseline, modeled this curve directly using restricted cubic splines — a statistical technique that doesn't assume the relationship is a straight line, which matters because sleep-mortality relationships usually aren't. The researchers confirmed a clear U-shaped association between total daily sleep duration and incident cardiovascular disease.
Practical takeaway: Most large studies converge on roughly 7–8 hours per night as the lowest-risk zone, with risk climbing on both sides of that range. But — and this is the part duration-only advice misses — where exactly your personal low-risk zone sits, and how steep the climb is outside it, depends partly on your existing health status (more on this in Section 5).
3. Sleep Regularity: The Risk Factor Hiding in Plain Sight
This is the newest and arguably most underreported part of the sleep-heart story, and it deserves more attention than most health articles give it.
The Finland Study That Changed the Conversation
Published in early 2026, a study following 3,231 adults from the Northern Finland Birth Cohort 1966 used wrist-worn activity monitors — not self-report — to measure three separate sleep timing variables: bedtime variability, wake-up time variability, and sleep midpoint variability. Participants were tracked for major adverse cardiac events (heart attack, stroke, unstable angina, heart failure hospitalization, or cardiovascular death) over ten years.
The standout finding: people with highly variable bedtimes faced roughly double the risk of major cardiovascular events compared to those with stable bedtimes — and this held even after adjusting for total sleep duration. Variable wake-up times did not show the same independent association. As lead researcher Laura Nauha put it, bedtime regularity in particular appears to matter, possibly because it most directly reflects the consistency (or chaos) of someone's daily life rhythms.
The risk was most pronounced in people who were also getting under eight hours of sleep, suggesting irregularity acts as a multiplier on top of insufficient duration, rather than an entirely separate risk pathway.
The UK Biobank Confirms It at Scale
A 2025 study published in the Journal of the American Heart Association used objective accelerometer data from 86,219 UK Biobank participants who were free of cardiovascular disease at baseline. Sleep irregularity was measured as the standard deviation of sleep duration across seven days of continuous monitoring. Higher night-to-night variability in sleep duration was linked to increased risk of incident cardiovascular disease, supporting circadian disruption as a genuine, independent contributor to heart risk — not just a side effect of sleeping too little overall.
Why This Probably Hasn't Reached You Yet
Sleep regularity research has exploded only in the last two to three years, largely because wearable devices made it cheap and accurate to measure objectively across large populations. Older studies relied on one-time questionnaires asking "how many hours do you usually sleep?" — a question that can't capture night-to-night variability at all. As device-based data has accumulated, regularity has emerged as a risk factor that may be just as important as duration, and possibly easier to act on for some people, since it's about when you sleep rather than forcing more hours into a packed schedule.
4. The Mechanisms: How Sleep Actually Affects Your Heart
Understanding why sleep affects cardiovascular risk helps make the recommendations in this article feel less like arbitrary rules and more like something your body is actually doing every night.
Blood Pressure and the Nighttime "Dip"
Healthy cardiovascular physiology includes a phenomenon called nocturnal blood pressure dipping — your blood pressure should drop by roughly 10–20% during sleep compared to your daytime average. Short, fragmented, or irregularly timed sleep disrupts this dip. Over years, a blunted nocturnal dip is associated with arterial stiffening and higher rates of hypertension, a primary driver of heart attack and stroke risk.
Inflammation: The Quiet Driver
Sleep loss and circadian disruption both elevate systemic inflammatory markers, including C-reactive protein (CRP) and interleukin-6 (IL-6). Chronic low-grade inflammation is now understood as a core mechanism in atherosclerosis — the buildup of plaque inside artery walls that eventually narrows or ruptures, causing heart attacks and strokes.
Circadian Hormones and the Heart's Internal Clock
Your cardiovascular system isn't just along for the ride while your brain sleeps — it has its own circadian rhythm, governed by the same master clock (the suprachiasmatic nucleus) that regulates your sleep-wake cycle. Heart rate, blood pressure, and even the electrical stability of heart tissue follow daily rhythms tied to this clock. Irregular sleep timing appears to desynchronize peripheral clocks (including ones in your heart and blood vessels) from your central brain clock — a state researchers sometimes call "circadian misalignment," which has been linked to impaired glucose metabolism, increased blood pressure variability, and elevated cardiovascular risk independent of how many total hours you slept.
Autonomic Nervous System Imbalance
Deep sleep stages are when your parasympathetic ("rest and digest") nervous system dominates, allowing heart rate to slow and heart rate variability — a marker of cardiovascular resilience — to increase. Insufficient or fragmented sleep shifts this balance toward sympathetic ("fight or flight") dominance for more of the 24-hour day, which over years contributes to sustained higher resting heart rate and blood pressure.
Metabolic Knock-On Effects
Sleep loss and irregularity also impair insulin sensitivity and glucose regulation, raising the risk of type 2 diabetes — itself one of the strongest independent risk factors for cardiovascular disease. This creates a secondary pathway: poor sleep doesn't just affect the heart directly, it also worsens the metabolic conditions that damage the heart over time.
5. Does Your Current Heart Health Change the Sleep You Need?
Research comparing sleep-mortality relationships across different baseline cardiovascular health groups has found that the shape of the risk curve genuinely differs:
Healthy individuals: U-shaped curve. A wide "safe zone" of moderate sleep duration (roughly 7–8 hours) with risk rising gradually on both sides.
Individuals with cardiovascular risk factors (but no diagnosed disease): Also U-shaped, but the safe zone may be narrower, and the rise on either side somewhat steeper.
Individuals with existing cardiovascular disease: J-shaped curve. Short sleep still raises risk, but long sleep duration shows a steeper, more concerning climb — without the same protective plateau seen in healthy people.
What this means practically: If you have diagnosed heart disease, a risk-factor profile that already includes things like hypertension or high cholesterol, or a family history of early cardiac events, generic "just get 7–9 hours" advice may not fully apply to you — particularly the upper end of that range. This is exactly the kind of situation where a conversation with your cardiologist or primary care physician about your specific sleep patterns is worth having, rather than relying on general population averages.
6. Evidence Summary: Comparing the Major Studies
Cui et al., 2023 (BMC Public Health)
Population: 33,883 adults in China.
Measure: Self-reported night sleep duration.
Key Finding: Confirmed a clear link between sleep duration and incident cardiovascular disease (CVD), highlighting that an individual's underlying chronic disease status is a critical confounding factor to adjust for in data analysis.
Cheraghian et al., 2023 (BMC Cardiovasc Disord)
Population: 8,362 adults in Iran.
Measure: Self-reported sleep duration evaluated against the Framingham Risk Score.
Key Finding: Found that both short sleep (sub-optimal) and long sleep durations are associated with an elevated 10-year risk of developing cardiovascular disease.
Park et al., 2025 (Scientific Reports)
Population: 9,641 adults in Korea tracked over a 15+ year follow-up period.
Measure: A combined look at sleep duration and sleep regularity.
Key Finding: Discovered that long sleep (>8 hours) raised all-cause mortality risk by 27%. Crucially, combining poor sleep duration with an irregular schedule compounded the total risk.
Huang et al., 2025 (JAHA / UK Biobank)
Population: 86,219 adults in the United Kingdom.
Measure: Objective, accelerometer-measured night-to-night sleep duration variability.
Key Finding: Demonstrated that higher sleep irregularity acts as an independent risk factor directly linked to incident cardiovascular disease, meaning the variance itself matters regardless of average sleep totals.
Nauha et al., 2026 (BMC Cardiovasc Disord)
Population: 3,231 adults in Finland tracked over a 10-year follow-up period.
Measure: Device-measured bedtime, wake time, and sleep midpoint variability.
Key Finding: Discovered that an irregular bedtime roughly doubled the risk of Major Adverse Cardiac Events (MACE). Interestingly, irregularity in wake-up times did not show a statistically significant risk increase.
Ge et al., 2026 (J Affective Disorders)
Population: NHANES cohort in the United States.
Measure: Sleep time evaluated across populations with varying baseline cardiovascular health statuses.
Key Finding: Found a U-shaped risk curve (risk rises at both ends) for healthy individuals and those with basic cardiovascular risk factors. However, for patients with pre-existing cardiovascular disease, the curve shifted to a J-shape, showing a much steeper, more dangerous risk trajectory for long sleep duration.
Habibi et al., 2026 (BMC Cardiovasc Disord)
Population: 5,432 adults in the Eastern Mediterranean Region.
Measure: Sleep duration trajectories.
Key Finding: Mathematically confirmed a stark U-shaped association between total sleep duration and incident cardiovascular disease within this population.
Wang et al., 2026 (Sleep Health)
Population: A massive cohort of 495,398 adults in the UK Biobank.
Measure: The co-occurrence of insomnia symptoms and excessive daytime sleepiness.
Key Finding: Revealed that the joint presence of both symptoms significantly drives up mortality and incident CVD risk far beyond experiencing either symptom alone.
7. Your Practical Action Plan
Here's how to translate this research into an actual nightly routine, broken into duration and regularity since they require slightly different strategies.
Step 1: Find Your Personal Duration Target
Start with 7–8 hours as your baseline target.
Track your sleep for two weeks (a basic wearable or even a simple sleep diary works) alongside how you feel — energy, mood, afternoon alertness.
If you have existing cardiovascular risk factors, lean toward the lower-middle of the 7–8 hour range rather than pushing toward 9+, given the steeper long-sleep risk in that population.
Step 2: Build Bedtime Consistency (Even More Than Wake-Time Consistency)
Based on the bedtime-specific finding from the Finland study, prioritize:
A fixed bedtime window — aim to be within 30 minutes of the same bedtime every night, including weekends.
A consistent 30–45 minute wind-down routine before that bedtime (dim lights, no screens, same low-stimulation activity) so your body gets a reliable cue.
If your schedule varies (shift work, travel, irregular obligations), focus on minimizing the range of your bedtime swings even if you can't hit one exact time — research suggests the variability itself, not just hitting a magic number, is what carries risk.
Step 3: Address the Metabolic and Inflammatory Side Pathways
Limit alcohol and heavy meals within 3 hours of bedtime — both interfere with the nocturnal blood pressure dip.
Get morning sunlight exposure, which helps anchor your circadian rhythm and has been shown to improve both sleep timing consistency and nighttime blood pressure regulation.
Keep your bedroom cool (around 65–68°F / 18–20°C) — body temperature regulation is tightly linked to circadian sleep signaling.
Step 4: Know When to Get Screened
If you experience any of the following alongside poor sleep, bring it up with your doctor rather than trying to self-manage through lifestyle changes alone:
Loud snoring, gasping, or witnessed pauses in breathing during sleep (possible sleep apnea, which independently and substantially raises cardiovascular risk)
Excessive daytime sleepiness despite adequate time in bed
Difficulty falling or staying asleep most nights for more than a month
Known cardiovascular risk factors (hypertension, high cholesterol, diabetes, family history) combined with consistently poor sleep
8. Common Myths and Mistakes
Myth: "I can train my body to need less sleep." There's no strong evidence that adults can sustainably adapt to chronically short sleep without accumulating cardiovascular and metabolic risk, even if subjective sleepiness decreases over time. Feeling less tired isn't the same as your cardiovascular system no longer being affected.
Myth: "Weekend catch-up sleep cancels out weekday sleep debt." Catching up on sleep over the weekend doesn't fully reverse the metabolic and cardiovascular effects of weekday short sleep, and the swing between weekday and weekend sleep timing is itself a form of irregularity — potentially working against you even as you try to "catch up."
Myth: "More sleep is always better for my heart." As covered in Section 2, long sleep duration carries its own independent risk, particularly for people with existing cardiovascular disease. More isn't automatically better past a certain point.
Myth: "Naps make up for bad nighttime sleep." Naps can help with alertness, but they don't replicate the same sleep architecture or circadian timing benefits as consolidated nighttime sleep, and relying on naps to compensate for irregular nighttime sleep doesn't appear to neutralize the irregularity-related cardiovascular risk in the available research.
Myth: "If I feel fine, my sleep must be fine." Several of the mechanisms discussed in Section 4 — blunted nocturnal blood pressure dipping, low-grade inflammation, circadian misalignment — operate silently over years without producing noticeable daytime symptoms until cardiovascular disease is already underway.
9. Frequently Asked Questions
How many hours of sleep is best for heart health? Most large cohort studies point to roughly 7–8 hours per night as the lowest-risk range for cardiovascular outcomes in the general population, with risk increasing at both shorter and longer durations. The exact optimal range can shift somewhat depending on your existing cardiovascular health status.
Is it worse to sleep too little or too much for your heart? Both carry elevated risk compared to the 7–8 hour range, but the relationship differs: in healthy people, the curve is U-shaped with similar risk increases on both ends, while in people with existing cardiovascular disease, long sleep tends to show a steeper risk increase than the same amount of "too little" sleep would.
Does an irregular sleep schedule really affect heart disease risk? Yes — multiple recent device-based studies, including a large UK Biobank analysis and a 10-year Finnish cohort study, found that night-to-night sleep irregularity was independently associated with increased cardiovascular risk, even after accounting for total sleep duration.
Is bedtime consistency more important than wake-time consistency? Based on the most detailed study to separate these two variables, yes — variable bedtimes showed a strong, independent association with major cardiac events, while variable wake-up times did not show the same association in that cohort. More research is needed to confirm this pattern holds broadly.
Can poor sleep cause a heart attack directly? Poor sleep doesn't cause a heart attack in an immediate, mechanical sense, but chronic short, long, or irregular sleep contributes to the underlying conditions — hypertension, inflammation, atherosclerosis, arrhythmia risk — that lead to heart attacks over time. Acute severe sleep deprivation has also been studied as a possible trigger for cardiac events in vulnerable individuals, though this is a separate question from chronic sleep patterns.
Does sleep apnea make this worse? Yes, significantly. Sleep apnea causes repeated drops in blood oxygen and fragmented sleep architecture throughout the night, and it's independently associated with hypertension, arrhythmias, and increased cardiovascular event risk. If you suspect sleep apnea, this isn't something to address through general sleep hygiene alone — it warrants a sleep study and medical evaluation.
How quickly can improving my sleep lower my cardiovascular risk? The cohort studies referenced in this article tracked outcomes over years to decades, so they can't tell us how quickly risk changes after improving sleep habits. However, some of the underlying mechanisms — like nocturnal blood pressure dipping and inflammatory markers — have been shown to improve within weeks of sleep improvement in smaller physiological studies, suggesting the benefit isn't purely a decades-long payoff.
Does this apply the same way to older adults? Several of the cohorts discussed (Hoveyzeh, UK Biobank, Ansung-Ansan) included middle-aged and older adults specifically, and the general U-shaped/J-shaped patterns held across these age groups, though the studies on midlife sleep timing (like the Finland cohort) focused on a narrower midlife age band, so caution is warranted extending those specific bedtime-variability findings to much older populations.
What's the single most actionable change someone can make tonight? Based on the available evidence, picking a consistent bedtime — and treating that consistency as seriously as the total number of hours — appears to be a high-leverage, low-cost place to start, particularly if your current bedtime varies by more than an hour or two night to night.
Do sleep tracking apps and wearables actually help with this? They can help you see patterns you wouldn't otherwise notice — particularly bedtime variability, which is easy to underestimate without data. They're not diagnostic tools, though, and shouldn't replace a clinical sleep study if sleep apnea or another sleep disorder is suspected.
10. Conclusion: What to Do With This Information
The research is genuinely converging on a more complete picture than "just sleep more." Your cardiovascular system responds to both the amount of sleep you get and the consistency of when you get it — and increasingly, the evidence suggests these aren't separate concerns but two dials on the same machine.
Three action steps to start tonight:
Set a bedtime window within 30 minutes, and protect it as consistently as you would a work meeting.
Track your actual sleep duration for two weeks before assuming you know your number — most people underestimate their own variability.
Flag any red-flag symptoms (snoring, gasping, excessive daytime sleepiness) to your doctor now rather than waiting, especially if you already carry other cardiovascular risk factors.
None of this requires extreme intervention. It requires treating sleep timing with the same seriousness you'd give to diet or exercise — because the evidence increasingly suggests your heart is, quite literally, keeping time with it.
If you have existing heart disease, hypertension, diabetes, or other cardiovascular risk factors, talk to your doctor before making significant changes to your sleep schedule, especially if you currently sleep more than 8 hours and are considering reducing that significantly — this should be done gradually and with medical input given the J-shaped risk pattern discussed above.
Related Articles
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWA
Sources
Cui, H., Xu, R., Wan, Y., Ling, Y., Jiang, Y., Wu, Y., Guan, Y., Zhao, Q., Zhao, G., & Zaid, M. (2023). Relationship of sleep duration with incident cardiovascular outcomes: a prospective study of 33,883 adults in a general population. BMC Public Health, 23(1), 124. https://doi.org/10.1186/s12889-023-15042-x
Nauha, L., Niemelä, M., Azadifar, S., Korpelainen, R., & Farrahi, V. (2026). Sleep timing irregularity in midlife: association with incident major adverse cardiac events and cardiovascular disease mortality over a 10-year follow-up. BMC Cardiovascular Disorders, 26, 299. https://doi.org/10.1186/s12872-026-05762-4
Park, S.J., Park, J., Kim, B.S. et al. (2025). The impact of sleep health on cardiovascular and all-cause mortality in the general population. Scientific Reports, 15, 30034. https://doi.org/10.1038/s41598-025-15828-6
Ge, Y., Zhang, X., Sun, J., Zhang, H., & Zhang, J. (2026). Associations of sleep time and all-cause mortality in individuals with a different cardiovascular health status: A population-based cohort study. Journal of Affective Disorders, 393(Part A), 120324. https://doi.org/10.1016/j.jad.2025.120324
Huang, T., Kianersi, S., Wang, H., Potts, K.S., Noordam, R., Sofer, T., Rutter, M.K., & Redline, S. (2025). Sleep duration irregularity and risk for incident cardiovascular disease in the UK Biobank. Journal of the American Heart Association, 14(15), e040027. https://doi.org/10.1161/JAHA.124.040027
Wang, R., Li, T., Zheng, C., Liu, B., Bao, W., & Rong, S. (2026). Associations of concurrent insomnia symptoms and excessive daytime sleepiness with mortality and incident cardiovascular disease. Sleep Health. Advance online publication. https://doi.org/10.1016/j.sleh.2026.05.007
Habibi, D., Kazemi Naeini, M., Haghjooy Javanmard, S., Mohamadifard, N., Hassannejad, R., Rafiei, T., Najafian, J., Akbarzadeh, M., Marateb, H.R., Mansourian, M., Mañanas, M.Á., & Sarrafzadegan, N. (2026). Optimal sleep duration for cardiovascular prevention in Eastern Mediterranean populations: insights from a prospective cohort study. BMC Cardiovascular Disorders, 26, 55. https://doi.org/10.1186/s12872-025-05385-1
Cheraghian, B., Heybar, H., Saki, N., Raeisizadeh, M., Hashemi, S.J., & Bitaraf, S. (2023). Sleep duration and Framingham's cardiovascular risk score: results from the Hoveyzeh Cohort Study (HCS). BMC Cardiovascular Disorders, 23, 570. https://doi.org/10.1186/s12872-023-03611-2
Li, J., Wu, Q., Fan, L., Yan, Z., Shen, D., & Zhang, M. (2023). Nonlinear associations between sleep duration and the risks of all-cause and cardiovascular mortality among the general adult population: a long-term cohort study. Frontiers in Cardiovascular Medicine. https://doi.org/10.3389/fcvm.2023.1109225
Zhao, B., Meng, Y., Jin, X., Xi, W., Ma, Q., Yang, J. et al. (2023). Association of objective and self-reported sleep duration with all-cause and cardiovascular disease mortality: a community-based study. Journal of the American Heart Association, 12(6), e027832. https://doi.org/10.1161/JAHA.122.027832
Chaput, J.P., Biswas, R.K., Ahmadi, M., Cistulli, P.A., Rajaratnam, S.M.W., Bian, W., St-Onge, M.P., & Stamatakis, E. (2025). Sleep regularity and major adverse cardiovascular events: a device-based prospective study in 72,269 UK adults. Journal of Epidemiology and Community Health, 79, 257–264. https://doi.org/10.1136/jech-2024-222795
American Heart Association. Life's Essential 8 — Getting Healthy Sleep. Retrieved 2026 from heart.org.
Cappuccio, F.P., Cooper, D., D'Elia, L., Strazzullo, P., & Miller, M.A. (2011). Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European Heart Journal, 32, 1484–1492.
Daghlas, I., Dashti, H.S., Lane, J., Aragam, K.G., Rutter, M.K., Saxena, R., & Vetter, C. (2019). Sleep duration and myocardial infarction. Journal of the American College of Cardiology, 74, 1304–1314.
Smolensky, M.H., Hermida, R.C., & Portaluppi, F. (2017). Circadian mechanisms of 24-hour blood pressure regulation and patterning. Sleep Medicine Reviews, 33, 4–16.