Thin-Fat Phenotype Explained: Why Normal Weight Doesn’t Mean Low Heart Risk
Lean doesn’t equal healthy. The thin-fat phenotype explains how hidden fat and poor metabolism increase heart disease risk.
HEARTOBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/22/202614 min read
Can you have a heart disease risk with a normal BMI?
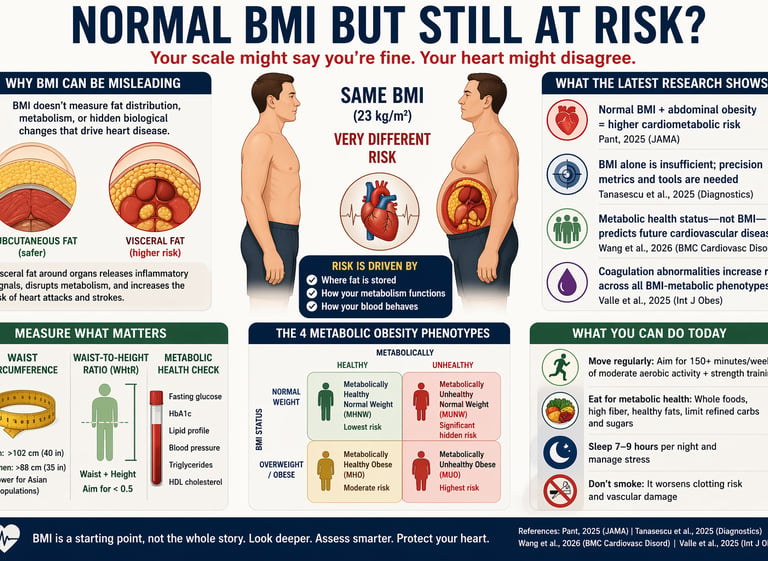
Yes. A normal Body Mass Index (BMI) does not guarantee cardiovascular health. Recent research (2025–2026) shows that individuals with normal BMI but excess abdominal fat or metabolic dysfunction can have a significantly increased risk of heart disease.
This condition—often called metabolically unhealthy normal weight (MUNW)—is associated with:
Insulin resistance
High triglycerides and low HDL cholesterol
Elevated blood pressure
Chronic inflammation
Studies published in JAMA (2025) and BMC Cardiovascular Disorders (2026) demonstrate that metabolic health status—not BMI—is the strongest predictor of cardiovascular disease risk. Additionally, abnormal fat distribution (especially visceral fat around organs) and pro-thrombotic blood markers further increase hidden risk.
Key takeaway:
BMI is a screening tool, not a diagnosis. To accurately assess heart risk, clinicians recommend evaluating:
Waist circumference or waist-to-height ratio
Blood glucose and HbA1c
Lipid profile
Blood pressure
Bottom line: You can look “healthy” on the scale but still be at risk. True cardiovascular health depends on metabolism, fat distribution, and internal biomarkers—not just body weight.
Clinician’s Perspective: Rethinking Cardiovascular Risk Beyond BMI
BMI should no longer be used as a standalone screening tool.
While convenient, BMI fails to capture fat distribution and metabolic dysfunction. Patients with “normal” BMI frequently present with insulin resistance, dyslipidemia, and hypertension—hallmarks of the metabolically unhealthy normal weight (MUNW) phenotype (Pant, 2025).Central adiposity must be routinely assessed.
Waist circumference and waist-to-height ratio (WHtR) are simple, low-cost tools with superior predictive value for cardiometabolic risk. A WHtR >0.5 should trigger further metabolic evaluation, regardless of BMI (Tanasescu et al., 2025).Metabolic health status is a stronger predictor than body weight.
Longitudinal evidence demonstrates that metabolic dysfunction—not BMI category—drives cardiovascular outcomes, with elevated risk seen across all BMI strata in metabolically unhealthy individuals (Wang et al., 2026).Adopt the metabolic phenotype framework in routine practice.
Classifying patients into MHNW, MUNW, MHO, and MUO provides a more clinically meaningful risk-stratification model and helps guide the intensity of intervention.Consider expanded biomarker profiling in selected patients.
Beyond standard lipid panels and glucose metrics, emerging data support the role of coagulation markers (e.g., fibrinogen, PAI-1) in identifying subclinical vascular risk, particularly in metabolically unhealthy individuals (Valle et al., 2025).Ethnicity-specific thresholds are critical.
South Asian populations develop visceral adiposity and metabolic disease at lower BMI levels. Lower cut-offs for BMI and waist circumference should be applied in clinical decision-making.Intervention should target metabolic health, not just weight loss.
Improvements in exercise, dietary quality, sleep, and insulin sensitivity can significantly reduce cardiovascular risk—even in the absence of major weight change.Clinical messaging must evolve.
Reassuring patients solely based on “normal BMI” risks missed diagnoses. The focus should shift to comprehensive cardiometabolic profiling and individualized risk assessment.
For decades, Body Mass Index (BMI) has served as the gatekeeper of cardiometabolic health. Step on a scale, calculate your BMI, and if the number falls between 18.5 and 24.9, you are reassured: “normal,” “healthy,” “low risk.” But emerging evidence from 2025–2026 challenges this comforting narrative with increasing urgency. A growing body of research now shows that a normal BMI does not reliably exclude cardiovascular risk—and in some cases, it may obscure it entirely.
A research letter in JAMA reported that individuals with normal BMI but central (abdominal) obesity exhibit significantly elevated cardiometabolic risk, including insulin resistance, dyslipidemia, and hypertension (Pant, 2025). This phenotype—often described as metabolically unhealthy normal weight (MUNW)—is not rare; it represents a substantial and underdiagnosed segment of the population. Parallel findings from a comprehensive review in Diagnostics emphasize that BMI, as a population-level metric, fails to capture fat distribution, metabolic heterogeneity, and individual cardiovascular vulnerability, prompting calls for more precise risk stratification tools (Tanasescu et al., 2025).
Longitudinal data further reinforce this paradigm shift. In a prospective cohort study, metabolic health status—not BMI category—emerged as the dominant predictor of incident cardiovascular disease, with metabolically unhealthy individuals facing significantly higher risk regardless of body weight (Wang et al., 2026). Adding another layer of complexity, recent work has identified pro-thrombotic alterations in coagulation markers among metabolically unhealthy individuals across all BMI groups, suggesting that vascular risk may be silently progressing even in those who appear “healthy” by conventional standards (Valle et al., 2025).
Taken together, these findings redefine how we should think about weight, metabolism, and cardiovascular risk. The scale may look reassuring—but beneath the surface, biology may be telling a very different story.
Part 1: The BMI Blind Spot — A Metric Designed for Populations, Not People
What BMI Was Never Built to Do
BMI was originally developed in the 19th century by Belgian mathematician Adolphe Quetelet — not as a clinical tool, but as a statistical descriptor of population-level weight trends. It was never validated as an individual health diagnostic. Yet for over half a century, it has functioned as exactly that.
The core limitation is anatomical: BMI cannot distinguish between fat mass and muscle mass, nor between subcutaneous fat (stored under the skin) and visceral fat (stored around internal organs). Visceral fat is metabolically active and inflammatory. It releases cytokines, disrupts insulin signaling, and directly accelerates atherosclerosis — the arterial plaque buildup that leads to heart attacks and strokes.
A person with a BMI of 22 (firmly "normal") can carry excess visceral fat around the abdomen while having relatively little muscle mass — a pattern increasingly called "normal weight obesity" or "thin-fat" phenotype. Conversely, a highly muscular athlete may register a BMI in the "overweight" or even "obese" range while carrying minimal metabolic risk.
What the JAMA Research Letter Revealed
Pant (2025), writing in JAMA, highlighted that normal BMI with abdominal obesity is associated with a clinically meaningful constellation of cardiometabolic risks, including dyslipidemia, insulin resistance, hypertension, and elevated inflammatory markers. The data reinforced what many cardiologists have suspected: the distribution of body fat — not just total body fat — is the critical determinant of cardiovascular risk.
This has profound implications for how screening should work. Waist circumference, waist-to-hip ratio, and waist-to-height ratio are each more predictive of cardiometabolic risk than BMI alone, yet they remain inconsistently measured in routine clinical practice.
Part 2: Beyond BMI — Precision Medicine Enters the Picture
Rethinking Obesity Metrics in 2025
The review by Tanasescu et al. (2025), published in Diagnostics, offers one of the most comprehensive arguments yet for moving beyond BMI as a standalone metric. Framed within the context of precision medicine — the paradigm of tailoring medical care to the individual based on their unique biological profile — the authors argue that our current obesity classification system is too blunt an instrument for the complexities of modern cardiovascular risk assessment.
The paper highlights several alternative and complementary metrics worth understanding:
Waist Circumference (WC): A simple tape measure reading at the navel level. In general, a waist circumference above 88 cm (35 inches) in women and 102 cm (40 inches) in men signals elevated abdominal adiposity and metabolic risk.
Waist-to-Hip Ratio (WHR): Compares the circumference of the waist to that of the hips, capturing the "apple vs. pear" body shape distinction that significantly affects risk.
Waist-to-Height Ratio (WHtR): Many researchers now favor this metric, with a general threshold of 0.5 (your waist should be less than half your height). It accounts for body frame variation and predicts cardiovascular risk more robustly than BMI across diverse populations.
Body Adiposity Index (BAI): Estimates body fat percentage using hip circumference and height, without requiring a scale.
Visceral Adiposity Index (VAI): A formula-based index combining waist circumference, BMI, triglycerides, and HDL cholesterol that estimates visceral fat dysfunction.
Crucially, Tanasescu et al. (2025) argue that precision medicine tools — including genetic profiling, metabolic phenotyping, and advanced imaging like DEXA scans and MRI-based fat quantification — represent the future frontier. Risk is not one-size-fits-all, and medicine must stop treating it that way.
Part 3: Metabolic Obesity Phenotypes — Four Profiles, Dramatically Different Risks
The Four Phenotypes You Need to Know
Perhaps the most clinically actionable framework emerging from recent research is the metabolic obesity phenotype classification. This approach categorizes individuals along two axes: BMI status (normal weight vs. overweight/obese) and metabolic health status (metabolically healthy vs. metabolically unhealthy). The result is four distinct phenotypes:
1. Metabolically Healthy Normal Weight (MHNW): Normal BMI + healthy metabolism. Lowest risk.
2. Metabolically Unhealthy Normal Weight (MUNW): Normal BMI + metabolic dysfunction. Significant hidden risk.
3. Metabolically Healthy Obese (MHO): High BMI + relatively healthy metabolism. Moderate and evolving risk.
4. Metabolically Unhealthy Obese (MUO): High BMI + metabolic dysfunction. Highest risk.
What the Chinese Longitudinal Study Found
Wang et al. (2026), publishing in BMC Cardiovascular Disorders, tracked middle-aged and elderly Chinese individuals over time, examining how these four metabolic phenotypes corresponded to incident cardiovascular disease (CVD). This is particularly valuable because it is a prospective study — it follows people forward in time rather than looking back — making causal inferences more reliable.
The findings confirmed that being Metabolically Unhealthy, regardless of BMI, significantly elevated the risk of developing CVD compared to Metabolically Healthy Normal Weight individuals. Critically, even the Metabolically Healthy Obese (MHO) group showed an elevated long-term risk compared to lean healthy individuals, suggesting that metabolic health status — not BMI — is the dominant predictor of future cardiovascular events.
This has enormous implications for Asian populations specifically, who are known to develop significant visceral adiposity and metabolic dysfunction at lower BMI thresholds than Western populations. The World Health Organization already recommends lower BMI cut-off points for obesity in Asian adults (≥27.5 kg/m² rather than ≥30 kg/m²), but many clinical workflows have not caught up with this guidance.
Key Takeaway
If you have a normal or near-normal BMI but also have elevated fasting glucose, high triglycerides, low HDL cholesterol, high blood pressure, or insulin resistance, you may fall into the Metabolically Unhealthy Normal Weight category — and face cardiovascular risks that standard BMI screening will never flag.
Part 4: The Blood Tells the Story — Coagulation Factors as Cardiovascular Risk Markers
An Underappreciated Dimension of Heart Risk
Valle et al. (2025), writing in the International Journal of Obesity, introduced an especially innovative dimension to this conversation: coagulation factors as biomarkers of cardiovascular risk across BMI-metabolic phenotypes. Published in a rigorous peer-reviewed journal with data spanning diverse participants, this study adds a layer of biological specificity that moves the field closer to true precision risk assessment.
Coagulation factors — the proteins in your blood that control clotting — include fibrinogen, Factor VII, Factor VIII, von Willebrand factor, and plasminogen activator inhibitor-1 (PAI-1), among others. When these factors are elevated or dysregulated, they create a pro-thrombotic state: blood becomes more prone to forming dangerous clots inside arteries, dramatically raising the risk of heart attacks and strokes.
What Valle et al. (2025) found was that metabolically unhealthy individuals — across all BMI categories — showed more adverse coagulation profiles compared to their metabolically healthy counterparts. Notably, some of the most alarming coagulation abnormalities appeared in the Metabolically Unhealthy Normal Weight group — people who, by every standard visual or BMI-based assessment, would appear perfectly healthy.
Why This Matters for You
Most routine blood panels do not include coagulation factor analysis beyond basic PT/INR testing. Yet this research suggests that for individuals with metabolic risk factors — regardless of BMI — targeted coagulation screening could identify hidden cardiovascular danger far earlier than current practice allows.
Part 5: Practical Applications — What You Can Do Right Now
1. Measure Your Waist, Not Just Your Weight
Use a tape measure at the level of your navel — relaxed, not sucked in. Women: aim for under 80 cm (31.5 inches) for lower risk, under 88 cm (34.6 inches) for safety. Men: aim for under 94 cm (37 inches) for lower risk, under 102 cm (40 inches) for safety. (Thresholds vary by ethnicity; South Asian and East Asian individuals should use lower benchmarks.)
2. Calculate Your Waist-to-Height Ratio
Divide your waist circumference by your height (both in the same units). If the result is above 0.5, discuss this with your doctor regardless of your BMI.
3. Ask for a Metabolic Panel, Not Just Weight
Request: fasting glucose, HbA1c, fasting lipid panel (total cholesterol, LDL, HDL, triglycerides), blood pressure, and if warranted, insulin levels. These collectively reveal your metabolic health status.
4. Understand Your Phenotype
Ask your doctor: "Am I metabolically healthy? Could I be in the MUNW category?" This single question can open a very different and more productive clinical conversation.
5. Target Visceral Fat Specifically
Visceral fat responds well to: aerobic exercise (especially moderate-intensity sustained cardio like brisk walking, cycling, swimming), resistance training, Mediterranean-style or low-glycemic dietary patterns, adequate sleep (7–9 hours), and stress reduction. Weight loss on the scale is less important than reductions in waist circumference.
6. Limit Refined Carbohydrates and Sugars
Visceral fat accumulation is heavily driven by excess refined carbohydrate and fructose intake. Shifting to whole grains, legumes, vegetables, lean protein, and healthy fats (olive oil, nuts, fatty fish) directly targets the metabolic abnormalities described in these studies.
7. Don't Smoke — At Any Weight
Smoking dramatically worsens the coagulation profiles described by Valle et al. (2025) and independently raises cardiovascular risk across all BMI categories.
Frequently Asked Questions (FAQs)
FAQ 1: Can I really have heart disease risk with a normal BMI?
Absolutely — and this is one of the most important messages from recent research. Pant (2025) specifically highlighted that individuals with a normal BMI but excess abdominal fat carry meaningful cardiometabolic risks, including high blood pressure, abnormal cholesterol, and insulin resistance. BMI only measures your weight relative to height — it says nothing about where your fat is located or how your metabolism is functioning. A slim-looking person with a "pot belly" and metabolic dysfunction can have a significantly elevated cardiovascular risk.
FAQ 2: What exactly is "metabolic health" and how do I know if I have it?
Metabolic health generally means your body is processing glucose, lipids, and energy efficiently without systemic inflammation or hormonal disruption. Clinically, metabolic health is typically assessed by five markers: waist circumference, blood pressure, fasting glucose, triglycerides, and HDL (good) cholesterol. If three or more of these are outside healthy ranges, you meet criteria for metabolic syndrome — a major cardiovascular risk factor, regardless of BMI. Ask your doctor to review all five at your next check-up.
FAQ 3: Is it possible to be obese but metabolically healthy?
Yes — but with an important caveat. The Metabolically Healthy Obese (MHO) phenotype does exist. Wang et al. (2026) confirmed it in their longitudinal study of Chinese adults. However, MHO is often a transitional state — long-term follow-up studies show that many MHO individuals eventually transition to the Metabolically Unhealthy Obese category over time. So while being metabolically healthy provides some protection even at higher BMI, it does not eliminate risk andshould not be grounds for complacency.
FAQ 4: What is the best measurement to assess my real cardiovascular risk from body fat?
No single measurement tells the complete story, but the waist-to-height ratio (WHtR) is increasingly favored by researchers for its simplicity and predictive power across diverse populations. A WHtR above 0.5 (your waist circumference exceeds half your height) signals elevated cardiometabolic risk. Combine this with a metabolic blood panel and you have a far more complete picture than BMI alone. For advanced assessment, DEXA body composition scanning or abdominal MRI can quantify visceral fat directly.
FAQ 5: Are certain ethnic groups at higher risk for normal-weight cardiovascular problems?
Yes — significantly so. South Asian (including Indian, Pakistani, Bangladeshi) and East Asian populations are known to accumulate visceral fat and develop metabolic dysfunction at substantially lower BMI values than people of European descent. The Wang et al. (2026) study specifically examined Chinese adults and reinforced this concern. For South Asian individuals, many experts recommend using a BMI threshold of ≥23 kg/m² for "overweight" and ≥27.5 kg/m² for "obese" — rather than the standard Western thresholds of 25 and 30.
FAQ 6: Can exercise fix my metabolic health even without significant weight loss?
Yes — and this is genuinely encouraging news. Research consistently shows that regular physical activity improves metabolic health markers independently of weight loss. Aerobic exercise reduces visceral fat, improves insulin sensitivity, lowers triglycerides, raises HDL cholesterol, and reduces blood pressure — all key components of metabolic health. Even 150 minutes per week of moderate-intensity aerobic activity (brisk walking qualifies) produces measurable metabolic improvements. The goal should be metabolic fitness, not just a lower number on the scale.
FAQ 7: Should I ask my doctor about coagulation testing?
Based on the findings of Valle et al. (2025), targeted coagulation testing may be appropriate if you have multiple metabolic risk factors — especially if you also have a personal or family history of blood clots, unexplained cardiovascular events, or conditions like polycystic ovary syndrome (PCOS) or non-alcoholic fatty liver disease (NAFLD) that are associated with pro-thrombotic states. Discuss your individual risk profile with your doctor or a cardiologist. Coagulation testing is not routine for everyone but may reveal critical hidden risks in higher-risk individuals.
Clinical pearls
1. The "Thin-Fat" Phenotype (MUNW)
Scientific Tone: Metabolically Unhealthy Normal Weight (MUNW) individuals often exhibit a "pro-inflammatory" profile. Despite a BMI $< 25$, these patients may have low muscle mass and high visceral adipose tissue, leading to insulin resistance and elevated PAI-1 (plasminogen activator inhibitor-1) levels.
You can’t judge a book by its cover, and you can’t judge a heart by the scale. Some people who look "thin" actually store dangerous fat inside around their organs. This "hidden fat" can make your blood more likely to clot and raise your risk for a heart attack, even if your jeans size hasn't changed.
2. The Dominance of Waist-to-Height Ratio (WHtR)
Scientific Tone: WHtR is a superior predictor of cardiovascular mortality compared to BMI because it accounts for both abdominal adiposity and body frame. A WHtR $> 0.5$ serves as a critical proxy for visceral fat dysfunction and should trigger a formal metabolic workup.
Forget the complex BMI math. A better rule of thumb is: Keep your waist circumference to less than half your height. If your waist is more than half your height, your body is likely carrying a "metabolic load" that puts extra stress on your heart and arteries.
3. Coagulation as a Silent Risk Driver
Scientific Tone: Pro-thrombotic markers, specifically fibrinogen and Factor VIII, are often elevated in metabolically unhealthy phenotypes regardless of weight. In patients with "normal" lipids but high metabolic risk, screening for these coagulation factors may identify subclinical cardiovascular danger.
Heart health isn't just about "clogged pipes" (cholesterol); it’s also about how "sticky" your blood is. Even if your cholesterol looks okay, metabolic issues can make your blood more prone to forming dangerous clots. If you have high blood sugar or a large waistline, your blood might be stickier than it should be.
4. The Asian BMI Threshold Shift
Scientific Tone: Due to a genetic predisposition for increased visceral adiposity at lower weights, the BMI cut-offs for Asian populations are lower. Overweight is defined as $\ge 23$ $kg/m^2$ and obesity as $\ge 27.5$ $kg/m^2$. Using Western standards in these populations leads to a significant underdiagnosis of metabolic syndrome.
Not all bodies handle weight the same way. For people of Indian or East Asian descent, the "danger zone" for weight starts much earlier. A BMI that is considered "healthy" in New York might be considered "overweight" in Mumbai or Beijing because of how the body stores fat.
5. Fitness vs. Fatness (The MHO Caveat)
Scientific Tone: While "Metabolically Healthy Obesity" (MHO) exists, longitudinal data (Wang et al., 2026) suggest it is frequently a transient state. Cardiorespiratory fitness can mitigate, but rarely fully eliminates, the long-term inflammatory risks associated with a high BMI.
Exercise is a miracle drug—it can make you "metabolically healthy" even if you are carrying extra weight. However, being "fit but heavy" is often a temporary shield. Over time, that extra weight can still wear down your body’s defenses, so it’s important to monitor your blood pressure and sugar levels every year.
Author’s Note
This article was written to challenge one of the most deeply ingrained assumptions in modern medicine—that a “normal” Body Mass Index equates to cardiovascular safety. As clinicians, we have long relied on BMI for its simplicity and scalability. However, emerging evidence from journals such as JAMA, Diagnostics, and the International Journal of Obesity suggests that this reliance may inadvertently obscure a substantial burden of hidden cardiometabolic risk.
In everyday clinical practice, it is not uncommon to encounter patients who appear lean yet present with insulin resistance, dyslipidemia, or early hypertension. These individuals often fall into the category of metabolically unhealthy normal weight, a phenotype that remains under-recognized and under-screened. The goal of this article is not to dismiss BMI entirely, but to reposition it—as a starting point rather than a definitive diagnostic tool.
The synthesis presented here reflects a broader shift toward precision medicine, where cardiovascular risk assessment is increasingly individualized. Parameters such as fat distribution, metabolic biomarkers, and even coagulation profiles are proving to be more informative than body weight alone. For regions like South Asia, where visceral adiposity occurs at lower BMI thresholds, this shift is particularly urgent.
For clinicians, the message is clear: expand the lens beyond weight. For patients, the takeaway is empowering: health cannot be reduced to a single number on the scale.
Ultimately, this piece aims to bridge the gap between evolving scientific evidence and real-world application—encouraging more nuanced conversations, earlier detection of risk, and more targeted prevention strategies in cardiovascular care.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Fatty Liver and Heart Disease: The Hidden MASLD Risk You Can't Ignore
Beyond BMI: Why Waist-to-Height Ratio (WHtR) is the New Clinical Gold Standard
What Causes Visceral Fat? Hormones, Lifestyle, and Metabolic Risk Explained | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
Why Belly Fat Causes Insulin Resistance: Portal Theory Explained Simply
Visceral Fat vs Subcutaneous Fat: The Hidden Belly Fat Driving Diabetes and Heart Disease | DR T S DIDWAL
References
Pant, S. (2025). Normal BMI with abdominal obesity associated with cardiometabolic risks. JAMA, 334(21), 1875. https://doi.org/10.1001/jama.2025.17532
Tanasescu, M.-D., Rosu, A.-M., Minca, A., Rosu, A.-L., Grigorie, M.-M., Timofte, D., & Ionescu, D. (2025). Beyond BMI: Rethinking obesity metrics and cardiovascular risk in the era of precision medicine. Diagnostics, 15(23), 3025. https://doi.org/10.3390/diagnostics15233025
Valle, M. M., Robledo, A., O'Leary, S., et al. (2025). Cardiovascular risk factors associated with BMI and metabolic health phenotypes based on measures of coagulation factors. International Journal of Obesity, 49, 2530–2537. https://doi.org/10.1038/s41366-025-01915-1
Wang, K., Zhang, T., & Lin, Y. (2026). Associations between metabolic obesity phenotypes and incident cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovascular Disorders. https://doi.org/10.1186/s12872-026-05849-y