Fatty Liver & Heart Disease: The Hidden MASLD Risk You Can’t Ignore
Discover how Metabolic Dysfunction-Associated Steatotic Liver Disease raises heart attack and stroke risk. Learn symptoms, causes, screening, and proven lifestyle strategies to protect your liver and heart.
HEARTMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/22/202612 min read
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), commonly known as fatty liver disease, significantly increases the risk of heart attack and stroke. It drives systemic inflammation, insulin resistance, and vascular damage—even without symptoms. Early screening, lifestyle changes, and metabolic control can reduce both liver disease progression and cardiovascular risk.
MASLD is no longer a “liver-only” diagnosis
In contemporary practice, Metabolic Dysfunction-Associated Steatotic Liver Disease should be viewed as a systemic cardiometabolic disorder. The presence of hepatic steatosis signals underlying insulin resistance and vascular risk—even when traditional risk scores appear acceptable.Cardiovascular risk stratification must be intensified
Patients with MASLD warrant early and more aggressive ASCVD risk assessment, including lipid profiling, glycaemic status, and, where appropriate, coronary calcium scoring. Standard risk calculators may underestimate true risk in this population.“Metabolically unhealthy” phenotype matters more than BMI
Normal-weight individuals with insulin resistance or dyslipidaemia (MUNW phenotype) often go undetected. Waist circumference, triglyceride–HDL ratio, and HbA1c provide greater clinical insight than BMI alone.The liver is an active driver of atherogenesis
Hepatic overproduction of atherogenic lipoproteins (small dense LDL), inflammatory cytokines (TNF-α, IL-6), and procoagulant factors contributes directly to endothelial dysfunction and plaque instability.Screen beyond liver enzymes
Normal ALT/AST does not exclude clinically significant MASLD. Incorporate non-invasive fibrosis scores (e.g., FIB-4) and imaging modalities when risk factors are present.Therapeutic approach must be dual-targeted (liver + heart)
Lifestyle therapy remains foundational, but pharmacologic agents such as semaglutide, pioglitazone, and empagliflozin offer pleiotropic benefits—improving insulin sensitivity, reducing hepatic fat, and lowering cardiovascular events.Statins are underutilized but essential
Despite persistent myths, statins are safe in MASLD and should be prescribed aggressively when indicated for cardiovascular risk reduction.Think multidisciplinary, not siloed care
Optimal outcomes require coordination between hepatology, cardiology, and endocrinology. Fragmented care leads to missed opportunities for early intervention.Early intervention is the turning point
MASLD represents a window of reversibility. Identifying and treating patients at the stage of metabolic dysfunction can prevent progression to both cirrhosis and major adverse cardiovascular events.
Bottom Line for Clinicians
MASLD is a cardiovascular disease equivalent in evolution—recognize it early, stratify risk aggressively, and treat comprehensively.
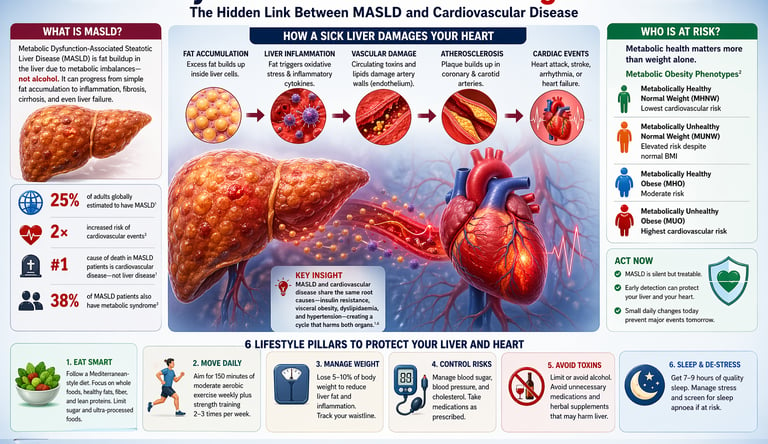
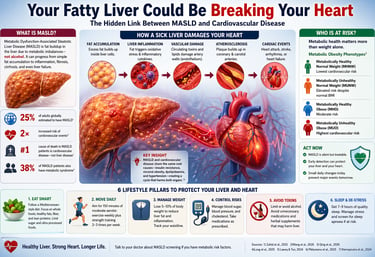
1. What Is MASLD? The Liver Disease You Might Not Know You Have
Your liver may be quietly accumulating fat right now—and sending dangerous signals to your heart long before you feel anything is wrong. This condition, now termed Metabolic Dysfunction-Associated Steatotic Liver Disease, affects nearly one in four adults worldwide, yet remains largely undiagnosed because it is often symptomless in its early stages (Long et al., 2025). Most people assume fatty liver disease is a benign or purely hepatic issue. The science tells a far more concerning story.
Over the past few years, a paradigm shift has emerged: MASLD is not just a liver disorder—it is a systemic cardiometabolic disease that significantly increases the risk of heart attack, stroke, and cardiovascular death (Zahid et al., 2025). In fact, cardiovascular disease—not liver failure—is the leading cause of death in individuals with MASLD (Laeeq & Tun, 2024). This challenges traditional thinking and reframes fatty liver as an early warning system for deeper metabolic dysfunction.
What makes this link so powerful is that it persists even after accounting for conventional risk factors like obesity, smoking, or high cholesterol. In other words, MASLD itself independently accelerates vascular damage through mechanisms such as chronic inflammation, oxidative stress, and endothelial dysfunction (Pădureanu et al., 2025; Ktenopoulos et al., 2024). At the molecular level, emerging research even shows shared genetic and oxidative pathways driving both liver disease and atherosclerosis simultaneously (Qing et al., 2026).
The implication is clear: a diagnosis of fatty liver is not something to ignore—it is a cardiovascular red flag. Understanding this connection offers a critical opportunity for early intervention. The sooner you act, the greater your chance of protecting not just your liver—but your heart and long-term survival.
Important to Know
MASLD is often called a "silent" disease because most people have no noticeable symptoms in the early stages. Fatigue and right-sided abdominal discomfort may occur, but many patients are diagnosed only through routine blood tests or ultrasound scans done for other reasons.
What makes MASLD particularly concerning, however, is not what it does to the liver alone — it's what it does to your heart. A growing body of research from 2024 to 2026 confirms that MASLD is not just a liver disease but a powerful driver of cardiovascular disease (CVD) — the world's leading cause of death. Understanding this connection could literally save your life.
25% of adults globally estimated to have MASLD
2× increased risk of cardiovascular events in MASLD patients
#1 cause of death in MASLD patients is cardiovascular disease, not liver disease
38% of MASLD patients also have metabolic syndrome
2. The MASLD–Heart Disease Connection: More Than a Coincidence
For decades, doctors treated the liver and the heart as separate concerns. You went to a gastroenterologist for your liver and a cardiologist for your heart. But cutting-edge research is dismantling this artificial divide — powerfully and permanently.
A comprehensive 2025 review by Zahid, Lal, Almas et al. published in Current Atherosclerosis Reports describes MASLD as "a growing threat beyond the liver," documenting how the condition substantially elevates the risk of coronary artery disease, heart failure, atrial fibrillation, stroke, and overall cardiovascular mortality. The connection is not merely statistical overlap — it is mechanistic, biological, and deeply intertwined.
Similarly, a 2024 clinical review by Laeeq and Tun in Clinical Liver Disease confirms that patients with MASLD face a significantly higher burden of cardiovascular events, even after adjusting for traditional heart disease risk factors like smoking, hypertension, and high cholesterol. In other words, MASLD is an independent risk factor for heart disease, not just a marker of an unhealthy lifestyle.
"The leading cause of death in patients with MASLD is not liver failure — it is cardiovascular disease."
This single fact should change how both patients and physicians think about fatty liver disease. A diagnosis of MASLD is, in effect, a warning signal from your cardiovascular system, demanding attention and proactive management.
3. How a Sick Liver Damages Your Heart: The Biological Pathway
The Biological Domino Effect
The transition from a fatty liver to a cardiac event follows a specific pathological chain reaction:
Hepatic Fat Accumulation: Excess lipids build up within hepatocytes (liver cells). This isn't just "stored energy"; it is biologically active and toxic in high amounts.
Systemic "Inflammatory Leak": The stressed liver releases pro-inflammatory cytokines—specifically TNF-α, IL-6, and C-reactive protein—into the general circulation.
Vascular Irritation: These inflammatory markers travel to the blood vessels, damaging the endothelium (the delicate inner lining of your arteries).
Atherogenic Lipid Shift: A dysfunctional liver stops producing "clean" cholesterol and begins pumping out small, dense LDL particles. These are stickier and more likely to lodge in artery walls than normal LDL.
Plaque Formation (Atherosclerosis): The combination of "sticky" fats and irritated vessel walls accelerates the buildup of plaque in the coronary and carotid arteries.
Cardiac Events: Eventually, these plaques can rupture or narrow the vessels enough to cause a heart attack, stroke, or heart failure.
The Shared Root Causes
It is helpful to view MASLD and Heart Disease as two branches of the same tree. They are both fueled by Metabolic Syndrome, which consists of:
Insulin Resistance: The body’s inability to manage blood sugar effectively, forcing the liver to create more fat.
Visceral Adiposity: Fat stored deep around the organs (the "beer belly" or "apple shape"), which is more inflammatory than fat stored under the skin.
Dyslipidemia: High triglycerides and low "good" (HDL) cholesterol.
Hypertension: High blood pressure that physically strains both the heart and the liver's vascular network.
Key Takeaway
The liver acts as a metabolic master regulator. When it is "clogged" with fat, it loses its ability to filter toxins and regulate proteins that control blood clotting. This transforms the liver from a protective filter into a source of systemic "biological trash" that directly degrades heart health.
4. Who Is at Risk? The Metabolic Obesity Factor
You might assume that only people who are significantly overweight face these risks. The science tells a more nuanced story. A landmark 2026 study by Wang et al.(2026) published in Atherosclerosis examined the relationship between metabolic obesity phenotypes and incident cardiovascular disease in middle-aged and elderly Chinese individuals — and found that the metabolic profile matters at least as much as body weight alone.
The study identified four metabolic obesity phenotypes:
Metabolically Healthy Normal Weight (MHNW) — lowest cardiovascular risk
Metabolically Unhealthy Normal Weight (MUNW) — elevated risk despite normal BMI
Metabolically Healthy Obese (MHO) — moderate risk
Metabolically Unhealthy Obese (MUO) — highest cardiovascular risk
The critical finding? Metabolically unhealthy individuals face significantly elevated cardiovascular risk regardless of their weight. A person with a "normal" BMI but insulin resistance, elevated triglycerides, or high blood pressure may be in far more danger than an obese person with healthy metabolic markers. This challenges the oversimplified narrative that heart and liver risk is simply about being "fat."
Research Fact
Studies consistently find that visceral fat (fat stored around abdominal organs, including the liver) is far more metabolically dangerous than subcutaneous fat (fat under the skin). A large waistline is a better predictor of MASLD and cardiac risk than total body weight.
5. Oxidative Stress: The Silent Molecular Saboteur
At the cellular level, one of the most important links between MASLD and atherosclerosis is oxidative stress — the imbalance between harmful free radicals and the body's antioxidant defences. When the liver is overloaded with fat, it produces excessive reactive oxygen species (ROS) that damage cell membranes, proteins, and DNA both locally and in distant organs.
A sophisticated 2026 bioinformatics and machine learning study by Qing, Peng, and Peng in Scientific Reports identified shared oxidative stress–related hub genes between NAFLD and atherosclerosis — providing some of the most granular molecular evidence yet that these two diseases are biologically intertwined, not merely coincident.Using machine learning algorithms to analyse gene expression datasets, the team pinpointed specific molecular nodes where the pathways of liver disease and arterial disease converge — opening potential new avenues for targeted therapies.
In practical terms, this means that fighting oxidative stress through diet, exercise, and antioxidant-rich foods is not just good for your liver or just good for your heart — it simultaneously protects both organs through shared molecular pathways.
6. Endothelial Dysfunction: When Your Blood Vessels Give Up
The inner lining of every blood vessel in your body — a single cell-layer thick — is called the endothelium. In a healthy person, the endothelium is a dynamic, active tissue that regulates blood pressure, prevents clots, and controls inflammation. In a person with MASLD, this lining begins to malfunction — a condition called endothelial dysfunction — and this is one of the earliest events in the development of coronary artery disease.
A thorough 2024 review by Ktenopoulos and colleagues in the International Journal of Molecular Sciences explored the bidirectional relationship between NAFLD/MASLD and coronary artery disease through the lens of endothelial dysfunction. Their analysis showed that MASLD damages the endothelium by increasing oxidative stress and inflammatory signalling — and that coronary artery disease, in turn, may worsen liver function through reduced hepatic blood flow, creating a dangerous, mutually reinforcing cycle.
The Bidirectional Problem
MASLD and coronary artery disease do not merely coexist — they accelerate each other. Treating one while ignoring the other is insufficient. A comprehensive, integrated treatment approach is essential for patients who have both conditions.
7. Screening & Early Detection: Your First Line of Defence
Given how silently both MASLD and early cardiovascular disease progress, proactive screening is essential. A 2025 landmark article in The Lancet Gastroenterology & Hepatology by Long, Robbins, and Loomba makes a direct "call to action" to primary care physicians and endocrinologists to routinely screen for MASLD in patients with metabolic risk factors — rather than waiting for symptoms to emerge.
Who Should Be Screened for MASLD?
According to current clinical guidance, the following individuals should discuss MASLD screening with their doctor:
Adults with Type 2 diabetes or pre-diabetes
Adults with obesity (BMI ≥ 30) or elevated waist circumference
Individuals with high triglycerides or low HDL cholesterol
Patients with hypertension
Adults with unexplained elevation in liver enzymes (ALT, AST)
Anyone with a family history of fatty liver disease or cardiovascular disease
What Does Screening Involve?
Screening for MASLD typically begins with simple, non-invasive steps: a physical examination, fasting blood tests (liver enzymes, lipids, blood glucose, HbA1c), and an abdominal ultrasound to detect fat in the liver. If intermediate or high-risk disease is suspected, more advanced tools like FibroScan (transient elastography) or MRI-based liver fat quantification may be used. A liver biopsy — once the gold standard — is now reserved for complex cases.
8. Practical Action Plan: 6 Lifestyle Pillars to Protect Your Liver and Heart
The most empowering message in all of this research is that MASLD and its cardiovascular consequences are largely preventable and modifiable. No single drug yet approved specifically cures MASLD, but lifestyle changes remain the most powerful intervention available — and they benefit your heart at the same time.
Mediterranean-Style Diet
Emphasise vegetables, fruits, whole grains, olive oil, legumes, and oily fish. Minimise ultra-processed foods, refined carbohydrates, and added sugars. Even a 7–10% body weight reduction can significantly reduce liver fat.
Regular Physical Activity
Aim for at least 150 minutes of moderate-intensity aerobic exercise weekly (brisk walking, cycling, swimming). Resistance training 2–3 times per week adds metabolic benefit. Exercise reduces both liver fat and arterial stiffness.
Healthy Weight Management
Even modest weight loss of 5–10% can reduce liver inflammation. Focus on sustainable changes rather than crash diets. Track waist circumference — a shrinking waistline is a direct indicator of falling visceral fat.
Limit Alcohol & Toxic Exposures
Even moderate alcohol worsens liver inflammation in MASLD. Minimise alcohol consumption entirely. Avoid unnecessary medications, supplements, or herbal remedies that can add to liver burden without medical guidance.
Prioritise Sleep & Stress Reduction
Poor sleep and chronic stress worsen insulin resistance, promote visceral fat accumulation, and increase cardiovascular risk. Screen for obstructive sleep apnoea — it is common in MASLD and independently worsens heart outcomes.
Manage Metabolic Risk Factors
Keep blood sugar, blood pressure, and cholesterol within target ranges. Work with your doctor to optimise medications if lifestyle changes alone are insufficient. Statins benefit both cardiovascular and liver outcomes.
Practical Application
Start small and stack habits: Replace one refined carbohydrate (white rice, bread, sugary drinks) with a whole food alternative daily. Add a 20-minute walk after dinner. Schedule a fasting lipid panel and liver enzyme check with your GP this month. Each step alone is modest; together they are transformative. Patients who combine dietary changes with exercise consistently show the greatest reductions in liver fat, cardiovascular inflammation markers, and all-cause mortality risk.
9 . Pharmacotherapy Update for MASLD
GLP-1 receptor agonists (e.g., semaglutide, liraglutide)
Improve weight loss, insulin resistance, and liver fat. Emerging evidence shows resolution of steatohepatitis in some patients, with added cardiovascular risk reduction.Pioglitazone (pioglitazone)
Enhances insulin sensitivity and reduces liver inflammation; recommended in selected patients (especially with Type 2 diabetes). Limitation: weight gain, edema risk.SGLT2 inhibitors (e.g., empagliflozin)
Show promise in reducing liver fat and improving metabolic profile, with proven cardiovascular and renal benefits.Statins (atorvastatin)
Safe in MASLD and essential for atherosclerotic risk reduction, though not a primary liver treatment.
Key Takeaway: No drug is yet universally approved specifically for MASLD, but therapies targeting insulin resistance and weight loss provide dual liver–heart benefits.
Frequently Asked Questions
1. Can I have fatty liver disease without being overweight?
The Answer: Yes. This is known as "Lean MASLD." It often affects individuals who have a genetic predisposition or those with a "metabolically unhealthy" profile (high visceral fat around the organs despite a normal BMI). Even if the scale looks fine, your internal metabolic markers (like insulin and triglycerides) might not be.
2. How is MASLD different from alcoholic liver disease?
The Answer: While both involve fat in the liver, the cause differs. Alcoholic liver disease is triggered by excessive ethanol consumption. MASLD is triggered by metabolic issues like insulin resistance and obesity. However, the 2023 renaming to MASLD was specifically done to focus on these metabolic drivers rather than just the absence of alcohol.
3. If I have MASLD, does that mean I will definitely get heart disease?
The Answer: Not necessarily, but it is a major warning sign. MASLD is an "independent risk factor," meaning it raises your heart disease risk even if your cholesterol and blood pressure are normal. Early intervention through lifestyle changes can stop—and often reverse—the damage before it reaches the heart.
4. What blood tests should I ask my doctor for if I'm concerned about MASLD?
The Answer: Start with a Liver Function Test (LFT) to check enzymes like ALT and AST. You should also request a Fasting Lipid Panel (cholesterol/triglycerides) and an HbA1c (blood sugar). For a more accurate assessment, ask for an FIB-4 score, which is a simple calculation doctors use to estimate liver scarring based on your blood work and age.
5. Are there any approved medications specifically for MASLD?
The Answer: As of early 2026, new therapies like Resmetirom have been approved for patients with liver scarring (fibrosis). Additionally, GLP-1 receptor agonists (often used for diabetes/weight loss) are showing significant promise in reducing liver fat. However, these are supplementary; lifestyle modification remains the "gold standard" treatment.
6. Can children get MASLD, and should parents be concerned about their child's heart health?
The Answer: Unfortunately, yes. Pediatric MASLD is rising due to high-sugar diets and sedentary lifestyles. Because the liver-heart connection starts early, children with fatty liver may develop premature "stiffening" of the arteries, making early dietary intervention critical to prevent heart issues in their 20s and 30s.
7. Is MASLD reversible? Can my liver heal itself?
The Answer: The liver is incredibly resilient. Early-stage MASLD (simple fat buildup) is highly reversible. By reducing caloric intake, cutting out refined sugars (fructose), and increasing physical activity, you can physically "burn off" the fat in the liver cells, which simultaneously lowers your cardiovascular risk.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your medication, diet, or treatment plan. The clinical thresholds discussed represent general evidence-based guidance; individual targets should be determined with your physician.
Related Articles
GLP-1 Receptor Agonists and Cardiovascular Protection: Evidence from CVOT Trials Explained
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Atherogenic Dyslipidemia Explained: The Role of ApoB in Hidden Cardiovascular Risk
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
References
[1] Zahid, M. D., Lal, A., Almas, A., et al. (2025). Metabolic dysfunction-associated steatotic liver disease and cardiovascular disease: A growing threat beyond the liver. Current Atherosclerosis Reports, 27, 108. https://doi.org/10.1007/s11883-025-01353-4
[2] Wang, K., Zhang, T., & Lin, Y. (2026). Associations between metabolic obesity phenotypes and incident cardiovascular disease in middle-aged and elderly Chinese individuals. Atherosclerosis, 391, 117624. https://doi.org/10.1016/j.atherosclerosis.2024.117624
[3] Qing, G., Peng, B., & Peng, H. (2026). Identification of shared oxidative stress related hub genes in NAFLD and atherosclerosis using bioinformatics and machine learning. Scientific Reports, 16, 4644. https://doi.org/10.1038/s41598-025-34958-5
[4] Long, M. T., Robbins, J. J., & Loomba, R. (2025). Screening for and management of MASLD in primary care and endocrinology: A call to action. The Lancet Gastroenterology & Hepatology, 10(1), 84–95. https://doi.org/10.1016/S2468-1253(24)00310-8
[5] Laeeq, T., & Tun, K. M. (2024). Metabolic dysfunction-associated steatotic liver disease and cardiovascular disease. Clinical Liver Disease, 23(1), e0181. https://doi.org/10.1097/CLD.0000000000000181
[6] Pădureanu, V., Forțofoiu, M. C., Pîrșcoveanu, M., Pădureanu, R., Rădulescu, D., Donoiu, I., & Pîrșcoveanu, D. F. V. (2025). Cardiovascular manifestations of patients with non-alcoholic fatty liver disease. Metabolites, 15(3), 149. https://doi.org/10.3390/metabo15030149
[7] Ktenopoulos, N., Sagris, M., Gerogianni, M., Pamporis, K., Apostolos, A., Balampanis, K., Tsioufis, K., Toutouzas, K., & Tousoulis, D. (2024). Non-alcoholic fatty liver disease and coronary artery disease: A bidirectional association based on endothelial dysfunction. International Journal of Molecular Sciences, 25(19), 10595. https://doi.org/10.3390/ijms251910595