The Hidden Longevity Factor Most Doctors Never Talk About: Metabolic Flexibility Explained
What is metabolic flexibility, and why does it hold the key to cellular health and longevity? Reframe your healthspan with evidence-based lifestyle insights
AGINGMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/14/202622 min read
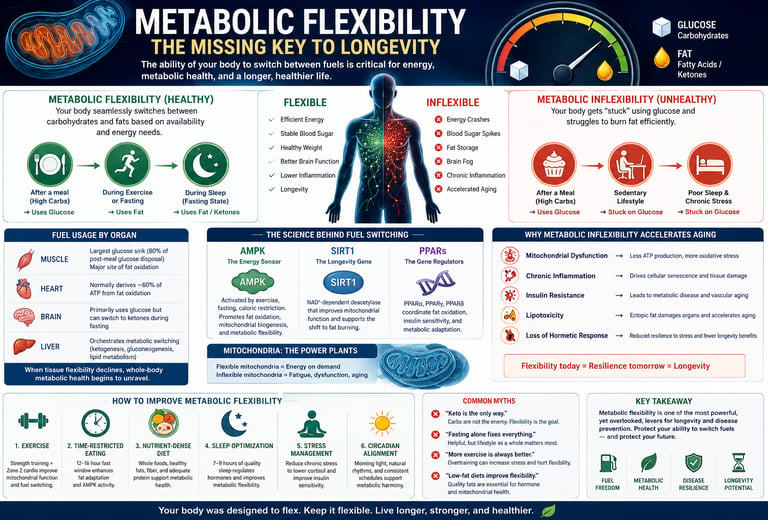
Metabolic flexibility is your body's capacity to shift between burning glucose after meals and burning fat during fasting or exercise. Healthy individuals make this switch seamlessly. When inflexibility occurs, the body gets stuck burning sugar, leading to energy crashes, weight gain, and increased disease risk. Research shows metabolically flexible adults have significantly lower rates of type 2 diabetes and cardiovascular events. Key regulators include mitochondria, AMPK, and phosphatidylcholine levels, all of which respond to lifestyle interventions like exercise and sleep.
Key Takeaways: Metabolic Flexibility & Longevity
1. Metabolic flexibility is the biological capacity to dynamically shift between glucose and fatty acid oxidation based on fuel availability, hormonal state, and energy demand.
Regulated by the Randle Cycle and coordinated through AMPK, SIRT1, and PPAR pathways, this fuel-switching capacity is a fundamental characteristic of metabolic health.
Your body is supposed to run like a hybrid car. After you eat carbs, it should burn glucose. When you sleep or go hours without food, it should smoothly switch to burning fat. If it gets stuck only using sugar, that's metabolic inflexibility.
2. Loss of metabolic flexibility is a primary driver, not merely a consequence, of age-related chronic diseases including type 2 diabetes, cardiovascular disease, and metabolic syndrome.
Impaired fat oxidation capacity precedes insulin resistance and contributes to intramyocellular lipid accumulation, endothelial dysfunction, and cardiac metabolic rigidity.
We used to think bad metabolism caused diseases like diabetes. New research shows it’s often the other way around: losing your ability to burn fat efficiently is what kicks off the disease process in the first place.
3. Mitochondrial dysfunction and ageing-associated decline in phosphatidylcholine synthesis are malleable, mechanistic triggers of metabolic inflexibility.
Poliezhaieva et al., 2026, identified reduced phosphatidylcholine synthesis as a trigger of mitochondrial aging that impairs oxidative capacity. This is modulated by lifestyle intervention.
Your mitochondria are your cellular batteries. As you age, the protective coating around them breaks down, and they get worse at burning fat. The good news: food, sleep, and exercise can help repair that coating.
4. Skeletal muscle is the principal organ of postprandial glucose disposal and a critical determinant of whole-body metabolic flexibility.
Skeletal muscle accounts for approximately 80% of insulin-stimulated glucose uptake. Sarcopenia directly reduces the metabolic buffer capacity for glucose clearance.
Your muscles are like a giant sponge for blood sugar after you eat. The more muscle you have, the bigger your sponge. Losing muscle as you age shrinks that sponge, making blood sugar control much harder.
5. Circadian misalignment disrupts the nocturnal shift to lipid oxidation, accelerating metabolaging.
Melatonin secretion and core body temperature decline are physiologically coupled to increased fatty acid oxidation. Late-night feeding and sleep disruption maintain glucose dependence.
Your body is wired to burn fat while you sleep. Eating late at night or sleeping poorly forces it to stay in "sugar-burning mode" when it should be doing its nightly fat-burning workout. Over the years, that ages you faster.
6. Time-restricted eating improves metabolic flexibility through AMPK activation, independent of caloric restriction.
TRE upregulates beta-oxidation enzymes, induces autophagy, and enhances mitochondrial biogenesis during the fasting window, restoring fuel-switching capacity.
Not eating for 12-14 hours overnight isn't just about eating less. It gives your cells a break so they can flip the "fat-burning switch" back on and clean house. Think of it as daily maintenance for your metabolism.
7. Metabolic inflexibility promotes cellular senescence and systemic low-grade inflammation, creating a feedback loop that accelerates biological aging.
Inflexible cells are more susceptible to entering the senescence-associated secretory phenotype, or SASP, which degrades tissue function via inflammatory cytokine release.
When your cells can't switch fuels, they get stressed and turn into "zombie cells." These zombies don't die, but they pump out inflammation that damages the healthy cells around them, making your whole body age faster.
8. Metabolic flexibility is highly trainable and reversible at most stages through multimodal intervention targeting exercise, nutrition, sleep, and stress.
Moderate-intensity aerobic exercise, resistance training, sleep optimization, and dietary quality demonstrate efficacy in restoring fat oxidation capacity and insulin sensitivity. Genetic predisposition is not deterministic.
You're not stuck with the metabolism you have. Your ability to burn fat is like a muscle. Regular cardio, lifting weights, sleeping well, and managing stress all train it to get stronger, even if it's been weak for years.
Introduction
You eat well. You exercise. You try to sleep enough. Yet something still feels off — energy that crashes after meals, stubborn weight that won't budge, brain fog that clouds your afternoons. What if the missing piece isn't what you eat, but how well your body can switch between fuels?
That ability — to seamlessly shift from burning carbohydrates to burning fat and back again — is called metabolic flexibility, and a growing body of research now frames it as one of the most important yet overlooked determinants of longevity and healthy aging.
In this comprehensive guide, you'll learn exactly what metabolic flexibility is, why metabolic inflexibility silently drives cardiovascular disease, neurodegeneration, and accelerated aging, and — most importantly — the proven, practical steps you can take today to restore and strengthen this fundamental capacity.
Whether you're a clinician, a health-conscious adult, or someone already managing a metabolic condition, this article will give you the clearest, most up-to-date picture available of why metabolic flexibility may be the missing link in your longevity strategy.
What Is Metabolic Flexibility?
Metabolic flexibility is your body's capacity to dynamically shift between burning carbohydrates (glucose) and fats (fatty acids) in response to fuel availability, hormonal signals, and energy demands (Goodpaster & Sparks, 2017).
In a healthy, metabolically flexible individual, this switching is seamless and largely invisible. After a carbohydrate-rich meal, the body preferentially uses glucose. During fasting, sleep, or endurance exercise, it efficiently taps into stored fat. This elegant adaptability is metabolic flexibility in action.
The inverse — metabolic inflexibility — occurs when your body loses this adaptive capacity. Instead of smoothly transitioning between fuel sources, it becomes "stuck," often in a state of chronic glucose dependency. This inability to efficiently oxidize fat is now recognized not merely as a symptom of metabolic disease, but as a primary driver of it (Shoemaker et al., 2023).
Tissue-Specific Metabolic Flexibility
The concept extends beyond whole-body energy management. Different organs have distinct metabolic identities:
Skeletal muscle is the body's largest glucose sink and a primary site of fat oxidation — accounting for roughly 80% of post-meal glucose disposal
The heart normally derives approximately 60% of its ATP from fat oxidation
The brain relies primarily on glucose, but can efficiently shift to ketone utilization during fasting states
The liver orchestrates metabolic switching by regulating gluconeogenesis, ketogenesis, and lipid metabolism
When tissue-specific flexibility is preserved, the whole system thrives. When it degrades — even in one major tissue — systemic metabolic health begins to unravel (Ang et al., 2025).
The Science Behind Fuel Switching
Understanding metabolic flexibility requires a brief look at the molecular machinery that makes it possible.
The Randle Cycle: Your Metabolic Traffic Light
The glucose-fatty acid (Randle) cycle describes the reciprocal inhibition between glucose and fatty acid oxidation. When glucose is abundant, fat burning is suppressed. When fasting or exercising, the switch flips toward fat oxidation. Metabolic inflexibility represents a breakdown in this regulatory toggle — the traffic light gets stuck on red.
Key Molecular Regulators
Three major signaling pathways coordinate fuel switching:
1. AMPK (AMP-Activated Protein Kinase) Often called the body's "energy sensor," AMPK is activated when cellular energy runs low — during exercise, fasting, or caloric restriction. It promotes fat oxidation, stimulates mitochondrial biogenesis, and suppresses glucose-consuming pathways. Interventions that activate AMPK (exercise, time-restricted eating, caloric restriction) measurably improve metabolic flexibility.
2. SIRT1 (Sirtuin 1) This NAD⁺-dependent deacetylase senses nutrient status and modulates metabolic gene expression. SIRT1 activity increases during fasting and exercise, facilitating the transition to fat burning and promoting mitochondrial health.
3. PPAR Family (Peroxisome Proliferator-Activated Receptors) PPARα drives fat oxidation in the liver and heart; PPARγ regulates adipogenesis and insulin sensitivity; PPARδ enhances fat burning in skeletal muscle. Together, these receptors form the transcriptional backbone of metabolic flexibility.
The Mitochondrial Connection
At the cellular level, metabolic flexibility lives and dies in the mitochondria. Mitochondrial dysfunction — reduced oxidative capacity, impaired electron transport chain efficiency, increased reactive oxygen species production — is both a cause and consequence of metabolic inflexibility (Smith et al., 2018).
A landmark 2026 study published in Nature Communications (Poliezhaieva et al., 2026) identified aging-associated decline in phosphatidylcholine synthesis as a malleable trigger of natural mitochondrial aging. Critically, the study showed this decline is not inevitable — it can be modulated through dietary and lifestyle interventions, offering a direct mechanistic link between metabolic health practices and the pace of biological aging.
Complementary research in Nature Aging (Sharma et al., 2026) revealed that peroxisomes — long considered minor cellular compartments — act as master orchestrators of metabolic flexibility and longevity via an interorganelle cascade involving mitochondria and the endoplasmic reticulum. When peroxisome function declines with age, so does the body's ability to efficiently oxidize long-chain fatty acids, accelerating metabolic rigidity.
Why Metabolic Inflexibility Accelerates Aging
The emerging field of "metabolaging" — a term coined in a 2025 review in Metabolism (Khalaf et al., 2025) — proposes that metabolic dysfunction and biological aging are not parallel processes but deeply intertwined ones. Metabolic inflexibility is both a driver and an accelerator of aging through several converging mechanisms:
1. Mitochondrial Deterioration
As metabolic flexibility declines, mitochondrial quality control mechanisms — autophagy, mitophagy, and biogenesis — become less efficient. Damaged mitochondria accumulate, amplifying oxidative stress and impairing energy production in every cell. This is especially pronounced in long-lived postmitotic cells like neurons and cardiomyocytes.
2. Cellular Senescence
A 2023 study in Cell Metabolism (Colville et al., 2023) identified key regulators of cell death and senescence that overlap significantly with metabolic pathways. Metabolically inflexible cells are more susceptible to entering senescence — a state where cells stop dividing but resist death, secreting inflammatory molecules (the SASP: senescence-associated secretory phenotype) that degrade surrounding tissue. This "zombie cell" burden accumulates with age and is measurably lower in metabolically healthy individuals.
3. Chronic Low-Grade Inflammation
Metabolic inflexibility is intimately linked to chronic, low-grade systemic inflammation — sometimes called "inflammaging." Excess intramyocellular lipid accumulation, elevated circulating free fatty acids, and hyperglycemic episodes all activate inflammatory cascades (NF-κB, NLRP3 inflammasome) that accelerate tissue aging.
4. Impaired Circadian Metabolism
Your body is designed to be metabolically different at different times of day. Nocturnal melatonin secretion and the drop in core body temperature are coupled with a shift toward lipid oxidation. Disrupting this rhythm — through late eating, poor sleep, or shift work — locks the body in "glucose mode," blunting the fat-burning window that normally occurs during sleep. Over years, this circadian metabolic disruption significantly accelerates aging (Khalaf et al., 2025).
5. Phosphatidylcholine Depletion
The 2026 Nature Communications study (Poliezhaieva et al.) highlights a surprisingly actionable finding: mitochondrial membranes depend on phosphatidylcholine for their structural integrity and function. As this lipid declines with age — partly due to reduced biosynthetic enzyme activity — mitochondrial function degrades. Dietary strategies that support phosphatidylcholine levels (choline-rich foods, targeted supplementation) may partially reverse this age-related decline.
Metabolic Flexibility and Chronic Disease
Metabolic inflexibility isn't just a longevity concern — it's a near-universal feature of the most common chronic diseases affecting modern populations.
Type 2 Diabetes
Impaired fat oxidation capacity precedes and predicts the development of type 2 diabetes (Goodpaster & Sparks, 2017). Individuals with reduced metabolic flexibility accumulate intramyocellular lipids that impair insulin receptor signaling, creating a vicious cycle: less fat burning → more lipid accumulation → greater insulin resistance → less fat burning.
Restoring metabolic flexibility through structured exercise and temporal eating has demonstrated improvements rivaling pharmaceutical interventions in clinical trials.
Cardiovascular Disease
A metabolically inflexible heart cannot efficiently shift to fat oxidation during metabolic stress. This cardiac metabolic rigidity contributes to:
Reduced exercise tolerance
Diastolic dysfunction
Increased vulnerability to ischemic injury
Accelerated atherosclerosis
Research confirms that individuals with high metabolic flexibility have substantially lower rates of cardiovascular events, better lipid profiles, and improved endothelial function (Palmer & Clegg, 2022).
Obesity and Metabolic Syndrome
Evidence increasingly suggests that metabolic inflexibility drives obesity rather than the reverse. When the body cannot efficiently oxidize fat, it accumulates it — creating a self-reinforcing cycle where excess adipose tissue further impairs fat oxidation capacity (Shoemaker et al., 2023).
Metabolic syndrome — the cluster of central obesity, dyslipidemia, hypertension, and glucose intolerance — represents a clinical manifestation of severe, multi-tissue metabolic inflexibility.
Neurodegenerative Disease
The brain's metabolic flexibility matters too. Emerging evidence suggests that neurons capable of efficiently shifting to ketone utilization during glucose scarcity demonstrate greater resilience against neurodegenerative processes. While mechanistic and human research in this area remains ongoing, the preservation of brain metabolic flexibility is emerging as a promising frontier in dementia prevention.
The "Metabolaging" Framework
The 2025 Metabolism review by Khalaf et al. introduces the "metabolaging" framework, which proposes that metabolic dysfunction and biological aging share common molecular roots — and that intervening at the metabolic level may slow multiple aging pathologies simultaneously. This unifying framework suggests that treating metabolic inflexibility isn't just disease management — it's geroscience-based prevention.
Key Research and Evidence Summary
1. Foundational & Clinical Frameworks
The Metabolic Paradigm: Metabolic flexibility is the ultimate baseline indicator of health, while metabolic inflexibility acts as the primary driver of chronic disease states (Goodpaster & Sparks, 2017).
Mitigating Age-Related Decline: Age-related drops in metabolic flexibility are not an inevitable part of growing older; the system remains highly malleable through targeted lifestyle interventions (Smith et al., 2018).
Cardiometabolic Biomarkers: High metabolic flexibility serves as a direct shield against major cardiovascular risks, explicitly correlating with lower type 2 diabetes (T2D) rates, optimized blood pressure, and superior lipid profiles (Palmer & Clegg, 2022).
The "Metabolaging" Concept: Metabolic dysfunction and biological aging are no longer viewed as separate issues; they are deeply intertwined, mutually reinforcing pathological processes (Khalaf et al., 2025).
2. Tissue & Systemic Mechanisms
Systemic Failure Cascades: Metabolic inflexibility is not isolated to one organ; it involves a progressive, synchronized loss of adaptive capacity that spans multiple tissues simultaneously (Shoemaker et al., 2023).
Interconnected Crosstalk: Whole-body energetic homeostatis and localized, tissue-specific metabolic flexibility are deeply codependent, heavily influencing the progression of cardiometabolic diseases (Ang et al., 2025).
3. Cellular & Organelle Aging Mechanisms
The Senescence Link: Cellular senescence and metabolic regulation share overlapping senolytic pathways; cells that lose their metabolic flexibility are significantly more vulnerable to entering a destructive senescent state (Colville et al., 2023).
Mitochondrial Decay: A decline in phosphatidylcholine levels acts as a critical, yet reversible, trigger for mitochondrial aging, offering a specific target to restore organelle function (Poliezhaieva et al., 2026).
Peroxisomal Orchestration: Peroxisomes act as vital control centers for longevity, regulating overall metabolic flexibility and lifespan through complex, inter-organelle signaling cascades (Sharma et al., 2026).
4. Translational Application
Goodpaster & Sparks (2017) | Cell Metabolism
Finding: Metabolic flexibility is a fundamental marker of health; conversely, inflexibility characterizes multiple chronic disease states.
Relevance: Establishes the foundational framework for the field.
Smith et al. (2018) | Endocrine Reviews
Finding: Metabolic flexibility is highly modifiable through lifestyle adjustments; age-related decline is not an inevitable outcome.
Relevance: Provides the clinical basis for lifestyle interventions.
Palmer & Clegg (2022) | Mayo Clinic Proceedings
Finding: High metabolic flexibility correlates directly with lower Type 2 Diabetes rates, optimized blood pressure, and improved lipid profiles.
Relevance: Demonstrates clear cardiometabolic protection.
Shoemaker et al. (2023) | Journal of Clinical Medicine
Finding: Metabolic inflexibility involves a progressive, synchronized loss of adaptive capacity across multiple distinct tissues.
Relevance: Maps the overarching pathophysiology mechanism.
Ang et al. (2025) | Cell Reports Medicine
Finding: Whole-body energy balance and tissue-specific metabolic flexibility are deeply interconnected in driving cardiometabolic disease.
Relevance: Highlights localized, tissue-specific implications.
Khalaf et al. (2025) | Metabolism
Finding: Defines "Metabolaging"—the reality that metabolic dysfunction and biological aging are deeply intertwined, mutually reinforcing pathological processes.
Relevance: Supplies a unifying Geroscience framework.
Colville et al. (2023) | Cell Metabolism
Finding: Senolytic pathways significantly overlap with metabolic regulation; metabolically inflexible cells are far more prone to cellular senescence.
Relevance: Uncovers a key cellular aging mechanism.
Poliezhaieva et al. (2026) | Nature Communications
Finding: A decline in cellular phosphatidylcholine acts as a highly malleable, reversible trigger of mitochondrial aging.
Relevance: Pinpoints a specific mitochondrial mechanism.
Sharma et al. (2026) | Nature Aging
Finding: Peroxisomes orchestrate overall metabolic flexibility and organismal longevity via complex interorganelle signaling cascades.
Relevance: Outlines a novel longevity pathway.
Murillo-Cancho et al. (2025) | Int. J. Molecular Sciences
Finding: Aging-related metabolic pathways can be actively altered using targeted dietary and pharmacological modulation.
Relevance: Provides direct translational evidence for therapeutic interventions.
Clinical Pearls: How Inflexibility Shows Up in Daily Life
Pearl 1: The "Mitochondrial Traffic Jam"
Metabolic inflexibility creates competition at the mitochondrial level. When the cell cannot switch from glucose to lipid oxidation, intramyocellular lipids and metabolic intermediates accumulate — "congesting" the cellular energy highway. This impairs GLUT4 translocation and worsens insulin resistance.
Pearl 2: Post-Prandial Somnolence as a Diagnostic Signal
That afternoon energy crash after lunch isn't just tiredness — it's a clinically meaningful signal. It reflects failure of the Randle Cycle: the inability to transition to lipid-derived ATP as post-meal glucose levels decline creates a transient cellular "energy crisis."
The takeaway: Persistent post-meal fatigue is one of the earliest, most accessible signs of metabolic inflexibility — long before any lab value becomes abnormal.
Pearl 3: Muscle as Your "Metabolic Sponge"
Skeletal muscle accounts for roughly 80% of post-prandial glucose disposal. Sarcopenia — muscle loss with aging — shrinks this metabolic buffer zone. Every pound of muscle lost reduces your capacity to safely clear blood glucose and increases metabolic vulnerability.
The prescription: Resistance training is not a vanity exercise — it is metabolic medicine. Preserving lean mass is one of the highest-yield interventions for lifelong metabolic flexibility.
Pearl 4: Circadian Rhythm and the Fat-Burning Window
Your body is biologically programmed to preferentially burn fat during sleep. Melatonin secretion and core body temperature decline are coupled with a shift toward lipid oxidation. Late-night eating, excessive light exposure, and fragmented sleep disrupt this rhythm, forcing glucose reliance at a time when your body should be practicing fat oxidation.
The prescription: Closing your eating window 2–3 hours before bed allows your mitochondria to run their nightly "fat-burning workout."
Pearl 5: TRE as a Non-Pharmacological AMPK Activator
Time-Restricted Eating (TRE) works not primarily by reducing calories, but by activating AMPK, upregulating beta-oxidation enzymes, and inducing autophagy during the extended fasting window. A 12–14 hour overnight fast is sufficient to initiate meaningful metabolic adaptations.
The prescription: The simplest version: finish dinner by 7 PM, don't eat until 7–9 AM. That's it. You're training your internal fat-burning engine without any other dietary changes.
How to Improve Metabolic Flexibility: A Practical Protocol
Metabolic flexibility is trainable. Like cardiovascular fitness or muscle strength, it responds to consistent, deliberate practice. Here's an evidence-based framework organized by intervention type.
1. Exercise: The Most Powerful Tool
Endurance Training (Zone 2 Cardio) Moderate-intensity aerobic exercise — where you can hold a conversation but feel slightly challenged — is particularly effective at enhancing fat oxidation capacity. At this intensity, your body primarily burns fat, which trains the enzymatic and mitochondrial machinery needed for metabolic flexibility.
Prescription: 3–5 sessions per week, 30–60 minutes each
Examples: Brisk walking, cycling, swimming, light jogging
Resistance Training Building and maintaining muscle mass expands your metabolic buffer — your body's capacity to absorb and dispose of glucose after meals. Resistance training also improves mitochondrial density in muscle tissue.
Prescription: 2–3 sessions per week, targeting all major muscle groups
Key focus: Progressive overload and consistency over intensity
Variety Matters Incorporating different exercise intensities, durations, and modalities prevents metabolic adaptation stagnation and keeps your energy systems responsive and flexible.
2. Dietary Strategies
Time-Restricted Eating (TRE) Compressing your eating window to 8–12 hours creates a fasting period that activates metabolic switching. Start with a 12-hour window (e.g., 7 AM – 7 PM) and gradually adjust as your body adapts. This is not about eating less; it's about creating temporal separation between feeding and fasting.
Macronutrient Considerations
Adequate protein (1.2–1.6g per kg body weight): preserves muscle mass and supports metabolic adaptation
Quality fats (olive oil, avocado, nuts, fatty fish): support hormone production and cellular signaling; provide fuel during fasted states
Unprocessed carbohydrates timed around activity: leverage glucose availability when your body can most efficiently use it
Choline-Rich Foods Given the 2026 Nature Communications research linking phosphatidylcholine decline to mitochondrial aging, prioritizing choline-rich foods — eggs, liver, fish, legumes — may support mitochondrial membrane health. Discuss supplementation with your healthcare provider if dietary intake is consistently low.
Minimize Ultra-Processed Foods Highly processed, high-glycemic foods disrupt Randle Cycle function, promote chronic low-grade inflammation, and impair the enzymatic machinery needed for efficient fat oxidation.
3. Sleep Optimization
Sleep is non-negotiable metabolic medicine. Poor sleep impairs metabolic flexibility through multiple mechanisms:
Elevates fasting cortisol, promoting glucose reliance
Reduces growth hormone secretion, impairing fat mobilization
Disrupts circadian metabolic rhythms
Increases appetite hormones (ghrelin) and decreases satiety hormones (leptin)
Practical sleep hygiene:
Consistent sleep/wake times (even on weekends)
Cool sleeping environment (65–68°F / 18–20°C)
Complete darkness or a sleep mask
No screens 60–90 minutes before bed
Avoid eating within 2–3 hours of sleep
Goal: 7–9 hours of quality sleep per night.
4. Stress Management
Chronic psychological stress impairs metabolic flexibility through sustained cortisol elevation. Cortisol promotes carbohydrate utilization, suppresses fat oxidation, and impairs glucose tolerance — effectively inducing a state of "stress-driven metabolic inflexibility."
Evidence-based stress reduction practices:
Daily mindfulness meditation (even 10 minutes produces measurable physiological effects)
Controlled breathing exercises (4-7-8 breathing, box breathing)
Regular time in nature ("green exercise")
Adequate social connection and community
5. Monitoring Progress
You don't need advanced metabolic testing to track improvement. Indirect markers include:
✅ Stable energy between meals (no crashing)
✅ Reduced intensity of sugar cravings
✅ Improved cognitive clarity in fasted states
✅ Better exercise performance, especially at moderate intensities
✅ Improved morning glucose readings (if you monitor)
✅ Reduced post-meal fatigue
Common Myths and Mistakes
Myth 1: "Metabolic flexibility means I can eat anything." Metabolic flexibility reflects your physiological capacity to utilize different fuels — not a license to ignore nutrition quality. Even metabolically flexible individuals benefit profoundly from nutrient-dense food choices. High metabolic flexibility doesn't protect against the cumulative damage of chronic ultra-processed food consumption.
Myth 2: "You have to be lean to have good metabolic flexibility." Weight and metabolic flexibility are related but not identical. Some individuals with higher body weight maintain reasonable metabolic flexibility; some lean individuals display significant metabolic inflexibility. Body composition and the location of fat (especially visceral vs. subcutaneous) matter more than total weight.
Myth 3: "One intervention is enough." Metabolic flexibility is a multi-system property. Optimizing it requires a multi-modal approach: exercise, nutrition, sleep, and stress management working together. Doing one well while neglecting the others produces limited results (Smith et al., 2018).
Myth 4: "Metabolic flexibility is genetic — I'm stuck with what I inherited." Genetics influences your metabolic baseline, but research consistently shows that lifestyle factors exert far greater influence on metabolic flexibility than genetic predisposition (Goodpaster & Sparks, 2017). Your DNA is not your destiny here.
Myth 5: "Once you have metabolic inflexibility, it's irreversible." This is perhaps the most damaging myth. Research demonstrates meaningful reversibility of metabolic inflexibility at virtually every stage except end-stage disease. The earlier intervention begins, the greater the restoration of adaptive capacity — but even late interventions produce measurable benefits (Shoemaker et al., 2023).
Myth 6: "You need expensive testing to know if you're metabolically flexible." While clinical tools like indirect calorimetry and continuous glucose monitoring provide useful data, practical markers — your energy stability, exercise capacity, post-meal alertness, and sleep quality — are meaningful, accessible, and actionable indicators.
FAQs
Q: What is the fastest way to improve metabolic flexibility? A: The fastest, most evidence-backed approach combines moderate-intensity aerobic exercise with time-restricted eating. Even a single bout of moderate exercise significantly enhances fat oxidation capacity. Starting a 12-hour eating window simultaneously activates AMPK and begins upregulating fat-burning enzymes. Most individuals notice tangible energy improvements within 2–4 weeks; significant physiological adaptation takes 8–12 weeks of consistency.
Q: Can I improve metabolic flexibility without intermittent fasting? A: Absolutely. Regular exercise, quality sleep, stress management, and a minimally processed diet meaningfully improve metabolic flexibility independent of any specific eating schedule. Intermittent fasting is one tool, not a requirement (Smith et al., 2018).
Q: Does metabolic flexibility matter if I'm healthy and have no metabolic conditions? A: Yes, significantly. Metabolic flexibility directly influences your daily energy levels, cognitive performance, mood stability, athletic capacity, resilience to stress, and long-term disease risk. Everyone benefits from optimizing it — and the earlier you start, the more longevity dividend you accumulate (Goodpaster & Sparks, 2017).
Q: How is metabolic flexibility different from having a "fast metabolism"? A: These are entirely different concepts. Metabolic rate refers to how many calories you burn at rest. Metabolic flexibility refers to how effectively you can switch between fuel sources. You can have a slow metabolic rate with excellent metabolic flexibility, or a fast metabolic rate with significant inflexibility. Flexibility matters more for long-term health.
Q: What does metabolic inflexibility feel like in daily life? A: Common experiences include: afternoon energy crashes, intense carbohydrate cravings, difficulty going more than 2–3 hours without eating, fatigue that isn't relieved by adequate sleep, difficulty losing weight despite calorie restriction, brain fog after meals, and poor exercise recovery. These are functional signals worth taking seriously.
Q: Is age-related decline in metabolic flexibility inevitable? A: No. While sedentary aging is associated with declining metabolic flexibility, physically active individuals with healthy lifestyles maintain high metabolic flexibility well into advanced age. The 2026 Nature Aging research (Sharma et al.) further confirms that peroxisome function — a key regulator of fat oxidation — can be preserved through targeted interventions. Decline is common; it is not inevitable (Smith et al., 2018).
Q: Can children and adolescents have metabolic inflexibility? A: Yes, and it's becoming more prevalent with rising rates of pediatric obesity and sedentary behavior. Early metabolic inflexibility in youth significantly predicts adult cardiometabolic disease. Encouraging regular physical activity, reducing ultra-processed food intake, and protecting sleep in children and adolescents is directly relevant to their long-term metabolic health.
Q: What role do peroxisomes play in metabolic flexibility? A: Peroxisomes are cellular organelles responsible for oxidizing very long-chain fatty acids — a fat-burning pathway that mitochondria cannot handle alone. The 2026 Nature Aging study (Sharma et al.) demonstrated that peroxisome function is essential for longevity and declines with age, partly through communication with mitochondria and the endoplasmic reticulum. Supporting peroxisomal health through regular aerobic exercise and adequate dietary fat quality appears to preserve this critical aspect of metabolic flexibility.
Q: Is there a clinical test for metabolic flexibility? A: Yes. Research-grade assessments include indirect calorimetry (measuring respiratory quotient shifts from a fasted to fed state) and hyperinsulinemic-euglycemic clamp studies. Clinically accessible proxies include fasting insulin levels, HOMA-IR, fasting triglyceride-to-HDL ratio, and continuous glucose monitoring data. Discuss testing options with your physician if you suspect significant metabolic inflexibility.
Q: Can metabolic flexibility training help with weight loss? A: Yes, though through mechanisms beyond calorie counting. Improved metabolic flexibility enhances your body's ability to oxidize stored fat as fuel, reduces the hormonal drivers of fat storage (especially around the abdomen), decreases chronic inflammation that impairs fat metabolism, and stabilizes appetite hormones — all of which support sustainable, healthy weight management.
Conclusion and Action Steps
Metabolic flexibility is not a niche research concept. It is, increasingly, one of the most clinically relevant and actionable dimensions of human health — a fundamental biological capacity that determines how gracefully you age, how resilient you remain against chronic disease, and how fully you experience life at every stage.
The convergence of evidence from molecular biology, clinical epidemiology, and emerging geroscience is unmistakable: metabolic inflexibility is a primary driver of the most common aging-related diseases, and it is largely modifiable.
Here are your clear action steps:
Start moving daily. Prioritize 30–45 minutes of moderate-intensity aerobic exercise at least 5 days per week. Add resistance training 2–3 times weekly.
Compress your eating window. Begin with a 12-hour overnight fast (e.g., 7 PM to 7 AM). Gradually extend to 14–16 hours as your body adapts.
Protect your sleep. Commit to 7–9 hours of quality sleep with consistent timing, a cool dark environment, and no food in the 2–3 hours before bed.
Manage stress actively. Build a daily stress-reduction practice — even 10 minutes of breathwork or meditation produces measurable metabolic benefits.
Eat to support mitochondria. Prioritize whole foods, adequate protein, quality fats, and choline-rich foods. Minimize ultra-processed food consumption.
Track your signals. Notice post-meal energy, craving intensity, fasted clarity, and exercise capacity. These are your most accessible real-time metabolic flexibility monitors.
Consult your healthcare provider. If you suspect significant metabolic inflexibility or have existing metabolic conditions, work with a qualified clinician to personalize your approach and consider appropriate metabolic testing.
Here is a rewrite of the Author’s Note that weaves in a relatable patient example to ground the complex science in real-world clinical practice.
Author’s Note
This article was written to bridge the widening gap between advanced metabolic science and everyday clinical reality. Consider a patient like Sarah, a 48-year-old schoolteacher. On paper, Sarah seems to be doing everything right: she watches her weight and counts her calories. Yet, she feels chronically fatigued, experiences intense energy crashes two hours after eating, and notices that the same diet that worked for her a decade ago now yields no results. While standard public discourse might simply label Sarah's struggles as "early insulin resistance" or an "inevitable part of aging," these labels obscure the true underlying issue: Sarah has lost her metabolic flexibility.
Metabolic flexibility—the body's capacity to seamlessly switch between burning carbohydrates after a meal and burning fat during a fast—is no longer just an abstract research concept. It has emerged as the unifying framework that explains why metabolic diseases develop, why they progress, and why two patients can respond so differently to the exact same diet or exercise routine.
The perspectives presented here are grounded in peer-reviewed human and mechanistic research from leading metabolic journals. However, this article does not advocate for extreme dietary restrictions, rigid protocols, or one-size-fits-all solutions. Instead, it emphasizes restoring physiological resilience through evidence-based lifestyle strategies that align with basic human biology.
For Clinicians: I encourage you to view patients like Sarah not as cases of inevitable age-related decline, but as individuals experiencing an early, highly modifiable pathological state.
For Patients: I hope to show you that true metabolic health is not defined by physical appearance or obsessive calorie counting, but by your body’s dynamic ability to efficiently adapt to changing energy demands.
Ultimately, the goal of this work is to reframe metabolic health as a trainable, dynamic capacity—one that offers powerful, practical opportunities for disease prevention, improved healthspan, and longevity.
Medical Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice. Individual circumstances vary significantly. Always consult with a qualified healthcare professional before making changes to your diet, exercise routine, or any aspect of your health management, particularly if you have existing medical conditions.
Related Articles
Diet, Longevity, Genes, and Life Expectancy: How Your Food Choices May Help You Live Longer
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health | DR T S DIDWAL
References
Ang, J. C., Sun, L., Foo, S. R., Leow, M. K., Vidal-Puig, A., Fontana, L., & Dalakoti, M. (2025). Perspectives on whole body and tissue-specific metabolic flexibility and implications in cardiometabolic diseases. Cell Reports Medicine, 6(9), Article 102354. https://doi.org/10.1016/j.xcrm.2025.102354
Anton, S. D., Moehl, K., Donahoo, W. T., Marosi, K., Lee, S. A., Mainous, A. G., ... & Mattson, M. P. (2018). Flipping the metabolic switch: Understanding and applying the health benefits of fasting. Obesity, 26(2), 254–268. https://doi.org/10.1002/oby.22065
Colville, A., Liu, J.-Y., Rodriguez-Mateo, C., Thomas, S., Ishak, H. D., Zhou, R., … Rando, T. A. (2023). Death-seq identifies regulators of cell death and senolytic therapies. Cell Metabolism, 35(10), 1814–1829.e6. https://doi.org/10.1016/j.cmet.2023.08.008
Goodpaster, B. H., & Sparks, L. M. (2017). Metabolic flexibility in health and disease. Cell Metabolism, 25(5), 1027–1036. https://doi.org/10.1016/j.cmet.2017.04.015
Hargreaves, M., & Spriet, L. L. (2020). Skeletal muscle energy metabolism during exercise. Nature Metabolism, 2(9), 817–828. https://doi.org/10.1038/s42255-020-0251-4
Holloszy, J. O. (2011). Regulation of mitochondrial biogenesis and GLUT4 expression by exercise. Comprehensive Physiology, 1(2), 921–940. https://doi.org/10.1002/cphy.c100052
Kelley, D. E., He, J., Menshikova, E. V., & Ritov, V. B. (2002). Dysfunction of mitochondria in human skeletal muscle in type 2 diabetes. Diabetes, 51(10), 2944–2950. https://doi.org/10.2337/diabetes.51.10.2944
Khalaf, F., Barayan, D., Saldanha, S., & Jeschke, M. G. (2025). Metabolaging: A new geroscience perspective linking aging pathologies and metabolic dysfunction. Metabolism, 166, Article 156158. https://doi.org/10.1016/j.metabol.2025.156158
Lira, V. A., Benton, C. R., Yan, Z., & Bonen, A. (2010). PGC-1α regulation by exercise training and its influences on muscle function and insulin sensitivity. American Journal of Physiology—Endocrinology and Metabolism, 299(2), E145–E161. https://doi.org/10.1152/ajpendo.00755.2009
Longo, V. D., & Panda, S. (2016). Fasting, circadian rhythms, and time-restricted feeding in healthy lifespan. Cell Metabolism, 23(6), 1048–1059. https://doi.org/10.1016/j.cmet.2016.06.001
Moro, T., Tinsley, G., Bianco, A., Marcolin, G., Pacelli, Q. F., Battaglia, G., … Paoli, A. (2016). Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. Journal of Translational Medicine, 14, Article 290. https://doi.org/10.1186/s12967-016-1044-0
Murillo-Cancho, A. F., Lozano-Paniagua, D., & Nievas-Soriano, B. J. (2025). Dietary and pharmacological modulation of aging-related metabolic pathways: Molecular insights, clinical evidence, and a translational model. International Journal of Molecular Sciences, 26(19), Article 9643. https://doi.org/10.3390/ijms26199643
Palmer, B. F., & Clegg, D. J. (2022). Metabolic flexibility and its impact on health outcomes. Mayo Clinic Proceedings, 97(4), 761–776. https://doi.org/10.1016/j.mayocp.2022.01.012
Petersen, K. F., Befroy, D., Dufour, S., Dziura, J., Ariyan, C., Rothman, D. L., … Shulman, G. I. (2003). Mitochondrial dysfunction in the elderly: Possible role in insulin resistance. Science, 300(5622), 1140–1142. https://doi.org/10.1126/science.1082889
Poliezhaieva, T., Li, Y., Chaudhari, P. S., Isildak, U., Alonso-Pernas, P., Valentim, I. S., … Ermolaeva, M. A. (2026). Aging-associated decline of phosphatidylcholine synthesis is a malleable trigger of natural mitochondrial aging. Nature Communications, 17(1), Article 71508. https://doi.org/10.1038/s41467-026-71508-7
Randle, P. J., Garland, P. B., Hales, C. N., & Newsholme, E. A. (1963). The glucose fatty-acid cycle: Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. The Lancet, 281(7285), 785–789. https://doi.org/10.1016/S0140-6736(63)91500-9
Sharma, A., Prabhakar, A., Valera-Alberni, M., et al. (2026). Peroxisomes orchestrate metabolic flexibility and longevity via an interorganelle cascade. Nature Aging, 6, 987–1006. https://doi.org/10.1038/s43587-026-01122-1
Shoemaker, M. E., Gillen, Z. M., Fukuda, D. H., & Cramer, J. T. (2023). Metabolic flexibility and inflexibility: Pathology underlying metabolism dysfunction. Journal of Clinical Medicine, 12(13), Article 4453. https://doi.org/10.3390/jcm12134453
Smith, R. L., Soeters, M. R., Wüst, R. C. I., & Houtkooper, R. H. (2018). Metabolic flexibility as an adaptation to energy resources and requirements in health and disease. Endocrine Reviews, 39(4), 489–517. https://doi.org/10.1210/er.2017-00211
Van Loon, L. J. C., Greenhaff, P. L., Constantin-Teodosiu, D., Saris, W. H. M., & Wagenmakers, A. J. M. (2001). The effects of increasing exercise intensity on muscle fuel utilisation in humans. Journal of Physiology, 536(1), 295–304. https://doi.org/10.1111/j.1469-7793.2001.00295.x