The 9-Year Healthspan Gap: Living Longer, Not Better
Discover the science of healthspan vs lifespan and learn why the average person spends nearly a decade in poor health before death. Explore the latest 2025–2026 research on healthy ageing, longevity medicine, exercise, sleep, nutrition, inflammation, and functional independence — with practical strategies to help you live longer and live better.
AGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/19/202622 min read
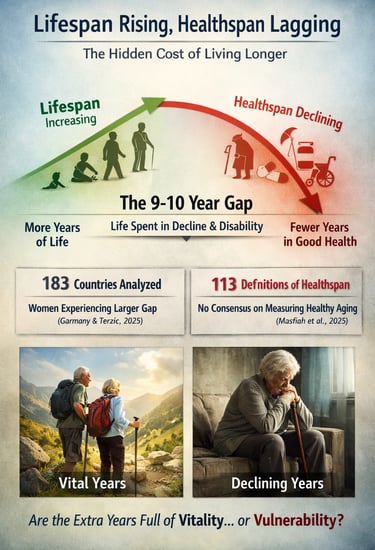

For most of human history, medicine fought a single enemy: early death. Vaccines, antibiotics, safer childbirth, cardiovascular therapies, and modern cancer treatments transformed that battle with astonishing success. In just over a century, global life expectancy has risen dramatically, allowing millions to survive diseases that once killed in childhood or middle age. Yet modern medicine now faces a more complex and uncomfortable challenge: many people are living longer without living better. Across 183 World Health Organization member states, researchers estimate that the average person spends nearly a decade of life coping with chronic illness, disability, frailty, or cognitive decline — a widening divide now known as the healthspan–lifespan gap (Garmany & Terzic, 2025).
This shift is redefining the future of healthy ageing, longevity medicine, and preventive healthcare. The critical question is no longer simply How long can humans live? but How long can humans remain strong, independent, cognitively sharp, and fully engaged in life? Researchers studying biological ageing increasingly argue that extending lifespan without preserving functional capacity represents only partial success (Olshansky, 2018).
The newest science suggests that healthspan is not determined solely by genetics or luck. Physical activity, sleep quality, nutrition, metabolic health, skeletal muscle preservation, social connection, and even sense of purpose appear to influence the rate at which the body biologically ages (Biswas et al., 2026; Liubertas, 2026). In other words, ageing is not merely the passage of time — it is the gradual accumulation of biological damage that may be slowed, compressed, and, in some cases, partially prevented. The future of medicine may depend less on helping people survive longer and more on helping them remain truly alive within those added years.
9–10 Years: The average global gap between total lifespan and healthy, independent living (Garmany & Terzic, 2025 — analysis of 183 WHO member states)
Key Takeaways
1. What Is the Healthspan Gap?
The healthspan gap is the difference between how long people live and how many of those years are spent in good health. Current research shows the average global gap is approximately 9–10 years, meaning many adults spend nearly a decade managing chronic illness, disability, or frailty (Garmany & Terzic, 2025).
2. Healthspan Matters More Than Lifespan Alone
Lifespan measures total years lived, while healthspan measures years lived free from major disease and functional decline. Modern longevity medicine increasingly focuses on preserving independence, mobility, cognition, and quality of life — not simply extending survival.
3. Exercise Is the Strongest Healthspan Intervention
Regular physical activity — especially resistance training combined with aerobic exercise — improves muscle mass, metabolic health, cardiovascular fitness, mitochondrial function, and cognitive resilience. Exercise is one of the most evidence-based tools for slowing biological ageing.
4. Sleep, Nutrition, and Movement Work Together
Emerging 2026 research shows that combined lifestyle adequacy across sleep, physical activity, and nutrition produces greater healthspan benefits than optimising any single factor alone (Biswas et al., 2026). Consistency across all three pillars is more important than perfection.
5. Muscle Strength Predicts Healthy Ageing
Grip strength, gait speed, balance, and VO2 max are powerful predictors of long-term survival and independence. Preserving skeletal muscle through resistance training is essential for reducing frailty, falls, and disability in later life.
6. Loneliness Accelerates Biological Ageing
Social isolation increases chronic inflammation, stress hormone dysregulation, and the risk of cognitive decline. Strong social connection and a sense of purpose are increasingly recognised as biologically important components of healthy ageing and longevity.
7. The Goal of Longevity Medicine Is Functional Independence
The future of ageing science is not merely helping people live longer — it is helping them remain physically capable, mentally sharp, emotionally engaged, and independent for as many years as possible. True longevity means extending both lifespan and healthspan together.
Part 1: Understanding the Language of Longevity
Before we can close the gap, we need to understand exactly what we are measuring. Three terms are used interchangeably in popular media — lifespan, healthspan, and longevity — but they represent fundamentally different concepts, and conflating them has real consequences for how we live, how we invest in healthcare, and what we demand from our doctors.
Lifespan: The Blunt Instrument
Lifespan is the total number of years an individual lives from birth to death. As a population metric, it is expressed as life expectancy. It is objective, binary, and easily measurable. You are either alive or you are not. This simplicity makes lifespan an appealing metric for governments and researchers, but it tells us absolutely nothing about the quality of those years.
Healthspan: The Metric That Actually Matters
Healthspan refers to the period of life spent in genuinely good health — free from significant chronic disease, disability, or functional limitation. It is the answer to the question that most of us actually care about: not just how long will I live, but how well will I live?
Here is where the science becomes complicated. A landmark 2025 systematic review by Masfiah and colleagues searched the published literature and found an astonishing 113 different published definitions of healthspan. Some researchers mark the end of healthspan at the first diagnosis of a chronic disease. Others focus on functional capacity — can the person climb stairs, manage their finances, or live independently? Still others incorporate biomarkers, quality-of-life questionnaires, psychological well-being, or composite frailty indices.
The Measurement Crisis
"Without a universally accepted metric for healthspan, we cannot reliably compare interventions, track population trends, or allocate healthcare resources optimally." The 113-definition problem is not merely inconvenient — it is a scientific crisis that slows every aspect of progress in this field (Masfiah et al., 2025).
Longevity: A Shifting Goalpost
Longevity was historically used interchangeably with lifespan. Increasingly, however, longevity in scientific and clinical contexts refers to the achievement of exceptional age while maintaining health and function. The emerging field of longevity medicine explicitly aims to extend the healthy years of life — not simply to delay biological death.
This semantic evolution matters enormously, because it reshapes what we are trying to optimise. As Olshansky argued in JAMA as far back as 2018, the mission of modern medicine must shift from merely adding years to life toward adding life to those years.
A bold new extension of this framework has been proposed by Liubertas (2026) in Frontiers in Aging Neuroscience, who introduces the concept of experienced longevity — a biological framework that moves beyond objective health metrics to incorporate the subjective quality of conscious ageing. In this view, a long life that feels purposeful, engaged, and rich in experience is qualitatively different from a long life that simply registers as disease-free on a biomarker panel. The field is maturing toward a more complete, human-centred definition of what it means to age well
Part 2: The 9-Year Gap — What the Evidence Really Shows
The most powerful quantification of the healthspan–lifespan problem to date comes from Garmany and Terzic (2025), whose analysis in Communications Medicine examined data from all 183 WHO member states. Their findings are both sobering and, crucially, hopeful.
The global average gap of 9 to 10 years between lifespan and healthspan is not uniform. It differs dramatically in both magnitude and in the specific diseases that drive it depending on world region. Some areas have achieved meaningful compression of morbidity — keeping the period of significant illness relatively brief relative to total lifespan. Others have seen the gap widen considerably. These differences, the authors argue, are not random. They reflect differences in healthcare systems, economic resources, cultural factors, dietary patterns, physical activity norms, and public health infrastructure — all of which are potentially modifiable.
This regional variation is one of the most important findings in recent ageing science, because it proves a central point: the healthspan gap is not biologically inevitable. It is, to a meaningful degree, a product of choices — personal, clinical, and political.
The Gender Health-Survival Paradox
Women consistently outlive men — yet spend a greater proportion of their additional years managing disability, chronic illness, and frailty. Garmany and Terzic (2025) documented this gendered gap across their global analysis. Women live longer marathons but are often less structurally prepared for the distance, partly due to post-menopausal hormonal shifts, lower baseline skeletal muscle mass, and historically underserved cardiovascular care.
This means women in particular must be proactive — and early — about strength training, bone density preservation, and cardiovascular health monitoring. The longevity advantage becomes a burden unless it is supported by adequate healthspan investment.
The Economic Consequence of Getting This Wrong
Jugran (2025), writing in the Journal of Global Health, frames the problem in stark policy terms: extending lifespan without extending healthspan is a policy failure. Additional years marked by multimorbidity translate directly into higher medication burdens, more frequent hospitalisations, long-term care dependency, and escalating caregiver strain. Health systems optimised for episodic disease treatment are fundamentally ill-equipped to manage a population experiencing prolonged, multi-decade frailty.
The economic case for investing in healthspan is, if anything, even stronger than the humanitarian one.
Part 3: What the Newest Science Tells Us (2025–2026)
The science of healthy ageing is advancing rapidly. Three landmark studies published in 2025 and 2026 have added crucial new dimensions to our understanding, with direct implications for how individuals and health systems should respond.
1. Sleep + Exercise + Nutrition: The Triple Combination That Moves the Needle
One of the most practically significant recent findings comes from Biswas and colleagues (2026), publishing in eClinicalMedicine. Their population cohort study investigated something previous research had largely neglected: not individual lifestyle factors in isolation, but the minimum combined thresholds of sleep, physical activity, and nutritional quality that together produce measurable improvements in both lifespan and healthspan outcomes.
The findings are immediately actionable. You do not need to be an elite athlete, follow a perfect diet, or achieve laboratory-grade sleep architecture to move the needle on your healthspan. What matters is consistently meeting a minimum combined threshold across all three domains. Optimising one at the expense of the others is far less effective than achieving adequate levels across all three simultaneously.
Clinical Takeaway
The evidence from Biswas et al. (2026) suggests a practical hierarchy: prioritise adequacy in all three lifestyle pillars — sleep, movement, and nutrition — before chasing excellence in any single one. A mediocre diet, combined with good sleep and regular activity, outperforms a perfect diet combined with sedentary behaviour and poor sleep.
2. Experienced Longevity: The Role of Subjective Wellbeing
The biological framework proposed by Liubertas (2026) in Frontiers in Aging Neuroscience challenges the field to look beyond measurable biomarkers and functional tests. Experienced longevity recognises that the quality of conscious experience during the ageing process — purpose, engagement, emotional richness, and personal meaning — constitutes a distinct and scientifically important dimension of healthy ageing.
This is more than philosophy. Chronic loneliness and loss of purpose accelerate a process called inflammaging — the progressive rise in systemic low-grade inflammation that drives accelerated biological ageing. High-quality social engagement is correlated with lower levels of interleukin-6 (IL-6) and C-reactive protein (CRP), markers that are themselves predictive of shortened healthspan. Isolation, the science now makes clear, is as biologically damaging as smoking.
3. Discover Aging: A Field Committing to Convergence
Crasta and colleagues (2026) launched Discover Aging, a new multidisciplinary research forum in the journal of the same name, explicitly dedicated to understanding and improving healthspan. The launch of such a forum signals something important: the ageing science community recognises that progress requires convergence — across disciplines, across definitions, and across methodologies.
The existence of 113 definitions of healthspan (Masfiah et al., 2025) is a problem the field is now actively mobilising to solve. A standardised, validated, culturally sensitive healthspan metric — one that incorporates biological markers, functional tests, cognitive performance, and subjective wellbeing — is the prerequisite for meaningful population-level progress.
Part 4: Exercise Is Not Optional — It Is Medicine
Of all the lifestyle factors associated with extended healthspan, regular physical activity has the strongest and most consistent evidence base. Roychowdhury et al (2020) commentary in the Journal of Functional Morphology and Kinesiology synthesised the evidence across the entire lifespan, demonstrating that physical activity improves physical, psychological, and social health at every stage of life — from childhood bone development and cognitive function in adolescence through to reduced chronic disease risk, improved metabolic health, and slower cognitive decline in older adults.
Critically, exercise acts on almost every hallmark of biological ageing simultaneously. It preserves mitochondrial function, supports proteostasis (the quality control system for cellular proteins), reduces systemic inflammation, improves insulin sensitivity, and maintains skeletal muscle mass — the very tissue that determines functional independence in later life.
The distinction that matters most, however, is this: exercise has a modest effect on how many total years you live, but a massive effect on how well you live those years. It is, in the words of geroscience, the difference between climbing stairs at 80 and needing a lift. It is the difference between being a participant in your own life and being a passenger.
Exercise as Healthspan Insurance
Think of exercise not as weight loss but as healthspan insurance. Two sessions of resistance training per week, combined with regular aerobic activity achieving a VO2 max appropriate for your age group, represents one of the highest-return investments available to any individual seeking to close their personal healthspan gap.
Part 5: Why Individual Effort Is Not Enough — The Systems Challenge
Von Blanquet (2025), writing in Springer's Innovations in Healthcare and Outcome Measurement, frames the healthspan–lifespan gap as a systems challenge rather than a purely biomedical one. Closing the gap requires not just better medicines or better personal choices — it requires better systems.
Healthcare delivery models remain largely organised around treating disease episodes. A patient arrives with a cardiac event, a cancer diagnosis, or a diabetic crisis; the system mobilises to address that acute episode; and then the patient returns to a life that may be systematically undermining their functional capacity. This is a model optimised for survival, not for thriving.
The regional variation documented by Garmany and Terzic (2025) demonstrates that morbidity compression — keeping the period of significant illness brief relative to total lifespan — is achievable. Some regions have done it. The blueprint exists. The question is whether health systems can align their incentives, measurement frameworks, and resource allocation to follow it.
What would a healthspan-optimised health system look like? It would measure functional capacity and cognitive performance routinely, not just blood pressure and cholesterol. It would invest in preventive interventions that maintain independence rather than solely in acute treatments that prolong biological survival. It would develop standardised healthspan metrics — as the Discover Aging initiative (Crasta et al., 2026) is working toward — that allow progress to be tracked at the population level. And it would recognise, as Liubertas (2026) argues, that experienced longevity — the subjective quality of the years lived — is as legitimate a health outcome as any biomarker.
Your Personal Healthspan Audit
Use this evidence-based checklist during your next medical consultation. These markers help shift the focus from simply preventing disease to preserving strength, independence, cognitive function, and quality of life as you age.
1. Grip Strength
Check whether your grip strength falls within the top 25% for your age and sex.
Low grip strength is strongly associated with increased all-cause mortality, frailty, and reduced functional independence.
2. Gait Speed
Aim for a comfortable brisk walking speed of approximately 1 metre per second.
Slower gait speed is linked to higher risks of disability, hospitalisation, and cognitive decline.
3. Balance Assessment
Test whether you can stand on one leg with eyes open for at least 10 seconds.
Poor balance predicts fall risk and future mobility limitations.
4. VO2 Max (Cardiorespiratory Fitness)
Ask your doctor or fitness professional about VO2 max testing.
VO2 max is one of the strongest physiological predictors of longevity and cardiovascular resilience.
5. HbA1c or Continuous Glucose Monitoring (CGM)
Monitor long-term glucose control and glycaemic variability — not just fasting blood sugar.
Stable glucose levels are essential for metabolic health and healthy ageing.
6. hs-CRP (High-Sensitivity C-Reactive Protein)
Assess for chronic low-grade inflammation.
Elevated hs-CRP is associated with accelerated biological ageing, cardiovascular disease, and metabolic dysfunction.
7. ApoB (Apolipoprotein B)
Consider ApoB testing for a more accurate assessment of cardiovascular risk than total cholesterol alone.
ApoB reflects the number of atherogenic lipoprotein particles driving plaque formation.
8. Sleep Quality
Aim for 7–9 hours of restorative sleep nightly.
Adequate REM and deep sleep are critical for brain health, hormonal regulation, recovery, and immune function.
9. Social Connection
Maintain at least 3 meaningful social relationships with regular weekly interaction.
Social isolation increases inflammation, depression risk, and cognitive decline.
10. Resistance Training
Perform at least 2 sessions of load-bearing or resistance exercise weekly.
Strength training preserves muscle mass, bone density, metabolic health, and long-term independence.
Evidence Summary: Key Studies Shaping the Science of Healthspan
1. Garmany & Terzic (2025) — Communications Medicine
This large-scale global analysis examined health and longevity data from all 183 World Health Organization member states. The researchers found that people worldwide spend an average of 9–10 years living with chronic disease, disability, or reduced functional capacity before death. Importantly, the magnitude of this healthspan–lifespan gap varied substantially across regions and disease patterns, demonstrating that prolonged late-life decline is not biologically inevitable. The findings strongly suggest that healthcare systems, lifestyle factors, preventive medicine, and public health infrastructure can meaningfully influence healthy ageing outcomes.
2. Masfiah et al. (2025) — Ageing Research Reviews
This systematic review identified 113 different published definitions of “healthspan,” exposing a major scientific challenge within ageing research. Some definitions focused on disease-free survival, while others emphasized physical function, cognition, frailty, or subjective wellbeing. The study highlighted the urgent need for standardized, universally accepted healthspan metrics to allow meaningful comparison between studies, accurate tracking of interventions, and effective public health policy planning.
3. Biswas et al. (2026) — eClinicalMedicine
This population cohort study demonstrated that healthy ageing depends on the interaction of multiple lifestyle factors rather than a single intervention alone. Researchers found that achieving minimum combined thresholds of quality sleep, regular physical activity, and adequate nutrition produced measurable improvements in both lifespan and healthspan outcomes. The study reinforced the concept that consistency across foundational lifestyle pillars is more important than perfection in any one domain.
4. Liubertas (2026) — Frontiers in Aging Neuroscience
Liubertas proposed an innovative framework called “experienced longevity,” expanding the concept of healthy ageing beyond biomarkers and disease metrics. The paper argued that emotional wellbeing, social engagement, purpose, and the subjective experience of ageing are biologically meaningful dimensions of longevity. This framework aligns ageing science more closely with psychological resilience, quality of life, and the lived human experience of growing older.
5. Crasta et al. (2026) — Discover Aging
This publication introduced Discover Aging, a multidisciplinary scientific forum dedicated specifically to understanding and improving healthspan. The initiative reflects growing recognition that ageing research requires collaboration across geroscience, neurology, cardiology, metabolism, psychology, public health, and preventive medicine. The launch signals a broader movement toward unified frameworks for measuring and extending healthy years of life.
6. von Blanquet (2025) — Springer Innovations in Healthcare
von Blanquet framed the healthspan–lifespan gap as not merely a biological problem, but a healthcare systems challenge. The paper argued that most modern healthcare models remain focused on treating acute disease episodes rather than preserving long-term functional capacity and independence. The study advocates for redesigned healthcare systems that prioritize prevention, mobility, cognition, frailty reduction, and quality-of-life outcomes alongside traditional disease treatment.
7. Jugran (2025) — Journal of Global Health
Jugran argued that extending lifespan without simultaneously improving healthspan should be viewed as a public health and policy failure. Longer survival accompanied by prolonged multimorbidity creates escalating burdens on healthcare systems, caregivers, and economies. The paper emphasizes that future healthcare priorities must shift toward maintaining physical function, cognitive resilience, and independence rather than focusing exclusively on mortality reduction.
Practical Applications: From Research to Daily Life
The science of healthspan is compelling — but it only matters if it changes behaviour. Here are seven evidence-based steps you can begin today.
1. Reframe Your Health Goals
Stop asking only 'Am I sick?' and start asking 'How is my functional capacity trending?' Request that your doctor assess gait speed, grip strength, and cognitive baseline at routine appointments. These functional metrics predict your trajectory far better than most standard blood tests.
2. Build Your Triple Foundation
Based on the findings of Biswas et al. (2026), prioritise achieving minimum adequate thresholds across all three lifestyle pillars simultaneously. Aim for 7–9 hours of quality sleep, at least 150 minutes of moderate-intensity physical activity per week (including 2 resistance sessions), and a diet with high fibre density, adequate protein, and minimal ultra-processed food.
3. Invest in Muscle Before You Need It
Skeletal muscle is your biological savings account for independence. Every decade of life after 30 brings measurable muscle loss without deliberate resistance training. Start now. Two sessions of progressive load-bearing exercise per week is the evidence-based minimum. Women in particular — given the gendered frailty data — should prioritise this early.
4. Treat Social Connection as a Clinical Intervention
Maintain at least three deep social connections with weekly interaction. Join a community group, volunteer organisation, or structured regular activity with others. Loneliness elevates inflammatory markers as reliably as a poor diet, and its effects on cognitive and cardiovascular health are profound.
5. Know Your Longevity Biomarkers
Move beyond standard annual blood tests. Ask your doctor about hs-CRP (inflammation), ApoB (cardiovascular risk), Cystatin C (kidney reserve), HbA1c or continuous glucose monitoring (metabolic health), and a baseline cognitive screen such as the MoCA. These markers give you an early warning system — years before clinical symptoms appear.
6. Ask the Right Questions in the Consulting Room
When you see your doctor, do not only ask about disease risk. Ask: 'How is my physical function trending compared to my age group? What can we do to preserve my independence over the next decade?' These questions shift the clinical encounter from disease management to healthspan optimisation.
7. Find Your Ikigai
Research consistently shows that a clear sense of purpose — your reason for getting up in the morning — is associated with lower cortisol levels, reduced inflammatory markers, and longer healthspan. Whether it is creative work, community engagement, caregiving, or spiritual practice, cultivating purpose is not a luxury. It is a biological necessity.
Frequently Asked Questions
Q1. What is the simplest way to understand the difference between lifespan, healthspan, and longevity?
Lifespan is how long you live in total. Healthspan is how many of those years you spend in genuine good health — free from significant chronic disease, disability, or functional limitation. Longevity, as the term is now used in science, refers to achieving advanced age while maintaining health and function. You can have a long lifespan but a short healthspan if your final decade is spent managing serious illness and dependency. The goal of modern ageing medicine is to make these three numbers as close together as possible.
Q2. Is the 9-year healthspan gap inevitable, or can it actually be reduced?
The evidence strongly suggests it is not inevitable. The regional variation documented by Garmany and Terzic (2025) across 183 countries demonstrates that some world regions have achieved meaningful compression of morbidity — keeping the period of significant illness relatively brief. The size of the gap reflects differences in healthcare systems, diet, physical activity, social connection, and public health investment — all of which are modifiable. Individual choices matter enormously, and so do the systems that support or undermine those choices.
Q3. Why is healthspan so difficult to measure if it is so important?
Unlike lifespan, which has a single objective endpoint, healthspan is multidimensional. It incorporates biological markers, physical function, cognitive capacity, and subjective quality of life. Cultural context matters too — what constitutes good health varies across populations. A systematic review by Masfiah et al. (2025) found 113 different published definitions, reflecting a profound lack of scientific consensus. New research initiatives such as Discover Aging (Crasta et al., 2026) are working toward standardisation, which is the prerequisite for reliable progress.
Q4. Why do women experience a larger healthspan gap than men, even though they live longer?
Women generally live longer than men but do not spend proportionally more years in good health. The additional years tend to come with higher rates of chronic disease, disability, and frailty. Partly this reflects post-menopausal hormonal shifts that accelerate bone density loss and cardiovascular risk. Partly it reflects historically lower skeletal muscle mass and a reduced baseline reserve of physical capacity. Garmany and Terzic (2025) documented this gap consistently across their global analysis. The practical implication is that women must be especially proactive about strength training, bone health, and cardiovascular monitoring — ideally starting well before menopause.
Q5. What does the new research by Biswas et al. (2026) actually tell us to do differently?
The key insight from the Biswas et al. (2026) population cohort study is that it is the combination of sleep, physical activity, and nutrition — meeting minimum adequate thresholds across all three simultaneously — that drives measurable improvements in both lifespan and healthspan. Previous research often studied these factors in isolation. The practical implication is to resist the temptation to obsessively optimise one domain while neglecting the others. Adequate sleep combined with regular movement and a reasonably nutritious diet produces greater healthspan benefit than perfection in any single domain combined with deficiency in the others.
Q6. What is 'experienced longevity' and why does it matter clinically?
Experienced longevity, as proposed by Liubertas (2026) in Frontiers in Aging Neuroscience, refers to the subjective quality of the conscious ageing experience — the sense of purpose, engagement, emotional richness, and personal meaning that colours the years we live. It matters clinically because the biological mechanisms underpinning positive subjective wellbeing — including lower inflammatory markers, healthier cortisol rhythms, and better cardiovascular function — are real and measurable. Loneliness, purposelessness, and social disengagement are not merely sad; they are biologically damaging in ways that accelerate ageing at a cellular level.
Q7. What should I ask my doctor at my next appointment to start optimising my healthspan?
Shift the conversation from disease risk to functional trajectory. Useful questions include: How is my physical function — grip strength, gait speed, balance — trending compared to others my age? Have we established a cognitive baseline I can track over time? Are any of my current medications affecting my long-term functional capacity? What single change, given my current profile, would most improve my healthspan over the next decade? These questions reorient the clinical encounter toward the outcomes that will determine your quality of life in your later years.
Clinical pearls
1. The "Triple Adequacy" Principle Over Individual Excellence
Clinical Perspective: Data from Biswas et al. (2026) demonstrate that healthspan outcomes are optimized by meeting minimum concurrent thresholds across sleep, physical activity, and nutrition, rather than maximizing a single variable. In clinical terms, a syndemic approach to lifestyle modification implies that the physiological harms of a sedentary state or sleep deprivation cannot be fully compensated for by an isolated, highly optimized dietary intervention.
Patient Perspective: You don’t need to be perfect in any single area to see massive health benefits. Achieving a "B grade" across sleep, exercise, and diet all at once does far more to extend your healthy years than getting an "A+" in diet while failing at sleep and exercise. Consistency across all three pillars beats perfection in just one.
2. Prioritize "Experienced Longevity" to Mitigate Inflammaging
Clinical Perspective: As outlined by Liubertas (2026), subjective well-being and sense of purpose are structural components of conscious aging that directly modulate biological pathways. Chronic isolation and a lack of purpose drive "inflammaging"—elevating systemic inflammatory cytokines like interleukin-6 (IL-6) and C-reactive protein (CRP). Social depth must be treated as a clinical variable on par with metabolic markers.
Patient Perspective: Having a reason to get out of bed and maintaining deep friendships isn't just good for your mood—it’s medicine for your cells. Loneliness causes a silent, low-grade inflammation in the body that accelerates aging just like a poor diet or smoking. Cultivating a hobby or a community group is a vital part of your healthcare plan.
3. Early and Aggressive Muscle Mass Preservation (Especially for Women)
Clinical Perspective: The "Gender Health-Survival Paradox" highlighted by Garmany & Terzic (2025) notes that while women have a longer lifespan, they face a disproportionately wider healthspan gap due to accelerated post-menopausal bone density loss and lower baseline skeletal muscle mass. Preventive geroscience demands early, proactive resistance training interventions to build a functional metabolic and structural reserve before frailty onset.
Patient Perspective: Women tend to live longer than men, but they spend more of those extra years dealing with pain or a loss of independence. Skeletal muscle is your biological savings account. For women especially, lifting weights or doing resistance training twice a week early in life is non-negotiable to protect your bones, keep your metabolism sharp, and ensure you can move freely in your 70s and 80s.
4. Track Functional Biomarkers Over Static Chronological Metrics
Clinical Perspective: Standard metabolic panels (e.g., fasting glucose, total cholesterol) are lagging indicators optimized for episodic disease diagnosis rather than functional preservation. Predictive healthspan monitoring requires tracking functional proxies—such as grip strength, gait speed, and VO2 Max—alongside advanced biomarkers like ApoB and high-sensitivity CRP (hs-CRP) to catch subclinical declines in physiological reserve.
Patient Perspective: Being "disease-free" on a standard blood test is not the same as being truly healthy. Simple physical tests—like how fast you naturally walk, your grip strength, and your balance—are actually better at predicting how long you will stay independent. Ask your doctor to measure how your body is actually functioning, not just whether you meet the criteria for a disease.
5. Shift Care Models from "Disease Suppression" to "Morbidity Compression"
Clinical Perspective: Modern healthcare delivery models inherently default to extending lifespan by treating acute cardiovascular or oncological events without improving the underlying healthspan, resulting in prolonged periods of late-life multimorbidity (Jugran, 2025). Clinicians must pivot toward a framework of "morbidity compression"—using preventive therapeutics and lifestyle intervention to keep the period of chronic illness as brief as possible at the very end of life.
Patient Perspective: The goal of modern medicine shouldn't just be to keep you alive after a major health crisis; it should be to keep you healthy enough so that you don't have the crisis in the first place. We want to squeeze the time you spend dealing with sickness into a very short window at the very end of a long, active life, rather than spending a whole decade managing illness.
6. Combat the Healthspan "Measurement Crisis" with Personalized Baseline Tracking
Clinical Perspective: With over 113 competing definitions of healthspan in the literature (Masfiah et al., 2025), there is no standardized clinical benchmark. Until initiatives like Discover Aging (Crasta et al., 2026) establish unified, validated metrics, clinicians must establish personalized, multidimensional baselines for each patient. This should encompass cognitive performance (e.g., MoCA), cardiovascular fitness (VO2 Max), and glycemic variability (HbA1c/CGM).
Patient Perspective: Because science is still arguing over the exact definition of "healthspan," you have to define and track your own. Work with your doctor to create a personalized health blueprint. By measuring your memory baseline, your cardiovascular fitness, and your blood sugar stability now, you can catch minor deviations and fix them years before they turn into permanent health problems.
Clinician’s Perspective: The Real Goal Is Functional Independence, Not Just Survival
As physicians, we have historically been trained to measure success through survival statistics: lower mortality rates, improved disease control, and longer life expectancy. These are undeniably important achievements. Yet in daily clinical practice, a deeper reality becomes impossible to ignore: many patients are living longer while simultaneously losing strength, mobility, cognitive resilience, and independence. The modern challenge in medicine is no longer simply preventing premature death — it is preventing prolonged decline.
The emerging science of healthspan reframes ageing as a process of functional deterioration that begins decades before disability becomes visible. By the time frailty, sarcopenia, metabolic disease, or cognitive impairment are clinically obvious, the biological processes driving them have often been progressing silently for years. This is why clinicians must increasingly focus on early preservation of physiological reserve rather than late-stage disease management alone.
From a practical standpoint, the most powerful interventions remain remarkably consistent across the literature: regular resistance training, aerobic fitness, restorative sleep, metabolic health optimisation, social engagement, and preservation of muscle mass. In many cases, grip strength, gait speed, balance, and VO2 max predict long-term outcomes more meaningfully than traditional laboratory values alone. The future of preventive medicine will likely rely as much on functional metrics as on biochemical markers.
Equally important is recognising that healthy ageing is multidimensional. Emotional wellbeing, social connection, purpose, and cognitive engagement are not “soft” variables — they exert measurable biological effects through inflammation, stress physiology, and neuroendocrine regulation. Loneliness and inactivity can accelerate biological ageing as profoundly as hypertension or poor nutrition.
The true measure of longevity is not how long the heart continues beating, but how long the human being remains capable of fully participating in life.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Living to 100: Is it Genetics or Lifestyle? What the New Science Says | DR T S DIDWAL
Time-Restricted Eating: Metabolic Advantage or Just Fewer Calories? | DR T S DIDWAL
Can You Revitalize Your Immune System? 7 Science-Backed Longevity Strategies | DR T S DIDWAL
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
Light and Longevity: Can Sunlight Slow Cellular Aging? | DR T S DIDWAL
References
Biswas, R. K., et al. (2026). Minimum combined sleep, physical activity, and nutrition variations associated with lifespan and healthspan improvements: A population cohort study. eClinicalMedicine, 92, Article 103741. https://doi.org/10.1016/j.eclinm.2025.103741
Crasta, K., Deng, L., Chhabra, Y., et al. (2026). Discover Aging: A new multidisciplinary research forum for understanding and improving healthspan. Discover Aging, 1, 1. https://doi.org/10.1007/s44518-026-00002-5
Crimmins, E. M. (2015). Lifespan and healthspan: Past, present, and promise. The Gerontologist, 55(6), 901–911. https://doi.org/10.1093/geront/gnv130
Garmany, A., Yamada, S., & Terzic, A. (2021). Longevity leap: Mind the healthspan gap. npj Regenerative Medicine, 6, Article 57. https://doi.org/10.1038/s41536-021-00169-5
Garmany, A., & Terzic, A. (2025). Healthspan-lifespan gap differs in magnitude and disease contribution across world regions. Communications Medicine, 5, Article 381. https://doi.org/10.1038/s43856-025-01111-2
Jugran, D. K. (2025). Too well to die; too ill to live: An update on the lifespan versus healthspan debate. Journal of Global Health, 15, Article 03022. https://doi.org/10.7189/jogh.15.03022
Kaeberlein, M. (2018). How healthy is the healthspan concept? GeroScience, 40, 361–364. https://doi.org/10.1007/s11357-018-0036-9
Liubertas, T. (2026). Beyond lifespan and healthspan: A biological framework for experienced longevity. Frontiers in Aging Neuroscience, 18, 1815030. https://doi.org/10.3389/fnagi.2026.1815030
Masfiah, S., Kurnialandi, A., Meij, J. J., & Maier, A. B. (2025). Definitions of healthspan: A systematic review. Ageing Research Reviews, 111, Article 102806. https://doi.org/10.1016/j.arr.2025.102806
Olshansky, S. J. (2018). From lifespan to healthspan. JAMA, 320(13), 1323–1324. https://doi.org/10.1001/jama.2018.12621
Roychowdhury, D. (2020). Using physical activity to enhance health outcomes across the life span. Journal of Functional Morphology and Kinesiology, 5(1), 2. https://doi.org/10.3390/jfmk5010002
Seals, D. R., Justice, J. N., & LaRocca, T. J. (2016). Physiological geroscience: Targeting function to increase healthspan and achieve optimal longevity. The Journal of Physiology, 594(8), 2001–2024. https://doi.org/10.1113/jphysiol.2014.282665
von Blanquet, H. M. (2025). The healthy longevity challenge: Closing the gap between lifespan and healthspan. In P. Plugmann & D. Portius (Eds.), Innovations in healthcare and outcome measurement. Springer. https://doi.org/10.1007/978-3-031-77302-0_10