Time-Restricted Eating: Metabolic Advantage or Just Fewer Calories?
New 2025 clinical trials reveal how time-restricted eating compares with calorie restriction for weight loss, insulin sensitivity, blood pressure, and cardiometabolic health.
NUTRITIONOBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/26/202621 min read
Time-restricted eating is comparable but not superior to calorie restriction for weight loss and metabolic health. 2025–2026 randomized trials show TRE works mainly by reducing overall calorie intake and aligning meals with circadian rhythms, with modest additional benefits for blood pressure. The most effective approach is the one you can sustain long-t
Key takeaways
1. TRE’s primary mechanism is caloric reduction, not independent metabolic superiority.
Under isocaloric conditions (identical calorie intake), TRE does not produce meaningfully better cardiometabolic outcomes than calorie restriction, despite clear shifts in peripheral circadian clocks (Peters et al., 2025). The “metabolic advantage” largely disappears when energy intake is controlled.
2. TRE offers modest, specific benefits for blood pressure and endothelial health.
Meta-analyses indicate TRE can reduce systolic blood pressure and improve certain lipid markers even with minimal weight loss, potentially through reduced oxidative stress, sympathetic modulation, and avoidance of late-night eating — effects that are not fully explained by weight loss alone (Yi et al., 2025).
3. Early time-restricted eating (eTRE) has stronger mechanistic support than later windows.
Aligning food intake with peak insulin sensitivity and circadian biology (e.g., 8 AM–4 PM) shows more consistent benefits for insulin dynamics and blood pressure than midday or late TRE, though real-world adherence often favors standard 16:8 protocols.
4. Adherence and individualization are the dominant predictors of long-term success.
Network meta-analyses show that no intermittent fasting strategy is clearly superior to continuous calorie restriction when adherence is matched. TRE frequently demonstrates higher retention rates due to reduced cognitive burden of tracking (Semnani-Azad et al., 2025; Chang et al., 2025).
5. Diet quality within the eating window remains critical.
TRE does not inherently improve dietary quality. Consuming the same calories in a compressed window does not compensate for poor food choices; nutrient density, protein intake, and minimization of ultra-processed foods continue to drive health outcomes (Flynn et al., 2026).
6. Special populations require caution and medical supervision.
While TRE can improve glycemic control in type 2 diabetes and insulin resistance, benefits are mostly mediated by caloric deficit. Risks include hypoglycemia (with certain medications), sarcopenia in older adults, and potential hormonal disruption in women. A 10–12 hour window with adequate protein is generally safer than aggressive protocols in these groups.
Introduction
Every few years, a dietary strategy arrives that promises to make weight loss simpler, smarter, and more sustainable. Right now, time-restricted eating (TRE) — eating all your calories within a defined window of 8 to 12 hours — is that strategy. Its appeal is obvious: no calorie counting, no complicated food rules, just watching the clock.
But does the science back up the hype?
If you've been wondering whether time-restricted eating is genuinely superior to traditional calorie restriction (CR) — or whether it's just another clever way to eat less — you're asking exactly the right question. And in 2025 and 2026, a new wave of clinical trials has finally given us the most rigorous answers yet.
This article breaks down everything you need to know: how TRE works at the cellular level, what the latest randomized controlled trials actually show, who benefits most, who should be cautious, and how to decide which approach is right for your life and biology.
Whether you're managing your weight, trying to improve your blood pressure, or simply looking for a sustainable eating pattern, this is the most complete, evidence-based guide to TRE vs. calorie restriction available in 2026.
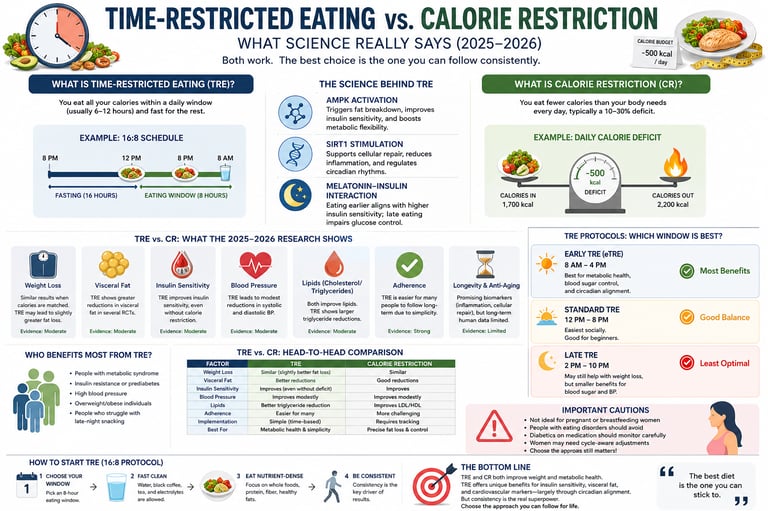
1. What Is Time-Restricted Eating?
Time-restricted eating is an eating pattern in which you consume all of your daily food within a set window — typically 6 to 12 hours — and fast during the remaining hours. Unlike traditional calorie restriction, TRE does not require you to track or limit how much you eat; the intervention is purely about when you eat.
The most popular format is 16:8, where you fast for 16 hours and eat within an 8-hour window (for example, 12:00 PM to 8:00 PM). But as the science has evolved, researchers have identified that not all TRE windows are created equal — the timing of that window matters as much as its length.
Time-restricted eating (TRE) is a dietary approach that limits food consumption to a specific daily window, typically 6–12 hours, without necessarily restricting calories. It is a form of intermittent fasting that works partly by reducing overall calorie intake and partly by aligning eating patterns with the body's natural circadian rhythms.
TRE is also called intermittent fasting with time windows, time-limited eating, or simply "eating in a window." For clarity, this article uses TRE throughout.
2. How TRE Works: The Cellular Mechanisms
Understanding why TRE can affect metabolism requires a brief look under the hood. Three key molecular pathways explain most of its effects:
AMPK Activation: Your Body's Energy Sensor
During a fast, cellular energy levels drop. This activates AMPK (AMP-activated protein kinase) — essentially the body's fuel gauge. When AMPK switches on:
Fat breakdown (lipolysis) accelerates
Liver fat production slows
Insulin sensitivity improves
Mitochondria become more efficient
Think of AMPK activation as flipping your metabolism from "storage mode" into "burn mode." This shift typically begins within 12–14 hours of fasting, which is why shorter windows (say, only 10 hours of fasting) may not activate the same pathways as a 16-hour fast.
SIRT1 Stimulation: Cellular Repair and Rhythm Regulation
Fasting also upregulates SIRT1 (Sirtuin-1), a protein that governs cellular repair, inflammation control, and glucose regulation. SIRT1 works synergistically with AMPK to improve metabolic efficiency and support healthy circadian rhythm signaling — the body's 24-hour internal clock that controls hormone secretion, digestion, and sleep-wake cycles.
The Melatonin–Insulin Interaction: Why Timing Matters
This is where TRE gets genuinely nuanced. Melatonin — the hormone that signals nighttime — rises in the evening and directly suppresses insulin secretion. When you eat late at night, your body is physiologically less equipped to manage the resulting blood sugar rise. Glucose stays elevated longer, and over time this can worsen insulin resistance.
This is the biological rationale for early time-restricted eating (eTRE): by front-loading calories earlier in the day, you align food intake with peak insulin sensitivity, not minimum insulin sensitivity.
3. Types of TRE Protocols: Which Window Is Best?
Not all TRE protocols produce the same results. Here's how the three main formats compare:
Standard 16:8 (12 PM – 8 PM)
The most widely practised format. You skip breakfast and eat from midday until early evening. Social adherence is easier because dinner is included.
Pros: Easy to adopt, fits most social schedules
Cons: Misses morning metabolic peak; evening eating may blunt some benefits
Early TRE / eTRE (8 AM – 4 PM)
The most metabolically studied format in 2025–2026 research. By eating earlier, eTRE aligns food intake with peak insulin sensitivity and AMPK activity.
Pros: Strongest evidence for blood pressure reduction and beta-cell improvement; optimal circadian alignment
Cons: Eliminates dinner, which is socially and practically challenging for most people
Late TRE / lTRE (2 PM – 10 PM)
Accommodates evening social eating by shifting the window later.
Pros: Socially convenient
Cons: Eating close to bedtime may disrupt nocturnal glucose regulation and melatonin signaling; potentially counterproductive for metabolic health
Bottom line: If metabolic optimization is your priority, eTRE has the strongest mechanistic support. If adherence is your priority, standard 16:8 is likely your best bet — because a strategy you follow consistently beats a perfect strategy you abandon.
4. What Is Calorie Restriction?
Calorie restriction is the intentional reduction of total daily energy intake — typically by 500–1,000 calories below your total daily energy expenditure (TDEE) — without triggering malnutrition. It is the most studied dietary intervention for weight loss in the scientific literature, with decades of randomized controlled trial data supporting its efficacy.
CR does not specify when you eat. It can be practiced with three meals, six small meals, or any eating pattern, as long as total calories remain below maintenance.
The primary mechanism is simple: consuming fewer calories than you expend forces the body to draw on stored energy (primarily body fat), resulting in weight loss. Over time, sustained caloric deficits also improve insulin sensitivity, blood pressure, lipid profiles, and inflammatory markers — largely as downstream effects of fat loss itself.
CR's main challenge is adherence. Tracking calories requires sustained cognitive effort, and most people find it difficult to maintain long-term without behavioral support.
5. TRE vs. Calorie Restriction: What the 2025–2026 Research Actually Shows
The past 18 months have produced a landmark body of research on this exact question. Here's a rigorous review of the key studies — and what they really tell us.
Study 1: Parrotta et al. (2025) — TRE as a Practical Alternative
Published in Current Obesity Reports, this systematic narrative review by Parrotta, Colangeli, Scipione, and colleagues examined whether TRE represents a viable alternative to calorie restriction for managing obesity.
Key findings:
TRE reduces the cognitive burden of constant calorie monitoring
It produces comparable short-term weight loss to CR in most trials
Eating within defined windows may synchronize naturally with circadian rhythms, improving hormonal regularity
Long-term efficacy data remain limited
The takeaway: TRE works as a behavioral simplification tool. It's not metabolic magic — it's a psychological strategy that creates a caloric deficit without the arithmetic. For people who find calorie apps stressful or unsustainable, TRE offers a meaningful alternative.
Study 2: Peters et al. (2025) — The Isocaloric Reality Check
This is arguably the most important TRE study of the decade. Published in Science Translational Medicine, Peters, Schwarz, Schuppelius, and colleagues conducted a carefully controlled randomized trial that isolated the effect of meal timing from caloric intake.
The study design: participants in both the TRE group and the control group consumed identical total calories. Only the eating window differed.
Key findings:
TRE does shift peripheral circadian clocks — liver enzymes and other molecular oscillators adjusted to the restricted window
Despite this circadian shift, no improvements in cardiometabolic health were observed in women with overweight when calories were equalized
The "metabolic advantage" of TRE largely disappears when total energy intake is controlled
What this means in plain language: If you eat 2,200 calories in an 8-hour window versus 2,200 calories spread across 16 hours, your weight loss and metabolic outcomes will be essentially the same. The clock shift is real. The metabolic bonus (without a caloric deficit) is not.
This finding directly challenges a common TRE marketing claim: that when you eat matters more than how much you eat. The data say otherwise — at least for cardiometabolic endpoints in the short term.
Study 3: Chang, Heilbronn & Hutchison (2025) — Prevention and Cardiovascular Health
Published in Cell Reports Medicine, this comparative analysis positioned TRE within the broader landscape of cardiovascular disease prevention strategies, including the Mediterranean diet and traditional calorie restriction.
Key findings:
TRE, Mediterranean-style eating, and calorie restriction all produced similar cardiovascular outcomes when adherence was matched
TRE showed specific advantages for blood pressure reduction and lipid profile improvement in some subgroups
No single dietary pattern was clearly superior; individual adherence was the dominant variable
The takeaway: There is no universally "best" diet for heart health. The intervention most likely to succeed is the one the individual can sustain for months and years, not weeks.
Study 4: Yi et al. (2025) — Meta-Analysis of Blood Pressure and Cardiometabolic Markers
Published in Frontiers in Nutrition, Yi, Yan, Daut, and colleagues conducted a systematic review and meta-analysis of randomized controlled trials examining TRE's effects on blood pressure and cardiometabolic markers in non-diabetic adults — specifically excluding caloric restriction.
Key findings:
TRE produced modest but statistically significant reductions in blood pressure
Some improvements in insulin sensitivity and glucose control were observed
A critical caveat: many included studies involved inadvertent caloric reduction even in the "non-calorie-restricted" TRE groups, complicating attribution
Effects were strongest in individuals without diabetes
Significant individual variability suggests that genetics, baseline metabolic health, and adherence all modulate outcomes
The takeaway: TRE does appear to offer real — if modest — benefits for blood pressure and lipid profiles even beyond pure weight loss. But the mechanism is complex, and these benefits are not universal.
Study 5: Semnani-Azad et al. (2025) — Network Meta-Analysis of Intermittent Fasting Strategies
Published in The BMJ, this large-scale network meta-analysis compared multiple intermittent fasting strategies — including TRE, alternate-day fasting, and 5:2 — against continuous calorie restriction and control diets across a wide range of cardiometabolic outcomes.
Key findings:
All intermittent fasting strategies produced modest but meaningful improvements in body weight, fasting glucose, and lipid profiles
No single IF protocol was clearly superior to continuous CR when total caloric intake was accounted for
Adherence rates varied significantly between strategies, with TRE demonstrating among the highest retention rates in longer trials
Study 6: Wu et al. (2026) — TRE for Healthy Lifespan
Published in Frontiers in Medicine, this 2026 review evaluated TRE's potential role in extending healthy lifespan — a newer and more ambitious research direction. While most mechanistic findings are from animal models, early human data suggest that TRE may reduce markers of cellular aging (including inflammatory cytokines and oxidative stress biomarkers) independently of weight loss.
This emerging area positions TRE not just as a weight management tool but as a potential longevity strategy — though much more human evidence is needed before strong claims can be made.
Study 7: Kramer et al. (2026) — TRE in Type 2 Diabetes
Published in the International Journal of Obesity, Kramer, Zinman, Feig, and colleagues examined energy balance regulation in adults with overweight/obesity and type 2 diabetes following TRE protocols.
Key findings:
TRE induced meaningful reductions in energy intake in individuals with T2DM
Improvements in HbA1c and fasting glucose were observed but were proportional to the degree of caloric reduction achieved
Medication timing and hypoglycemia risk remain clinically significant concerns requiring physician supervision
Study 8: Flynn, Parr & Devlin (2026) — Does TRE Improve Diet Quality?
Published in Nutrition Reviews, this systematic review examined whether TRE changes not just how much people eat but what they eat.
Key findings:
TRE does not reliably improve diet quality in humans
Some participants naturally reduced ultra-processed food intake due to shorter eating windows
The quality of the diet within the eating window remains critical and should not be ignored
The practical implication: TRE is not a license to eat whatever you want in 8 hours. Dietary quality still matters enormously for long-term health outcomes.
6. Blood Pressure, Heart Health, and Lipid Profiles
One of TRE's most consistent and interesting findings is its effect on cardiovascular markers — even when weight loss is minimal.
The meta-analysis by Yi et al. (2025) found that TRE can produce modest reductions in systolic blood pressure even in non-diabetic individuals not actively restricting calories. Proposed mechanisms include:
Reduced oxidative stress during fasting periods, lowering endothelial damage
Sympathetic nervous system modulation — fasting appears to reduce sympathetic tone, lowering resting heart rate and blood pressure
Improvements in vascular endothelial function mediated by AMPK and SIRT1 activation
Reduced nighttime eating, which is independently associated with elevated nocturnal blood pressure
For people with prehypertension or borderline high blood pressure who are not yet on medication, TRE may offer a non-pharmacological avenue worth exploring — in consultation with a physician.
7. Who Benefits Most from TRE?
Based on current evidence, TRE appears to provide the most meaningful benefits for:
People who struggle with calorie tracking — TRE's simplicity dramatically lowers cognitive load
Adults with prehypertension — The blood pressure effects are among TRE's most consistent findings
People with insulin resistance who are not yet diabetic — Early TRE in particular shows promise for improving beta-cell function and insulin sensitivity
Individuals with irregular snacking habits — Shortening the eating window naturally eliminates late-night snacking, a common source of excess calories
Those seeking a sustainable long-term approach — The BMJ meta-analysis (Semnani-Azad et al., 2025) found TRE among the highest-retention intermittent fasting strategies
TRE is less well-suited for:
People who prefer dietary flexibility within their eating hours
Those whose work or family schedules make eating windows impractical
Athletes with high protein and calorie needs timed around training
Individuals with a history of disordered eating, for whom rigid eating rules may be harmful
8. Special Populations: What the Research Says
Type 2 Diabetes
TRE can improve fasting glucose and insulin sensitivity in some individuals with T2DM. However, this population requires careful clinical management because:
Sulfonylureas and insulin can cause hypoglycemia during fasting windows
Medication timing often needs to be adjusted
The Kramer et al. (2026) data confirm that benefits are primarily mediated through caloric reduction, not timing per se
Recommendation: Never initiate TRE with T2DM without physician supervision. A shorter eating window (10–12 hours rather than 8) is generally safer as a starting point.
Older Adults (60+)
For adults over 60, TRE presents both opportunities and risks:
Opportunity: Modest weight loss and improvements in insulin sensitivity are achievable
Risk: Extended fasting periods without adequate protein intake can accelerate sarcopenia (muscle wasting), which is already a significant concern in aging
Best practice for older adults:
Use a 10–12 hour eating window rather than 8 hours
Prioritize protein at 1.0–1.2 g/kg body weight per day
Combine TRE with resistance training at least 2–3 times per week
Monitor hydration carefully — aging reduces thirst perception and kidney reserve
Women with PCOS
Polycystic ovary syndrome (PCOS) is characterized by insulin resistance, hyperandrogenism, and irregular menstrual cycles — all of which can be influenced by dietary patterns.
TRE may improve insulin resistance and reduce androgen levels in some women with PCOS
However, excessively long fasting periods can dysregulate cortisol rhythms, potentially worsening both metabolic and reproductive symptoms
An 8–10 hour eating window with consistent mealtimes and balanced macronutrients appears safest
Women with PCOS should work with an endocrinologist or registered dietitian before adopting TRE, given the complexity of hormonal interactions involved.
Pregnant and Breastfeeding Women
TRE is not recommended during pregnancy or breastfeeding. Caloric restriction and extended fasting during these periods can compromise fetal development and milk production. Consult your OB-GYN before making any significant dietary changes.
9. TRE vs. Calorie Restriction: Head-to-Head Comparison
Time-Restricted Eating (TRE)
Primary Mechanism: Restricts food consumption to a specific daily time window (e.g., 16:8), which often reduces overall calorie intake indirectly.
Ease of Adherence: High — requires tracking time rather than logging food or counting calories.
Weight Loss Efficacy: Comparable to Calorie Restriction when the net calorie intake matches.
Circadian Benefits: Yes — actively aligns and shifts peripheral circadian clocks in the body.
Blood Pressure: Shows modest improvements (as highlighted by Yi et al., 2025).
Insulin Sensitivity: Provides modest improvements, with particularly strong benefits seen in early Time-Restricted Eating (eTRE).
Dietary Flexibility: Limited by your daily eating time window.
Social Compatibility: Can be challenging, as it often requires skipping regular social meals.
Long-Term Sustainability: High for motivated individuals who adapt well to routine.
Diet Quality Impact: Minimal — the practice does not inherently improve food choices (Flynn et al., 2026).
Potential Risks: Risk of muscle mass loss (especially in older adults) and hypoglycemia for individuals with Type 2 Diabetes (T2DM).
Best Suited For: People who prefer not to count calories or track their food.
Calorie Restriction (CR)
Primary Mechanism: Directly and intentionally reduces the total daily calorie intake below baseline needs.
Ease of Adherence: Moderate — requires ongoing logging, weighing, and tracking of food.
Weight Loss Efficacy: Well-established with decades of robust clinical and scientific evidence.
Circadian Benefits: No direct or inherent circadian alignment effect.
Blood Pressure: Improves directly as a downstream result of overall weight loss.
Insulin Sensitivity: Improves proportionally to the total amount of weight lost.
Dietary Flexibility: Higher flexibility throughout the day; theoretically, any type of food can fit within the daily calorie allowance.
Social Compatibility: Flexible timing allows for social dining, though managing strict portion sizes can be difficult.
Long-Term Sustainability: Variable — tracking fatigue is a common reason for dropping the protocol over time.
Diet Quality Impact: Heavily dependent on the individual's food choices to maintain health.
Potential Risks: Risk of nutritional deficiencies if the restricted diet is poorly planned.
Best Suited For: People who prefer precise data tracking and control over their food choices.
Key Insight: Peters et al. (2025) confirmed that under isocaloric conditions, TRE does not produce superior cardiometabolic outcomes. Both approaches ultimately achieve results through a caloric deficit.
10. Common Myths and Mistakes About Time-Restricted Eating
Myth 1: "TRE lets me eat whatever I want"
False. The Flynn, Parr & Devlin (2026) systematic review confirmed that TRE does not reliably improve diet quality. Eating 2,000 calories of ultra-processed food in 8 hours will not produce the same health outcomes as 2,000 calories of whole, minimally processed food. Dietary quality remains critically important.
Myth 2: "The later I eat, the worse it is"
Partly true, but nuanced. Late eating does conflict with melatonin signaling and can impair nocturnal glucose regulation. However, the most important variable is total caloric intake. A large, late dinner is problematic mainly if it pushes you into a caloric surplus — not purely because of its timing.
Myth 3: "TRE speeds up my metabolism"
No evidence supports this. Peters et al. (2025) found no metabolic rate advantage in isocaloric TRE. Your total daily energy expenditure is not meaningfully altered by eating window alone.
Myth 4: "I need to fast for 16+ hours to get any benefit"
Not necessarily. Research supports meaningful benefits from 12–14 hour fasting windows, especially for blood pressure and circadian alignment. Starting with 12 hours is both safer and more sustainable for most people.
Myth 5: "TRE will fix my insulin resistance without weight loss"
Unlikely. The Peters et al. (2025) data showed that circadian alignment alone — without caloric reduction — was insufficient to reverse insulin resistance in women with overweight. Fat loss remains the primary driver of insulin sensitivity improvements in overweight individuals.
Mistake 1: Breaking the fast with processed food or sugary drinks
The first meal after a fasting period sets the metabolic tone for the day. Reaching for a pastry or fruit juice creates a rapid glucose spike that can undermine TRE's potential benefits. Prioritize protein, fiber, and healthy fats to break your fast.
Mistake 2: Under-eating protein while practicing TRE
Fitting adequate protein into a compressed eating window requires active planning. Protein needs (typically 1.6–2.2 g/kg/day for active individuals; 1.0–1.2 g/kg/day for older adults) don't decrease just because your eating window does.
Mistake 3: Ignoring sleep timing
Emerging research suggests that the eating window's relationship to your sleep timing matters as much as the window itself. Ideally, your last meal should end at least 2–3 hours before sleep to support nocturnal metabolic processes.
11. How to Start Time-Restricted Eating: A Practical Protocol
Step 1: Audit Your Current Eating Window (Week 1)
Before changing anything, track when you first eat and when you last eat each day for 7 days. Most people are surprised to find their current eating window spans 14–16 hours. Your first goal is simply to compress this.
Step 2: Start with a 12-Hour Window (Weeks 2–3)
If you currently eat between 7 AM and 10 PM (15 hours), move to 8 AM to 8 PM (12 hours). This is the most evidence-supported starting point for metabolic benefits with minimal risk of muscle loss or energy crashes.
Step 3: Decide on Your Window Position (Weeks 4+)
Based on your lifestyle, choose:
eTRE (8 AM – 4 PM): Best for metabolic optimization; challenging socially
Standard 16:8 (12 PM – 8 PM): Best for most people; socially compatible
10:14 (9 AM – 7 PM): A middle-ground option with solid evidence and good adherence
Step 4: Optimize Your First and Last Meals
Break your fast with:
30–40g of protein (eggs, Greek yogurt, cottage cheese, legumes)
Fiber-rich vegetables or fruit
Healthy fats (avocado, olive oil, nuts)
End your eating window with:
A moderate-sized meal (not your largest of the day)
Minimal refined carbohydrates
Ideally finished 2–3 hours before bed
Step 5: Stay Hydrated During the Fast
Water, black coffee, and plain tea are all acceptable during fasting hours and do not break the fast in any metabolically meaningful way. Aim for at least 2–3 liters of fluid daily.
Step 6: Monitor Key Metrics
Track the following every 2–4 weeks:
Body weight (morning, fasted)
Energy levels (1–10 scale)
Sleep quality
Blood pressure (if available)
Fasting glucose (if you have a monitor or periodic blood work)
12. Frequently Asked Questions
Q: Can I lose weight with TRE without counting calories?
Yes — for most people, restricting the eating window naturally reduces total calorie intake by eliminating snacking opportunities. However, Peters et al. (2025) confirmed that when calories are truly equal, TRE does not produce additional weight loss. If weight loss stalls, you may need to assess total intake.
Q: Is time-restricted eating safe long-term?
Current evidence (Parrotta et al., 2025; Yi et al., 2025) suggests TRE is safe for most healthy adults over the medium term. Long-term safety data beyond 12 months remain limited, particularly for special populations. Always consult a physician if you have existing health conditions.
Q: Does TRE affect muscle mass?
In healthy, active adults who consume adequate protein, TRE does not appear to significantly reduce muscle mass compared to unrestricted eating with the same protein intake. However, older adults and those already at low muscle mass should be cautious and prioritize protein and resistance training.
Q: Which is better for blood sugar — TRE or calorie restriction?
Both improve insulin sensitivity and fasting glucose primarily through fat loss. Early TRE (eTRE) may offer additional benefits through circadian alignment of insulin secretion, but the evidence in individuals with existing T2DM is mixed and requires medical supervision.
Q: Can I exercise during my fasting window?
Yes. Many people train in a fasted state without performance detriment, especially for moderate-intensity exercise. High-intensity or strength training sessions may benefit from some pre-workout nutrition. If you feel lightheaded or significantly impaired, schedule your training within or closer to your eating window.
Q: Does TRE affect women differently than men?
Emerging evidence suggests women may experience different hormonal responses to extended fasting. Some women report disrupted menstrual cycles with aggressive fasting protocols. The Peters et al. (2025) study, which focused on women with overweight, found no cardiometabolic benefit from isocaloric TRE — a finding that may not fully generalize to men. More sex-stratified research is needed.
Q: What can I drink during the fast?
Water, plain sparkling water, black coffee, and unsweetened herbal teas are all safe during fasting hours. Avoid any beverages with calories, including milk in coffee, fruit juice, or sweetened beverages. Even diet sodas, while calorie-free, may trigger insulin-related responses in some individuals and are best consumed in moderation.
Q: How long until I see results with TRE?
Most people notice changes in appetite and energy levels within 1–2 weeks. Measurable weight loss typically appears within 4–6 weeks. Blood pressure improvements, where they occur, may take 8–12 weeks to become apparent. Metabolic markers like fasting glucose and lipids generally require 12+ weeks of consistent practice to show meaningful change.
Q: Can TRE help with longevity?
Early mechanistic data are promising. The Wu et al. (2026) review in Frontiers in Medicine found that TRE may reduce oxidative stress markers and inflammatory cytokines associated with cellular aging. However, long-term human longevity data do not yet exist, and most lifespan evidence comes from animal models. TRE may be one component of a longevity-supportive lifestyle, but it is not a proven anti-aging intervention at this time.
Q: Should I try TRE or calorie restriction first?
The Parrotta et al. (2025) and Chang et al. (2025) research both support the same conclusion: the "best" approach is the one you will actually sustain. If you dislike tracking food, start with TRE. If you prefer precise control and flexibility in meal timing, calorie restriction may suit you better. Both are valid, evidence-based strategies.
Q: Is 16:8 the best TRE protocol?
It's the most studied and most socially feasible. However, from a purely metabolic standpoint, eTRE (8 AM – 4 PM) may offer superior benefits for blood pressure and insulin function. The "best" protocol is the one that aligns with your biology, schedule, and social life.
13. Conclusion and Action Steps
The 2025–2026 research has given us a clear, nuanced picture of time-restricted eating — one that cuts through both the hype and the dismissiveness.
Here's what the evidence actually tells us:
TRE works primarily by facilitating a caloric deficit — not through any unique metabolic magic. Peters et al. (2025) demonstrated this conclusively under isocaloric conditions.
TRE's circadian benefits are real — it does shift molecular clocks and improve circadian alignment — but these shifts alone are insufficient to produce cardiometabolic improvements without a concurrent reduction in body fat.
TRE offers modest, meaningful benefits for blood pressure and lipid profiles in non-diabetic adults, even beyond weight loss — an advantage that traditional CR does not clearly replicate.
Diet quality within the eating window matters enormously. TRE is not a license to eat freely.
Adherence is the master variable. The BMJ meta-analysis, the Chang et al. prevention data, and the Parrotta review all reach the same conclusion: the superior dietary strategy is the one the individual can sustain over 12+ months.
Your Action Steps
This week: Track your current eating window for 7 days. Note your first and last bite.
Week 2: Compress your window by 1–2 hours without changing what you eat.
Week 3–4: Choose your target window (12:8 or 16:8) and begin gradually.
Month 2: Optimize your break-fast meal for protein and fiber. Assess energy, sleep, and weight trends.
Ongoing: Consult your physician if you have diabetes, cardiovascular disease, or take medications that require food.
The bottom line: Whether you watch the clock or count calories, consistency is the mechanism. Pick the approach that fits your life — then give it at least 3 months before judging.
Medical Disclaimer
This article is for educational and informational purposes only, reflecting research current as of 2025. It does not constitute medical advice, diagnosis, or treatment. Consult a Professional: Always seek guidance from a physician or registered dietitian before altering your diet or fasting patterns. Specialized medical supervision is mandatory for high-risk individuals, including those who:
Have Type 1 or Type 2 Diabetes (risk of hypoglycemia).
Have a history of disordered eating.
Are pregnant or breastfeeding.
Take medications requiring food (e.g., insulin, NSAIDs).
Have a low BMI or risk of malnutrition.
Related Articles
Lowering Cholesterol with Food: 4 Phases of Dietary Dyslipidemia Treatment | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
References
Chang, Y. J., Heilbronn, L. K., & Hutchison, A. T. (2025). Established dietary interventions and time-restricted eating for cardiovascular disease prevention. Cell Reports Medicine, 6(9), Article 102326. https://doi.org/10.1016/j.xcrm.2025.102326
Cienfuegos, S., Gabel, K., Kalam, F., et al. (2020). Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial. Cell Metabolism, 32(3), 366–378. https://doi.org/10.1016/j.cmet.2020.04.013
Flynn, M. K., Parr, E. B., & Devlin, B. L. (2026). The impact of time-restricted eating on diet quality in humans: A systematic review. Nutrition Reviews, 84(3), 633–645. https://doi.org/10.1093/nutrit/nuaf301
Kramer, C. K., Zinman, B., Feig, D. S., et al. (2026). The effects of time-restricted eating on energy balance regulation in adults with overweight/obesity and type 2 diabetes. International Journal of Obesity. Advance online publication. https://doi.org/10.1038/s41366-026-02042-1
Lowe, D. A., Wu, N., Rohdin-Bibby, L., et al. (2020). Effects of time-restricted eating on weight loss and other metabolic parameters in women and men with overweight and obesity. JAMA Internal Medicine, 180(11), 1491–1499. https://doi.org/10.1001/jamainternmed.2020.4153
Lowe, M. R., Doshi, S. D., Katterman, S. N., & Feig, E. H. (2013). Dieting and restrained eating as prospective predictors of weight gain. Frontiers in Psychology, 4, Article 577. https://doi.org/10.3389/fpsyg.2013.00577
Manoogian, E. N. C., Chow, L. S., Taub, P. R., et al. (2022). Time-restricted eating for the prevention and management of metabolic diseases. Endocrine Reviews, 43(2), 405–436. https://doi.org/10.1210/endrev/bnab027
Parrotta, M. E., Colangeli, L., Scipione, V., et al. (2025). Time restricted eating: A valuable alternative to calorie restriction for addressing obesity? Current Obesity Reports, 14, Article 17. https://doi.org/10.1007/s13679-025-00609-z
Peters, B., Schwarz, J., Schuppelius, B., et al. (2025). Intended isocaloric time-restricted eating shifts circadian clocks but does not improve cardiometabolic health in women with overweight. Science Translational Medicine, 17(822). https://doi.org/10.1126/scitranslmed.adv6787
Ravussin, E., Beyl, R. A., Poggiogalle, E., et al. (2019). Early time-restricted feeding reduces appetite and increases fat oxidation but does not affect energy expenditure in humans. Obesity, 27(8), 1244–1254. https://doi.org/10.1002/oby.22518
Semnani-Azad, Z., Khan, T. A., Chiavaroli, L., et al. (2025). Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: Systematic review and network meta-analysis. BMJ, 389, Article e082007. https://doi.org/10.1136/bmj-2024-082007
Sutton, E. F., Beyl, R., Early, K. S., et al. (2018). Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metabolism, 27(6), 1212–1221. https://doi.org/10.1016/j.cmet.2018.04.010
Wilkinson, M. J., Manoogian, E. N. C., Zadourian, A., et al. (2020). Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metabolism, 31(1), 92–104. https://doi.org/10.1016/j.cmet.2019.11.004
Wu, H., Shi, Y., Wang, Z., et al. (2026). Time-restricted eating as a potential strategy for healthy lifespan: An evaluation of current evidence. Frontiers in Medicine, 12, Article 1701888. https://doi.org/10.3389/fmed.2025.1701888
Yi, X., Yan, J., Daut, U. N., et al. (2025). Effects of time-restricted eating without caloric restriction on blood pressure and cardiometabolic profile in non-diabetic adults: A systematic review and meta-analysis. Frontiers in Nutrition, 12, Article 1631477. https://doi.org/10.3389/fnut.2025.1631477