Sympathetic Overactivity: How Stress Reduces Blood Flow, Harms Heart Health, and Promotes Insulin Resistance
Explore how sympathetic nervous system overactivity links chronic stress to heart dysfunction, reduced muscle blood flow, and insulin resistance.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/15/202624 min read
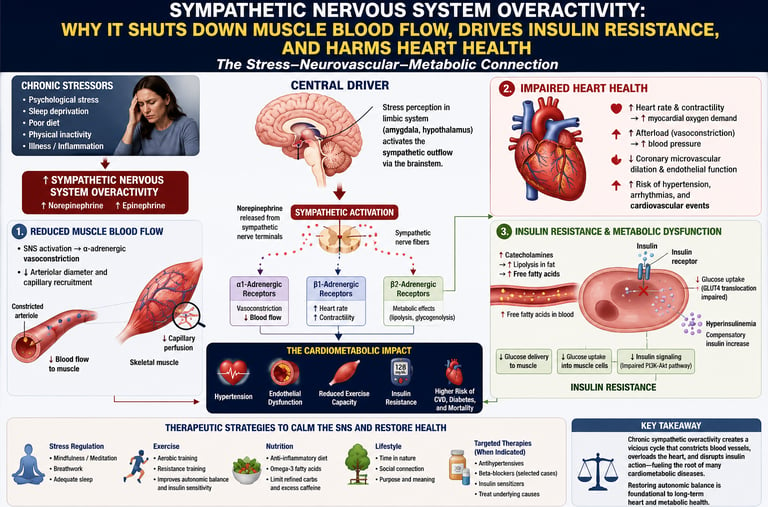
Sympathetic nervous system (SNS) overactivity is a chronically elevated “fight-or-flight” state where your body’s stress nerves never fully switch off. It damages the heart by raising blood pressure, thickening the heart wall, promoting inflammation in blood vessels, and lowering heart rate variability. Major drivers include visceral belly fat, obstructive sleep apnea, chronic stress, and type 2 diabetes. You can lower SNS tone with 150–300 minutes of aerobic exercise per week, slow-paced breathing, 7–9 hours of sleep, weight loss, and treatment for sleep apnea. American Heart Association recommends lifestyle changes as first-line therapy for autonomic imbalance.
How to lower sympathetic nervous system overactivity:
1. Exercise 150+ min/week: Aerobic training reduces resting sympathetic tone and improves HRV.
2. Slow breathing 10 min/day: 4.5–6 breaths per minute activates the baroreflex and boosts parasympathetic activity.
3. Treat sleep apnea: CPAP therapy cuts 24-hour catecholamines and lowers blood pressure.
4. Lose visceral fat: Even 5–10% weight loss reduces leptin-driven sympathetic outflow.
5. Limit sodium & alcohol: Both directly activate the SNS and RAAS system.
6. Manage stress: MBSR, yoga, and CBT lower sympathetic biomarkers in clinical trials.
Key Takeaways
1. A Hidden Driver of Cardiovascular Disease
Persistently elevated sympathetic tone causes systemic damage long before traditional blood tests flag a problem. Chronic SNS overactivity:
Damages the endothelial lining of blood vessels.
Triggers chronic vascular inflammation.
Accelerates atherosclerosis (plaque buildup in arteries).
2. Causes Cardiac Remodeling and Fatal Arrhythmias
Sustained exposure to high levels of norepinephrine physically alters the structure of the heart and disrupts its electrical stability.
Left Ventricular Hypertrophy thickens and stiffens the walls of the heart’s main pumping chamber.
Arrhythmia Risk: Lowers the threshold for dangerous heart rhythms, significantly increasing the risk of sudden cardiac death (SCD).
3. The Root Cause of Resistant Hypertension
SNS overactivity is a primary mechanism behind high blood pressure and a leading reason why some cases become resistant to standard medications. It raises blood pressure by:
Increasing resting heart rate and constricting blood vessels.
Activating the kidney's renin-angiotensin-aldosterone system (RAAS) causes fluid retention.
Blunting baroreflex sensitivity (the body's natural blood pressure regulation system).
4. The Vicious Cycle of Visceral Fat and SNS Flow
Belly fat acts as an active neuroendocrine organ, creating a feedback loop that worsens cardiovascular health.
Visceral fat releases excess leptin and inflammatory adipokines, which signal the brain to increase sympathetic outflow.
In turn, elevated SNS activity promotes further visceral fat storage and prevents its breakdown.
[Visceral Fat Accumulation] ➔ [Excess Leptin & Adipokines] ➔ [Brain Signals SNS Outflow] ➔ [Increased Fat Storage]
5. Worsens Type 2 Diabetes via 4 Metabolic Pathways
Chronic sympathetic dominance directly impairs glucose metabolism and insulin sensitivity through four distinct pathways:
Suppressed Insulin: Inhibits insulin secretion from the pancreas.
Insulin Resistance: Reduces blood flow to skeletal muscles, preventing glucose uptake.
Hepatic Glucose Output: Signals the liver to release excess glucose into the bloodstream.
Elevated Free Fatty Acids: Stimulates lipolysis (fat breakdown), which further drives insulin resistance.
6. Low Heart Rate Variability (HRV) Signals High SNS Tone
Because you cannot easily measure norepinephrine at home, clinicians look to specific biomarkers of autonomic dysfunction:
Low HRV: A consistently low Heart Rate Variability is the most accessible non-invasive marker of sympathetic dominance.
Elevated Resting Heart Rate: An RHR consistently over 80–85 bpm.
Blood Pressure Volatility: Excessive, erratic swings in daily blood pressure readings.
7. Exercise Safely Lowers Sympathetic Tone
Physical activity is the most potent lifestyle intervention to restore autonomic balance, boost parasympathetic (rest-and-digest) tone, and lower plasma norepinephrine.
Aerobic Exercise: 150–300 minutes per week of moderate-intensity cardio improves baroreflex sensitivity.
HIIT & Resistance Training: Highly effective when properly programmed.
Resonant Breathing: Slow, controlled breathing at 4.5–6 breaths per minute acutely downregulates the SNS.
8. Sleep Apnea and Chronic Stress are Major Amplifiers
Unaddressed sleep disorders and psychological stress act as 24/7 accelerators of sympathetic drive.
Obstructive Sleep Apnea (OSA): Every oxygen drop during an apnea episode triggers a massive SNS surge. CPAP therapy directly mitigates this risk.
Mind-Body Interventions: 7–9 hours of quality sleep, Mindfulness-Based Stress Reduction (MBSR), yoga, and Cognitive Behavioral Therapy (CBT) measurably reduce sympathetic biomarkers and improve HRV within weeks.
There is a storm brewing inside millions of people's bodies right now — and most of them have no idea it's happening.
It doesn't show up on a standard blood panel. Your doctor may not test for it. Yet according to a growing body of research published in top journals like Circulation Research, Nature Reviews Endocrinology, and Frontiers in Neuroscience, chronically elevated sympathetic nervous system (SNS) tone may be one of the most significant, underrecognized contributors to heart disease, hypertension, type 2 diabetes, and early death.
This article will show you exactly what sympathetic overactivity is, why it silently damages your heart and metabolic health over years or decades, which lifestyle and medical factors drive it, and — critically — what you can do to bring your nervous system back into balance.
By the end, you'll understand your body in a way most people never do, and you'll have a science-backed roadmap to protect your cardiovascular system from the inside out.
What you'll learn:
What the sympathetic nervous system does and why chronic activation is dangerous
How SNS overactivity causes hypertension, heart disease, and type 2 diabetes
The adipose tissue–brain axis: how body fat keeps your SNS stuck in "on" mode
Which neurotransmitters are involved and how they damage blood vessels
Practical, evidence-based strategies to lower sympathetic tone and protect your heart
1. What Is Sympathetic Nervous System Overactivity?
Your autonomic nervous system (ANS) controls all the bodily processes you don't consciously think about — heart rate, blood pressure, digestion, breathing rate, and much more. It has two main branches:
The sympathetic nervous system (SNS): Your "fight-or-flight" system. It accelerates heart rate, constricts blood vessels, raises blood pressure, and prepares you to respond to perceived threats.
The parasympathetic nervous system (PNS): Your "rest-and-digest" system. It slows the heart, lowers blood pressure, and facilitates recovery.
In a healthy body, these two systems work in dynamic balance. The SNS fires up when you need it — during exercise, stress, or danger — and then the PNS restores calm.
The problem arises when the SNS never fully switches off.
In a significant portion of the population — particularly those with obesity, hypertension, type 2 diabetes, obstructive sleep apnea, or chronic psychological stress — the sympathetic system remains tonically elevated. This is what researchers call sympathetic overactivity or elevated sympathetic tone.
Key definition: Sympathetic overactivity refers to a chronically elevated baseline state of sympathetic nervous system activity, characterized by increased norepinephrine spillover into the bloodstream, elevated heart rate, reduced heart rate variability (HRV), and heightened vascular resistance — even at rest.
According to a 2026 review in Frontiers in Neuroscience by Varzideh et al., autonomic neurotransmission plays a central regulatory role in cardiovascular physiology, and dysregulation of this system underpins a wide spectrum of cardiovascular diseases.
2. How Chronic SNS Activation Damages the Heart
When your sympathetic nervous system is activated acutely — say, during a sprint or a near-miss car accident — it serves a vital purpose. Your heart pumps harder, blood flow increases to muscles, and you're ready to act.
But when this state persists 24 hours a day, 7 days a week, year after year, the cumulative damage is profound.
Cardiac Remodeling
Sustained SNS activation leads to left ventricular hypertrophy (LVH) — a thickening of the heart's main pumping chamber. This initially seems like an adaptation, but over time it stiffens the heart wall, impairs filling, reduces output, and dramatically increases the risk of heart failure and arrhythmias.
A landmark 2025 paper in Circulation Research by Ziegler, Engelhardt, Carnevale, McAlpine, Guzik, Dimmeler, and Swirski laid out in detail how neural mechanisms — including sympathetic overdrive — directly govern cardiovascular health and contribute to the pathophysiology of heart disease at the cellular and systems level.
Arrhythmias and Sudden Cardiac Death
Chronic norepinephrine excess sensitizes cardiac tissue, lowering the threshold for dangerous arrhythmias including ventricular tachycardia and fibrillation. The heart, constantly stimulated, becomes electrically unstable. This is one reason why psychological stress and sleep deprivation — both potent SNS activators — are strongly associated with increased rates of sudden cardiac death.
Accelerated Atherosclerosis
SNS overactivity promotes vascular inflammation. Norepinephrine stimulates the production of pro-inflammatory cytokines and reactive oxygen species (ROS) in blood vessel walls, which accelerates the formation of arterial plaques. Over time, these plaques narrow the arteries and raise the risk of heart attack and stroke.
Endothelial Dysfunction
The endothelium — the thin inner lining of your blood vessels — is exquisitely sensitive to sympathetic tone. Chronic SNS activation reduces the availability of nitric oxide (NO), the molecule that keeps vessels relaxed, flexible, and dilated. Less NO means stiffer, narrower arteries — a setup for hypertension and cardiovascular events.
In short: Your heart and blood vessels are not designed for perpetual "fight-or-flight." When pushed into it chronically, they wear out faster.
3. The SNS–Hypertension Connection
High blood pressure (hypertension) is the world's leading modifiable cardiovascular risk factor, affecting roughly 1.3 billion adults globally. And the sympathetic nervous system is deeply implicated in both its development and its persistence.
A comprehensive 2024 state-of-the-art review by Grassi and Drager in Current Medical Research and Opinion documented that sympathetic overactivity is:
A primary driver of hypertension onset
A key factor in making hypertension resistant to treatment
Independently associated with worse cardiovascular outcomes beyond blood pressure levels alone
The mechanism is multi-pronged:
Increased heart rate and cardiac output: The SNS tells the heart to beat faster and harder, directly raising systolic blood pressure.
Vasoconstriction: Norepinephrine binds to alpha-1 receptors in blood vessel walls, causing them to narrow — raising peripheral vascular resistance and diastolic blood pressure.
Sodium and water retention: The SNS activates the renin-angiotensin-aldosterone system (RAAS), causing the kidneys to retain sodium and fluid, increasing blood volume and pressure.
Reduced baroreflex sensitivity: Chronic SNS overactivity blunts the body's natural blood pressure regulatory reflexes, making hypertension harder to control.
Resistant Hypertension: The SNS Problem
In many patients whose blood pressure doesn't respond to multiple medications, the underlying culprit is persistent SNS overactivity. This has spurred interest in interventional therapies like renal denervation — a catheter-based procedure that disrupts sympathetic nerves to the kidneys — as a treatment for resistant hypertension.
4. Adipose Tissue as a Neuroendocrine Hub
One of the most exciting and paradigm-shifting areas in cardiovascular medicine right now is the recognition that fat tissue — especially visceral (belly) fat — is not metabolically inert. It is a highly active neuroendocrine organ that actively communicates with both the brain and the sympathetic nervous system.
A landmark 2026 review in Nature Reviews Endocrinology by Tsuji and Tseng, titled "Adipose tissue as a humoral–neuronal hub in metabolic regulation," describes adipose tissue as a key node in a bidirectional communication network between peripheral metabolic organs and the central nervous system
What This Means in Practice
visceral fat dysregulates this hub in several ways:
Increased leptin signaling: Visceral fat produces leptin, a hormone that — in excess — chronically activates hypothalamic sympathetic outflow. Leptin resistance, common in obesity, paradoxically keeps SNS tone elevated.
Adipokine imbalance: Visceral fat secretes pro-inflammatory adipokines (like resistin and TNF-α) that activate sympathetic afferent nerves and drive central sympathoexcitation.
Reduced adiponectin: Adiponectin, a protective adipokine, suppresses SNS activity. Visceral obesity reduces adiponectin levels, removing this brake.
Sympathetic innervation of adipose tissue: Fat depots are richly innervated by sympathetic nerves. Chronic SNS activation promotes further visceral fat accumulation, creating a vicious feedback loop.
The key takeaway: Visceral fat and sympathetic overactivity amplify each other. Reducing one helps break the cycle.
5. SNS Overactivity and Type 2 Diabetes
The connection between sympathetic nervous system overactivity and type 2 diabetes is increasingly recognized as a core pathophysiological link — not just a correlation, but a causal relationship operating through multiple biological pathways.
A 2026 commentary in Diabetes, Obesity and Metabolism by Dr. Ralph DeFronzo — one of the world's foremost diabetes researchers — made a striking case: that chronically elevated sympathetic tone is a significant, common, and poorly recognized contributor to cardiometabolic disease in type 2 diabetes. He argued it deserves far more clinical attention than it currently receives.
Mechanisms Linking SNS Overactivity to T2DM
1. Impaired insulin secretion Sympathetic nerve terminals innervate the pancreatic islets. Chronic norepinephrine release suppresses beta-cell insulin secretion via alpha-2 adrenergic receptors, contributing to relative insulin deficiency.
2. Insulin resistance SNS-driven vasoconstriction reduces blood flow to skeletal muscle — the primary site of glucose disposal. Less blood flow means less insulin and glucose delivery to muscle, worsening insulin resistance. Additionally, catecholamines directly impair insulin signaling at the cellular level.
3. Hepatic glucose overproduction Elevated sympathetic tone signals the liver to produce and release more glucose via glycogenolysis and gluconeogenesis, raising fasting blood sugar.
4. Adipose tissue lipolysis SNS activation promotes fat breakdown (lipolysis), flooding the bloodstream with free fatty acids. Elevated FFA levels worsen insulin resistance in muscle and liver, further driving the diabetes cycle.
Key takeaway: In type 2 diabetes, treating the SNS overactivity — not just the blood sugar — may be critical to improving long-term cardiometabolic outcomes.
6. Neurotransmitters Involved: Norepinephrine, Epinephrine, and Beyond
When the SNS fires, it does so primarily through the release of specific chemical messengers. Understanding these neurotransmitters helps explain both how SNS overactivity harms the cardiovascular system and how it can be measured and treated.
Norepinephrine (Noradrenaline)
Norepinephrine (NE) is the primary neurotransmitter of sympathetic nerve terminals in the heart and blood vessels. It binds to:
Alpha-1 receptors: Causing vasoconstriction (raised blood pressure)
Beta-1 receptors: Causing increased heart rate and contractility
Beta-2 receptors: Causing relaxation of some vascular beds and airway dilation
In chronic SNS overactivity, NE "spillover" into the bloodstream is elevated. Plasma norepinephrine levels are used as a marker of sympathetic activity in research settings.
Epinephrine (Adrenaline)
Released primarily from the adrenal medulla, epinephrine amplifies the sympathetic response — particularly in acute stress. In chronically stressed or sleep-deprived individuals, adrenal output can remain persistently elevated.
Neuropeptide Y (NPY)
Co-released with norepinephrine from sympathetic nerve terminals, NPY potentiates vasoconstriction, promotes vascular smooth muscle growth, and has additional pro-inflammatory effects. Elevated NPY is increasingly linked to cardiovascular disease progression.
The 2026 Frontier: Beyond Classical Neurotransmitters
A 2026 paper in Frontiers in Neuroscience (Varzideh et al.) reviews how the spectrum of autonomic neurotransmission extends well beyond classical catecholamines to include purines, peptides, and gasotransmitters — all of which contribute to cardiovascular regulation and, when dysregulated, to disease. This emerging picture underscores how complex and multifaceted the SNS–cardiovascular disease relationship truly is.
7. Critical Insights: Mechanisms, Drivers, and Consequences of SNS Overactivity
Sympathetic overactivity doesn't affect everyone equally. Several well-established risk factors dramatically increase baseline SNS tone:
1. The Invisible Driver of Endothelial Injury
Chronic sympathetic nervous system (SNS) overactivity acts as a silent catalyst for cardiovascular disease long before standard clinical markers flag a problem. Sustained sympathetic tone directly damages the delicate endothelial lining of blood vessels, triggers systemic vascular inflammation, and accelerates the development of atherosclerosis.
2. Pathological Cardiac Remodeling & Arrhythmia Risk
Persistent exposure to elevated plasma norepinephrine levels alters the physical architecture and electrical stability of myocardium. This chronic stimulation drives Left Ventricular Hypertrophy (LVH)—thickening and stiffening the walls of the main pumping chamber—while simultaneously lowering the threshold for dangerous ventricular arrhythmias and sudden cardiac death (SCD).
3. The Engine Behind Resistant Hypertension
Sympathetic overactivity is a primary driver of essential and medication-resistant hypertension. It chronically elevates blood pressure via a multi-pronged mechanism: increasing resting heart rate, inducing peripheral vasoconstriction, blunting baroreflex sensitivity, and activating the renal renin-angiotensin-aldosterone system (RAAS) to promote fluid retention.
4. The Visceral Obesity Feedback Loop
Visceral fat acts as a highly active neuroendocrine organ rather than a passive energy storage site. Excess visceral adiposity drives leptin resistance and alters adipokine secretion, which directly signals the brain to increase central sympathetic outflow. This elevated SNS tone, in turn, favors further visceral fat deposition and impairs lipolysis.
5. Hypoxia-Driven Surges in Obstructive Sleep Apnea (OSA)
Obstructive Sleep Apnea serves as a severe, repetitive trigger for autonomic dysfunction. Every individual nocturnal airway collapse causes intermittent hypoxia, which provokes an immediate, massive sympathetic surge. Over time, these repetitive nighttime spikes spill over into the daytime, causing sustained, 24-hour sympathoexcitation.
6. Four-Way Metabolic Disruption in Type 2 Diabetes
The relationship between SNS tone and metabolic dysfunction is highly bidirectional. Chronic sympathetic dominance directly impairs glucose homeostasis through four distinct pathways:
Suppression of pancreatic insulin secretion.
Reduction of skeletal muscle blood flow (driving peripheral insulin resistance).
Stimulation of hepatic glucose output.
Acceleration of lipolysis, which floods the circulation with free fatty acids.
7. Renal Afferent Signaling in Chronic Kidney Disease (CKD)
The kidneys are critical players in central autonomic regulation. Ischemic, inflamed, or damaged renal tissue activates renal afferent pathways, which transmit stress signals back to the central nervous system. This direct feedback loop drives profound, systemic central sympathoexcitation, worsening both renal and cardiovascular outcomes.
8. Maladaptive Neurohormonal Activation in Heart Failure
In the failing heart, the SNS is initially recruited as a vital short-term compensatory mechanism to maintain cardiac output and tissue perfusion. However, sustained, long-term sympathetic activation becomes highly pathological, accelerating myocardial apoptosis, worsening remodeling, and increasing mortality.
9. Central Neurocircuitry Dysregulation in Anxiety and Depression
Psychological health directly manifests in autonomic tone. Chronic psychological stress, anxiety, and clinical depression cause persistent dysregulation of central neurocircuitry. This leads to the sustained co-activation of the hypothalamic-pituitary-adrenal (HPA) axis and peripheral sympathetic pathways, stripping away the body's baseline resilience.
10. Nutritional Amplifiers: High Sodium and Volumetric Stress
Dietary factors significantly modulate autonomic tone. A high-sodium diet causes transient volume overload and triggers central nervous system salt-sensitive pathways. This activates both the systemic RAAS and sympathetically mediated vasoconrictive responses, compounding vascular stiffness.
11. Chemical Drivers: Nicotine and Alcohol Abuse
Exogenous substances serve as potent chemical triggers for autonomic imbalance. Nicotine acts as a direct, immediate agonist that stimulates central and peripheral norepinephrine release. Conversely, heavy alcohol intake causes acute sympathetic spikes while progressively blunting the nocturnal parasympathetic (vagal) recovery necessary for cardiovascular tissue repair.
12. Diagnostic Markers and Targeted Lifestyle Reversal
Autonomic status can be effectively tracked and modulated without invasive testing:
Biomarkers: Low Heart Rate Variability (HRV), an elevated resting heart rate (>80–85 bpm), and high blood pressure volatility are clear clinical indicators of sympathetic dominance.
Interventions: Regular aerobic exercise (150–300 min/week) and resistance training restore baroreflex sensitivity and boost vagal tone. This can be acutely complemented by resonant breathing (4.5–6 breaths/min) and targeted sleep interventions (like CPAP therapy) to rapidly lower sympathetic biomarkers.
Sympathetic Nervous System Overactivity, Longevity, and Biological Aging
Emerging research suggests that chronic sympathetic nervous system (SNS) overactivity may not only increase the risk of cardiovascular disease but may also accelerate the biological aging process itself. While aging is influenced by genetics, environment, and lifestyle, persistent activation of the body's "fight-or-flight" system appears to amplify many of the cellular mechanisms associated with age-related decline.
When sympathetic activity remains chronically elevated, the body is exposed to sustained increases in catecholamines such as norepinephrine and epinephrine. Over time, this contributes to oxidative stress, vascular inflammation, endothelial dysfunction, insulin resistance, and impaired mitochondrial function—hallmarks that are closely linked to accelerated biological aging. Elevated sympathetic tone has also been associated with reduced heart rate variability (HRV), a marker of diminished autonomic resilience that predicts cardiovascular events, frailty, and all-cause mortality.
The blood vessels may be particularly vulnerable. Chronic SNS activation promotes arterial stiffness, increases blood pressure variability, and accelerates atherosclerotic plaque development. These vascular changes can impair blood flow to critical organs, including the brain, heart, and kidneys, contributing to the gradual decline in physiological function that characterizes aging.
8. How to Measure Sympathetic Tone
Unlike cholesterol or blood sugar, sympathetic nervous system activity isn't routinely measured in clinical practice. However, several tools are used in research and some clinical settings:
Heart Rate Variability (HRV)
HRV measures the natural variation in time intervals between heartbeats. Low HRV is a reliable proxy for high sympathetic tone and reduced parasympathetic activity. It can be measured with:
ECG in a hospital or clinic (gold standard)
Wearable devices (Garmin, Oura Ring, Polar, Apple Watch — all reasonable for trends)
Smartphone apps using camera-based photoplethysmography (less accurate but accessible)
A consistently low resting HRV — particularly the RMSSD metric — is associated with elevated sympathetic activity and poorer cardiovascular outcomes.
Resting Heart Rate
While a crude measure, a persistently elevated resting heart rate (above 80–85 bpm) is associated with higher SNS tone and independently predicts cardiovascular mortality.
Plasma Norepinephrine / Catecholamines
Used in research settings; elevated plasma NE spillover indicates increased sympathetic firing. Can also be measured in 24-hour urine collections.
Muscle Sympathetic Nerve Activity (MSNA)
The gold-standard research tool — a microneurography technique involving electrode recording directly from peripheral sympathetic nerve fascicles. Highly accurate but invasive and available only in specialized labs.
Blood Pressure Variability
Excessive variability in blood pressure across measurements (or between visits) is another indicator of sympathetic dysregulation and baroreflex impairment.
9. Evidence Summary: Key Studies
The Humoral–Neuronal Adipose Hub (Tsuji & Tseng, Nature Reviews Endocrinology, 2026)
Establishes that adipose tissue acts as a highly active, bidirectional humoral–neuronal hub. It plays a central role in concurrently regulating systemic metabolic homeostasis and central sympathetic tone.
The Cardiometabolic Impact in Diabetes (DeFronzo, R.A., Diabetes, Obesity and Metabolism, 2026)
Demonstrates that chronically elevated SNS tone is a significant, common, and frequently underappreciated pathological driver of cardiometabolic disease progression in individuals with Type 2 Diabetes.
The Sustained Driver of Vascular Resistance (Grassi & Drager, Current Medical Research and Opinion, 2024)
Confirms that sympathetic overactivity acts as a primary initiator and sustainer of essential hypertension, serving as an independent predictor of adverse long-term cardiovascular outcomes.
Autonomic Pathophysiology & Regulation (Varzideh et al., Frontiers in Neuroscience, 2026)
Provides a comprehensive analysis of autonomic neurotransmission, mapping out its precise role in both baseline cardiovascular regulation and downstream clinical pathophysiology.
Cellular and Systems-Level Neural Mechanisms (Ziegler et al., Circulation Research, 2025)
Identifies that neural mechanisms—with a specific emphasis on sympathetic pathways—are foundational to cardiovascular health and disease across both isolated cellular levels and integrated systems-level tracking.
Study limitations to note: Many mechanistic studies are performed in animal models or small human cohorts. Measuring SNS activity precisely in large population studies remains challenging. Nevertheless, the convergence of evidence from multiple methodologies and research groups is compelling.
10. How to Lower Sympathetic Nervous System Overactivity
This is where science meets real life. The good news: there are multiple well-evidenced, practical strategies to reduce SNS tone — many of them free and immediately accessible.
A. Exercise: The Most Powerful Tool
Regular aerobic exercise is the single most robustly studied intervention for reducing chronic sympathetic tone. The mechanisms include:
Improved baroreflex sensitivity (your body gets better at auto-regulating blood pressure)
Increased parasympathetic tone at rest (higher resting HRV)
Reduced plasma norepinephrine at matched workloads
Weight loss, which reduces leptin-driven sympathoexcitation
What the evidence recommends:
Aerobic exercise: 150–300 minutes per week of moderate intensity (brisk walking, cycling, swimming) — the backbone of SNS reduction
Resistance training: 2–3 sessions per week — independently beneficial for blood pressure and insulin sensitivity
High-Intensity Interval Training (HIIT): Emerging evidence suggests HIIT produces faster improvements in HRV and autonomic balance than moderate continuous exercise for equivalent time investment
⚠️ Safety note: If you have existing heart disease, hypertension, or diabetes, consult your physician before starting a new exercise program.
B. Stress Reduction and Mind-Body Practices
Chronic psychological stress is one of the most potent drivers of sustained SNS activation. Interventions with robust evidence include:
Mindfulness-Based Stress Reduction (MBSR) Multiple randomized controlled trials show that 8-week MBSR programs significantly reduce blood pressure, improve HRV, and lower sympathetic biomarkers.
Slow-Paced Breathing / Resonance Frequency Breathing Breathing at approximately 4.5–6 breaths per minute maximally stimulates the baroreflex and dramatically shifts the autonomic balance toward parasympathetic dominance. Even 10 minutes daily produces measurable HRV improvements.
Yoga and Tai Chi Both combine slow breathing, gentle movement, and meditation — a triple autonomic intervention. Meta-analyses support clinically meaningful reductions in resting blood pressure and sympathetic tone.
Cognitive Behavioral Therapy (CBT) For those with anxiety and depression — major SNS amplifiers — CBT has demonstrated downstream improvements in autonomic and cardiovascular metrics.
C. Sleep Optimization
Obstructive sleep apnea (OSA) is one of the most powerful drivers of sympathetic overactivity known. Each apneic episode — during which breathing stops and oxygen drops — triggers an acute SNS surge. Repeated hundreds of times per night, this creates a state of persistent daytime sympathetic elevation.
CPAP therapy for OSA significantly reduces 24-hour urinary catecholamines, lowers blood pressure, and improves HRV
Optimizing sleep duration to 7–9 hours reduces both cortisol and catecholamine profiles
Reducing late-night blue light exposure and maintaining consistent sleep-wake timing improves parasympathetic recovery during sleep
D. Dietary Strategies
Specific dietary patterns and nutrients directly modulate sympathetic activity:
The Mediterranean Diet Framework
Autonomic Impact: Down-regulates central sympathetic tone and reduces the secretion of circulating inflammatory adipokines.
Evidence Level: Strong (supported by multiple randomized controlled trials).
High Sodium Intake
Autonomic Impact: Activates the systemic RAAS and central, salt-sensitive sympathetic pathways, directly compounding peripheral vascular resistance.
Evidence Level: Strong (established via epidemiological and clinical tracking).
Therapeutic Weight Loss (Any Methodology)
Autonomic Impact: Blunts leptin-driven central sympathoexcitation, mitigates visceral adipose inflammation, and significantly restores baseline Heart Rate Variability (HRV).
Evidence Level: Strong (validated across multiple clinical cohorts).
Alcohol Consumption
Autonomic Impact: Provokes sharp, acute spikes in peripheral sympathetic activity and systematically degrades the nocturnal parasympathetic (vagal) recovery required for tissue repair.
Evidence Level: Strong (demonstrated in experimental and observational settings).
High-Dose Caffeine Intake
Autonomic Impact: Induces sharp, transient elevations in plasma catecholamines (epinephrine and norepinephrine) primarily via central and peripheral adenosine receptor antagonism.
Evidence Level: Strong (confirmed through acute interventional testing).
Omega-3 Fatty Acid Optimization (EPA/DHA)
Autonomic Impact: Suppresses excessive cardiac sympathetic neural traffic and directly supports baseline autonomic regulation, as reflected by improved HRV.
Evidence Level: Moderate to Strong (backed by RCTs and robust biometric data).
Magnesium Status
Autonomic Impact: Attenuates NMDA receptor excitability, stabilizes cell membranes, and dampens systemic neuromuscular reactivity to sympathetic stressors.
Evidence Level: Moderate (supported by targeted clinical trials).
Dietary Polyphenols (e.g., Berries, Dark Cocoa)
Autonomic Impact: Enhances endothelial nitric oxide synthase (eNOS) activation, boosting nitric oxide bioavailability and subtly improving secondary autonomic balance.
Evidence Level: Early to Moderate (derived from mechanistic insight and small-scale human trials)
.E. Pharmacological Approaches
Several classes of medications work in part by reducing SNS activity:
Beta-blockers (e.g., metoprolol, carvedilol): Block beta-adrenergic receptors; widely used in heart failure and hypertension
Alpha-2 agonists (e.g., clonidine, moxonidine): Reduce central sympathetic outflow; used in resistant hypertension
ACE inhibitors / ARBs: Reduce RAAS activity, indirectly lowering SNS-mediated vasoconstriction
Renal denervation: A catheter-based procedure disrupting sympathetic nerves to the kidneys; emerging evidence supports its use in resistant hypertension
⚠️ Medical disclaimer: The pharmacological approaches above require a physician's evaluation and prescription. Do not modify your medications without medical supervision
Your Personal SNS Reduction Protocol: A Checklist
Use this evidence-based checklist to audit your current lifestyle:
[ ] Getting 150+ minutes of moderate aerobic exercise per week
[ ] Including 2+ resistance training sessions per week
[ ] Practicing 10+ minutes of slow-paced breathing or meditation daily
[ ] Sleeping 7–9 hours per night in a dark, cool room
[ ] Screened for obstructive sleep apnea if you snore or feel unrefreshed
[ ] Limiting sodium intake to <2,300 mg/day (ideally <1,500 mg if hypertensive)
[ ] Eating a predominantly whole-food, plant-rich, Mediterranean-style diet
[ ] Limiting alcohol to ≤1 drink/day (or none if cardiovascular disease is present)
[ ] Managing chronic stress with structured psychological support if needed
[ ] Having resting heart rate and blood pressure checked regularly
[ ] Discussing HRV monitoring with your healthcare provider
11. Common Myths and Mistakes
Myth 1: "If my blood pressure is controlled by medication, I've solved the problem."
Reality: Blood pressure control is important, but medications alone don't always normalize underlying sympathetic overactivity. The Grassi & Drager (2024) review specifically highlighted that residual SNS activation persists even in treated hypertensives, contributing to ongoing cardiovascular risk. Lifestyle interventions targeting SNS tone directly are additive to medication effects.
Myth 2: "Stress only affects your mental health, not your heart."
Reality: Psychological stress is a direct physiological cardiovascular stressor via SNS activation. Chronic stress raises plasma catecholamines, promotes vascular inflammation, impairs endothelial function, and increases arrhythmia risk — all documented in human studies and confirmed mechanistically by Ziegler et al. (2025) in Circulation Research.
Myth 3: "Exercise raises my heart rate — it must be bad for my nervous system."
Reality: Acute exercise temporarily activates the SNS, but regular training produces long-term reductions in resting sympathetic tone. This "sympatholytic" effect of exercise training is one of the best-established adaptations in cardiovascular physiology. Your resting heart rate and HRV are what matter for assessing baseline autonomic health.
Myth 4: "Thin people don't have SNS overactivity problems."
Reality: While visceral obesity is a major driver, SNS overactivity also affects lean individuals with high chronic stress loads, sleep apnea, kidney disease, depression, or genetic predisposition. Body weight alone does not determine sympathetic tone.
Myth 5: "Supplements alone can fix autonomic imbalance."
Reality: No supplement replaces the effect of exercise, sleep, and stress management on SNS tone. While magnesium, omega-3s, and certain herbal compounds show modest effects in trials, they are adjuncts — not primary treatments.
12. FAQs
Q1: What is the sympathetic nervous system in simple terms?
The sympathetic nervous system is the part of your autonomic (autonomic) nervous system responsible for your "fight-or-flight" response. It increases your heart rate, raises blood pressure, and prepares your body for physical action. In small doses, it's essential for survival. When it's chronically overactivated, it becomes a driver of disease.
Q2: What are the signs of sympathetic nervous system overactivity?
Common signs include: persistently elevated resting heart rate (above 80–85 bpm), high or variable blood pressure, low heart rate variability (HRV), poor sleep, chronic anxiety or hypervigilance, excessive sweating, cold hands or feet, difficulty digesting food, and fatigue despite rest. However, many people with SNS overactivity have no obvious symptoms — it progresses silently for years.
Q3: Can stress really cause heart disease?
Yes. Chronic psychological stress activates the SNS and HPA axis, leading to sustained elevations in catecholamines and cortisol. These promote vascular inflammation, endothelial dysfunction, blood clotting, and arrhythmias. Multiple large-scale studies have established chronic stress as an independent risk factor for heart attack, stroke, and cardiovascular death.
Q4: Does obesity directly increase sympathetic nervous system activity?
Yes, through several mechanisms. Excess visceral fat increases leptin secretion, which stimulates hypothalamic SNS outflow. Visceral fat also secretes pro-inflammatory adipokines that activate sympathetic afferent nerves. Additionally, obesity commonly causes obstructive sleep apnea, itself a major SNS activator. Losing even 5–10% of body weight measurably reduces resting sympathetic tone.
Q5: What is heart rate variability and why does it matter for SNS health?
Heart rate variability (HRV) is the variation in the time between consecutive heartbeats. High HRV reflects strong parasympathetic (rest-and-digest) activity and healthy autonomic balance. Low HRV reflects sympathetic dominance and poor parasympathetic tone. It's one of the most accessible, non-invasive markers of autonomic nervous system health and is independently predictive of cardiovascular outcomes.
Q6: Is sympathetic overactivity reversible?
In most cases, yes — especially when lifestyle factors are the primary drivers. Exercise, stress management, sleep optimization, and dietary changes can meaningfully reduce SNS tone within weeks to months. When underlying conditions like OSA, kidney disease, or heart failure are present, treating those conditions also reduces sympathetic activity substantially.
Q7: How does type 2 diabetes affect the sympathetic nervous system?
The relationship is bidirectional. SNS overactivity impairs insulin secretion, worsens insulin resistance, promotes hepatic glucose production, and drives obesity — all of which contribute to type 2 diabetes. And once diabetes develops, it further amplifies sympathetic activity through mechanisms including insulin resistance in the brain and renal nerve activation. DeFronzo (2026) argues this two-way relationship is underappreciated and undertreated in clinical practice.
Q8: Can children have sympathetic nervous system overactivity?
Yes. Childhood obesity, chronic stress (including adverse childhood experiences), poor sleep, and anxiety can all elevate sympathetic tone in young people. Early-onset SNS dysregulation may predispose children to hypertension and cardiovascular disease in adulthood, making pediatric lifestyle interventions particularly important.
Q9: Does caffeine cause long-term sympathetic overactivity?
Acute caffeine consumption (200–400 mg) measurably elevates plasma catecholamines and temporarily raises blood pressure and heart rate. Regular coffee consumers develop partial tolerance to these acute effects. At typical intake levels (1–3 cups/day), long-term cardiovascular outcomes are not consistently worsened and may even be slightly favorable. However, high-dose caffeine from energy drinks or pre-workout supplements is a different matter and warrants caution in those with cardiovascular risk.
Q10: What is renal denervation and who is it for?
Renal denervation is a catheter-based procedure that uses radiofrequency energy or ultrasound to disrupt sympathetic nerve fibers in the renal artery wall. Because the kidneys play a central role in SNS-mediated blood pressure control, severing these nerves can produce sustained blood pressure reductions. It is currently under investigation and in limited clinical use for resistant hypertension — blood pressure that remains uncontrolled despite three or more medications at optimal doses.
Q11: Does the Mediterranean diet actually lower sympathetic tone?
Yes. Multiple randomized trials have shown that Mediterranean dietary patterns reduce inflammatory adipokines, improve endothelial function, and improve HRV — all markers of reduced sympathetic dominance. The diet's combination of omega-3 rich fish, polyphenol-rich vegetables and olive oil, low processed food content, and magnesium-rich nuts and legumes may act synergistically on autonomic balance.
Q12: How quickly can lifestyle changes improve sympathetic nervous system balance?
Measurable improvements in HRV and resting heart rate can occur within 4–8 weeks of consistent aerobic exercise training. Slow-paced breathing practices can shift autonomic balance during a single 10-minute session, with cumulative baseline benefits emerging over weeks. Sleep optimization (especially treating OSA) can produce substantial reductions in sympathetic activity within days to weeks of effective treatment.
13. Conclusion and Action Steps
The sympathetic nervous system is meant to be your emergency response system — powerful, precise, and temporary. When it becomes your default mode, the consequences accumulate silently across the heart, blood vessels, pancreas, kidneys, and fat tissue.
The science reviewed here — drawn from some of 2024–2026's most important cardiovascular and metabolic research — makes clear that chronic sympathetic overactivity is not a peripheral footnote in cardiovascular medicine. It is a central mechanism.
The exciting part? Unlike genetics or age, your autonomic nervous system responds powerfully to the choices you make every day.
Your Action Steps
This week:
Start tracking your resting heart rate each morning before getting out of bed
Practice 10 minutes of slow-paced breathing (4–6 breaths per minute) daily
If you snore heavily or feel unrefreshed after sleep, discuss sleep apnea screening with your doctor
This month:
Build to 150+ minutes of moderate aerobic exercise per week
Reduce processed food and sodium; increase omega-3s, vegetables, and magnesium-rich foods
If you have high blood pressure, diabetes, or heart disease, ask your doctor specifically about your autonomic health and whether SNS overactivity may be contributing
Long term:
Make stress management a non-negotiable health priority — not just mental wellness, but cardiovascular medicine
Monitor HRV trends over time as a window into your autonomic health
Stay informed: this is one of the fastest-moving areas in cardiovascular medicine, with new research emerging monthly
Medical disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your medical treatment, exercise program, or diet — especially if you have an existing health condition.
This article is intended for educational purposes and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment decisions.
Related Articles
Your Resting Heart Rate Could Predict Heart Failure Years Before Symptoms Appear
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Sources and References
Tsuji, T., & Tseng, Y-H. (2026). Adipose tissue as a humoral–neuronal hub in metabolic regulation. Nature Reviews Endocrinology. https://doi.org/10.1038/s41574-026-01265-6
DeFronzo, R. A. (2026). Chronically elevated sympathetic nervous system tone: A significant, common, and poorly realised contributor to cardiometabolic disease in type 2 diabetes. Diabetes, Obesity and Metabolism, 28(3), 1595–1598. https://doi.org/10.1111/dom.70347
Grassi, G., & Drager, L. F. (2024). Sympathetic overactivity, hypertension and cardiovascular disease: State of the art. Current Medical Research and Opinion, 40(sup1), 5–13. https://doi.org/10.1080/03007995.2024.2305248
Varzideh, F., Jankauskas, S. S., Mone, P., Kansakar, U., & Santulli, G. (2026). Autonomic neurotransmission in cardiovascular regulation and pathophysiology. Frontiers in Neuroscience, 19, 1739330. https://doi.org/10.3389/fnins.2025.1739330
Ziegler, K. A., Engelhardt, S., Carnevale, D., McAlpine, C. S., Guzik, T. J., Dimmeler, S., & Swirski, F. K. (2025). Neural mechanisms in cardiovascular health and disease. Circulation Research, 136(11). https://doi.org/10.1161/CIRCRESAHA.125.325580
Esler, M. (2021). Sympathetic nervous system and metabolic syndrome. Journal of Hypertension, 39(11), 2185–2191.
Mancia, G., & Grassi, G. (2014). The autonomic nervous system and hypertension. Circulation Research, 114(11), 1804–1814.
Floras, J. S. (2009). Sympathetic nervous system activation in human heart failure. Journal of the American College of Cardiology, 54(5), 375–385.
Egan, B. M. (2003). Sympathetic responses to obesity and hypertension: Implications for the pathogenesis of cardiovascular disease. Current Opinion in Nephrology and Hypertension, 12(2), 195–200.
Grassi, G. (2016). Assessment of sympathetic cardiovascular drive in human hypertension: Achievements and perspectives. Hypertension, 67(1), 6–11.
Narkiewicz, K., & Somers, V. K. (2003). Sympathetic nerve activity in obstructive sleep apnoea. Acta Physiologica Scandinavica, 177(3), 385–390.
Anderson, E. A., Sinkey, C. A., Lawton, W. J., & Mark, A. L. (1991). Elevated sympathetic nerve activity in borderline hypertensive humans. Hypertension, 17(2), 164–171.
Palatini, P., & Julius, S. (2009). The role of cardiac autonomic function in hypertension and cardiovascular disease. Current Hypertension Reports, 11(3), 199–205.
Schlaich, M. P., et al. (2004). Sympathetic augmentation in hypertension: Role of nerve firing, norepinephrine reuptake, and angiotensin neuromodulation. Hypertension, 43(2), 169–175.
Kario, K., et al. (2023). Renal denervation for hypertension: 2023 comprehensive review of clinical evidence. Journal of Human Hypertension, 37(8), 595–618.
Bhatt, D. L., et al. (2014). A controlled trial of renal denervation for resistant hypertension (SYMPLICITY HTN-3). New England Journal of Medicine, 370(15), 1393–1401.
Patel, S. R., & Hu, F. B. (2008). Short sleep duration and weight gain: A systematic review. Obesity, 16(3), 643–653.
Theorell-Haglöw, J., et al. (2021). Sleep and cardiovascular disease risk: A systematic review. European Heart Journal – Cardiovascular Pharmacotherapy, 7(2), 144–158.
Cornelissen, V. A., & Smart, N. A. (2013). Exercise training for blood pressure: A systematic review and meta-analysis. Journal of the American Heart Association, 2(1), e004473.
Hegde, S. M., & Solomon, S. D. (2015). Influence of physical activity on hypertension and cardiac structure and function. Current Hypertension Reports, 17(10), 77.
Lopes, H. F., et al. (2003). Sympathetic nervous system activity in resistant hypertension. Journal of Hypertension, 21(2), 395–400.
Montano, N., et al. (2009). Heart rate variability explored in the frequency domain. Philosophical Transactions of the Royal Society A, 367(1887), 1315–1338.
Thayer, J. F., & Lane, R. D. (2007). The role of vagal function in the risk for cardiovascular disease and mortality. Biological Psychology, 74(2), 224–242.
Sousa, A. C., et al. (2012). Heart rate variability as a cardiovascular risk factor in patients with type 2 diabetes mellitus. Diabetologia, 55(4), 1–8.
Kuehl, M., & Stevens, M. J. (2012). Cardiovascular autonomic neuropathies as complications of diabetes mellitus. Nature Reviews Endocrinology, 8(7), 405–416.
Straznicky, N. E., et al. (2010). Effects of dietary weight loss on sympathetic activity and early metabolic risk factors. Journal of Clinical Endocrinology & Metabolism, 95(4), 1609–1618.
Martins, F. L., et al. (2022). Mechanisms underlying sympathetic activation in obesity-associated hypertension. Frontiers in Physiology, 12, 699357.
Bhargava, M., & Bhargava, A. (2020). Interplay of sympathetic nervous system and inflammation in cardiovascular disease. Hypertension Research, 43(8), 789–801.
Last reviewed and updated: June 2026. This article incorporates the latest peer-reviewed evidence available at time of publication.