Your Resting Heart Rate Could Predict Heart Failure Years Before Symptoms Appear
Your resting heart rate is more than a fitness metric. Discover how changes in heart rate, sleep regularity, and meal timing may influence long-term cardiovascular health.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/23/202619 min read
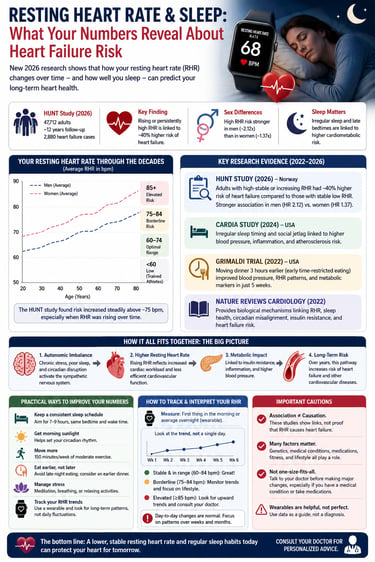
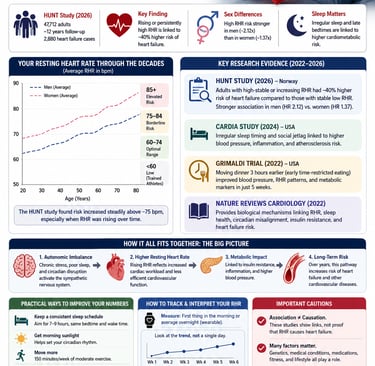
A rising resting heart rate over several years appears more predictive of future heart failure risk than a single heart-rate measurement. New 2026 research involving nearly 48,000 adults found that individuals with persistently elevated or rising resting heart rates had approximately a 40% higher risk of heart failure compared with those whose heart rates remained low and stable.
Key Takeaways :
1. Your RHR trend matters more than any single reading
A longitudinal analysis derived from the 2026 Nord-Trøndelag Health Study (HUNT), evaluating a cohort of 47,712 adult participants, demonstrates that temporal trajectories of resting heart rate (RHR) serve as a significantly more robust predictor of heart failure (HF) incidence than single-point baseline assessments.
2. Women aren’t protected from RHR risk — older studies missed this
Single-measurement research used to say RHR didn’t predict heart failure in women. The 2026 HUNT analysis using longitudinal data overturned that. Each 10-bpm increase in RHR raised risk by 15% in women vs 9% in men. Sex-specific interpretation matters. “Normal for men” isn’t your benchmark if you’re female.
3 RHR ≥85 bpm is your “pay attention” threshold
Average baseline RHR in the HUNT cohort was 74 bpm for women and 70 bpm for men. Clinical guidance treats 60–84 bpm as normal. Consistently above 85 bpm, or a sustained rise >10 bpm from your personal baseline, is worth discussing with your doctor — especially if paired with other risk factors.
4. Irregular sleep timing shows up in your waistline first
The 2026 CARDIA ancillary study of 861 adults found rest-activity rhythm disruption was most strongly tied to BMI and waist circumference, not glucose or blood pressure. Cross-sectional, so no causation claim. But regularity — not just total hours — looks metabolically relevant.
5. Elevated RHR is tied to future diabetes, and insulin resistance explains ~30% of it
In a 5-year Japanese cohort, people with RHR ≥80 bpm had nearly 3x the odds of developing type 2 diabetes vs <60 bpm. Mediation analysis attributed ~27.5% of that link to insulin resistance. Wide confidence intervals mean the true effect size is uncertain, but RHR is a cheap early-warning signal, not a diagnosis.
6. When you stop eating at night can shift overnight heart patterns within weeks
A 2026 Northwestern Medicine RCT tested sleep-aligned fasting: last meal 3+ hours before habitual bedtime, 13–16 hr overnight fast. Result: better nighttime blood pressure dipping and heart rate rhythms vs controls. N=39, mostly female, short-term. Promising mechanism, not yet a population prescription.
7. These are associations, not proof that lowering RHR prevents disease
All the big cohort studies here are observational. Rising RHR might be an early symptom of subclinical heart dysfunction, not just a cause. The RCT shows meal timing can move physiology, but we lack long-term outcome data on heart attacks or heart failure. Correlation ≠ prescription.
8. Track monthly averages, not daily anxiety
Most people’s RHR stays within ~12 bpm of baseline over years. Use wearables to watch multi-week or monthly averages. Flag sustained upward trends. Share the trend with your doctor at checkups. One bad night isn’t a diagnosis — a multi-year climb is a conversation.
Bottom line: RHR is now a longitudinal vital sign. The real value is in trends, sex-specific context, and how it intersects with sleep regularity and meal timing. Use it as one data point to inform — not replace — clinical care.
Introduction
If you check your smartwatch every morning and glance at your resting heart rate (RHR), you're not just satisfying curiosity — you're looking at a number that several large 2026 studies now link directly to your long-term cardiovascular future.
A new analysis of nearly 48,000 adults followed for over a decade found that how your resting heart rate changes over the years — not just a single reading — predicts your risk of developing heart failure. Around the same time, separate research teams have shown that irregular sleep and circadian misalignment are tied to cardiometabolic disease, and that something as simple as adjusting when you stop eating at night can shift blood pressure and heart rate patterns measurably within weeks.
This guide pulls together the newest evidence — peer-reviewed studies from 2022 through 2026, including a HUNT cohort study, a CARDIA ancillary analysis, a Northwestern Medicine randomized trial, and a major Nature Reviews Cardiology synthesis — and translates it into something you can actually use.
1. What Is Resting Heart Rate, and Why Does It Matter?
Your resting heart rate is the number of times your heart beats per minute while you're at complete rest — ideally measured first thing in the morning, before you get out of bed, or via a wearable device that averages your lowest overnight readings.
Normal Ranges, According to the Latest Research
The 2026 HUNT study analysis from Norway — one of the largest longitudinal datasets on this topic — reported the following population averages among nearly 48,000 adults:
Average baseline RHR in women: 74 beats per minute (bpm)
Average baseline RHR in men: 70 bpm
This lines up with general clinical guidance that a normal RHR sits somewhere between 60–84 bpm, with women generally running about 3–7 bpm higher than men due to differences in heart size, autonomic balance, and hormonal influences. A resting heart rate of 85 bpm or higher is generally considered elevated and worth monitoring, since it often coexists with other risk factors such as hypertension, physical inactivity, smoking, or higher age.
Why a Single Reading Isn't the Full Story
Most public health messaging treats RHR as a static number you compare against a chart. But the newest research — particularly the HUNT trajectory analysis — makes a more nuanced and clinically useful point: the direction your RHR moves over years matters more than where it sits on any single day.
That distinction is the foundation for the rest of this article.
2. The HUNT Study: Resting Heart Rate Trajectories and Heart Failure
Study Overview
Published in Frontiers in Cardiovascular Medicine in 2026, this analysis by Hansen and colleagues drew on the Trøndelag Health Study (HUNT), a Norwegian population cohort with repeated health surveys between 1995 and 2019.
Study design at a glance:
Detail Value Participants 47,712 adults Mean follow-up ~12 years (continuous RHR analysis); ~7 years (trajectory analysis) New heart failure cases 2,880 Statistical method Cox regression with restricted cubic splines and latent class trajectory modeling Population Norwegian adults, two to three health survey attendances
This is important methodologically: rather than relying on a single RHR measurement (as most prior studies did), the researchers tracked how RHR changed across repeated visits and grouped participants into RHR "trajectories" — patterns of change over time, such as stable-low, stable-high, increasing, or decreasing.
What They Found
Heart failure incidence differed by sex. Women had a lower rate of new-onset heart failure than men — 4.27 versus 5.68 cases per 1,000 person-years, a 33% lower relative rate in women
Most people's RHR stayed fairly stable. Roughly 74% of participants maintained their RHR within about 12 bpm of baseline between survey visits, with an average change of just -2 bpm. In other words, large swings in RHR are the exception, not the rule, for most healthy adults.
Each 10-bpm increase in RHR raised heart failure risk for both sexes — but slightly more for women. After adjusting for confounders, every 10-bpm rise in RHR was associated with:
15% higher heart failure risk in women
9% higher heart failure risk in men
RHR trajectory was a stronger predictor than a single measurement. People classified into a high RHR trajectory — meaning their heart rate stayed elevated or climbed over repeated measurements — had substantially higher heart failure risk compared with those in a low RHR trajectory:
43% higher risk in women
41% higher risk in men
Interpreting the Clinical Relevance
Why trajectories beat single readings. A one-time RHR check can be thrown off by caffeine, stress, illness, or poor sleep the night before. By tracking RHR longitudinally — exactly what wearables now make possible for ordinary people — clinicians and individuals get a signal that's less noisy and more reflective of underlying cardiovascular physiology, such as autonomic nervous system balance, ventricular function, and overall conditioning.
3. Sex Differences in Resting Heart Rate and Cardiovascular Risk
Sex-specific analysis isn't a footnote — it changes the clinical picture in ways that matter for how you interpret your own numbers.
What's Consistent Across Sexes
Both men and women show increased heart failure risk with rising RHR and with a high RHR trajectory.
The magnitude of trajectory-based risk is nearly identical between sexes (41–43% increase).
What Differs
Baseline RHR is higher in women (74 vs. 70 bpm in the HUNT cohort), consistent with decades of physiological data showing women's hearts beat faster at rest on average.
Overall heart failure incidence is lower in women than men in this cohort, even though each unit of RHR increase carries a somewhat larger relative risk for women.
Earlier meta-analyses of cross-sectional data found a 14% higher heart failure risk per 10-bpm RHR increase in men, with no significant association detected in women — a finding the 2026 HUNT analysis effectively overturned by using longitudinal trajectory data instead of single time-point measurements.
Why This Matters Clinically
This shift in findings — from "RHR doesn't predict heart failure in women" (older, single-measurement studies) to "it does, and possibly even more strongly" (2026 longitudinal data) — is a textbook example of why study design changes the conclusion. A woman whose single RHR reading looked unremarkable in an older study might have been miscategorised as low-risk when in fact,the her RHR trend over years carried real prognostic information.
Practical implication: Sex-specific reference ranges and risk thresholds should not be applied uniformly. If you're a woman tracking your RHR, don't assume that "normal for men" thresholds apply directly to you — and don't assume a single check at the doctor's office captures your real risk profile.
4. Sleep Regularity, Circadian Rhythm, and Cardiometabolic Disease
Resting heart rate doesn't operate in isolation — it's deeply intertwined with your sleep-wake cycle and circadian rhythm, the internal 24-hour clock that governs blood pressure, hormone release, glucose metabolism, and autonomic nervous system activity.
The CARDIA Sleep Ancillary Study
Published in the Journal of the American Heart Association in 2026, this analysis by Chapagai and colleagues examined rest-activity rhythms — objective, wearable-measured patterns of activity and rest across the 24-hour day — in 861 adults from the CARDIA (Coronary Artery Risk Development in Young Adults) cohort.
Methodology:
Participants wore wrist actigraphy devices for 7 days (2020–2023)
Cardiometabolic markers assessed: BMI, waist circumference, blood pressure, hypertension status, fasting glucose, estimated insulin resistance, and diabetes
The sample included 354 Black and 507 White participants, allowing the researchers to test whether race modified these associations
Key finding: The most consistent and robust associations were between rest-activity rhythm disruption and anthropometric markers — body mass index and waist circumference — rather than glucose or blood pressure measures, which showed weaker or less consistent signals in this particular sample.
Why anthropometric markers stood out. Body weight and waist circumference are relatively stable, easily and reliably measured outcomes that integrate effects over months or years — making them more likely to show a detectable cross-sectional association with a rhythm-disruption exposure than more variable, instant-in-time measures like fasting glucose.
The Bigger Picture: A 2026 Nature Reviews Cardiology Synthesis
A comprehensive review by Aggarwal and colleagues in Nature Reviews Cardiology (2026) synthesized the broader mechanistic literature connecting sleep and circadian biology to cardiovascular resilience. The review frames circadian disruption — irregular sleep timing, social jet lag, shift work, and misaligned eating — as a modifiable risk factor that operates through several overlapping pathways:
Disrupted autonomic nervous system balance (reduced parasympathetic, increased sympathetic tone)
Altered blood pressure "dipping" patterns overnight (a healthy heart's blood pressure should fall by roughly 10–20% during sleep)
Circadian misalignment of glucose and lipid metabolism
Increased systemic inflammation
Endothelial (blood vessel lining) dysfunction
The authors propose this as a roadmap for future research and intervention, not a finished clinical protocol — meaning many of the specific thresholds and intervention targets are still being defined and tested in trials like the one discussed in the next section.
5. The Resting Heart Rate–Insulin Resistance–Diabetes Connection
If elevated and rising RHR predicts heart failure, and circadian disruption predicts metabolic dysfunction, is there a more direct biological bridge connecting heart rate itself to diabetes risk? A widely cited prospective study suggests yes.
The Saito et al. Study (2022)
This Japanese prospective cohort study, published in the Journal of Diabetes and its Complications, followed 1,309 adults without diabetes for 5 years (2009–2014 enrollment period), during which 78 participants developed type 2 diabetes, confirmed via oral glucose tolerance testing.
Key results:
Compared with people whose RHR was below 60 bpm, those with an RHR of 80 bpm or higher had nearly three times the risk of developing type 2 diabetes
For every 1 standard deviation increase in RHR, the odds of developing diabetes rose by 37%
Using formal mediation analysis, the researchers calculated that approximately 27.5% (95% CI 1.5–53.5%) of the total effect of RHR on diabetes risk was explained by insulin resistance, measured using the HOMA-IR index
What This Means, and What It Doesn't
The headline finding: roughly 30% of the relationship between elevated resting heart rate and future type 2 diabetes appears to run through insulin resistance. The remaining ~70% of the effect likely reflects other pathways — autonomic nervous system dysfunction, inflammation, or unmeasured lifestyle and genetic factors — that the study wasn't designed to isolate.
Clinical relevance: This study supports resting heart rate as a low-cost, easily obtainable early-warning marker for metabolic risk — not a replacement for standard screening like fasting glucose, HbA1c, or oral glucose tolerance testing, but a complementary signal, especially in settings where lab testing is less accessible.
6. Can Changing When You Eat Improve Your Heart Rate Patterns?
If circadian misalignment contributes to cardiometabolic risk, can realigning your eating schedule with your sleep-wake cycle actually move the needle? A 2026 randomized controlled trial set out to answer exactly that.
The Grimaldi et al. Trial (Northwestern Medicine, 2026)
Published in Arteriosclerosis, Thrombosis, and Vascular Biology, this study tested a sleep-aligned extended overnight fasting protocol — distinct from standard time-restricted eating, because the fasting window was tied to each person's individual habitual sleep time rather than a fixed clock time.
Study design:
Detail Value Participants 39 overweight/obese adults, ages 36–75 Design Randomized, parallel-arm controlled trial Intervention Extended overnight fast of 13–16 hours, with the last meal at least 3 hours before habitual sleep time, plus dimmed evening lighting Control Maintained habitual eating patterns (similar evening light-dimming conditions in both arms) Adherence ~90% in the intervention group
Results: The intervention group showed improvements in nighttime blood pressure "dipping" (the healthy overnight drop in blood pressure) and healthier overnight heart rate rhythms compared with controls — without any instruction to change overall caloric intake. Benefits extended into measurable improvements in daytime cardiometabolic function as well.
Notably, since both groups dimmed lights similarly in the evening but only the intervention group changed meal timing, the researchers concluded the observed benefits were attributable specifically to the fasting-timing change, not lighting alone.
Bottom line for clinical relevance: This trial provides genuine, randomized, mechanistic evidence that timing your last meal a few hours before sleep can shift overnight cardiovascular physiology in a favourable direction — but it's an early, small-scale signal, not yet a population-level prescription.
7. How the Mechanisms Fit Together
Pulling across all five studies, a coherent (if still incomplete) biological story emerges:
Circadian rhythm governs autonomic balance. Your body's internal clock coordinates when sympathetic ("fight or flight") and parasympathetic ("rest and digest") nervous system activity should dominate across the 24-hour day.
Irregular sleep and late-night eating disrupt that coordination, shifting the body toward sympathetic dominance at times it shouldn't be — which shows up as elevated overnight heart rate and blunted blood pressure dipping (Aggarwal et al.; Grimaldi et al.).
Chronic sympathetic dominance correlates with rising resting heart rate over time — exactly the trajectory pattern the HUNT study linked to heart failure risk.
Elevated heart rate itself appears to partly drive insulin resistance (Saito et al.), creating a feed-forward loop where metabolic and cardiovascular risk reinforce each other.
Rest-activity rhythm disruption shows the clearest cross-sectional link to body weight and central adiposity (Chapagai et al.), which independently worsen both heart rate and insulin sensitivity.
This is a plausible integrated pathway, not a fully proven causal chain. Each study examined one or two links; no single study in this body of evidence traced the entire pathway from circadian disruption through to confirmed heart failure diagnosis in the same population.
8. Practical Application: How to Track and Interpret Your Own RHR
Step-by-Step: Building Your Own RHR Baseline
Measure consistently. Use a wearable device or check your pulse first thing in the morning, before caffeine, before getting out of bed.
Track for at least 2–4 weeks before drawing conclusions — day-to-day variation of several beats per minute is completely normal.
Look at your monthly or seasonal average, not single-day spikes. Stress, illness, alcohol, poor sleep, and even weather can temporarily raise RHR.
Watch the trend over months and years, not days. Based on the HUNT findings, a gradual upward trajectory over years is more clinically meaningful than any single elevated reading.
Flag a consistent RHR above 85–90 bpm, or a sustained rise of more than 10 bpm from your personal baseline, as a reason to discuss with your doctor — not a reason to panic.
A Practical Self-Monitoring Checklist
[ ] I check my RHR at roughly the same time each day
[ ] I track at least 4 consistent weeks before judging a "baseline"
[ ] I note major life changes (illness, new medication, big weight changes, new sleep schedule) alongside RHR data
[ ] I look at monthly averages, not single days
[ ] I share my RHR trend data with my doctor at annual check-ups, especially if trending upward
Sleep and Eating Timing Strategies Supported by Current Evidence
Based on the Grimaldi trial and the broader circadian health literature, consider discussing these strategies with your healthcare provider:
Aim to finish eating roughly 2–3 hours before your habitual bedtime.
Keep a consistent sleep and wake time, even on weekends — irregularity itself, independent of total sleep duration, was linked to worse rest-activity rhythm metrics in the CARDIA analysis.
Dim lights in the 2–3 hours before bed to support natural melatonin release and circadian alignment.
Avoid assuming more restriction is better. The trial tested a moderate 13–16 hour fasting window — not extreme prolonged fasting — and did not instruct participants to reduce total calories.
Safety note: Extended fasting protocols are not appropriate for everyone, including people with diabetes on insulin or sulfonylureas, those with a history of disordered eating, pregnant or breastfeeding individuals, and underweight people. Always consult your doctor before changing your eating schedule, especially if you take medications timed to meals.
9. Evidence Summary Table
Hansen et al., 2026 (HUNT Study)
Design & Sample: Longitudinal cohort study tracking 47,712 adults over an approximate 12-year follow-up period.
Key Finding: Sustained or upward trajectories in resting heart rate (RHR) correlate with a 41%–43% increase in heart failure risk across both sexes.
Evidence Weight: Strong. High statistical power due to sample size and long-term follow-up, though inherently limited by its observational nature.
Chapagai et al., 2026 (CARDIA Study)
Design & Sample: Cross-sectional analysis of 861 adult participants.
Key Finding: Disruptions in circadian rest-activity rhythms show a consistent correlation with increased body mass index (BMI) and waist circumference.
Evidence Weight: Moderate. The cross-sectional framework prevents the determination of a causal timeline, and findings are limited by small subgroup sizes.
Grimaldi et al., 2026 (Northwestern University)
Design & Sample: Randomized controlled trial (RCT) involving 39 overweight or obese adults.
Key Finding: Implementing sleep-aligned fasting windows significantly enhances nocturnal blood pressure dipping and restores healthy heart rate rhythmicity.
Evidence Weight: Moderate to Strong. Features a robust experimental design (RCT) with high internal validity, but is limited by a small sample size.
Aggarwal et al., 2026 (Nature Reviews Cardiology)
Design & Sample: Narrative and mechanistic review (secondary literature synthesis).
Key Finding: Outlines an integrated physiological framework detailing how circadian misalignment actively undermines cardiovascular resilience.
Evidence Weight: Qualitative. Offers an essential theoretical model for understanding biological mechanisms, but does not present primary empirical data.
Design & Sample: Prospective cohort study following 1,309 adults over 5 years, capturing 78 incident cases of diabetes.
Key Finding: Insulin resistance mediates roughly 30% of the statistical relationship linking an elevated RHR to the development of type 2 diabetes.
Evidence Weight: Moderate. Limited by wide confidence intervals around the mediation effect and a single-ethnicity study population.
10. Common Myths and Mistakes
Myth: "A high resting heart rate on one bad night means something is wrong." Reality: Single-day fluctuations are extremely common and were explicitly shown in the HUNT study to be less predictive than multi-year trends. One rough night doesn't define your cardiovascular risk.
Myth: "Lower is always better." Reality: Extremely low resting heart rate (well below 50 bpm) can sometimes reflect excellent cardiovascular fitness — but in certain contexts can also indicate a heart rhythm problem. Context (fitness level, symptoms, medications) matters more than the raw number.
Myth: "If my RHR is normal, my circadian health and metabolic risk must be fine too." Reality: The CARDIA and HUNT studies measured different things. A normal RHR doesn't rule out irregular sleep patterns, central adiposity, or early insulin resistance — these require their own tracking.
Myth: "Intermittent fasting and sleep-aligned fasting are the same thing." Reality: The Grimaldi trial tested a fasting window specifically timed to each person's habitual sleep schedule, not a fixed clock-time eating window. The mechanism researchers highlighted was circadian alignment, not calorie restriction.
Myth: "These findings mean wearable RHR data can diagnose heart failure or diabetes." Reality: None of these studies validate consumer wearables as diagnostic tools. They support RHR and rhythm tracking as risk-awareness tools to discuss with a clinician — not replacements for medical diagnosis.
11. Frequently Asked Questions
1. What is considered a dangerous resting heart rate? Generally, a sustained resting heart rate above 100 bpm (tachycardia) or below 60 bpm without explanation or symptoms (bradycardia) warrants medical evaluation. The studies referenced here focus on the more common range of 70–90 bpm and its long-term trend, which is a separate concern from acute arrhythmia.
2. How much can resting heart rate change naturally day to day? According to the HUNT study, most adults' RHR varies within about 12 bpm between health survey visits years apart, with an average shift of just -2 bpm. Day-to-day variation from factors like sleep, stress, and caffeine is typically smaller but still normal.
3. Does a rising resting heart rate always mean heart failure risk? No. It's one statistical risk factor among many, identified through population-level data. Many people with a rising RHR never develop heart failure, and the relationship is influenced by age, sex, fitness, weight, blood pressure, and other factors.
4. Are women or men at higher risk from elevated resting heart rate? Heart failure incidence overall was higher in men in the HUNT cohort, but each 10-bpm RHR increase carried a slightly larger relative risk in women (15% vs. 9%). Trajectory-based risk was nearly identical between sexes (41–43% increase).
5. Can improving sleep regularity lower my resting heart rate? Sleep regularity and circadian alignment are associated with healthier rest-activity rhythms and improved cardiometabolic markers in current research, though the strongest direct evidence (the CARDIA study) is cross-sectional and cannot prove cause and effect for RHR specifically.
6. What is sleep-aligned fasting, and is it the same as 16:8 intermittent fasting? Sleep-aligned fasting, as tested in the Grimaldi trial, extends the fast specifically around your habitual sleep window — last meal at least 3 hours before bed — rather than a generic fixed clock-time window. It's a related but distinct concept from popular intermittent fasting schedules.
7. How does resting heart rate relate to type 2 diabetes risk? A 2022 prospective study found people with RHR ≥80 bpm had roughly triple the diabetes risk of those under 60 bpm, with about 30% of that relationship explained by insulin resistance. This supports RHR as a meaningful, low-cost early signal — not a diagnostic test.
8. Should I be worried if my smartwatch shows my RHR trending up? A gradual upward trend over months to years is worth discussing with your doctor, especially alongside other symptoms (fatigue, shortness of breath, swelling) or risk factors. A short-term uptick tied to stress, illness, or poor sleep is usually not cause for alarm.
9. What's the difference between resting heart rate and heart rate variability (HRV)? RHR is simply how many times your heart beats per minute at rest. HRV measures the variation in time between heartbeats and reflects autonomic nervous system flexibility. Both are studied as cardiovascular risk markers, but they capture different physiological information.
10. Is it better to track resting heart rate trends or get periodic single measurements at the doctor's office? The HUNT study suggests longitudinal tracking (multiple measurements over time, as wearables now enable) provides stronger, more reliable risk information than a single office measurement — though office measurements remain clinically standardized and validated for diagnosis.
11. Can changing my dinner timing alone meaningfully change my heart health? Early randomized trial evidence (Grimaldi et al.) suggests modest, measurable short-term improvements in nighttime blood pressure dipping and heart rate rhythm from sleep-aligned fasting — but this was a small trial, and long-term cardiovascular outcome data don't yet exist.
12. Where can I get my resting heart rate and sleep patterns properly evaluated? Start with your primary care physician or a cardiologist, who can order appropriate testing (ECG, blood work including HbA1c and lipid panel, and possibly a sleep study) based on your full risk profile — not RHR data alone.
12. Conclusion: Your Action Steps
The newest research doesn't ask you to obsess over a single number on your wrist. It asks you to pay attention to trends — in your resting heart rate, your sleep regularity, and your eating timing — because that's where the strongest, most clinically meaningful signals live.
Here's what to do next:
Start tracking your RHR consistently for at least a month to establish your personal baseline.
Watch the trend, not the daily number — a gradual multi-year rise is the pattern most strongly tied to heart failure risk in the HUNT data.
Prioritize sleep regularity, not just sleep duration — go to bed and wake up at consistent times.
Consider finishing meals 2–3 hours before bed, in line with the sleep-aligned fasting evidence, after checking with your doctor if you take meal-timed medications.
Bring your data to your next checkup. Share your RHR trends with your physician, especially if you notice a sustained upward shift or symptoms like fatigue, breathlessness, or swelling.
Don't self-diagnose. These studies inform population-level risk, not individual diagnosis. Persistent concerns deserve a real clinical evaluation, not just an app notification.
Your heart rate is one of the most accessible, continuously available windows into your cardiovascular health that has ever existed. Used thoughtfully — and interpreted with the nuance this research demands — it can be a genuinely useful early-warning tool, not a source of anxiety.
Author's Note (Clinician Perspective)
As physicians, we often focus on blood pressure, cholesterol, blood sugar, and body weight when assessing cardiovascular risk. Yet one of the most accessible health metrics available today may be sitting quietly on your smartwatch or fitness tracker: your resting heart rate.
What makes the newer research particularly interesting is that it shifts our attention away from a single heart rate reading and toward long-term patterns. In clinical practice, I frequently remind patients that health is rarely defined by one measurement on one day. Instead, meaningful risk often emerges from trends that develop gradually over months and years.
Consider a 54-year-old patient who came for a routine wellness visit. She felt generally healthy, exercised occasionally, and had no major symptoms. However, data from her wearable device showed that her resting heart rate had increased steadily from the mid-60s to the upper 70s over several years. Further evaluation revealed poorly controlled blood pressure, weight gain, fragmented sleep, and early insulin resistance. Her rising resting heart rate was not a diagnosis, but it served as an early warning signal that prompted a deeper assessment.
The studies reviewed in this article suggest that resting heart rate may reflect the combined influence of cardiovascular fitness, autonomic nervous system balance, sleep quality, circadian health, metabolic function, and overall physiological stress. Importantly, these findings do not mean that a higher resting heart rate causes heart failure or diabetes. Rather, it may act as a valuable marker that helps identify individuals who could benefit from earlier lifestyle interventions or medical evaluation.
This article is intended for educational purposes and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment decisions.
Related Articles
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWA
References
Aggarwal, B., Gao, Y., Alfini, A., et al. (2026). Sleep and circadian rhythms in cardiovascular resilience: Mechanisms, implications, and a roadmap for research and interventions. Nature Reviews Cardiology, 23, 116–130. https://doi.org/10.1038/s41569-025-01188-1
American Diabetes Association. (n.d.). Standards of care in diabetes. https://diabetes.org
American Heart Association. (n.d.). Understanding blood pressure and heart rate readings. Ahajournals.org.
Centers for Disease Control and Prevention. (n.d.). Heart disease facts. https://cdc.gov/heartdisease
Chapagai, S., Schreiner, P. J., Thomas, S. J., Lewis, C. E., Alexandria, S. J., Carnethon, M. R., Reid, K. J., & Knutson, K. L. (2026). Association of rest-activity rhythm and sleep regularity with cardiometabolic disease in the CARDIA study. Journal of the American Heart Association, 15(7), Article e046839. https://doi.org/10.1161/JAHA.125.046839
Grimaldi, D., Reid, K. J., Abbott, S. M., Knutson, K. L., & Zee, P. C. (2026). Sleep-aligned extended overnight fasting improves nighttime and daytime cardiometabolic function. Arteriosclerosis, Thrombosis, and Vascular Biology, 46(4), Article e323355. https://doi.org/10.1161/ATVBAHA.125.323355
Hansen, L. M. S., Jui, S. S. H., Braaten, T., Dalen, H., Forr-Garnvik, L. B., & Karlsen, T. (2026). Sex-specific longitudinal changes in resting heart rate and all-cause heart failure: Insights from the HUNT study. Frontiers in Cardiovascular Medicine, 13, Article 1752910. https://doi.org/10.3389/fcvm.2026.1752910
National Heart, Lung, and Blood Institute. (n.d.). Heart failure overview and risk factors. https://nhlbi.nih.gov
Saito, I., Maruyama, K., Kato, T., Takata, Y., Tomooka, K., Kawamura, R., Osawa, H., & Tanigawa, T. (2022). Role of insulin resistance in the association between resting heart rate and type 2 diabetes: A prospective study. Journal of Diabetes and its Complications, 36(11), Article 108319. https://doi.org/10.1016/j.jdiacomp.2022.108319
Sleep Foundation. (n.d.). Sleep regularity and cardiovascular health overview. https://sleepfoundation.org
Note: This article synthesizes findings from the primary studies listed above (1–5) along with general clinical context from major health authorities (6–10). Readers seeking the full statistical methodology and complete limitations sections should consult the original peer-reviewed articles via their DOIs.