One Diet Lowers Triglycerides. Another May Lower LDL. Here's What New Research Reveals.
One diet lowers triglycerides. The other may lower LDL. Discover what the latest clinical research says about choosing the best diet for heart health.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/15/202623 min read
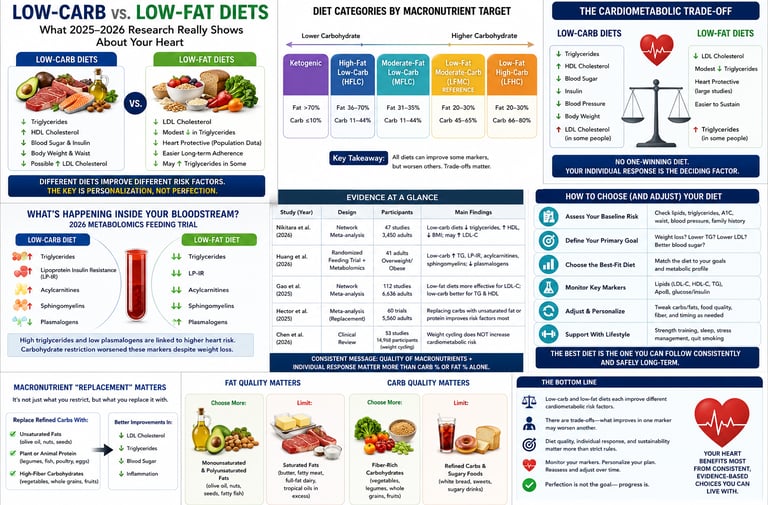

Low-carb and low-fat diets each improve different aspects of cardiometabolic health rather than one being universally superior. Recent 2025–2026 research shows that low-carb diets generally lower triglycerides, increase HDL cholesterol, and promote modest weight loss but may raise LDL cholesterol in some individuals. Low-fat diets may better suit people with elevated LDL cholesterol but can increase triglycerides if they rely heavily on refined carbohydrates. The healthiest diet is one that emphasizes high-quality foods, matches an individual's metabolic profile, and is monitored with regular blood tests.Meta description: New 2026 trials reveal the real cardiometabolic trade-offs of low-carb vs low-fat diets — what improves, what worsens, and how to choose wisely.
Key Takeaways
1. There is No "Winning" Diet—Only Trade-offs
The newest network meta-analyses show that neither low-carb nor low-fat has a monopoly on heart health. Each diet improves some cardiometabolic markers while worsening others. Rather than trying to find a perfect, universally optimal diet, the key is understanding which trade-offs align best with your personal baseline risk profile.
2. Low-Carb Excels at Lowering Triglycerides and Raising HDL
If your primary metabolic goal is to lower your triglycerides (fats in your blood) and boost your HDL ("good") cholesterol, reducing carbohydrates is highly effective. The 2026 Nikitara et al. network meta-analysis confirmed that restricting carbs dramatically lowers the liver’s production of triglyceride-carrying particles.
3. Ketogenic Diets Can Significantly Raise "Bad" LDL Cholesterol
While very-high-fat, ketogenic diets improve triglycerides and HDL, they also associate with the largest increases in total and LDL ("bad") cholesterol—raising LDL by an average of about 17 mg/dL (0.43 mmol/L). This means cutting carbs isn’t a free pass for your lipid panel; you must monitor your LDL response.
4. What You Use to Replace Carbs Matters Immensely
If you choose to restrict carbohydrates, you shouldn't just load up on any fat. A 2025 meta-analysis published in the American Journal of Clinical Nutrition found that replacing cut carbs with a balanced combination of both protein and unsaturated fats (like olive oil, nuts, and fish) yields far better cardiovascular and body composition outcomes than replacing carbs with saturated fat alone.
5. Molecular "Fingerprints" Prove Your Diet's Impact is Real
A landmark 2026 weight-independent feeding trial using mass spectrometry mapped 479 distinct blood metabolites. It revealed that carbohydrate-to-fat ratios systematically shift your biology, raising or lowering specific triglycerides, sphingomyelins, and amino acids. These molecular shifts show that your blood work results are highly traceable and directly tied to your diet's composition.
6. Food Quality Trump's Raw Macronutrient Percentages
Both major network meta-analyses stress that looking only at the "low-fat" or "low-carb" label ignores the most important factor: food quality. A high-carbohydrate diet rich in whole grains and legumes behaves entirely differently in the body than one built on refined sugars, just as olive oil is vastly different for your heart than butter.
7. "Yo-Yo Dieting" Does Not Cause Permanent Metabolic Damage
If you try a diet, struggle, regain weight, and want to try a different strategy, rest easy. A major 2026 clinical review in The Lancet Diabetes & Endocrinology debunked the myth that weight cycling ("yo-yo dieting") causes long-term metabolic harm or permanently slows your metabolism. Trying, adjusting, and trying again is far better than giving up.
8. Customization Over Dogma: Get a Baseline and Re-test
Because of individual genetic differences, there is no single rule for everyone. The safest, most scientific approach is to get a full baseline lipid and glucose panel, select a dietary strategy tailored to your specific metabolic needs, and re-test your blood work in 8 to 12 weeks to see how your unique body is responding.
If you've ever stood in a bookstore aisle staring at diet books that flatly contradict each other, you're not imagining the confusion. One expert insists that cutting carbs is the key to a healthy heart. Another swears that dietary fat is what really clogs your arteries. Both cite science. Both sound confident. And you're left wondering who's actually right.
Here's the honest, evidence-based answer: neither camp has the whole story, and the newest, highest-quality research from 2025 and 2026 finally explains why. Rather than one "winning" diet, large randomized trials and network meta-analyses now show that carbohydrate-focused and fat-focused diets each improve some cardiometabolic markers while worsening others. This is what researchers call a trade-off — and understanding it is far more useful than picking a side.
Why This Debate Refuses to Die
Cardiovascular disease remains the leading cause of death worldwide, and diet-related risk factors are estimated to account for a substantial share of those deaths. That single fact explains why nutrition scientists keep returning to the same basic question: when it comes to protecting your heart and metabolism, does the ratio of carbohydrate to fat in your diet actually matter — and if so, which direction should you lean?
For decades, the two dominant camps have talked past each other. Proponents of carbohydrate restriction point to trials showing improved triglycerides and HDL cholesterol. Proponents of fat restriction point to population data linking saturated fat and LDL cholesterol to atherosclerosis. Both are working from real data. The problem is that most of the underlying trials measured different outcomes, used inconsistent diet definitions, and rarely compared diets directly against one another under uniform conditions.
Network meta-analysis (NMA) was built to solve exactly this problem. Instead of comparing only two diets that happened to be tested against each other in one trial, NMA statistically links every diet that has ever been compared to any other diet — even indirectly — through a shared reference group. This lets researchers rank multiple diets simultaneously and estimate, with real confidence intervals, how a ketogenic diet compares to a low-fat diet even if the two were never tested in the same room.
Two major NMAs, published in 2025 and 2026, plus a landmark feeding trial with molecular-level metabolomics, now give us the clearest picture we've ever had.
The 2026 Network Meta-Analysis: Head-to-Head Results
A 2026 network meta-analysis published in the European Journal of Nutrition by Nikitara, Kontogianni, Haidich, and Bountziouka set out to answer this question with unusual rigor. The research team searched five databases from January 2013 through October 2025 and identified 47 studies involving 3,450 adults aged 35–75 who had at least one cardiovascular risk factor but no established heart disease.
How the diets were categorized
Rather than lumping every "low-carb" study into one bucket — a common flaw in earlier reviews — the researchers built eight precisely defined categories based on percentage of daily energy intake:
Ketogenic: fat >70%, carbohydrate ≤10%
High-fat, low-carb (HFLC): fat 36–70%, carbohydrate 11–44%
High-fat, moderate-carb (HFMC): fat 36–70%, carbohydrate 45–60%
Moderate-fat, low-carb (MFLC): fat 31–35%, carbohydrate 11–44%
Moderate-fat, moderate-carb (MFMC): fat 31–35%, carbohydrate 45–60%
Low-fat, moderate-carb (LFMC): fat ≤30%, carbohydrate 45–60% (used as the reference diet)
Low-fat, high-carb (LFHC): fat ≤30%, carbohydrate >60%
High-MUFA (hMUFA): ≥20% of energy from monounsaturated fat, regardless of overall fat/carb split
What actually happened to cardiometabolic markers
Here is what a random-effects network meta-analysis found when each diet was compared against the low-fat, moderate-carb reference diet:
Body weight/BMI: High-fat, low-carbohydrate diets produced a modest but statistically real reduction in BMI compared with the reference diet — a mean difference of −0.48 kg/m² (95% CI −0.74 to −0.22).
LDL cholesterol: Ketogenic diets produced the largest increase in LDL cholesterol of any category — +0.43 mmol/L (95% CI 0.13 to 0.74), equivalent to roughly +17 mg/dL.
Total cholesterol: Ketogenic diets also produced the largest increase in total cholesterol — +0.55 mmol/L (95% CI 0.13 to 0.96).
HDL cholesterol: Somewhat surprisingly, ketogenic diets also produced the largest increase in HDL cholesterol — +0.12 mmol/L (95% CI 0.06 to 0.18) — illustrating why "good" and "bad" cholesterol can move in the same direction at once.
Triglycerides: Here the pattern flipped. High-carbohydrate diets were the ones associated with a triglyceride increase — +0.24 mmol/L (95% CI 0.04 to 0.43) — compared with the moderate-carbohydrate reference.
Waist circumference, blood pressure, and glycaemic markers (fasting glucose, fasting insulin): Macronutrient distribution had limited, largely non-significant effects on these outcomes across the network.
The clinically important takeaway
This is the sentence worth re-reading: carbohydrate restriction improved triglycerides, HDL cholesterol, and adiposity, but was not consistently favorable for LDL cholesterol. No dietary pattern in this analysis was "safe" on every marker simultaneously. The authors explicitly concluded that no single macronutrient distribution is universally optimal, and that decisions should be individualized based on a person's baseline metabolic profile — not a blanket rule for everyone.
Clinically, this matters enormously for how a clinician (or you) should read a lipid panel after starting a new diet. If your triglycerides drop and your HDL rises after cutting carbohydrates, don't assume your overall cardiovascular risk has automatically improved — check your LDL and total cholesterol too. Conversely, if you switch to a very low-fat, high-carbohydrate approach and your triglycerides creep upward, that single number doesn't necessarily cancel out improvements elsewhere. The full lipid panel, interpreted together, is what actually predicts risk — not any one value in isolation.
It's also worth noting where the evidence was strongest and weakest. Heterogeneity was low for adiposity markers (I² = 0%) but substantial for several lipid outcomes, particularly LDL, total cholesterol, and triglycerides (I² roughly 62–79%). In plain terms: we can be fairly confident about the modest weight effects, but individual results for cholesterol markers varied more from study to study, so treatment rankings should be read as general tendencies, not guarantees for any one person.
The Cardiometabolic Trade-Off, Explained Clinically
Why would a diet improve triglycerides and HDL while raising LDL? This isn't a contradiction in the data — it reflects real physiology, and understanding the mechanism helps you interpret your own lab results more intelligently.
Carbohydrate restriction and triglycerides. When carbohydrate intake drops, especially refined carbohydrate and added sugar, the liver produces less of the very-low-density lipoprotein (VLDL) particles that carry triglycerides into the bloodstream. Less substrate for triglyceride synthesis generally means lower circulating triglycerides — one of the most consistent findings across low-carbohydrate research.
Fat intake and LDL cholesterol. Replacing carbohydrate with fat — particularly saturated fat, which rises by default in many popular low-carb and ketogenic diets unless people deliberately choose unsaturated sources — tends to increase LDL particle production. This is precisely why the 2026 network meta-analysis found the largest LDL increases in the ketogenic category, where fat intake exceeds 70% of calories, often without strict attention to fat quality.
Why HDL rises too, higher total fat intake, including saturated fat, is also one of the more reliable ways to raise HDL cholesterol — which is part of why ketogenic diets showed increases in both LDL and HDL simultaneously in the same analysis. This is a textbook example of why HDL alone is a poor risk marker in isolation; a rising HDL number doesn't offset a rising LDL number on a 1:1 basis for cardiovascular risk.
The clinical bottom line: cardiometabolic risk is multidimensional. A responsible interpretation of any diet's effect requires looking at the whole panel — LDL, HDL, triglycerides, blood pressure, waist circumference, and glycaemic markers together — rather than celebrating or panicking over a single number. This is exactly the kind of nuance a good clinician (and a good article) should walk you through, rather than declaring one "winning" diet.
What's Happening Inside Your Bloodstream: The Metabolomics Breakthrough
Lipid panels tell you the end result of a diet's effects. A 2026 study published in Nature Communications by Angelidi, Bartell, Huang, and colleagues — a team that includes some of the same investigators behind the well-known Framingham State Food Study — went a level deeper, asking what dietary carbohydrate-to-fat ratio (CFR) does to the hundreds of small molecules (metabolites) circulating in your blood, independent of whether you gain or lose weight.
The study design
This was a genuinely rigorous randomized controlled feeding trial. 164 adults with overweight or obesity first lost roughly 12% of their body weight, then were randomly assigned to one of three weight-maintenance diets for 20 weeks:
Low-carbohydrate: 20% carbohydrate, 60% fat, 20% protein
Moderate-carbohydrate: 40% carbohydrate, 40% fat, 20% protein
High-carbohydrate: 60% carbohydrate, 20% fat, 20% protein
All food was provided directly to participants — a feeding protocol, not just dietary advice — which dramatically improves adherence compared with typical "eat this way" trials. 147 participants completed the study, and researchers measured 479 distinct plasma metabolites using mass spectrometry at the start, midpoint, and end of the 20-week phase.
What they found
Of the 479 metabolites measured, 148 changed significantly in relation to carbohydrate-to-fat ratio, even after strict statistical correction for multiple comparisons. The pattern was consistent and biologically coherent:
Increased with higher carbohydrate intake: triglycerides, diglycerides, lysophosphatidylcholines, and lysophosphatidylethanolamines
Decreased with higher carbohydrate intake (i.e., increased with higher fat intake): phosphatidylcholine plasmalogens, phosphatidylethanolamine plasmalogens, sphingomyelins, several amino acids, acylcarnitines, and fatty acids
Crucially, these findings were externally validated in an entirely separate trial (the Popular Diets Study), with a strong correlation (rho = 0.618) between the two independent datasets — a meaningful sign that these aren't statistical flukes specific to one cohort.
The clinically critical detail: risk markers moved in both directions
Here's where the "weight-independent" framing in the study's title matters most. The researchers cross-referenced their findings against a separate meta-analysis of metabolites linked to future type 2 diabetes risk. They found:
Twenty metabolites — mostly triglycerides and diglycerides — increased with higher carbohydrate intake and were independently associated with elevated type 2 diabetes risk in other research. Specifically, eleven triglyceride species with three or fewer double bonds (a marker of lower fatty acid saturation) rose consistently with higher carbohydrate intake and have been separately linked to diabetes risk in prior lipidomic studies.
A smaller number of metabolites showed the opposite, discordant pattern — moving in a direction associated with lower diabetes risk even as carbohydrate intake rose, or vice versa.
In other words: the metabolic fingerprint of a higher-carbohydrate diet includes both some genuinely concerning shifts (the diabetes-associated triglycerides) and some neutral-to-favorable ones. This is exactly the kind of nuance that gets lost in oversimplified headlines claiming any single macronutrient is universally "good" or "bad" for metabolic health.
Why this matters for you, practically
This trial's mediation analysis went one step further, testing whether specific metabolites statistically explained the link between diet and cardiometabolic biomarkers like LDL cholesterol and a marker called the lipoprotein insulin resistance index (LP-IR). Several metabolites — including specific phosphatidylcholines, sphingomyelins, and cholesteryl esters — showed statistically significant mediation effects, meaning they may represent part of the actual biological pathway connecting diet composition to your lab results, not just a correlation.
The clinical translation: your bloodwork after a dietary change isn't a coincidence — it reflects traceable, reproducible molecular shifts. That's reassuring in one sense (the data is real and mechanistic) and sobering in another (no macronutrient ratio shifts every risk marker in a favorable direction at once).
A Second Network Meta-Analysis: Where the Evidence Agrees (and Disagrees)
A separate 2025 network meta-analysis published in Scientific Reports by Sun, Shang, Zhang, and colleagues took a broader approach, comparing eight named dietary patterns — low-fat, Mediterranean, ketogenic, low-carbohydrate, high-protein, vegetarian, intermittent fasting, and DASH — rather than macronutrient percentage bands. Using Surface Under the Cumulative Ranking Curve (SUCRA) scores to rank each diet's relative effectiveness, this analysis found:
Weight and BMI reduction: ketogenic and high-protein diets ranked best
Waist circumference: ketogenic and low-carbohydrate diets ranked best
Blood pressure control: DASH and intermittent fasting ranked best
Triglycerides and total cholesterol reduction: ketogenic and high-protein diets ranked best
HDL-C elevation: low-carbohydrate and low-fat diets ranked best
LDL-C lowering: ketogenic and low-carbohydrate diets ranked best
Glycemic control: DASH and low-carbohydrate diets ranked best
Customary/control diets underperformed nearly every structured dietary pattern
Why this seems to conflict with the 2026 NMA — and why that's actually useful information
At first glance, this looks contradictory: the 2026 Nikitara et al. analysis found ketogenic diets produced the largest LDL increase of any category, while the Sun et al. analysis ranked ketogenic diets favorably for LDL lowering. This is not a data error — it's a demonstration of exactly why methodology matters so much in nutrition science.
The two studies used different comparator groups, different study pools, different diet definitions (macronutrient-percentage bands vs. named branded patterns), and different statistical ranking methods (mean differences against a specific reference vs. SUCRA probability rankings across the whole network). Individual trials within "ketogenic diet" categories also vary enormously in fat quality, protein source, and study population, and both papers note important heterogeneity in their lipid outcome networks.
The honest clinical conclusion: across the totality of 2025–2026 evidence, ketogenic and low-carbohydrate diets consistently and reliably improve triglycerides and often HDL. Their effect on LDL cholesterol is genuinely inconsistent across studies — sometimes favorable, sometimes unfavorable — likely depending heavily on the specific fat sources used, individual genetic factors (some people are "hyper-responders" who see large LDL increases on very low-carb diets), and baseline metabolic status. This is precisely why LDL cholesterol should be checked before and 6–12 weeks after starting any significant low-carbohydrate diet, rather than assumed to move in either direction.
Macronutrient "Replacement" Matters More Than Restriction
A 2025 meta-analysis of randomized trials published in the American Journal of Clinical Nutrition by Feng, Liu, Thompson, and colleagues asked a subtly different — and arguably more practical — question: when you cut carbohydrates, what you replace them with may matter as much as the act of cutting them.
This analysis compared carbohydrate-restricted diets against different macronutrient replacement strategies (replacing the missing carbohydrate calories predominantly with fat, predominantly with protein, or a combination of both) and their downstream effects on cardiovascular risk markers and body composition.
The headline finding: combination replacement — spreading the displaced carbohydrate calories across both fat and protein rather than loading up on one or the other — appeared optimal for improving both cardiovascular and anthropometric outcomes simultaneously.
Why this is clinically useful
This finding helps explain some of the inconsistency seen between the two network meta-analyses above. A "low-carbohydrate diet" that replaces bread and rice mostly with additional protein (lean meats, legumes, dairy) behaves differently in the body than one that replaces those same calories mostly with additional saturated fat (butter, fatty cuts, cream). Both would be correctly labeled "low-carb" in a study, yet they can produce meaningfully different lipid and body-composition outcomes.
Practical translation: if you're planning to reduce carbohydrate intake, deliberately building your plate around a mix of protein and unsaturated fat — rather than simply adding more of whichever fat is convenient — is the approach best supported by this comparative evidence.
Weight Cycling: Is Yo-Yo Dieting Actually Dangerous?
No honest discussion of dietary trade-offs is complete without addressing one of the most persistent fears in popular nutrition culture: that losing weight and regaining it repeatedly — "yo-yo dieting" — causes lasting metabolic damage, accelerates muscle loss, and leaves you worse off than if you'd never tried to lose weight at all.
A 2026 Personal View published in The Lancet Diabetes & Endocrinology by Magkos and Stefan critically re-examined decades of observational studies, randomized trials, and animal research on this exact question. Their conclusion was notably reassuring: there is no convincing causal evidence that weight cycling itself causes long-term metabolic harm in people with obesity.
Why the fear was overstated
The authors found that once studies properly account for pre-existing health conditions, aging, and a person's cumulative lifetime exposure to excess adiposity, the supposedly damaging effects of weight cycling — a disproportionate rebound in fat mass, blunted lean mass recovery, a "damaged" metabolic rate — largely disappear as independent, causal effects. Much of the historical association between weight cycling and poor health outcomes likely reflects the fact that people who cycle their weight often already have higher baseline adiposity or other risk factors driving both the cycling and the poor outcomes — a classic case of confounding, not causation.
The clinical significance
This matters enormously for real-world dietary decision-making, including everything discussed above. If someone tries a low-carbohydrate diet for six months, sees genuine triglyceride and blood pressure improvements, then regains some weight and later switches to a different approach — that pattern, by itself, is not evidence of metabolic damage. The authors explicitly note that intermittent weight loss, even when it isn't permanently maintained, can still provide meaningful windows of improved metabolic health and quality of life.
This is a genuinely important, practice-changing message: the fear of "failing" at a diet and regaining weight should not discourage someone from attempting weight loss or trying a different dietary strategy in the first place. The all-or-nothing mindset — "if I can't keep it off forever, it's not worth doing" — is not supported by the current clinical evidence.
Practical Application: How to Choose (and Adjust) Your Diet
Given everything above, here is a clinically grounded, step-by-step framework — not a one-size-fits-all prescription.
Step 1: Get a full baseline panel before changing anything
Before starting any significant carbohydrate or fat modification, get a fasting lipid panel (LDL, HDL, triglycerides, total cholesterol), fasting glucose or HbA1c, blood pressure, and waist circumference. You cannot meaningfully interpret how a diet affects you without knowing your starting point.
Step 2: Match the diet direction to your personal risk profile
If your triglycerides are elevated and HDL is low (a common pattern in insulin resistance and metabolic syndrome), the evidence above suggests a moderate-to-significant reduction in refined carbohydrate is likely to help, particularly if replaced with a combination of protein and unsaturated fat rather than saturated fat alone.
If your LDL cholesterol is already elevated, or you have a strong family history of early cardiovascular disease, be cautious with very-high-fat, ketogenic-style approaches, given the consistent LDL increases seen in the 2026 network meta-analysis. A moderate-fat, moderate-carbohydrate pattern emphasizing monounsaturated fat (the "hMUFA" category, similar in spirit to a Mediterranean-style diet) may be a more conservative starting point.
If blood pressure or glycaemic control is your primary concern, the comparative evidence points toward DASH-style or structured low-carbohydrate approaches over unstructured "customary" eating, though macronutrient ratio alone had limited effects on these markers in the largest 2026 analysis — meaning factors like sodium intake, fiber, weight loss itself, and physical activity likely matter just as much or more.
Step 3: Prioritize fat and carbohydrate quality, not just quantity
Every study reviewed here notes the same limitation: broad macronutrient percentage targets don't capture food quality. A 60%-carbohydrate diet built on whole grains, legumes, and fruit is a different biological exposure than one built on refined sugar and white bread, even though both would be labeled identically in a macronutrient-based study. The same logic applies to fat — olive oil and nuts are not metabolically interchangeable with processed meat and butter, even at the same total fat percentage.
Step 4: Re-test after 8–12 weeks, not before
Metabolomic and lipid changes were detectable within the first 10 weeks in the feeding trial reviewed above, but some changes continued to shift or stabilize through 20 weeks. Give any dietary change at least two to three months before drawing conclusions from bloodwork, and don't judge a diet's success on the scale alone — track your lipid panel, blood pressure, and waist circumference together.
Step 5: Don't fear "falling off" the plan
Based on the 2026 weight cycling review, an imperfect, inconsistent effort that includes periods of regain is not evidence that you've done metabolic damage. A partially successful, repeated effort at improving your diet is measurably better than an all-or-nothing standard that leads to giving up entirely.
Safety note: None of the findings above should be used to self-manage an existing diagnosis of diabetes, familial hypercholesterolemia, kidney disease, or cardiovascular disease. If you have any of these conditions, or take medication affecting blood sugar, blood pressure, or lipids, work with your physician or a registered dietitian before making a significant macronutrient shift — some of these changes (especially large increases in dietary fat or protein) can interact meaningfully with medication dosing and existing organ function.
Evidence Summary Tables
Here is a breakdown of the key studies and their findings, organized by core themes for quick scanning.
Part 1: The Core Studies & Their Designs
Nikitara et al., 2026 (Eur J Nutr): A massive network meta-analysis pooling data from 47 randomized controlled trials (n=3,450 adults with cardiovascular risk factors). It evaluated 8 distinct diet categories categorized strictly by their carbohydrate-to-fat percentages against a standard reference group.
Angelidi et al., 2026 (Nat Commun): A highly rigorous randomized controlled feeding trial that provided all food directly to 147 completers. It tracked 479 distinct blood molecules (metabolites) to measure how low, moderate, and high-carb diets shift your internal biology independent of weight loss.
Sun et al., 2025 (Sci Rep): A broad network meta-analysis that shifted away from strict percentages and instead ranked the real-world performance of 8 popular, named diets (such as Keto, Mediterranean, DASH, and Intermittent Fasting).
Feng et al., 2025 (Am J Clin Nutr): A focused meta-analysis examining replacement strategies. It evaluated what happens when you cut carbs and choose to replace those missing calories with either fat, protein, or a blend of both.
Magkos & Stefan, 2026 (Lancet Diabetes Endocrinol): A comprehensive clinical review analyzing decades of human and animal data to determine whether losing and regaining weight repeatedly ("yo-yo dieting") causes genuine long-term damage to human metabolism.
Part 2: Head-to-Head Effects by Diet Type
(Compared against a standard low-fat, moderate-carb diet)
The Ketogenic Pattern:
Weight Impact: Yielded mixed or highly limited long-term data.
Lipid Impact: Triggered the largest vertical increases in both "bad" LDL cholesterol and "good" HDL cholesterol simultaneously, while triglyceride responses remained highly variable.
The High-Fat, Low-Carb Pattern:
Weight Impact: Achieved a modest but statistically real reduction in overall BMI.
Lipid Impact: Consistently lowered triglycerides and frequently raised HDL, while its impact on LDL cholesterol remained highly mixed.
The Low-Fat, High-Carb Pattern:
Weight Impact: Mimicked the baseline reference diet closely with no unique weight benefit.
Lipid Impact: Remained completely neutral regarding total and LDL cholesterol, but caused a significant spike in circulating triglycerides.
The High-MUFA Pattern (Rich in Monounsaturated Fats):
Weight Impact: Showed stable, balanced outcomes with minor shifts.
Lipid Impact: Produced a uniquely well-rounded, favorable profile across LDL, HDL, and triglycerides without the stark trade-offs seen in other groups.
Clinical Reminder: Because statistical variations (I2) hovered around 62–79% for these cholesterol markers, these bullet points reflect broad biological tendencies rather than guarantees for how your individual body will respond.
Common Myths & Mistakes
Myth: "Low-carb is the best diet for heart health, full stop." Reality: Low-carbohydrate and ketogenic diets reliably improve triglycerides and often HDL, but the 2026 network meta-analysis found they can also produce the largest increases in LDL and total cholesterol of any diet category. Heart health depends on the whole lipid panel, not one favorable number.
Myth: "Low-fat is outdated and doesn't work." Reality: Low-fat, higher-carbohydrate approaches showed limited effects on waist circumference, blood pressure, and glycaemic markers in this evidence base, and can raise triglycerides if the added carbohydrate is refined. But they were not associated with the LDL increases seen in ketogenic diets, which matters for people with elevated cardiovascular risk.
Myth: "If my HDL goes up, my heart disease risk automatically goes down." Reality: The 2026 NMA found ketogenic diets increased both LDL and HDL simultaneously. A rising HDL does not cancel out a rising LDL on a simple point-for-point basis; overall risk still depends on the combined pattern, particle counts, and individual context.
Myth: "Any weight regain means I've permanently damaged my metabolism." Reality: According to the 2026 Lancet Diabetes & Endocrinology review, there's no convincing causal evidence that weight cycling itself inflicts lasting metabolic harm once pre-existing health status and aging are properly accounted for.
Myth: "Cutting carbs automatically means eating more fat." Reality: The 2025 AJCN meta-analysis found that replacing lost carbohydrate calories with a combination of protein and fat outperformed loading up on fat alone for both cardiovascular and body-composition outcomes.
Myth: "A percentage-based diet label tells you everything you need to know." Reality: Every study reviewed here explicitly notes that macronutrient percentage targets don't capture food quality — fiber, glycemic index, saturated vs. unsaturated fat, and food source all shape outcomes independently of the raw carb/fat split.
FAQs
1. Is a low-carb diet better than a low-fat diet for lowering cholesterol? It depends which type of cholesterol you mean. Low-carbohydrate and especially ketogenic diets tend to lower triglycerides and raise HDL cholesterol more than low-fat diets, according to the 2026 network meta-analysis. However, the same analysis found ketogenic diets produced the largest increases in LDL and total cholesterol of any diet category studied. There is no single answer that applies to every cholesterol marker at once.
2. Will a low-carb diet raise my LDL cholesterol? It can, particularly on very-high-fat, ketogenic-style diets, where a 2026 network meta-analysis found the largest LDL increase (+0.43 mmol/L) of any dietary pattern studied. Response varies by individual — some people are "hyper-responders" — so checking LDL 8–12 weeks after starting is a reasonable, practical safeguard.
3. Does cutting carbs actually help with weight loss more than cutting fat? Modestly, according to the biggest 2026 comparison: high-fat, low-carbohydrate diets produced a small but statistically significant BMI reduction (about −0.48 kg/m²) compared with a low-fat, moderate-carbohydrate reference diet. This is a real but modest effect, not a dramatic one, and other reviews have ranked high-protein and ketogenic diets similarly for weight outcomes.
4. What is a "cardiometabolic trade-off" in diet research? It refers to the fact that a single dietary pattern can improve some cardiovascular risk markers while simultaneously worsening others — for example, improving triglycerides while raising LDL cholesterol. The 2026 network meta-analysis by Nikitara and colleagues used this exact framing because no macronutrient distribution improved every marker at once.
5. Do carbohydrates or fat have a bigger effect on triglycerides? Based on the current evidence, carbohydrate intake — especially refined carbohydrate — has a stronger and more consistent relationship with triglyceride levels. The 2026 network meta-analysis found high-carbohydrate diets increased triglycerides compared with a moderate-carbohydrate reference, while carbohydrate-restricted, higher-fat diets tended to lower them.
6. Is yo-yo dieting dangerous for my metabolism? According to a 2026 critical review in The Lancet Diabetes & Endocrinology, there is no convincing causal evidence that weight cycling itself permanently damages metabolism in people with obesity once pre-existing conditions and aging are accounted for. The authors argue that even temporary weight loss can provide real, worthwhile health benefits, even if the weight is later regained.
7. What should I replace carbohydrates with if I reduce them? A 2025 meta-analysis in the American Journal of Clinical Nutrition found that replacing reduced carbohydrate calories with a combination of protein and fat — rather than loading up heavily on fat alone or protein alone — produced the best combined cardiovascular and body-composition outcomes.
8. Does diet composition affect diabetes risk independent of weight change? Yes. A 2026 metabolomics feeding trial in Nature Communications found that changing the carbohydrate-to-fat ratio altered levels of specific triglyceride species linked to type 2 diabetes risk, and that these changes occurred independent of whether participants gained or lost weight — suggesting diet composition itself, not just body weight, shapes future metabolic risk.
9. Which diet is best for blood pressure? Across the reviewed evidence, structured patterns like DASH and intermittent fasting ranked most favorably for blood pressure in one 2025 network meta-analysis. However, the largest 2026 macronutrient-focused analysis found limited effects of carbohydrate/fat ratio alone on blood pressure, suggesting factors like sodium intake and overall dietary pattern matter as much as the carb-to-fat split.
10. Is the ketogenic diet good or bad for heart health? Both, in different ways — which is the central point of this article. Ketogenic diets reliably lower triglycerides and, in some analyses, rank well for weight and waist circumference. But they also produced the largest LDL and total cholesterol increases of any category in the 2026 network meta-analysis. The honest answer is that ketogenic diets carry real trade-offs that should be monitored with bloodwork, not assumed to be uniformly good or bad.
11. How long does it take to see cardiometabolic changes after switching diets? In the 2026 metabolomics feeding trial, significant metabolite changes were detectable within 10 weeks, with most persisting or stabilizing through 20 weeks. A reasonable real-world guideline is to wait at least 8–12 weeks before checking bloodwork and drawing conclusions about a new diet's effects.
12. Should I trust a diet study that only reports "weight loss" as an outcome? Be cautious. As this article shows, weight change and cardiometabolic risk don't always move together — the 2026 metabolomics trial specifically found metabolic changes that occurred independent of weight change. A trustworthy diet study should report lipid panels, blood pressure, and glycaemic markers, not weight alone.
Conclusion & Action Steps {#conclusion}
The newest, highest-quality evidence from 2025 and 2026 delivers a clear but nuanced verdict: there is no single "best" diet for cardiometabolic health — there are trade-offs, and the right choice depends on your personal risk profile. Carbohydrate restriction reliably improves triglycerides and often HDL cholesterol, and can produce modest reductions in BMI, but is not consistently favorable for LDL cholesterol, particularly at the ketogenic end of the spectrum. Meanwhile, macronutrient ratio alone has limited power to move blood pressure and glycaemic markers, meaning other factors — sodium, fiber, physical activity, and overall food quality — deserve just as much attention as the carb-to-fat split.
Your next steps:
Get a full baseline panel — lipids, fasting glucose, blood pressure, waist circumference — before changing your diet.
Choose a direction (lower-carb or lower-fat) based on your specific risk markers, not general internet consensus.
If reducing carbohydrate, replace it with a mix of protein and unsaturated fat rather than saturated fat alone.
Prioritize food quality — whole grains, legumes, and fiber on the carbohydrate side; olive oil, nuts, and fatty fish on the fat side — regardless of which direction you lean.
Re-test your bloodwork at 8–12 weeks, and adjust based on the whole panel, not a single favorable number.
Don't let fear of regaining weight stop you from trying — the current evidence does not support the idea that imperfect, cyclical efforts cause lasting metabolic harm.
Talk to your doctor or a registered dietitian before making major changes if you have existing diabetes, cardiovascular disease, or take medications affected by diet.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. All dietary changes, particularly for individuals with chronic health conditions such as diabetes, cardiovascular disease, or hypertension, should be made in consultation with a qualified healthcare professional.
Related Articles
Visceral Fat Treatment: GLP-1, Semaglutide, and SGLT2 Explained
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Nikitara, K., Kontogianni, M.D., Haidich, A.B., Bountziouka, V. (2026). Cardiometabolic trade-offs of carbohydrate- and fat-focused diets: a network meta-analysis of randomised clinical trials. European Journal of Nutrition, 65, 204. https://doi.org/10.1007/s00394-026-04028-1
Angelidi, A.M., Bartell, E., Huang, Y., et al. (2026). Weight-independent effects of dietary carbohydrate-to-fat ratio on metabolomic profiles: secondary outcomes of a 5-month randomized controlled feeding trial. Nature Communications, 17, 1662. https://doi.org/10.1038/s41467-026-68353-z
Sun, Y., Shang, M., Zhang, Y., Hu, J., Wang, H. (2025). Comparative effect of dietary patterns on selected cardiovascular risk factors: A network study. Scientific Reports, 15, 28749. https://doi.org/10.1038/s41598-025-13596-x
Magkos, F., Stefan, N. (2026). Is weight cycling clinically harmful? The Lancet Diabetes & Endocrinology, 14(7), 594–607. https://doi.org/10.1016/S2213-8587(26)00037-9
Feng, S., Liu, R., Thompson, C., Colwell, B., Chung, S., Barry, A., Wang, H. (2025). Effects of carbohydrate-restricted diets and macronutrient replacements on cardiovascular health and body composition in adults: A meta-analysis of randomized trials. The American Journal of Clinical Nutrition, 122(5), 1461–1478. https://doi.org/10.1016/j.ajcnut.2025.09.012
Ebbeling, C.B., Feldman, H.A., Klein, G.L., et al. (2018). Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial. BMJ, 363, k4583.
Sacks, F.M., Bray, G.A., Carey, V.J., et al. (2009). Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. New England Journal of Medicine, 360, 859–873.
Global Burden of Cardiovascular Diseases and Risks Collaborators (2025). Global, regional, and national burden of cardiovascular diseases and risk factors in 204 countries and territories, 1990–2023. Journal of the American College of Cardiology, 86, 2167–2243.
Pörschmann, T., Meier, T., Lorkowski, S. (2025). Cardiovascular mortality attributable to dietary risk factors in 54 countries in the WHO European Region from 1990 to 2019. European Journal of Preventive Cardiology, 32, 1553–1563.
World Health Organization (2023). Total fat intake for the prevention of unhealthy weight gain in adults and children: WHO guideline.
Karam, G., Agarwal, A., Sadeghirad, B., et al. (2023). Comparison of seven popular structured dietary programmes and risk of mortality and major cardiovascular events in patients at increased cardiovascular risk: systematic review and network meta-analysis. BMJ, 380, e072003.
Bonekamp, N.E., Cruijsen, E., Geleijnse, J.M., et al. (2024). Diet in secondary prevention: the effect of dietary patterns on cardiovascular risk factors in patients with cardiovascular disease. Nutrition Journal, 23, 18.
Lou, Y., Wang, H., Wang, L., et al. (2025). Comparison with dietary groups of various macronutrient ratios on body weight and cardiovascular risk factors in adults: A systematic review and network meta-analysis. Nutrients, 17(16), 2683.
Goldenberg, J.Z., Day, A., Brinkworth, G.D., et al. (2021). Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission. BMJ, 372, m4743.
Morze, J., et al. (2022). Metabolomics and type 2 diabetes risk: an updated systematic review and meta-analysis of prospective cohort studies. Diabetes Care, 45, 1013–1024.