Fatty Liver Disease (MASLD), Obesity, and Heart Disease: A Triple Threat to Health
Explore the science behind obesity and MASLD, including liver fat, insulin resistance, heart disease risk, diagnosis, and proven treatment strategies
OBESITYMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/15/202626 min read
What is the link between obesity and fatty liver disease?
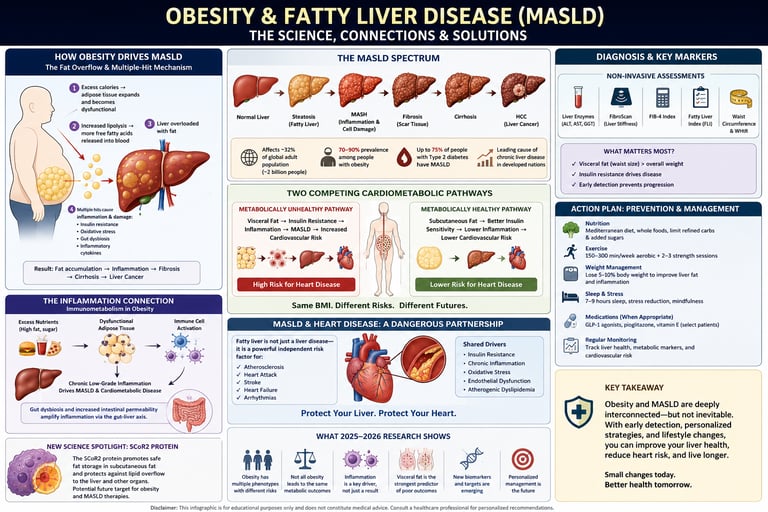
Obesity is the #1 cause of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), affecting 70–90% of people with obesity. Excess visceral fat overwhelms the liver with fatty acids and triggers insulin resistance, causing fat to build up in liver cells. This can progress to inflammation (MASH), fibrosis, and cirrhosis.
Key takeaways..
1. MASLD is a Global Epidemic Driven by Obesity
The Numbers: MASLD affects 32% of adults globally and a staggering 70–90% of individuals living with obesity.
The Cause: Rebranded from NAFLD to better reflect its origins, MASLD is primarily driven by insulin resistance and metabolic overflow, which causes excess fat to accumulate directly in the liver.
2. Waist Circumference Beats BMI as a Risk Predictor
When assessing liver disease risk, total body weight matters less than where that weight is carried. Visceral fat (fat around internal organs) is the primary driver of MASLD.
High-Risk Waist Measurements: Men > 40 inches | Women > 35 inches.
The Critical Metric: A waist-to-height ratio greater than 0.6 signals an urgent need for medical review.
3. Genetics and Fat Location Dictate Your Medical Path
Two people can share the same Body Mass Index (BMI) but experience entirely different health outcomes. Recent research highlights "competing cardiometabolic pathways." Depending on genetic factors and fat distribution, obesity may progress toward liver disease, manifest as heart disease, or remain relatively stable.
4. "Metabolically Healthy Obesity" is a Temporary Illusion
Normal blood work can provide a false sense of security. Liver fat frequently accumulates while cholesterol and blood sugar levels still appear healthy. Furthermore, up to 50% of MASLD patients present with normal ALT/AST liver enzymes, meaning standard blood panels are not enough to rule out liver damage.
5. The Dangerous Synergy of MASLD and Heart Disease
When MASLD and obesity coexist, they compound cardiovascular risks. This combination triggers atherogenic dyslipidemia, a dangerous lipid profile characterized by:
High triglycerides
Low HDL ("good") cholesterol
An increase in small, dense LDL ("bad") particles
Result: This specific lipid shift accelerates the risk of heart attacks and strokes far more aggressively than obesity or liver disease alone.
6. Exercise Rewires the Body’s Inflammatory Response
Inflammation in obesity is complex; total suppression can actually hinder tissue repair. However, targeted physical activity alters the immune landscape of fat tissue. Regular exercise successfully shifts fat tissue from pro-inflammatory M1 macrophages to protective, anti-inflammatory M2 macrophages.
7. Liver Imaging is Superior to Standard Blood Tests
Early detection requires specialized diagnostics rather than routine labs.
Ultrasound: Good for detecting fat, but fails to identify advanced scarring (fibrosis).
FIB-4 Score: A non-invasive calculation where a score < 1.3 indicates low risk, and > 2.67 indicates high risk.
Gold Standards: For individuals with obesity, a FibroScan (transient elastography) or MRI-PDFF provides the most accurate assessment of liver fat and fibrosis.
8. Reversing MASLD: Diet, Exercise, and Medical Advancements
Early-stage MASLD is highly reversible through targeted lifestyle changes and new medical therapies:
The Target: Achieving a 7–10% reduction in body weight significantly reduces liver fat and inflammation.
The Protocol: Emphasize a Mediterranean diet (rich in olive oil, fish, and coffee) paired with resistance training to directly target visceral fat.
Medical Options: For advanced cases, GLP-1 receptor agonists and newly FDA-approved medications like Resmetirom offer powerful therapeutic pathways.
Introduction
If you've been told you have a "fatty liver" — or you're carrying extra weight and wondering what it means for your long-term health — you're asking exactly the right question. And the science has never been clearer, or more nuanced, than it is right now.
Obesity and fatty liver disease (now officially called Metabolic Dysfunction-Associated Steatotic Liver Disease, or MASLD) are among the most consequential health issues of the 21st century. MASLD affects an estimated 32% of the global population, and obesity remains its single most powerful driver. Yet what makes this topic so important — and so often misunderstood — is that not all obesity leads to the same outcomes, and not all fatty livers behave the same way.
In this evidence-based guide, you'll learn:
Why obesity doesn't follow a single disease path (and what that means for your risk)
How liver fat silently sets the stage for heart disease, even before blood sugar rises
What your blood tests and body measurements are really telling you
Practical, science-backed strategies to reduce your risk — whether or not you've lost weight yet
The latest findings from 2025–2026 research that are already reshaping clinical care
1. What Is MASLD? The New Name for Fatty Liver Disease
For decades, the condition was called Non-Alcoholic Fatty Liver Disease (NAFLD). In 2023, an international consensus of liver disease experts renamed it Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) — a name that better captures what's actually happening biologically.
The name change matters for more than semantics. "NAFLD" was essentially defined by what it wasn't (alcoholic). "MASLD" is defined by what it is: a liver condition driven by metabolic dysfunction — the same system-wide dysregulation caused by obesity, insulin resistance, and poor metabolic health.
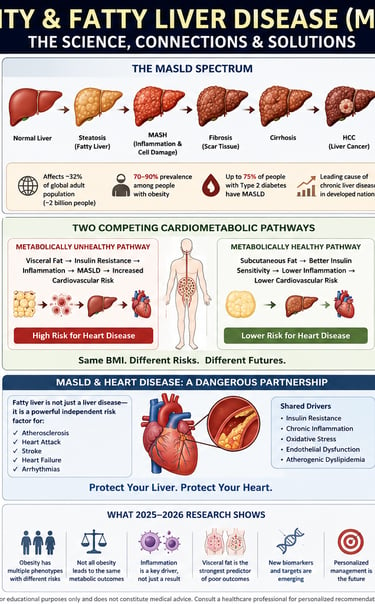
The MASLD Spectrum
MASLD isn't a single disease. It exists on a spectrum:
Simple steatosis (fatty liver): Fat accumulates in liver cells. Often asymptomatic and potentially reversible.
Metabolic-Associated Steatohepatitis (MASH): Fat plus inflammation and liver cell damage. This is the dangerous stage.
Fibrosis: Scar tissue forms as the liver tries to heal inflammation.
Cirrhosis: Advanced scarring that compromises liver function.
Hepatocellular carcinoma (HCC): Liver cancer, which can develop even before cirrhosis in MASLD patients.
How Common Is MASLD?
MASLD now affects approximately 32% of the global adult population — around 2 billion people
Among individuals with obesity, prevalence rises to 70–90%
Among people with Type 2 diabetes, MASLD is present in up to 75% of cases
It is now the leading cause of chronic liver disease in developed nations, surpassing alcohol-related liver disease
According to a landmark 2026 epidemiological review by Grocic, Nguyen, and Sanyal published in Diabetes, Obesity and Metabolism, the global burden of MASLD is rising in parallel with obesity rates — and the two conditions share so many biological pathways that they are increasingly being studied as a unified metabolic syndrome.
2. How Obesity Drives MASLD: The Biological Mechanisms
Understanding why obesity causes fatty liver disease requires a brief tour of liver biology. Your liver is the body's central metabolic hub — processing fats, sugars, hormones, and toxins. When the body accumulates excess fat, the liver is one of the first organs to bear the burden.
The Fat Overflow Hypothesis
In people with obesity, adipose (fat) tissue becomes overloaded and dysfunctional. Instead of safely storing fatty acids, adipose tissue begins releasing them into the bloodstream at abnormally high rates — a process called increased lipolysis. The liver, which is responsible for processing circulating fatty acids, becomes overwhelmed.
The result: hepatic steatosis — fat droplets accumulating within liver cells (hepatocytes).
Insulin Resistance: The Amplifier
Obesity-driven insulin resistance makes the fat problem worse in at least three ways:
Reduced fat burning: Insulin resistance impairs the liver's ability to oxidize (burn) fatty acids for energy.
Increased fat production: The liver compensates by upregulating de novo lipogenesis — manufacturing new fat from carbohydrates.
Impaired fat export: The liver's ability to package and export fat as VLDL particles is disrupted.
The result is a liver trapped in a cycle of fat accumulation it can't break out of.
Gut Dysbiosis and the Liver-Gut Axis
Emerging 2025–2026 research highlights a third critical mechanism: disruption of the gut-liver axis. Obesity alters the gut microbiome, increasing intestinal permeability ("leaky gut"). This allows bacterial endotoxins (lipopolysaccharides, or LPS) to enter portal circulation and travel directly to the liver, triggering inflammation.
A 2026 Frontiers in Nutrition study by Wang, Zhang, Lu, and colleagues used Mendelian randomization to identify shared biomarkers between obesity and NAFLD/MASLD — finding that several genetic and transcriptomic pathways governing inflammation and lipid metabolism are identical in both conditions. This strongly suggests a common biological origin, not merely an association.
3. Competing Cardiometabolic Pathways: Why Two People With the Same BMI Can Have Very Different Outcomes
One of the most important findings in recent MASLD research challenges a deeply held assumption: that obesity leads predictably to fatty liver disease in a linear, dose-dependent way.
It doesn't.
The Competing Pathways Model
A groundbreaking 2026 study by Hirooka and colleagues, published in Gastro Hep Advances, introduced the concept of "competing cardiometabolic pathways" in obesity and MASLD. Their research showed that multiple biological mechanisms operate simultaneously in people with obesity — and which pathway "wins" determines whether someone develops:
Severe liver disease (MASLD → MASH → fibrosis)
Primarily cardiovascular disease (atherosclerosis, coronary artery disease)
Relatively protected metabolic status despite obesity
A combination of all of the above
This isn't random. The "winning" pathway is determined by a person's unique combination of genetics, fat distribution, immune function, lipid metabolism, and lifestyle factors.
What This Means Practically
Two patients sitting in the same clinic, both with a BMI of 34, may face completely different biological futures:
Patient A: High visceral fat, insulin resistance, pro-inflammatory immune profile → rapid progression to MASH and fibrosis
Patient B: Predominantly subcutaneous fat, preserved insulin sensitivity, balanced immune responses → remains at "simple steatosis" stage for years
Understanding which pathway a patient is on requires going beyond BMI — it requires phenotyping. This is why the 2026 research is pushing clinicians toward metabolic phenotyping rather than weight-centric care.
💡 Clinical Pearl: Ask your doctor about comprehensive metabolic panel testing, body composition analysis, and inflammatory biomarkers — not just your weight and standard lipids.
4. The Obesity Phenotype Problem: Where You Store Fat Matters More Than How Much You Weigh
The concept of obesity phenotypes is one of the most clinically significant developments in metabolic medicine in the past decade — and 2025–2026 research has made the evidence stronger than ever.
Visceral vs. Subcutaneous Fat: Not All Fat Is Equal
Fat is stored in two primary depots:
Fat Type Location Metabolic Activity Cardiovascular Risk Visceral adipose tissue (VAT) Around internal organs (liver, pancreas, intestines) Highly active; releases inflammatory cytokines and free fatty acids High Subcutaneous adipose tissue (SAT) Under the skin Less metabolically active; acts as a "safe" storage depot Lower
A 2025 landmark study by Choe, Almas, Neeland, Lim, and Després, published in the European Journal of Clinical Investigation, demonstrated that visceral obesity is a significantly stronger driver of atherogenic dyslipidemia (dangerous blood fat patterns) than subcutaneous obesity.
Furthermore, a 2026 CT-scan-based cross-sectional analysis by Xu, Chen, Xie, and colleagues published in Frontiers in Nutrition provided sex-stratified evidence that CT-assessed abdominal visceral adiposity — not overall BMI — is the dominant predictor of MASLD presence and severity. The relationship was stronger in men than women, highlighting the importance of sex-specific assessment.
Why Waist Circumference Outperforms BMI
Multiple studies now confirm that waist circumference is a better predictor of cardiometabolic risk than BMI because it proxies for visceral fat accumulation.
Current clinical thresholds for high-risk visceral obesity:
Men: Waist circumference > 102 cm (40 inches)
Women: Waist circumference > 88 cm (35 inches)
Asian populations: Lower thresholds apply (>90 cm men, >80 cm women) due to higher metabolic risk at lower waist measurements
A 2026 prospective cohort study by Li, Guo, Zhang, and colleagues, published in Scientific Reports, examined multiple abdominal obesity indices — including waist circumference, waist-to-height ratio, and the Lipid Accumulation Product (LAP) — and found that all were prospectively associated with MASLD risk, with the strongest predictive power coming from waist-to-height ratio.
Practical Takeaway: Measure Your Waist, Not Just Your Weight
To assess your actual visceral fat risk, use this simple formula:
Waist-to-Height Ratio (WHtR) = Waist circumference ÷ Height
< 0.5: Healthy range
0.5–0.6: Moderate risk — lifestyle modification recommended
> 0.6: High risk — medical evaluation strongly advised
5. Metabolically Healthy Obesity: Is It Real?
The concept of "metabolically healthy obesity" (MHO) refers to individuals who are obese (BMI ≥ 30) but appear to have normal metabolic markers: normal blood sugar, normal blood pressure, normal cholesterol. The question is: are they truly protected from obesity-related disease?
The Short Answer: Probably Not — Especially for the Liver
A comprehensive 2025 review by Koliaki, Dalamaga, Kakounis, and colleagues, published in Current Obesity Reports, examined the intersection between MHO and MASLD and reached a sobering conclusion:
"Metabolically healthy obesity" is largely a temporary state. Most individuals classified as MHO show evidence of liver fat accumulation and subclinical metabolic dysfunction — they simply haven't yet crossed the threshold for a formal diagnosis.
Key findings from the review:
Liver disease begins before metabolic markers shift. MASLD often develops while blood sugar, insulin, and cholesterol still appear "normal."
The MHO state is unstable over time. Most MHO individuals transition to metabolically unhealthy obesity within 5–10 years.
Liver biopsy studies reveal hidden damage. Even "healthy" obese individuals frequently show early fibrosis on liver biopsy that blood tests miss.
The "Normal Lab Trap"
Up to 50% of MASLD patients present with completely normal liver enzyme levels (ALT, AST). This makes standard blood work an unreliable screening tool for this population.
A Nature Reviews Gastroenterology & Hepatology editorial published in 2025 titled "Reframing obesity and MASLD" argued that the field needs to move away from metabolic marker-based definitions of "healthy obesity" entirely — because the liver often tells a different story than the bloodwork.
💡 Clinical Pearl: If you have obesity (BMI ≥ 30) or elevated waist circumference, ask your doctor about liver imaging — even if your blood tests are "normal." A liver ultrasound or FibroScan can reveal fat accumulation and early fibrosis that blood tests routinely miss.
6. MASLD and Heart Disease: A Dangerous Partnership
The relationship between MASLD and cardiovascular disease is bidirectional and synergistic — meaning each condition makes the other worse, and together they create a risk greater than the sum of their parts.
Atherogenic Dyslipidemia: The Lipid Link
The specific blood fat pattern that bridges MASLD and heart disease is called atherogenic dyslipidemia, characterized by:
High triglycerides (≥ 150 mg/dL)
Low HDL cholesterol (< 40 mg/dL in men; < 50 mg/dL in women)
Elevated small, dense LDL particles (which penetrate arterial walls more easily than large LDL)
High apolipoprotein B (ApoB) levels
A 2026 study by Fotros, Hekmatdoost, and Yari, published in Scientific Reports, found that obesity was a significant predictor of atherogenic dyslipidemia in MASLD patients — and that the combination created compounded, synergistic cardiovascular risk rather than simply additive risk.
Why the Synergy Is So Dangerous
When obesity and MASLD coexist, multiple pro-atherogenic processes accelerate simultaneously:
The liver overproduces VLDL (triglyceride-rich particles that contribute to plaque formation)
Hepatic inflammation spills systemically, accelerating endothelial dysfunction in arteries
Insulin resistance drives small, dense LDL production — the most atherogenic LDL subtype
Adipokine dysregulation (low adiponectin, high leptin) further promotes arterial inflammation
This is why patients with both obesity and MASLD have a significantly elevated risk of myocardial infarction (heart attack) and stroke, independent of traditional risk factors like smoking or family history.
The TyG Index: A Smarter Insulin Resistance Marker
Clinicians are increasingly using the Triglyceride-Glucose (TyG) Index as a more sensitive surrogate marker for insulin resistance and cardiovascular risk in MASLD patients than fasting glucose alone.
TyG Index = Ln [Fasting triglycerides (mg/dL) × Fasting glucose (mg/dL) / 2]
TyG < 8.5: Lower risk
TyG 8.5–9.0: Borderline
TyG > 9.0: High insulin resistance; strong MASLD and cardiovascular risk indicator
7. The Inflammation Connection: Immunometabolism in Obesity
Inflammation is central to obesity-driven MASLD — but the relationship is far more nuanced than "inflammation is bad." New research in immunometabolism is revealing that some inflammatory responses in obesity are actually protective, while others drive disease. Getting this balance right is emerging as a key therapeutic target.
What Is Immunometabolism?
Immunometabolism is the study of how immune system function and metabolic processes are intertwined. In people with obesity, fat tissue becomes infiltrated with immune cells — primarily macrophages, T cells, and natural killer cells — that profoundly shape metabolic outcomes.
A landmark 2026 review by Lee, published in PLoS Biology, synthesized current evidence on the dual role of inflammation in obesity:
Harmful inflammatory effects in obesity:
M1 macrophage polarization in adipose tissue → chronic TNF-α and IL-6 release → systemic insulin resistance
Kupffer cell (liver macrophage) activation → hepatic inflammation → MASH progression
NLRP3 inflammasome activation → pyroptosis (inflammatory cell death) in hepatocytes → fibrosis
Protective inflammatory effects in obesity:
M2 macrophage responses → tissue repair and remodeling
Type 2 immune responses (IL-4, IL-13) → preserved adipose tissue structure
Acute inflammatory responses → pathogen defense and wound healing
Why This Matters for Treatment
This dual-role finding has a critical clinical implication: broadly suppressing inflammation in obesity may actually cause harm by eliminating protective immune responses.
This is why some anti-inflammatory supplements marketed for weight loss and liver health (fish oil megadoses, NSAIDs, non-specific immunosuppressants) have shown disappointing or mixed results in clinical trials — they may be suppressing beneficial along with harmful inflammation.
The therapeutic future likely lies in targeted immunomodulation: interventions that promote M2 macrophage polarization and anti-inflammatory cytokines (IL-10, TGF-β) while specifically suppressing M1-driven TNF-α and IL-6 cascades.
Exercise currently remains the most effective intervention that achieves this balance naturally — shifting adipose tissue macrophages from M1 to M2 phenotype without broadly suppressing immune function.
💡 Clinical Pearl: Don't try to "eliminate" inflammation with supplements. Focus on lifestyle interventions — especially exercise — that promote the right balance of immune responses.
8. New Molecular Findings: The SCoR2 Protein and Fat Storage
2025 brought a remarkable molecular discovery that may eventually lead to targeted therapies for obesity-driven MASLD.
The SCoR2 Denitrosylase Discovery
A 2025 study by Venetos, Stomberski, Zhou, and colleagues (including Nobel laureate Jonathan Stamler's group), published in Science Signaling, identified a previously little-studied protein called SCoR2 (Thioredoxin-related protein) as a key regulator of fat storage and lipogenesis.
SCoR2 functions as a protein denitrosylase — it removes nitric oxide (NO) groups from target proteins, a process that regulates their activity. The study found that:
SCoR2 controls the activity of key enzymes in hepatic de novo lipogenesis (new fat production in the liver)
Inhibiting SCoR2 reduced fat accumulation in experimental models
This pathway represents a novel, druggable target for MASLD treatment
Why This Is Significant
This discovery adds mechanistic depth to our understanding of why the liver becomes a fat-manufacturing factory in obesity. The nitric oxide signaling pathway that SCoR2 regulates is distinct from insulin signaling pathways — meaning SCoR2 inhibitors could theoretically work alongside (or instead of) existing metabolic therapies.
While this research is still at the experimental stage, it exemplifies how 2025–2026 research is moving from population-level observations to molecular precision — opening doors to treatments that target specific pathways in specific patients.
9. Key Diagnostic Markers and What They Mean
Understanding your test results is the first step toward proactive MASLD management. Here's what the key markers mean and what thresholds should prompt action:
Blood Tests
ALT (Alanine Aminotransferase)
Traditional "normal" range: Up to 40–56 U/L (varies by lab)
2026 research-informed threshold: Risk identified at > 30 U/L (men) and > 19 U/L (women)
What it means: ALT is the most liver-specific enzyme. Elevated levels suggest hepatocyte stress or damage.
⚠️ Caveat: Up to 50% of MASLD patients have "normal" ALT — normal ALT does not rule out MASLD
AST (Aspartate Aminotransferase) and AST:ALT Ratio
AST:ALT < 1: Typical in early MASLD (simple steatosis)
AST:ALT > 1: May signal transition to MASH or early fibrosis; warrants further investigation
What it means: AST is less liver-specific than ALT (also elevated in muscle disease), but the ratio carries diagnostic value
Triglycerides
≥ 150 mg/dL: Metabolic risk threshold
≥ 200 mg/dL: High risk; action required
What it means: High triglycerides are a core feature of atherogenic dyslipidemia and a direct consequence of hepatic fat overload
HDL Cholesterol
< 40 mg/dL (men) or < 50 mg/dL (women): Low HDL threshold
What it means: Low HDL is a hallmark of the atherogenic lipid phenotype; combined with high triglycerides, it signals high cardiovascular risk
Fasting Glucose and Insulin (HOMA-IR)
Fasting glucose > 100 mg/dL: Impaired fasting glucose (pre-diabetes territory)
HOMA-IR > 2.5: Insulin resistance indicator
TyG Index > 9.0: Strong insulin resistance and MASLD risk signal
FIB-4 Index
Formula: Age × AST / (Platelets × √ALT)
FIB-4 < 1.3: Low fibrosis risk
FIB-4 1.3–2.67: Indeterminate; FibroScan or liver biopsy may be warranted
FIB-4 > 2.67: High fibrosis risk; specialist referral recommended
What it means: FIB-4 is now the recommended first-line non-invasive fibrosis screening tool in most international guidelines
Imaging Studies
Test What It Detects Sensitivity for Fat Cost/Availability Liver ultrasound Gross steatosis (≥ 20–30% fat) Moderate Low cost, widely available FibroScan (vibration-controlled transient elastography) Liver stiffness (fibrosis) + CAP score (fat) High for both Moderate cost; specialist centers MRI-PDFF Precise fat quantification Very high High cost; research/specialist centers CT scan Fat and fibrosis estimation Moderate-high Moderate cost; radiation exposure Liver biopsy Gold standard for all stages Definitive Invasive; risk of complications
10. Evidence Summary: What the 2025–2026 Studies Tell Us
Summary Table of Key Recent Studies
Here is a streamlined, reader-friendly rewrite of the study data, organized into clear, actionable bullet points.
1. The Genetic & Biological Link Between Obesity and MASLD
Shared Genetic Roots: Mendelian randomization confirms that obesity and MASLD share identical genetic and metabolic pathways, proving they stem from a common biological origin (Wang et al., 2026).
Competing Health Pathways: Obesity does not hit everyone the same way. It follows multiple "competing" biological pathways, meaning two people with obesity can end up with entirely different health outcomes (Hirooka et al., 2026).
Clinical Takeaway: Treating one condition inherently helps the other. Because outcomes vary so wildly, doctors must use personalized metabolic phenotyping rather than treating obesity as a one-size-fits-all disease.
2. Visceral Fat vs. BMI: Tracking the Real Danger
The Power of WHtR: Prospective data shows that Waist-to-Height Ratio (WHtR) predicts MASLD risk far more accurately than standard BMI (Li et al., 2026).
The Visceral Fat Phenotype: CT scans reveal that visceral fat (fat around your organs), rather than total body weight, is the true driver of MASLD and dangerous lipid profiles. This risk also behaves differently between sexes (Xu et al., 2026; Choe et al., 2025).
Clinical Takeaway: Routine medical checkups must shift away from relying solely on BMI. Measuring waist circumference and tracking fat distribution are essential to catching early liver risk.
3. The Illusion of "Metabolically Healthy Obesity" (MHO)
A Temporary State: "Metabolically healthy obesity" is an unstable, temporary phase. Fat accumulates in the liver well before standard metabolic markers or blood tests begin to alter (Koliaki et al., 2025).
Clinical Takeaway: Normal blood work offers a false sense of security. Regular liver imaging should be standard practice for all patients with obesity, regardless of whether their lab results look "perfect."
4. Compounded Heart Disease & Lipid Risks
Synergistic Danger: When a patient has both obesity and MASLD, their cardiovascular risk doesn't just double—it compounds synergistically by triggering dangerous, atherogenic lipid patterns (Fotros et al., 2026).
Clinical Takeaway: An MASLD diagnosis should immediately trigger aggressive cardiovascular screenings. Protecting the heart is just as urgent as protecting the liver.
5. Rethinking Inflammation & Future Treatments
The Double-Edged Sword of Inflammation: Inflammation in obesity isn't entirely destructive; it plays a nuanced role that includes tissue repair (Lee, 2026).
The SCoR2 Breakthrough: Scientists have identified the SCoR2 denitrosylase protein as a key regulator of how the liver synthesizes and stores fat (Venetos et al., 2025).
Clinical Takeaway: Broad, heavy-handed anti-inflammatory treatments can do more harm than good; therapies must be highly targeted. Meanwhile, the SCoR2 protein opens a major new door for future MASLD drug development.
6. A Global Public Health Trajectory
Parallel Rising Trends: Global data confirms that the MASLD/MASH epidemic is rising in direct lockstep with global obesity rates (Grocic, Nguyen, Sanyal, 2026).
Clinical Takeaway: The liver crisis cannot be solved in isolation. Public health policies and interventions targeting obesity are the most direct way to blunt the rising wave of chronic liver disease.11. Common Myths and Mistakes About Obesity and Fatty Liver {#myths-mistakes}
Myth 1: "If My Blood Tests Are Normal, My Liver Is Fine"
Reality: Up to 50% of MASLD patients have completely normal liver enzyme levels. The liver can accumulate significant fat and even early fibrosis before enzyme levels rise above "normal." If you have obesity or elevated waist circumference, ask for imaging-based screening regardless of your bloodwork.
Myth 2: "Fatty Liver Is Only a Problem for Alcoholics"
Reality: MASLD (non-alcoholic fatty liver disease) is now the most common liver disease worldwide, and its primary driver is metabolic dysfunction — not alcohol. You can have severe MASLD without ever drinking.
Myth 3: "Metabolically Healthy Obese People Don't Need to Worry About Their Liver"
Reality: "Metabolically healthy obesity" is increasingly understood as a temporary state. Most MHO individuals transition to metabolic dysfunction within years, and liver disease often develops before standard metabolic markers (glucose, blood pressure, cholesterol) shift. Liver screening matters for all obese individuals.
Myth 4: "Losing Weight Will Fix Everything"
Reality: Weight loss is highly beneficial and can reverse early MASLD. However, the type and location of fat matter as much as total weight lost. Someone who loses 10 kg of subcutaneous fat without reducing visceral fat may not significantly reduce their MASLD or cardiovascular risk. Targeted approaches — including resistance training and dietary strategies that specifically reduce visceral fat — are more effective than weight loss alone.
Myth 5: "You Just Need to Reduce All Inflammation"
Reality: Inflammation in obesity is dual-natured. Broadly suppressing all inflammation can impair beneficial immune responses that protect against infection and support tissue repair. The goal is to modulate inflammation — specifically reducing chronic, metabolically harmful inflammation while preserving protective immune responses. Exercise achieves this more effectively than most supplements.
Myth 6: "MASLD Only Affects Overweight People"
Reality: While obesity is the strongest risk factor, "lean MASLD" — fatty liver disease in individuals with normal BMI — affects an estimated 5–20% of MASLD cases globally. Lean MASLD is particularly common in East Asian populations and is associated with visceral fat accumulation despite normal overall weight. This reinforces why fat distribution matters more than total weight.
Myth 7: "A Liver Ultrasound Will Catch Everything"
Reality: Standard liver ultrasound can detect fat accumulation (steatosis) reasonably well, but it cannot reliably detect fibrosis — the scarring that signals disease progression toward cirrhosis. FibroScan (transient elastography) or the FIB-4 score are needed to assess fibrosis.
Mistake: Skipping Cardiovascular Assessment in MASLD Patients
Many patients and even some clinicians focus exclusively on the liver when managing MASLD. However, cardiovascular disease — not liver failure — is the leading cause of death in MASLD patients. Cardiovascular risk assessment and management should be integrated into every MASLD care plan.
12. Action Plan: Prevention and Management of Obesity and MASLD
Step 1: Know Your Numbers — Go Beyond the Scale
Prioritize these assessments over BMI alone:
Measure:
✅ Waist circumference (and calculate waist-to-height ratio)
✅ Fasting triglycerides and HDL cholesterol
✅ ALT, AST, and AST:ALT ratio
✅ Fasting glucose and insulin (calculate HOMA-IR and TyG index)
✅ FIB-4 score (your doctor can calculate this from standard blood tests)
Consider:
✅ Liver ultrasound or FibroScan if you have obesity + any of the following: elevated waist circumference, abnormal lipids, elevated liver enzymes, family history of liver disease
✅ CT body composition analysis if available and clinically indicated
Step 2: Eat to Reduce Visceral Fat and Liver Fat — Not Just Calories
The science on dietary approaches for MASLD strongly supports the following strategies:
Mediterranean Diet: The Evidence Winner
Multiple meta-analyses confirm the Mediterranean diet as the most beneficial dietary pattern for MASLD, consistently reducing liver fat, inflammation, and cardiovascular risk.
Core principles:
Olive oil as primary fat source (2–4 tbsp daily)
Abundant vegetables, legumes, whole grains, nuts, and seeds
Fish 2–3 times weekly (especially oily fish for omega-3s)
Limited red meat (< 2 servings/week)
Moderate red wine only if already consumed (or avoid entirely)
Specific Foods With MASLD Evidence
Here is the nutritional evidence rewritten into clean, scannable bullet points, categorized by the strength of the clinical evidence.
Strong Evidence
Extra-Virgin Olive Oil
Mechanism: Rich in anti-inflammatory polyphenols.
Impact: Directly reduces liver fat accumulation and systemic inflammation.
Fatty Fish (Salmon, Sardines)
Mechanism: High concentration of Omega-3 fatty acids.
Impact: Inhibits hepatic de novo lipogenesis (the process where the liver creates new fat molecules).
Coffee (2–3 cups/day)
Mechanism: Contains bioactive compounds like caffeine and chlorogenic acid.
Impact: Shows a strong, proven inverse association with liver fibrosis progression.
Moderate Evidence
Walnuts
Mechanism: Synergistic effect of Omega-3 fatty acids and plant polyphenols.
Impact: Effectively lowers elevated liver enzymes.
Cruciferous Vegetables (Broccoli, Brussels Sprouts)
Mechanism: Contains sulforaphane, which activates the Nrf2 cellular defense pathway.
Impact: Significantly reduces oxidative stress within liver tissue.
Berries
Mechanism: High in anthocyanins (the pigments that give berries their rich color).
Impact: Lowers overall inflammation and minimizes liver fat storage.
Green Tea
Mechanism: Abundant in catechins (powerful antioxidants).
Impact: Helps reduce and normalize liver enzyme levels.
What to Minimize
🚫 Fructose and sugar-sweetened beverages — Fructose is metabolized almost exclusively by the liver and directly drives de novo lipogenesis; this is a top priority to eliminate
🚫 Ultra-processed foods — Strongly associated with MASLD progression
🚫 Refined carbohydrates — Spike insulin and contribute to triglyceride synthesis
🚫 Saturated fat — Promotes hepatic lipotoxicity and inflammation
A 2024 intervention study by Erdem and colleagues, published in Medicine, found that a low-fat dietary intervention significantly reduced inflammatory markers (including TNF-α and IL-6) in individuals with obesity/overweight and NAFLD — supporting the use of low-fat Mediterranean-style diets as a primary intervention.
Step 3: Exercise Strategically — Both Cardio and Resistance Training
Exercise is arguably the most powerful tool for reducing visceral fat and liver fat. Current evidence supports a combined approach:
Aerobic exercise:
Target: 150–300 minutes of moderate-intensity per week (brisk walking, cycling, swimming)
Effect on liver: Even without weight loss, aerobic exercise can reduce liver fat by 20–30%
Effect on visceral fat: Preferentially reduces VAT compared to SAT
Resistance training:
Target: 2–3 sessions per week, all major muscle groups
Effect on metabolism: Increases resting metabolic rate, improves insulin sensitivity, reduces HOMA-IR
Effect on inflammation: Promotes M2 macrophage polarization (anti-inflammatory)
HIIT (High-Intensity Interval Training):
Target: 2–3 sessions per week, 20–30 minutes each
Evidence: May produce greater liver fat reduction per unit of time compared to moderate continuous exercise
📸 Visual suggestion: Insert weekly exercise schedule template for MASLD management showing cardio, resistance, and rest day distribution.
Step 4: Address Sleep, Stress, and Metabolic Disruptors
Sleep: Short sleep duration (< 7 hours) and poor sleep quality are independently associated with obesity, insulin resistance, and MASLD. Prioritize 7–9 hours of quality sleep.
Stress: Chronic psychological stress drives cortisol-mediated visceral fat accumulation. Mindfulness, stress reduction practices, and social support are evidence-based metabolic interventions, not just wellness buzzwords.
Alcohol: Even "moderate" alcohol consumption (> 1 standard drink/day) can accelerate fibrosis progression in MASLD. Many guidelines now recommend complete abstinence for MASLD patients.
Medications that affect the liver: Some common medications (statins, amiodarone, tamoxifen, corticosteroids) can promote or worsen liver fat accumulation. Review your medications with your doctor if you have MASLD.
Step 5: Work With Your Healthcare Team — Personalized Medicine Is the Future
Given the competing pathway model and obesity phenotype evidence, no single treatment protocol works for everyone. Work with your healthcare provider to develop a personalized plan that includes:
Regular metabolic monitoring (every 6–12 months)
Cardiovascular risk stratification and management
Consideration of pharmacotherapy if lifestyle alone is insufficient
Emerging pharmacological options for MASLD (as of 2026):
GLP-1 receptor agonists (semaglutide, liraglutide): Reduce liver fat, weight, and cardiovascular risk — now FDA-approved for weight management and showing strong MASLD benefits
Resmetirom (Rezdiffra): First FDA-approved treatment specifically for MASH with fibrosis (approved 2024)
FXR agonists and other metabolic targets: In various stages of clinical trials
⚠️ Important: Always discuss medication options with a specialist (hepatologist, endocrinologist, or metabolic medicine physician). These drugs have specific indications and potential side effects.
13. FAQs
Q1: Does having obesity automatically mean I'll develop MASLD?
No. While obesity is the strongest risk factor for MASLD, the "competing cardiometabolic pathways" research demonstrates that individual variation in genetics, fat distribution, and immune function means that not everyone with obesity develops significant liver disease. That said, liver screening is recommended for all people with obesity, as MASLD often develops silently.
Q2: What's the difference between MASLD and NAFLD — is it the same thing?
Yes, essentially. MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease) is the new 2023 name for what was previously called NAFLD (Non-Alcoholic Fatty Liver Disease). The name change reflects a better understanding that the condition is driven by metabolic dysfunction rather than simply by the absence of alcohol use.
Q3: Can I have a fatty liver if I'm not overweight?
Yes. "Lean MASLD" — fatty liver in people with normal BMI — affects approximately 5–20% of all MASLD cases. It's particularly common in East Asian populations and in people who carry fat viscerally despite a normal overall weight. Waist circumference can be elevated even when BMI is normal.
Q4: How much weight do I need to lose to reverse fatty liver?
Research shows that losing 7–10% of body weight can significantly reduce liver fat and, in earlier stages, potentially reverse MASLD. Greater weight loss (10–15%) can lead to improvement in fibrosis. Importantly, even modest weight loss with exercise can reduce liver fat substantially, even without reaching these targets.
Q5: Is a liver ultrasound enough to diagnose MASLD?
Liver ultrasound is a good first-line test that can detect significant steatosis (fat accumulation). However, it cannot reliably detect fibrosis (scarring). The complete diagnostic picture typically requires combining ultrasound with blood-based fibrosis scores (FIB-4) and, when indicated, FibroScan or liver biopsy.
Q6: Are there medications to treat MASLD?
As of 2026, Resmetirom (Rezdiffra) is the first drug specifically approved for MASH with fibrosis (the more advanced inflammatory stage of MASLD). GLP-1 receptor agonists (semaglutide, liraglutide) are approved for obesity and Type 2 diabetes and have shown significant MASLD benefits. Several other drugs are in late-stage clinical trials. For earlier-stage MASLD (simple steatosis without significant fibrosis), lifestyle modification remains the primary treatment.
Q7: Is inflammation in obesity always harmful?
No — and this is one of the most important nuances in recent immunometabolism research. Some inflammatory responses in obesity serve protective functions (infection defense, tissue repair). The problem is chronic, low-grade inflammation that persists inappropriately and drives insulin resistance, MASH progression, and atherosclerosis. The therapeutic goal is modulating inflammation — not eliminating it.
Q8: Should I be worried about my heart if I have MASLD?
Yes — cardiovascular disease is actually the leading cause of death in MASLD patients, ahead of liver-related causes. MASLD drives atherogenic dyslipidemia (high triglycerides, low HDL, small dense LDL) that significantly accelerates atherosclerosis. Everyone with MASLD should have cardiovascular risk assessment and management as part of their care plan.
Q9: What is the TyG Index and should I ask my doctor about it?
The Triglyceride-Glucose (TyG) Index is a calculated measure of insulin resistance (TyG = Ln [triglycerides × glucose / 2]). It has emerged as a more sensitive predictor of insulin resistance and MASLD risk than fasting glucose or HbA1c alone. If you have MASLD or metabolic risk factors, asking your doctor to calculate your TyG Index from existing blood tests is worthwhile.
Q10: How is MASLD treated differently from general obesity?
MASLD management adds liver-specific monitoring and intervention targets to general obesity care. Beyond weight management, MASLD treatment specifically focuses on reducing hepatic fat and inflammation, preventing fibrosis progression, managing atherogenic dyslipidemia, and screening for cardiovascular complications. The two conditions share many lifestyle interventions (Mediterranean diet, exercise) but require integrated, multidisciplinary care — ideally involving hepatology, endocrinology, and cardiology.
Q11: What does the "liver-gut axis" have to do with fatty liver disease?
The liver-gut axis refers to the bidirectional communication between the gut microbiome, intestinal barrier function, and the liver. In obesity, disruption of the gut microbiome (dysbiosis) and increased intestinal permeability ("leaky gut") allow bacterial endotoxins to enter portal circulation and reach the liver, triggering inflammatory cascades that accelerate MASLD. This is why dietary interventions that improve gut health — like fiber-rich, plant-based diets and probiotic foods — may benefit MASLD beyond their direct metabolic effects.
Q12: Is MASLD reversible?
In its earlier stages (simple steatosis, early inflammation), MASLD is potentially reversible with sustained lifestyle intervention — particularly weight loss of ≥ 7–10% and regular exercise. Once significant fibrosis develops, reversibility is more limited but improvement is still possible. Early detection and intervention are therefore critical to preventing progression to irreversible cirrhosis.
14. Conclusion and Next Steps
The science of obesity and fatty liver disease has moved far beyond "eat less, move more." What 2025–2026 research is telling us is both sobering and empowering:
Sobering: MASLD is silent, widespread, and often present even when standard blood tests appear normal. The combination of obesity and MASLD creates compounded cardiovascular risk that demands proactive management. And "metabolically healthy obesity" provides far less protection than once believed.
Empowering: Not everyone with obesity follows the same disease path. Knowing your phenotype — where you store fat, what your specific metabolic markers show, how your immune system is functioning — gives you and your healthcare team the information to intervene precisely. Personalized medicine is no longer a future concept; it's the standard of care.
Your Immediate Action Steps
Measure your waist circumference and calculate your waist-to-height ratio today.
Ask your doctor for a full metabolic panel including triglycerides, HDL, fasting glucose, and liver enzymes — and request a FIB-4 score calculation.
Consider liver imaging (ultrasound or FibroScan) if you have obesity or elevated waist circumference, regardless of "normal" blood tests.
Start with the Mediterranean diet and commit to 150 minutes of aerobic activity per week, adding 2 resistance training sessions.
Prioritize sleep and stress management as metabolic interventions, not optional lifestyle additions.
Work with a multidisciplinary team — your primary care physician, a dietitian, and if needed, a hepatologist and cardiologist.
The research is clear: early, personalized, comprehensive action is your most powerful tool. The liver is resilient in its early stages — give it the chance it deserves.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
The New Era of Fatty Liver Disease: What Every Patient Should Know About New Treatments
Weight Loss vs Fat Loss: The Critical Difference Every GLP-1 User Must Understand
Visceral Fat Treatment: GLP-1, Semaglutide and SGLT2 Explained
GLP-1 Muscle Loss: You’re Losing Weight But Are You Losing Strength Too?
Why Your Body Resists Weight Loss: Understanding the Science of Weight Regain | DR T S DIDWAL
Obesity 2025: Revolutionary Research Advances in Treatment and Management | DR T S DIDWAL
References
Choe, H. J., Almas, T., Neeland, I. J., Lim, S., & Després, J.-P. (2025). Obesity phenotypes and atherogenic dyslipidemias. European Journal of Clinical Investigation, 51, e70151. https://doi.org/10.1111/eci.70151
Erdem, N. B., Kahramanoğlu Aksoy, E., Dikmen, D., Uçar Baş, K., Ağaçdiken, A., İlhan Esgin, M., & Göktaş, Z. (2024). Effects of low fat diet on inflammatory parameters in individuals with obesity/overweight and non-alcoholic fatty liver disease: A cross-sectional study. Medicine, 103(15), e37716. https://doi.org/10.1097/MD.0000000000037716
Elsabaawy, M. (2024). Liver at crossroads: unraveling the links between obesity, chronic liver diseases, and the mysterious obesity paradox. Clinical and Experimental Medicine, 24, 240. https://doi.org/10.1007/s10238-024-01493-y
Fotros, D., Hekmatdoost, A., & Yari, Z. (2026). Obesity as a predictor of atherogenic dyslipidemia in patients with metabolic dysfunction associated steatotic liver disease. Scientific Reports, 10. https://doi.org/10.1038/s41598-026-35525-2
Grocic, M., Nguyen, M., & Sanyal, A. J. (2026). Current trends in the epidemiology of obesity and the association between obesity and metabolic liver disease (MASLD/MASH). Diabetes, Obesity and Metabolism, 28(S2), 3–18. https://doi.org/10.1111/dom.70662
Hirooka, M., Miyake, T., Yano, R., Nakamura, Y., Okazaki, Y., Shimamoto, T., Yukimoto, A., Yamamoto, Y., Watanabe, T., Yoshida, O., Hirooka, K., & Tokumoto, Y. (2026). Competing cardiometabolic pathways of obesity and metabolic dysfunction-associated steatotic liver disease. Gastro Hep Advances. Advance online publication. https://doi.org/10.1016/j.gastha.2026.100882
Koliaki, C., Dalamaga, M., Kakounis, K., et al. (2025). Metabolically healthy obesity and metabolic dysfunction-associated steatotic liver disease (MASLD): Navigating the controversies in disease development and progression. Current Obesity Reports, 14, 46. https://doi.org/10.1007/s13679-025-00637-9
Lee, Y. S. (2026). Immunometabolism in obesity: Understanding the beneficial and detrimental roles of inflammation. PLoS Biology, 24(1), e3003620. https://doi.org/10.1371/journal.pbio.3003620
Li, S. L., Guo, S. X., Zhang, M. H., et al. (2026). The relationship between abdominal obesity indices and the risk of metabolic dysfunction-associated fatty liver disease: A prospective cohort study. Scientific Reports, 16, 17777. https://doi.org/10.1038/s41598-026-49030-z
Reframing obesity and MASLD [Editorial]. (2025). Nature Reviews Gastroenterology & Hepatology, 22, 147. https://doi.org/10.1038/s41575-025-01046-y
Venetos, N. M., Stomberski, C. T., Zhou, H.-L., Qian, Z., McLaughlin, P. J., Bansal, P. K., Feczko, J., Bederman, I., Nguyen, H., Hausladen, A., Schindler, J. C., Grimmett, Z. W., Brunengraber, H., Premont, R. T., & Stamler, J. S. (2025). The protein denitrosylase SCoR2 regulates lipogenesis and fat storage. Science Signaling, 18(918). https://doi.org/10.1126/scisignal.adv0660
Wang, J., Zhang, L., Lu, X., Niu, H., Zhao, W., Ma, P., & Han, J. (2026). Identification of shared biomarkers in obesity and non-alcoholic fatty liver disease: A comprehensive analysis of Mendelian randomization and transcriptomic data. Frontiers in Nutrition, 13, 1780686. https://doi.org/10.3389/fnut.2026.1780686
Xu, L., Chen, T., Xie, Y., Xiang, X., Liu, Y., Xu, C., & Wang, S. (2026). CT-assessed abdominal visceral adiposity and MASLD: A sex-stratified cross-sectional analysis. Frontiers in Nutrition, 13, 1750470. https://doi.org/10.3389/fnut.2026.1750470
Chalasani, N., Younossi, Z., Lavine, J. E., Charlton, M., Cusi, K., Rinella, M., Harrison, S. A., Brunt, E. M., & Sanyal, A. J. (2018). The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology, 67(1), 328–357. https://doi.org/10.1002/hep.29367
Rinella, M. E., Lazarus, J. V., Ratziu, V., Francque, S. M., Sanyal, A. J., Kanwal, F., Romero, D., Abdelmalek, M. F., Anstee, Q. M., Arena, U., Arrese, M., Bataller, R., Beuers, U., Boursier, J., Bugianesi, E., Byrne, C. D., Castro Narro, G. E., Cortez-Pinto, H., Croquefer, S., . . . Newsome, P. N. (2023). A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology, 78(6), 1966–1986. https://doi.org/10.1097/HEP.0000000000000520
Younossi, Z. M., Koenig, A. B., Abdelatif, D., Fazel, Y., Henry, L., & Wymer, M. (2016). Global epidemiology of nonalcoholic fatty liver disease — meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology, 64(1), 73–84. https://doi.org/10.1002/hep.28431
Lim, S., Taskinen, M.-R., & Borén, J. (2019). Crosstalk between nonalcoholic fatty liver disease and cardiometabolic syndrome. Obesity Reviews, 20(4), 599–611. https://doi.org/10.1111/obr.12820
Lonardo, A., Ballestri, S., Marchesini, G., Angulo, P., & Loria, P. (2015). Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome. Digestive and Liver Disease, 47(3), 181–190. https://doi.org/10.1016/j.dld.2014.09.020
Esler, W. P., & Bence, K. K. (2015). Metabolic targets in nonalcoholic fatty liver disease. Cellular and Molecular Gastroenterology and Hepatology, 1(1), 18–28. https://doi.org/10.1016/j.jcmgh.2014.11.004
Stols-Gonçalves, D., Mak, A. L., Hutten, B. A., & Nieuwdorp, M. (2023). The gut microbiome and metabolic syndrome. Endocrinology and Metabolism Clinics of North America, 52(3), 535–553. https://doi.org/10.1016/j.ecl.2023.05.003
Article written by Dr. T.S. Didwal, M.D. (Internal Medicine). This article synthesizes peer-reviewed research published through 2026. It is intended for informational and educational purposes only. Individual health decisions should always be made in consultation with a qualified healthcare professional.
Last updated: June 2026