Weight Loss vs Fat Loss: The Critical Difference Every GLP-1 User Must Understand
New 2026 research reveals how GLP-1 medications like Ozempic, Wegovy, and Mounjaro affect fat loss, muscle mass, metabolism, and long-term health.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/18/202615 min read
For decades, obesity treatment was framed as a simple equation of willpower: eat less, move more, try harder. But modern metabolic science is rewriting that narrative. A new generation of medications known as GLP-1 receptor agonists—including semaglutide (Ozempic®, Wegovy®) and tirzepatide (Mounjaro®, Zepbound®)—is transforming the treatment of obesity and type 2 diabetes by targeting the brain–gut pathways that regulate hunger, satiety, insulin signaling, and fat storage (Sawicka-Gutaj et al., 2026). In clinical trials, these therapies have produced weight-loss results once considered achievable only through bariatric surgery, with some patients losing 15–22% of their body weight over time. Yet beneath the excitement lies a more important scientific question: when the body loses weight rapidly, what exactly is being lost—fat, muscle, or both?
That distinction may determine whether weight loss improves long-term health or quietly undermines it. Muscle is not simply aesthetic tissue; it is a critical metabolic organ that supports glucose control, mobility, bone strength, and healthy ageing. Emerging evidence now shows that while GLP-1 medications preferentially reduce visceral and total fat mass, some lean tissue loss can also occur without adequate protein intake and resistance exercise (Lahav et al., 2026; Refalo et al., 2025). The future of obesity medicine may therefore depend not only on losing weight, but on losing it intelligently.
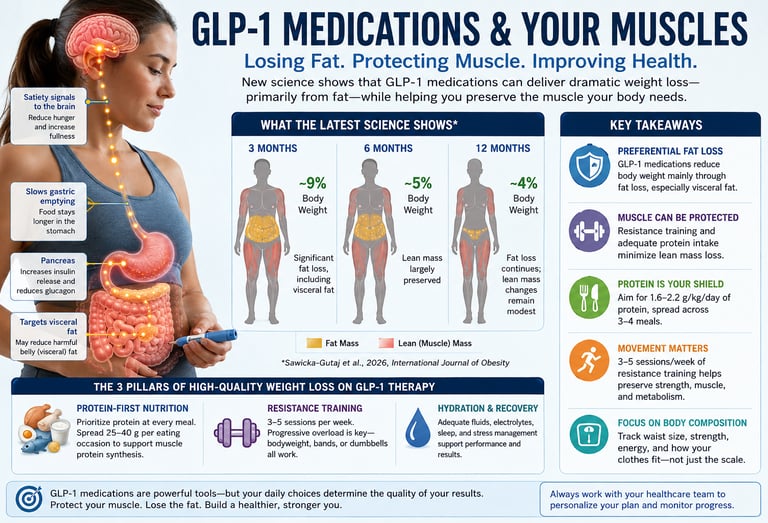
GLP-1 medications primarily reduce fat mass, especially dangerous visceral fat.
Some lean mass loss (≈20–30%) can occur without protective strategies.
Resistance training + adequate protein are the most effective ways to preserve muscle.
Tirzepatide produces greater total weight loss than semaglutide.
High-quality weight loss = maximum fat loss + minimum muscle loss.
Home-based resistance training is highly effective — no gym required.
Monitor waist circumference and strength, not just scale weight.
Best results come from combining medication with lifestyle intervention.
What Does the Latest Evidence Show?
The research team from Poznan University of Medical Sciences conducted a rigorous systematic search of PubMed, Scopus, and Web of Science—covering studies published up to December 2024—following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Sawicka-Gutaj et al., 2026
The Results: A Timeline of Body Composition Change
At 3 Months: Body weight dropped by approximately 9%, accompanied by marked reductions in fat mass and visceral adipose tissue—the dangerous deep belly fat surrounding internal organs. This early and dramatic fat loss is clinically significant, as visceral fat is strongly linked to cardiovascular disease, type 2 diabetes, and metabolic dysfunction.
At 6 Months: Weight reduction averaged 5% from baseline, with semaglutide, liraglutide, and exenatide showing broadly comparable effects. Critically, lean mass remained largely preserved at this stage—a reassuring finding for patients concerned about losing muscle alongside fat.
At 12 Months: Weight loss persisted at around 4% from baseline, though with greater variability between agents—most notably liraglutide, which showed more individual heterogeneity in outcomes. Fat mass continued to decline as the primary driver of weight reduction, while reductions in lean body mass remained modest across the cohort.
GLP-1 RAs provide clinically meaningful weight loss primarily through selective fat mass reduction, with relative preservation of lean tissue—supporting their role in achieving 'quality' weight loss." — Sawicka-Gutaj et al., 2026
Put simply: GLP-1 medications are not indiscriminate weight-loss tools. They preferentially dismantle fat—particularly the visceral variety—while sparing relatively more of your metabolically precious lean tissue. This is a meaningful distinction from historical weight-loss approaches, where crash dieting could strip away 30–40% of lost weight as muscle.
The Lean Mass Question: Should You Be Worried?
Honest medicine demands nuance. While the Sawicka-Gutaj review is encouraging about relative lean mass preservation, other meta-analyses add important context. A network meta-analysis published in early 2025, examining 22 randomized controlled trials (2,258 participants) found that GLP-1 RAs significantly reduced total body weight by a mean of 3.55 kg, fat mass by 2.95 kg, and lean mass by 0.86 kg—with lean mass loss comprising approximately 25% of total weight lost.
A separate systematic review of 36 RCTs involving 2,555 participants similarly confirmed that GLP-1 RAs decrease fat mass conspicuously—including fat mass percentage, visceral fat area, and subcutaneous fat area—while lean mass loss was observed in the majority of studies, with the effect more prominent in individuals with higher levels of overweight or obesity and in those undergoing longer-term treatment.
What does 25% lean mass loss actually mean in practice? For every 4 kilograms lost on a GLP-1 medication, approximately 1 kilogram may come from lean tissue, including muscle. Whether this is acceptable depends entirely on whether it is mitigated, and the science is increasingly clear that it can be, through two well-established interventions: resistance exercise and adequate dietary protein.
The Muscle Protector: Resistance Training During GLP-1 Therapy
A 2026 comprehensive review by Lahav, Yavetz, and Gepner published in Frontiers in Endocrinology examined resistance training as a key strategy for what they term 'high-quality weight loss'—defined not merely as a lower number on the scale, but as the selective reduction of adipose tissue while preserving fat-free mass and bone mineral density. Both men and women were included, and both sexes responded robustly.
The biological rationale is straightforward. When you perform resistance exercise—whether using gym weights, home dumbbells, resistance bands, or even bodyweight movements—you create a mechanical stimulus that signals muscle fibers to adapt and grow. This anabolic signal competes directly against the catabolic environment created by caloric restriction. When the two forces coexist, the muscle wins—or at the very least, it does not lose.
Importantly, a 2025 randomized controlled pilot trial by Binmahfoz and colleagues demonstrated that home-based resistance training programs can deliver these protective benefits even in people living with overweight or obesity—the very population most likely to be using GLP-1 medications. Participants maintained and even increased lean muscle mass during a weight loss phase, and improved their functional strength, without requiring gym memberships or expensive equipment. Progressive overload—gradually increasing the challenge—was the key variable, not the setting.
Practical Insight: If you are taking a GLP-1 medication and want to protect your muscle, you do not need to join a gym. Three to four sessions per week of progressive resistance exercise at home—using bands, dumbbells, or bodyweight—can provide meaningful protection against lean mass loss.
The Nutritional Shield: Protein Intake and Fat-Free Mass Preservation
The second pillar of lean mass protection is dietary protein—and the science here has become remarkably precise. An updated 2025 systematic review with meta-regression by Refalo, Trexler, and Helms examined how much protein resistance-trained individuals need to preserve fat-free mass during energy restriction. Their analysis revealed a clear dose-response relationship: more protein means better muscle retention, up to a point of diminishing returns.
This finding carries particular relevance for GLP-1 users. One well-documented side effect of these medications is reduced appetite—often dramatically so. While this is the mechanism behind their weight-loss efficacy, it creates a hidden risk: patients eating significantly less may also be consuming far less protein, inadvertently accelerating lean mass loss at the very time they most need adequate protein to protect it.
GLP-1 medications suppress appetite through central nervous system pathways that reduce hunger and slow gastric emptying. Patients describe feeling full after just a few bites. If those few bites are not protein-rich, muscle preservation suffers. Clinicians and dietitians working with GLP-1 patients are increasingly emphasizing protein-first eating strategies—prioritizing lean meats, eggs, dairy, legumes, or protein supplements at every meal before filling up on other foods.
"Higher leucine-rich protein intake sustains muscle protein synthesis even when energy availability is low—acting as a biological shield for your lean tissue." — Refalo, Trexler & Helms, 2025
How GLP-1 Medications Work
GLP-1 (glucagon-like peptide-1) is a hormone your gut naturally releases after eating. It signals your pancreas to release insulin, tells your liver to slow glucose production, and crucially, sends satiety signals to your brain. GLP-1 receptor agonist medications mimic and amplify these effects.
The four primary mechanisms are:
• Appetite suppression: GLP-1 RAs act on appetite centers in the brain, reducing hunger signals and increasing the sensation of fullness.
• Gastric slowing: These medications delay stomach emptying, meaning food stays in the stomach longer, extending the feeling of satiety after meals.
• Glucose regulation: They stimulate insulin release in response to meals and suppress glucagon, keeping blood sugar levels stable—important for reducing diabetes risk and managing existing type 2 diabetes.
• Visceral fat targeting: Emerging evidence suggests GLP-1 RAs may have preferential effects on metabolically harmful visceral (intra-abdominal) fat relative to subcutaneous fat.
GLP-1/GIP dual agonists (tirzepatide) add a second hormonal pathway—glucose-dependent insulinotropic polypeptide (GIP)—which further amplifies these metabolic effects and may explain the superior weight loss observed with tirzepatide compared to pure GLP-1 agonists in some trials.
Practical Applications: Maximizing Quality Weight Loss on GLP-1 Therapy
1. Prioritize Protein at Every Meal
Aim for 0.8–1.2 grams of protein per pound of body weight daily (approximately 1.8–2.6 g/kg). On reduced appetite, this requires intentional protein-first eating. Start every meal with your protein source—eggs, chicken, fish, Greek yogurt, cottage cheese, legumes, or a quality protein shake—before adding vegetables or carbohydrates.
2. Distribute Protein Throughout the Day
Research supports spreading protein intake across three to four meals or eating occasions. Aim for 25–40 grams of protein per eating occasion to optimally stimulate muscle protein synthesis at each sitting. Skipping meals or eating only once or twice, common on GLP-1 medications due to reduced appetite, may compromise total daily protein and increase lean mass loss risk.
3. Begin or Continue Resistance Training
Three to five sessions per week of progressive resistance exercise is the evidence-based recommendation. Begin with what is accessible—home bodyweight exercises, resistance bands, or light dumbbells—and progressively increase difficulty over time. Exercises that use large muscle groups simultaneously (squats, hinges, presses, rows) are particularly efficient. Even 20–30 minutes per session, three times weekly, provides significant lean mass protection.
4. Monitor Body Composition, Not Just Weight
The scale does not distinguish between fat and muscle. Tracking body composition—through DEXA scanning, BIA (bioelectrical impedance) scales, or simply measuring waist circumference and tracking strength progress—gives far more meaningful data than body weight alone. If your clothes fit better, your waist measurement is shrinking, and you are getting stronger, your weight loss is high-quality regardless of what the scale says.
5. Maintain Adequate Hydration and Electrolytes
Rapid initial weight loss on GLP-1 medications includes significant water and glycogen loss. Maintaining adequate hydration and ensuring sufficient sodium, potassium, and magnesium supports muscle function, reduces fatigue, and prevents the common side effects of early treatment.
6. Work With Your Healthcare Team
GLP-1 medication dosing, tolerability, and long-term strategy should be managed in partnership with a qualified clinician. Registered dietitians with experience in obesity medicine can help design protein-optimized meal plans compatible with reduced appetite. Exercise physiologists or certified personal trainers can develop progressive resistance programs tailored to your current fitness level and any physical limitations.
Comparing GLP-1 Agents: Does the Choice of Medication Matter?
The Sawicka-Gutaj et al. meta-analysis highlights meaningful differences between agents. At six months, semaglutide, liraglutide, and exenatide showed broadly comparable effects on body weight and composition. At twelve months, however, liraglutide demonstrated greater variability in individual responses—suggesting that some patients may respond better to one agent than another, reinforcing the importance of individualized treatment.
Tirzepatide (GLP-1/GIP dual agonist), while not the primary focus of the Sawicka-Gutaj review, consistently demonstrates superior total weight loss compared to pure GLP-1 agonists in head-to-head trials—with losses of 15–22% of body weight in some studies. Whether this greater overall weight loss comes with proportionally greater lean mass loss or whether the GIP pathway provides additional lean tissue protection remains an active area of research.
From a patient perspective, the key message is this: different medications have different efficacy and tolerability profiles. What works best for one person may not be optimal for another. The appropriate choice is a clinical conversation, not a social media decision.
The Bigger Picture: Metabolic Health Beyond the Scale
Weight loss on GLP-1 therapy consistently improves multiple cardiometabolic risk markers beyond body composition. Evidence from multiple systematic reviews and meta-analyses demonstrates reductions in BMI, waist circumference, blood pressure, HbA1c (a marker of blood sugar control), and liver fat. These benefits occur regardless of whether patients have type 2 diabetes.
A meta-analysis examining GLP-1 RAs in non-diabetic individuals with obesity found mean percentage body weight reductions of approximately 12.8%, accompanied by BMI reductions of 4.80 kg/m², waist circumference reductions of 9.78 cm, and systolic blood pressure reductions of 6.32 mmHg. These are clinically meaningful reductions that translate directly to reduced cardiovascular risk.
The visceral fat reductions observed in the Sawicka-Gutaj review are particularly significant from a metabolic standpoint. Visceral adipose tissue is not merely passive storage—it is an active endocrine organ that secretes pro-inflammatory cytokines, disrupts insulin signaling, and drives cardiovascular disease risk. Its preferential reduction with GLP-1 therapy may explain a substantial portion of the cardiometabolic benefits observed beyond simple weight reduction.
Clinical Pearls:
1. Navigating the 25% Lean Mass Loss Rule
Scientific Perspective: Meta-analyses indicate that unmitigated weight loss via GLP-1 receptor agonists (GLP-1 RAs) can result in approximately 25% of the total mass lost coming from lean tissue (including skeletal muscle). Clinicians must monitor for this to prevent sarcopenic obesity—a state where body weight decreases but body fat percentage relatively increases or muscle function drops, potentially compromising the patient's resting metabolic rate (RMR) and long-term functional capacity.
For every 4 kg you drop on the scale, about 1 kg could be muscle rather than fat if you don't actively protect it. Losing muscle makes you weaker and slows down your metabolism, making it much easier to regain weight later. The scale doesn't know the difference between fat and muscle, so focus on how your clothes fit and how strong you feel, rather than just the total number on the scale.
2. Overcoming Hormone-Induced Dietary Gaps (The "Protein-First" Mandate)
Scientific Perspective: GLP-1 RAs achieve efficacy by activating central nervous system satiety pathways and delaying gastric emptying, causing profound appetite suppression. However, this dramatically reduces total energy availability and inadvertently creates a severe deficit in essential amino acids. To maintain muscle protein synthesis (MPS) in an energy-restricted environment, targeted intake of higher leucine-rich proteins is required to act as an anabolic shield.
Because these medications slow down your stomach and make you feel full after just a few bites, it is very easy to accidentally starve your muscles of the protein they need. You need to use a "protein-first" strategy: whenever you sit down to eat, finish your eggs, chicken, fish, Greek yogurt, or protein shake before filling up on vegetables or carbs. If solid food feels unappealing, liquid protein options can be a lifesaver.
3. Demystifying the Exercise Setting (Progressive Overload vs. Gym Memberships)
Scientific Perspective: Mechanical tension is the primary driver of muscle hypertrophy and retention, providing an anabolic signal that counteracts the catabolic state of caloric restriction. Recent data by Binmahfoz et al. (2025) confirms that home-based resistance training programs utilizing progressive overload are structurally sufficient to preserve lean mass and improve functional strength in individuals with obesity, independent of traditional gym infrastructure.
You do not need a gym membership or heavy, expensive weights to work out your muscles. Doing simple exercises at home using resistance bands, light dumbbells, or your own body weight (like modified push-ups, squats, and planks) works incredibly well. The secret isn't the location; it's progressive overload—gradually making the exercises a little more challenging week by week as you get stronger.
4. The Metabolic Importance of Visceral Fat Sparing
Scientific Perspective: The 2026 Sawicka-Gutaj et al. meta-analysis highlights that GLP-1 and dual GLP-1/GIP agonists preferentially target visceral adipose tissue (the deep belly fat surrounding internal organs) while relatively sparing lean tissue. Because visceral fat acts as an active, hazardous endocrine organ that secretes pro-inflammatory cytokines and drives insulin resistance, its selective reduction explains why patients experience massive improvements in cardiometabolic markers (blood pressure, HbA1c, liver fat) early in therapy (by month 3).
These medications are uniquely smart: they specifically target the most dangerous type of fat in your body—the hidden "visceral" fat wrapped around your internal organs that causes heart disease and diabetes. Even if you are worried about muscle loss, the science shows the drug is actively working to dismantle this toxic belly fat first, which is why your health markers and waistline improve so quickly.
5. Framing Obesity as a Chronic Biological State
Scientific Perspective: Clinical data demonstrate a high incidence of weight regain within 1 to 2 years following the discontinuation of GLP-1 therapy. This trajectory should not be interpreted as a behavioral or moral failure on the part of the patient, but rather as evidence of the chronic, highly regulated biological nature of obesity. Pharmacotherapy modifies the metabolic setpoint temporarily; therefore, long-term management strategies must treat obesity as a chronic disease requiring sustained lifestyle or therapeutic maintenance.
If someone stops taking a GLP-1 medication and the weight starts to return, it is not a lack of willpower or a personal failure. Obesity is a chronic biological medical condition, much like high blood pressure. These medications work beautifully while you take them, but keeping the weight off long-term requires treating it as a permanent journey—one where building a foundation of muscle through resistance training serves as your best natural insurance policy against regaining fat.
Frequently Asked Questions
Q: I've started a GLP-1 medication and I'm barely hungry. How do I get enough protein when I can barely eat?
A: This is one of the most common—and important—challenges on GLP-1 therapy. The protein-first approach is your best strategy: at every meal or eating occasion, no matter how small, start with your protein source. Liquid proteins (Greek yogurt, protein shakes, milk) can help when solid food feels unappealing. High-quality protein supplements can fill gaps. Even small, frequent protein-rich snacks (a hard-boiled egg, cottage cheese, edamame) count toward your daily total. Aim for at least 25–30 grams per eating occasion.
Q: Will I definitely lose muscle on a GLP-1 medication?
A: Not necessarily, and not significantly if you take protective steps. The meta-analyses show that GLP-1 RAs predominantly reduce fat mass, with lean mass changes that, while statistically significant, are relatively modest. Combined with resistance training and adequate protein—the two most evidence-supported strategies for lean mass preservation—many patients maintain or even improve their muscle quality during treatment. Your outcome is substantially within your influence.
Q: I'm not a gym person. Can I still protect my muscles without lifting heavy weights?
A: Absolutely. The research by Binmahfoz and colleagues (2025) demonstrated meaningful muscle preservation and strength gains from home-based resistance training in people with obesity—no gym membership required. Resistance bands, bodyweight exercises (push-ups, squats, lunges, planks), and light adjustable dumbbells provide sufficient mechanical stimulus when performed progressively. The key is progressive overload—making the exercise gradually more challenging over time—not the equipment.
Q: How long does it take for GLP-1 medications to produce meaningful results?
A: The Sawicka-Gutaj et al. (2026) meta-analysis found approximately 9% body weight reduction at 3 months, with significant fat mass and visceral fat reductions occurring at this early stage. Clinical improvements in blood sugar, blood pressure, and waist circumference are often measurable within weeks to a few months. The full trajectory of weight loss typically unfolds over 12 months, with variability between individuals and between specific medications.
Q: I've heard tirzepatide is more powerful than semaglutide. Should I ask for that specifically?
A: Tirzepatide (a dual GLP-1/GIP agonist) does show numerically greater weight loss in head-to-head comparisons with semaglutide in some trials, with some patients losing 15–22% of body weight. However, 'more powerful' is not always 'right for you.' Efficacy, tolerability, cost, insurance coverage, and individual response all matter. This is a clinical conversation best had with a physician who knows your full medical history. Both agents are evidence-based and clinically meaningful.
Q: Are GLP-1 medications safe long-term? What about the cancer concerns I've seen online?
A: Rigorous systematic reviews examining oncological safety of GLP-1 receptor agonists have not established a causal link between these medications and increased cancer risk when studied in properly designed randomized controlled trials. Observational concerns about thyroid and pancreatic cancer have not been confirmed in RCT-level evidence. That said, these medications are still relatively new at population scale, and ongoing pharmacovigilance is appropriate. Your clinician is the right person to discuss the individual risk-benefit balance.
Q: What happens to my metabolism if I take a GLP-1 medication without exercising?
A: Without resistance exercise, a greater proportion of your weight loss may come from lean mass rather than fat—potentially reducing your resting metabolic rate, the calories your body burns at rest. This creates a less favorable metabolic state for long-term weight maintenance and may make weight regain more likely if medication is ever discontinued. Resistance training specifically preserves the metabolically active lean tissue that keeps your calorie burn higher over time, making exercise not merely complementary but strategically important for sustained results.
A Clinician’s Perspective: What We See in Real Practice
From a physician’s perspective, GLP-1 medications are changing obesity medicine in ways few therapies ever have. Patients who previously struggled for years with hunger, cravings, insulin resistance, and repeated cycles of weight regain are now achieving clinically meaningful fat loss with improvements in blood sugar, blood pressure, sleep apnea, fatty liver disease, and mobility. But in practice, one reality quickly becomes clear: not all weight loss is metabolically equal.
Consider a typical clinical scenario. A 52-year-old woman with obesity, prediabetes, hypertension, and knee osteoarthritis begins semaglutide therapy. Over six months, she loses 14 kilograms. Initially, she is thrilled—but she also reports fatigue, reduced strength when climbing stairs, and difficulty carrying groceries. On closer evaluation, her protein intake has fallen dramatically because of appetite suppression, and she has done no resistance exercise. Her body weight improved, but part of the lost tissue was metabolically important lean mass.
Now compare this with another patient of similar age and weight who combines GLP-1 therapy with protein-focused nutrition and three weekly resistance-training sessions. That patient loses a similar amount of weight, but waist circumference falls substantially, strength improves, mobility increases, HbA1c normalizes, and resting energy levels remain high. The difference is not simply the medication—it is the preservation of muscle during fat loss.
This is why many obesity specialists now emphasize “body composition medicine,” not merely weight reduction. The clinical goal is no longer just a smaller body, but a healthier metabolic profile with preserved strength, functional independence, and long-term resilience. In modern obesity care, the most successful outcomes occur when pharmacology, nutrition, and exercise physiology work together—not in isolation.
Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. GLP-1 medications are prescription therapies that carry specific indications, contraindications, and risks; they must be prescribed and monitored by a qualified healthcare professional. Readers should consult their physician before starting, changing, or stopping any medication or exercise and dietary program, particularly if they have chronic medical conditions, are pregnant, or are recovering from illness or injury. The author and publisher are not responsible for any outcomes resulting from the application of this information.
Related Articles:
GLP-1 Muscle Loss: You’re Losing Weight But Are You Losing Strength Too?
Obesity is a Disease: How GLP-1 Medications Are Changing Treatment Forever
Do You Need to Go Low-Carb for Diabetes? Mediterranean vs Low-Carb Explained (Doctor’s Guide)
Can You Reverse Type 2 Diabetes with Diet? Science-Based Guide 2026
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
References
Basami, M., Karimi, M., Poorhabibi, H., Sadeghi, A., & Amini, M. A. (2026). Trends in research combining resistance training and nutrition: A bibliometric analysis (2010–2024). Sport Sciences for Health, 22, 70. https://doi.org/10.1007/s11332-026-01653-5
Binmahfoz, A., Johnston, L., Dunning, E., Gray, C. M., & Gray, S. R. (2025). The effects of a home-based resistance training programme on body composition and muscle function during weight loss in people living with overweight or obesity: A randomized controlled pilot trial. Nutrition & Metabolism, 22, 90. https://doi.org/10.1186/s12986-025-00986-1
Chen, W. (2025). Nutritional interventions in muscle hypertrophy research: A scientometric analysis within the context of resistance training (1992–2025). Journal of Health, Population and Nutrition, 44(1), 272. https://doi.org/10.1186/s41043-025-01031-w
Lahav, Y., Yavetz, R., & Gepner, Y. (2026). Resistance training as a key strategy for high-quality weight loss in men and women. Frontiers in Endocrinology, 16, Article 1725500. https://doi.org/10.3389/fendo.2026.1725500
Refalo, M. C., Trexler, E. T., & Helms, E. R. (2025). Effect of dietary protein on fat-free mass in energy-restricted, resistance-trained individuals: An updated systematic review with meta-regression. Strength and Conditioning Journal. https://doi.org/10.1519/SSC.0000000000000888
Sawicka-Gutaj, N., Gruszczyński, D., Nijakowski, K., et al. (2026). GLP-1 agonists and changes in body mass and composition in adults with overweight or obesity with or without type 2 diabetes mellitus: A systematic review and meta-analysis. International Journal of Obesity. https://doi.org/10.1038/s41366-026-02088-1