Do You Need to Go Low-Carb for Diabetes? Mediterranean vs Low-Carb Explained (Doctor’s Guide)
Low-carb vs Mediterranean diet for Type 2 Diabetes: compare blood sugar control, weight loss, and heart health. Expert 2026 guide to choose the right plan.
DIABETESNUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/9/202617 min read
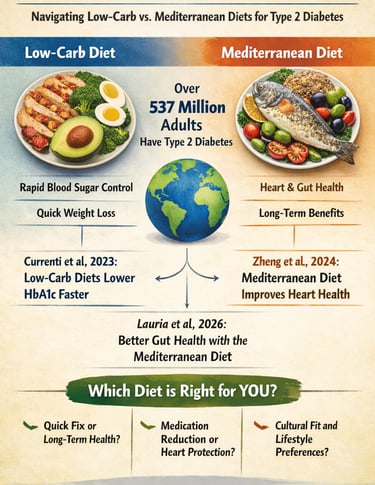
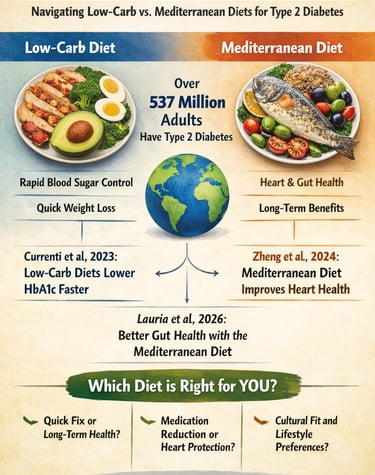
For people with Type 2 Diabetes, both low-carb and Mediterranean diets are effective—but serve different goals.
Low-carb diets reduce blood sugar faster and may help lower HbA1c within weeks, making them ideal for patients needing rapid glucose control.
Mediterranean diets provide strong long-term benefits, especially for heart health, weight maintenance, and gut health, with better sustainability.
Best choice:
Choose low-carb if your HbA1c is high and you need quick improvement.
Choose Mediterranean if your focus is long-term health and cardiovascular protection.
Consider a hybrid approach for balanced, sustainable results.
Bottom line: The most effective diet is the one you can follow consistently, tailored to your medical needs, lifestyle, and cultural food habits.
Clinician Perspective: Practical, Evidence-Based Takeaways
Match the diet to the clinical priority
For patients with markedly elevated HbA1c (>9%) or symptomatic hyperglycemia, a low-carbohydrate approach can deliver faster glycemic reductions and facilitate early medication de-escalation. For those with established cardiovascular disease or high risk, a Mediterranean pattern offers more robust long-term cardioprotection.Think beyond glucose: cardiometabolic risk matters
Glycemic control is only one component of diabetes care. Lipids, blood pressure, inflammation, and weight trajectory should guide dietary decisions. Mediterranean diets consistently improve LDL, Blood pressure, and inflammatory markers, while low-carb diets excel in lowering triglycerides and raising HDL.Monitor lipids intelligently, not simplistically
LDL may rise in a subset of patients on low-carb diets. Evaluate the full lipid profile—preferably including ApoB or non-HDL cholesterol—before making clinical decisions, rather than reacting to LDL alone.Preserve gut health and fibre intake
High-fibre, plant-forward diets support microbiome diversity and insulin sensitivity. If prescribing low-carb, ensure adequate intake of non-starchy vegetables, seeds, and nuts to mitigate fibre deficits.Medication safety is non-negotiable
Patients on insulin, sulfonylureas, or SGLT2 inhibitors require proactive dose adjustments when initiating carbohydrate restriction to avoid hypoglycemia or ketoacidosis.Adherence determines real-world success
The most effective diet is the one a patient can sustain. Mediterranean patterns generally show higher long-term adherence, while low-carb works well for patients who prefer structured, rule-based approaches.Use a dynamic, phased strategy
A pragmatic approach is to begin with moderate carbohydrate restriction for rapid control, then transition toward a Mediterranean-style pattern for sustainability and cardiovascular benefit.Integrate lifestyle pillars
Diet should not be prescribed in isolation—combine with resistance training, sleep optimization, and weight management for maximal metabolic impact.
“Doctor, do I have to give up Carbs forever?”
This is often the first question patients ask after being diagnosed with Type 2 Diabetes—and it reflects a deeper confusion created by conflicting nutrition advice. On one side, low-carbohydrate diets promise rapid blood sugar control and even remission. On the other, the Mediterranean diet is consistently ranked among the healthiest eating patterns for heart and metabolic health. For many patients, these approaches seem mutually exclusive. In reality, both are grounded in strong scientific evidence—and both can work.
Globally, more than 537 million adults live with diabetes, and nutrition remains the most powerful non-pharmacological tool for managing it. Yet, there is no universal “best diet.” A 16-week randomized trial by Currenti et al. (2023) demonstrated that low-carbohydrate diets can produce greater short-term reductions in HbA1c compared to Mediterranean diets—particularly in individuals with poorly controlled diabetes. At the same time, a large meta-analysis by Zheng et al. (2024) showed that Mediterranean-style eating delivers consistent improvements in glycemic control, body weight, and cardiovascular risk factors over the long term. More recently, Lauria et al. (2026) added another layer to this discussion, demonstrating that the Mediterranean diet favorably alters the gut microbiome—enhancing insulin sensitivity through increased production of short-chain fatty acids.
So the real question is not which diet is “better,” but which is better for you. Should you prioritize rapid glucose reduction or long-term sustainability? Do you need aggressive metabolic correction or a lifelong, heart-protective eating pattern? And most importantly, can you follow the plan consistently within your cultural and lifestyle context?
This article cuts through the noise, translating the latest evidence into practical, real-world guidance to help you make the right choice with clarity and confidence.
The Low-Carbohydrate Diet
A low-carbohydrate (low-carb) diet typically restricts daily carbohydrate intake to below 130 grams per day (moderate low-carb) or, in the case of very-low-carb or ketogenic variants, to below 50 grams per day. Nutritional emphasis falls on lean and fatty proteins, healthy dietary fats (such as olive oil, nuts, and avocado), and non-starchy vegetables (leafy greens, cucumber, capsicum, cauliflower). Foods minimized or eliminated include refined grains, sugary beverages, bread, rice, pasta, and most fruits in their standard quantities.
The Mediterranean Diet
The Mediterranean diet is not a single prescriptive plan but a broadly plant-forward eating pattern inspired by the traditional cuisines of Southern Europe and the Eastern Mediterranean. Its core elements include abundant vegetables, fruits, legumes, whole grains, fish, olive oil, and nuts — with moderate intake of dairy and poultry, and limited red meat and sweets. It does not prescribe a strict carbohydrate target; rather, it emphasizes food quality, dietary diversity, and eating in social contexts.
Comparison Table: Low-Carb vs Mediterranean Diet
1. Carbohydrate Intake
Low-Carb: Typically restricted to <50 g/day (ketogenic) or up to ~130 g/day; prioritizes tight glycemic control.
Mediterranean: Moderately higher (~200–300 g/day), with emphasis on complex, minimally processed carbohydrates.
2. Protein Content
Low-Carb: Relatively high (~25–35% of total calories); supports satiety, muscle preservation, and reduced glycemic variability.
Mediterranean: Moderate (~15–20%); derived from fish, poultry, legumes, and dairy, with less reliance on red meat.
3. Dietary Fat Profile
Low-Carb: High total fat intake; includes both saturated fats and unsaturated fats (nuts, seeds, oils), depending on food choices.
Mediterranean: Fat-rich but quality-focused; predominantly monounsaturated fats (MUFAs), especially from extra virgin olive oil and nuts.
4. Fibre and Micronutrients
Low-Carb: Moderate; requires planning (leafy greens, seeds, fibre supplements) to meet daily fibre needs.
Mediterranean: Naturally high; abundant in vegetables, fruits, legumes, and whole grains, supporting gut and metabolic health.
5. Primary Food Sources
Low-Carb: Eggs, meat, fish, non-starchy vegetables (e.g., spinach, cauliflower), nuts, seeds, and full-fat dairy.
Mediterranean: Plant-forward pattern with vegetables, legumes, whole grains, fish, olive oil, nuts, and seasonal fruits.
6. Role of Grains
Low-Carb: Minimal or excluded; grains are limited due to their impact on postprandial glucose.
Mediterranean: Included in moderation; favors whole or traditional grains (e.g., millets, ancient grains, sourdough).
7. Sustainability and Adherence
Low-Carb: Structured and effective short-term; adherence may decline due to dietary restrictions.
Mediterranean: Highly sustainable; diverse, palatable, and culturally adaptable, supporting long-term adherence.
Clinical Insight
For patients with Type 2 Diabetes, the choice is less about superiority and more about alignment with metabolic goals, lifestyle, and long-term adherence.
Head-to-Head Evidence: What the 2023–2026 Research Shows
Glycemic Control: HbA1c and Fasting Blood Glucose
A pivotal 16-week randomised clinical study by Currenti et al. (2023) directly compared a low-carbohydrate diet with a Mediterranean diet in overweight and obese patients with Type 2 diabetes. Both groups experienced statistically significant reductions in HbA1c, fasting glucose, and body weight. Crucially, however, the low-carbohydrate group showed a greater magnitude of HbA1c reduction in the short term — a finding consistent with the mechanistic logic that restricting dietary carbohydrate directly attenuates postprandial glucose excursions. This rapid glycemic improvement is particularly meaningful for patients whose HbA1c is above 9% and who need to reduce or discontinue diabetes medications quickly.
At the same time, a rigorous meta-analysis by Zheng et al. (2024), pooling data from multiple randomised controlled trials, demonstrated that the Mediterranean diet produces statistically significant and clinically meaningful improvements in HbA1c, fasting blood glucose, and insulin resistance over the medium-to-long term in patients with Type 2 diabetes. The effect size was consistent across trials, suggesting that the Mediterranean diet's benefits are durable, not merely a short-term novelty response.
Research Insight
Low-carb diets often deliver a stronger initial HbA1c reduction (commonly 0.3–0.5% greater in the first 3–6 months), but Mediterranean diet benefits are steadier and more sustained over 12+ months — making it a compelling strategy for lifelong management (Currenti et al., 2023; Zheng et al., 2024).
Weight Loss and Body Composition
Both diets produce meaningful weight loss — a critical therapeutic goal given that even a 5–10% reduction in body weight can substantially improve glycemic control and reduce cardiovascular risk in individuals with T2D. Low-carb diets typically produce greater initial weight loss, partially due to rapid glycogen depletion (and associated water loss) in the early weeks, and partly due to the satiety-promoting effects of higher protein and fat intake. However, Zheng et al.'s (2024) meta-analysis confirms that the Mediterranean diet also produces significant reductions in body weight and body mass index, with differences between the two diets narrowing considerably after six to twelve months of follow-up.
Cardiovascular and Metabolic Risk Markers
This is arguably the area where the Mediterranean diet holds its most compelling advantage. The meta-analysis by Zheng et al. (2024) documented consistent improvements in lipid profiles — specifically reductions in total cholesterol, LDL cholesterol, and triglycerides — alongside improvements in blood pressure and inflammatory markers in patients with T2D following a Mediterranean diet. These cardiovascular benefits are particularly significant because Type 2 diabetes is itself a major risk factor for cardiovascular disease.
Low-carb diets reliably reduce triglycerides (often dramatically) and raise HDL cholesterol, both of which are favourable outcomes. However, some individuals — particularly lean individuals or those with a specific genetic lipid phenotype — may experience a rise in LDL cholesterol on a high-fat, low-carb regimen. The clinical significance of this depends on the LDL particle size (large, buoyant LDL is less atherogenic than small, dense LDL), and on the overall metabolic context (Gorodeski Baskin & Karp, 2025).
For patients with existing cardiovascular disease or high cardiovascular risk, the Mediterranean diet's track record — including the landmark PREDIMED trial data — makes it the more cautious and evidence-supported first choice.
Gut Microbiome and Long-Term Health
An emerging and particularly exciting body of research concerns the gut microbiome — the trillions of microorganisms residing in the human intestine that profoundly influence metabolic health, immune function, and even mental well-being. A 2026 systematic review and meta-analysis by Lauria et al. — the most current evidence available at time of writing — examined the effects of the Mediterranean diet on gut microbiota composition and T2D outcomes across multiple intervention trials.
The findings were striking: Mediterranean diet adherence was associated with significant favourable shifts in gut microbiota diversity, including increases in beneficial short-chain fatty acid (SCFA)-producing bacteria. These microbiome changes correlated with improved glycemic control and reduced systemic inflammation, suggesting that part of the Mediterranean diet's benefit in T2D operates via the gut-metabolic axis. Low-carb diets, by contrast, reduce fibre intake (particularly fermentable fibres from legumes and whole grains), which may have neutral-to-negative effects on microbiome diversity unless deliberately compensated for through careful food choices.
2026 Research Highlight
Lauria et al. (2026) found that Mediterranean diet adherence positively reshapes gut microbiota in people with T2D — improving bacterial diversity and producing metabolites that support insulin sensitivity. This gut-health dimension adds a powerful, underappreciated mechanism to the Mediterranean diet's benefit profile.
Diabetes Remission
Both diets have been associated with Type 2 diabetes remission in recent-onset cases, particularly when combined with significant caloric restriction or very-low-calorie approaches. Very-low-carb and ketogenic diets have demonstrated particularly high short-term remission rates in early-stage T2D when implemented under close medical supervision. However, remission maintenance beyond two years requires sustained dietary adherence — a domain where the Mediterranean diet's higher palatability and cultural flexibility may offer a meaningful long-term advantage (Gorodeski Baskin & Karp, 2025).
Addressing Common Concerns
LDL Cholesterol on a Low-Carb Diet
While low-carb diets typically improve overall lipid profiles (lower triglycerides, higher HDL), a subset of patients — often lean, active individuals — may see LDL rise. Experts advise focusing on fat quality (prioritising monounsaturated fats from olive oil, nuts, and avocado rather than saturated fat from processed meats) and monitoring lipid panels at 3-month intervals. If LDL continues to rise meaningfully, transitioning toward a Mediterranean pattern or a hybrid approach is clinically prudent (Gorodeski Baskin & Karp, 2025).
Fibre Intake and Gut Health on Low-Carb Diets
The Mediterranean diet is naturally high in fibre from vegetables, legumes, whole grains, and fruits. Low-carb dieters must proactively plan their fibre intake through non-starchy vegetables (broccoli, spinach, flaxseeds, chia seeds) and nuts to avoid constipation and microbiome disruption. Lauria et al. (2026) underscore that maintaining microbiome diversity is a meaningful clinical goal in T2D management, not merely a wellness trend.
Medication Interactions and Safety
Important Safety Note
Patients on SGLT2 inhibitors, sulfonylureas, or insulin must not embark on a very-low-carb diet without informing their physician first. The risk of diabetic ketoacidosis (with SGLT2 inhibitors) and hypoglycaemia (with insulin/sulfonylureas) is real and requires medication dosage adjustments under medical supervision.
Sustainability and Adherence
The best diet is the one a patient can actually follow. Gorodeski Baskin & Karp (2025), reviewing four evidence-based nutrition options for T2D, emphasise that long-term adherence is the primary determinant of real-world dietary efficacy. The Mediterranean diet consistently demonstrates higher long-term adherence rates due to its food variety, flavour richness, cultural flexibility, and absence of absolute food restrictions. Low-carb diets suit patients who prefer clear rules and structure, but may feel prohibitively restrictive for those with strong cultural attachments to grain-based staples.
Which Diet Fits You Best? A Practical Decision Guide
Rather than prescribing a universal winner, use the following evidence-aligned framework to identify your optimal starting point. Always discuss with your healthcare team before making major dietary changes.
Choose Low-Carb If You…
Have HbA1c above 9% and need rapid glucose reduction
Want to reduce or eliminate diabetes medications quickly
Were recently diagnosed (within 2–3 years)
Have significant insulin resistance or metabolic syndrome
Prefer clear rules and structured eating patterns
Have tried Mediterranean without sufficient glycemic improvement
Choose Mediterranean If You…
Have existing heart disease or high cardiovascular risk
Want long-term, sustainable lifestyle change
Value food variety, enjoyment, and cultural flexibility
Have struggled with the restrictiveness of low-carb before
Are concerned about gut health and microbiome diversity
Have well-controlled HbA1c and want to maintain it
Consider a Hybrid "Low-Carb Mediterranean" If You…
Want the rapid glycemic benefits of low-carb AND the cardiovascular protection of Mediterranean
Love olive oil, fish, vegetables, and nuts — but need to moderate grains and legumes
Have multiple metabolic goals (glucose, weight, lipids, and gut health simultaneously)
Want to transition gradually: start with moderate low-carb, progressively add Mediterranean elements as glucose stabilises
Cultural Adaptations: Making It Work Worldwide
One of the most significant barriers to implementing evidence-based dietary patterns in South Asian and other non-Western populations is the perception that these diets are culturally foreign. They are not — both patterns can be readily adapted to traditional Indian cuisine with creativity and knowledge.
Indian Mediterranean Diet Adaptations
Substitute olive oil with mustard oil for everyday cooking (similar monounsaturated fatty acid profile), use dals (lentils) and rajma as your legume staples, incorporate millets (bajra, jowar, ragi) as whole-grain alternatives to refined wheat, use mustard-spiced grilled fish or chicken as your lean protein, and use homemade curd (dahi) instead of Greek yogurt. Turmeric, ginger, and garlic — cornerstones of Indian cooking — are themselves powerful anti-inflammatory agents that synergise beautifully with Mediterranean principles.
Indian Low-Carb Diet Adaptations
Focus on non-starchy sabzi (palak, methi, lauki, tinda, bhindi), paneer as a high-protein, low-carb staple, eggs prepared in various spiced preparations, curd (unsweetened), chicken or fish in Indian spice marinades, and generous use of ghee and mustard oil. Roti and rice are replaced or minimised — one small bajra or jowar roti may be permitted in moderate low-carb versions. Besan (gram flour) in controlled quantities can substitute for refined flour.
Universal Practical Tips
Food sequencing: With any diet, eat salad and vegetables first, protein second, and carbohydrates last — this simple sequence blunts postprandial glucose spikes significantly.
Consistent meal timing: Irregular meal timing disrupts circadian insulin rhythms. Aim for meals within a consistent 1-hour window each day.
Chew slowly and eat mindfully: Satiety signals take ~20 minutes to register. Slower eating naturally reduces caloric intake.
Monitor personally: A continuous glucose monitor (CGM) for even 2 weeks can reveal your unique glucose response to specific foods — invaluable for personalising any diet.
Sample 7-Day Meal Plans:
Sample Day — Mediterranean Diet
Breakfast
Vegetable omelette (2 eggs) with spinach, tomatoes, and onions sautéed in olive oil + plain yogurt + a small handful of walnuts
Mid-morning
Mixed nuts (almonds, walnuts) + unsweetened green tea or black coffee
Lunch
Grilled vegetables (zucchini, eggplant, bell peppers) + 1 serving whole grain (quinoa or whole-grain bread) + lentil or chickpea salad + side of yogurt
Snack
Roasted chickpeas or a fresh fruit (apple or pear)
Dinner
Grilled fish (salmon, sardines, or mackerel) + sautéed leafy greens (spinach or kale) + mixed vegetable salad with olive oil and lemon dressing + small portion of legumes (beans or lentils)
Sample Day — Low-Carb Diet | ~70–100 g carbs
Breakfast
Scrambled eggs (3 eggs) with spinach and cheese cooked in olive oil or butter + unsweetened coffee or tea
Mid-morning
Almonds or walnuts + plain yogurt with a teaspoon of flaxseeds
Lunch
Grilled chicken or tofu + sautéed non-starchy vegetables (broccoli, zucchini, bell peppers) + large green salad with olive oil dressing
Snack
Plain yogurt with chia seeds or a small portion of berries
Dinner
Grilled salmon or lean meat + roasted low-carb vegetables (cauliflower, asparagus) + fresh salad with olive oil dressing
Clinical Note
For individuals with Type 2 Diabetes, both patterns can be adapted globally using locally available foods. The key principles remain consistent:
Prioritize whole, minimally processed foods
Adjust carbohydrate quantity based on metabolic goals
Maintain protein adequacy and healthy fat quality
The effectiveness of any plan ultimately depends on consistency, personalization, and regular metabolic monitoring.
Practical Applications for Long-Term Success
Start with Medical Nutrition Therapy
Work with a registered dietitian experienced in diabetes before making major dietary changes. Medication adjustments often accompany dietary transitions.
Use a CGM for Personalised Data
A continuous glucose monitor for even 14 days reveals your unique glycemic response to foods — far more useful than generic guidelines alone.
Pair with Resistance Training
Muscle is your largest glucose disposal tissue. Even 2–3 sessions of resistance exercise weekly dramatically amplifies the benefit of any dietary pattern.
Prioritise Sleep and Meal Timing
Poor sleep increases cortisol and insulin resistance overnight. Consistent meal timing (within a 10-hour eating window) supports circadian metabolic health.
Consider a Transition Strategy
Start with moderate low-carb (130g/day) for the first 3 months to achieve rapid glycemic gains, then progressively incorporate Mediterranean elements for long-term sustainability.
Reassess Every 3–6 Months
Schedule structured reviews with your doctor or dietitian. Labs (HbA1c, lipids, kidney function), weight, energy levels, and medication needs should all inform dietary adjustments.
Frequently Asked Questions
Can I follow a low-carb diet if I am on insulin or sulfonylureas?
Yes, but only under close medical supervision. Low-carb diets can reduce blood glucose rapidly, which increases the risk of hypoglycaemia if insulin or sulfonylurea doses are not adjusted downward in parallel. Always inform your physician before reducing carbohydrate intake significantly — medication changes must follow simultaneously, not after the fact.
Is the Mediterranean diet effective for Indian patients with Type 2 diabetes?
Absolutely. While the classic Mediterranean diet is based on Southern European ingredients, its core principles — abundant vegetables, legumes, healthy fats, fish, and whole grains — map beautifully onto Indian cuisine. Dals, millets, mustard oil, curd, paneer, and Indian spices like turmeric and fenugreek align closely with Mediterranean nutritional philosophy. The evidence for the diet's efficacy in diverse populations, including South Asians, is growing.
Will a low-carb diet raise my LDL cholesterol?
It may, in a subset of individuals — particularly lean patients with a genetic tendency called "hyperresponder" lipid phenotype. However, this LDL rise is often in the larger, less atherogenic (buoyant) LDL particles, which carry lower cardiovascular risk. The clinical picture also includes improved triglycerides and HDL. That said, if your LDL rises significantly on a low-carb diet, discuss with your physician whether a Mediterranean or hybrid approach is more appropriate for your cardiovascular risk profile (Gorodeski Baskin & Karp, 2025).
How long does it take to see results on each diet?
Low-carb diets can produce measurable reductions in fasting glucose and postprandial spikes within days to two weeks. HbA1c typically reflects 3-month averages, so clinically meaningful reductions appear at the first follow-up. The Mediterranean diet shows meaningful HbA1c improvements over 3–6 months, with cardiovascular benefits (lipids, blood pressure, inflammation) accruing over 6–12 months of consistent adherence. Both produce weight loss detectable within the first 4–8 weeks (Currenti et al., 2023; Zheng et al., 2024).
Does the Mediterranean diet help with gut health in Type 2 diabetes?
Yes — and this is one of the most exciting recent findings. Lauria et al.'s 2026 systematic review and meta-analysis found that Mediterranean diet adherence significantly improves gut microbiota diversity and increases populations of beneficial short-chain fatty acid-producing bacteria. These microbiome changes correlate with improved glycemic control and reduced inflammation — suggesting a bidirectional relationship between gut health and metabolic health that the Mediterranean diet uniquely addresses through its rich fibre and polyphenol content.
Can I combine both diets? Is a hybrid approach safe and effective?
Yes, a "Low-Carb Mediterranean" hybrid is not only safe — it is increasingly recommended by clinicians as a pragmatic and highly effective compromise. This approach restricts refined carbohydrates and high-glycaemic foods (as in low-carb) while emphasising the Mediterranean diet's food quality framework: olive oil, fish, nuts, legumes (in moderated quantities), and abundant non-starchy vegetables. It captures glycemic benefits from carbohydrate restriction while preserving the cardiovascular and gut-health benefits of Mediterranean food quality.
Is one diet better for weight loss than the other in Type 2 diabetes?
Low-carb diets typically produce greater weight loss in the short term (first 3–6 months), partly due to water loss from glycogen depletion and partly due to the high satiety of protein and fat. However, Zheng et al.'s (2024) meta-analysis shows that the Mediterranean diet also produces significant, clinically meaningful weight loss, and the gap between the two diets narrows considerably after 6–12 months. Long-term, the Mediterranean diet may sustain weight management better due to its higher adherence rates and less restrictive nature.
Clinical pearls
1. The "Muscle-as-Medicine" Principle
Scientific Perspective: Skeletal muscle is the body’s largest organ for glucose disposal. Resistance training increases the expression of GLUT4 transporters, allowing for insulin-independent glucose uptake. In the context of aging (geroscience), maintaining muscle mass is a primary defense against metabolic "inflexibility."
Don't just focus on what you eat; focus on the "engine" that burns it. Building even a small amount of muscle through strength training acts like an extra storage tank for sugar, making your blood sugar much easier to manage even when you have a higher-carb meal.
2. The "Fiber-First" Sequencing Effect
Scientific Perspective: Ingesting fiber (pre-loading) before carbohydrates stimulates the secretion of Glucagon-like peptide-1 (GLP-1) and slows gastric emptying. This creates a physical "mesh" in the small intestine that delays glucose absorption, flattening the postprandial curve.
The order in which you eat matters as much as what you eat. Always start your meal with a bowl of salad or a fiber-rich sabzi before touching your roti or rice. This "layers" your stomach and prevents a sugar spike, acting like a natural version of diabetes medication.
3. The "Lipid Quality Over Quantity" Shift
Scientific Perspective: On low-carb regimens, the focus must shift from total fat to the MUFA:SFA ratio. High intake of saturated fats can downregulate LDL receptors in some genotypes, leading to a rise in ApoB-containing lipoproteins. Prioritizing Monounsaturated Fatty Acids (MUFAs) like those in mustard oil or olive oil maintains membrane fluidity and cardiovascular health.
Going "Low-Carb" isn't a license to eat unlimited butter or fatty red meats. To protect your heart, your fats should come from "liquid" oils (like mustard or olive), nuts, and seeds. Think of these as "clean fuel" that keeps your arteries clear while your sugar stays low.
4. The Circadian Metabolic Window
Scientific Perspective: Peripheral clocks in the liver and pancreas dictate that insulin sensitivity is highest in the morning and lowest in the evening. Late-night feeding disrupts melatonin-insulin signaling, leading to prolonged nocturnal hyperglycemia and poor sleep quality.
Your body processes sugar differently at 8:00 AM than it does at 10:00 PM. Aim to eat your largest meals during daylight hours and keep your dinner light and early. Eating late at night is like trying to put gas in a car when the station is closed; it just creates a mess in your system.
5. The Microbiome-Glycemic Connection
Scientific Perspective: The Mediterranean diet’s efficacy is partially mediated by the production of Short-Chain Fatty Acids (SCFAs) like butyrate by gut bacteria. These metabolites cross the gut barrier and improve systemic insulin sensitivity by activating G-protein-coupled receptors (GPR41/43).
You are eating for two: yourself and your gut bacteria. When you eat a diverse range of plant fibers (as in the Mediterranean or Indian-adapted diets), you are "fertilizing" a pharmacy inside your gut. These bacteria then produce chemicals that actually help your body lower its own blood sugar.
Author’s Note
As a clinician working closely with patients living with Type 2 Diabetes, I have seen firsthand how overwhelming nutrition advice can become. Patients are often caught between extremes—being told to eliminate entire food groups on one hand, and to “eat everything in moderation” on the other. The truth, as always in medicine, lies somewhere more nuanced.
This article is not written to declare a winner between low-carbohydrate and Mediterranean diets. Instead, it is meant to translate evolving scientific evidence into practical, patient-centred guidance. Both dietary patterns are powerful tools—when applied thoughtfully, monitored carefully, and adapted to the individual sitting in front of you.
Equally important is cultural context. Food is not just biochemistry; it is identity, tradition, and daily life. Any dietary approach that ignores this is unlikely to succeed in the long term. That is why global and Indian adaptations are emphasized here—not as modifications, but as essential components of effective care.
Finally, it is worth emphasizing that no diet works in isolation. Sustainable improvements in metabolic health come from the integration of nutrition, physical activity, sleep, and behavioral consistency. Small, consistent changes—guided by data and supported by clinical follow-up—often achieve more than drastic, short-lived interventions.
If there is one takeaway I hope you carry forward, it is this: the goal is not dietary perfection, but metabolic progress that you can sustain for life.
What I tell my patients in the clinic
Start with a plan you can sustain—low-carb if sugars are high and need quick control, Mediterranean if long-term heart health is the priority.
Focus less on labels and more on basics: real food, fewer refined carbs, adequate protein, and plenty of vegetables.
Reassess in 3 months—your HbA1c, lipids, and how you feel should guide whether to continue, adjust, or combine both approaches.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting, stopping, or adjusting any medication. Individual risk profiles and treatment decisions must be individualised.
Related Article
How Many Carbs Should Diabetics Eat? 2026 Evidence-Based Guidelines for Better Blood Sugar
Can You Reverse Type 2 Diabetes with Diet? Science-Based Guide 2026
Your Cholesterol Isn’t the Whole Story: The Hormone Imbalances Driving Heart Disease
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
References
Currenti, W., Losavio, F., Quiete, S., Alanazi, A. M., Messina, G., Polito, R., Ciolli, F., Zappalà, R. S., Galvano, F., & Cincione, R. I. (2023). Comparative evaluation of a low-carbohydrate diet and a Mediterranean diet in overweight/obese patients with type 2 diabetes mellitus: A 16-week intervention study. Nutrients, 16(1), Article 95. https://doi.org/10.3390/nu16010095
Gorodeski Baskin, R., & Karp, K. A. (2025). Navigating the spectrum of 4 evidence-based nutrition options for type 2 diabetes management. The Journal of Clinical Endocrinology & Metabolism, 110(Supplement 2), S112–S117. https://doi.org/10.1210/clinem/dgae646
Lauria, F., Formisano, A., Dello Russo, M., Quaglia, C., Giacco, R., Russo, G. L., Spagnuolo, C., & Vitale, M. (2026). Mediterranean diet, gut microbiota, and type 2 diabetes: A systematic review and meta-analysis of intervention trials. Nutrition, Metabolism and Cardiovascular Diseases, 36(5), Article 104433. https://doi.org/10.1016/j.numecd.2025.104433
Zheng, X., Zhang, W., Wan, X., et al. (2024). The effects of Mediterranean diet on cardiovascular risk factors, glycemic control and weight loss in patients with type 2 diabetes: A meta-analysis. BMC Nutrition, 10, Article 59. https://doi.org/10.1186/s40795-024-00836-y