Obesity Is a Disease: How GLP-1 Medications Are Changing Treatment Forever
Discover how GLP-1 drugs like semaglutide and tirzepatide are transforming obesity treatment in 2026. Learn benefits, risks, side effects, and who qualifies
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/14/202612 min read
"The landscape of obesity treatment has fundamentally changed. Weight-loss medications are no longer a last resort — they are a cornerstone of modern, evidence-based care."
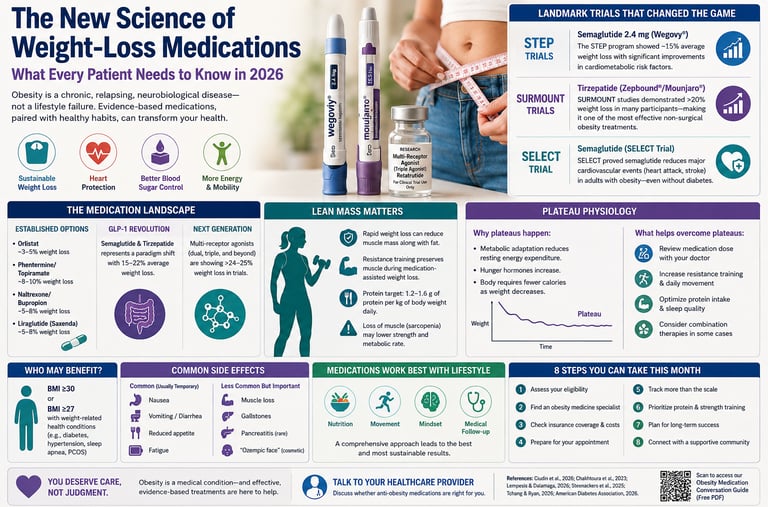
For decades, obesity was framed as a simple failure of willpower — a problem supposedly solved by eating less and exercising more. But modern medical science tells a very different story. In 2026, obesity is now recognised as a complex, chronic, relapsing metabolic disease driven by powerful interactions between the brain, hormones, genetics, gut biology, and the environment (Ciudin et al., 2026). This shift in understanding is transforming treatment strategies around the world.
One of the most important breakthroughs has been the emergence of highly effective anti-obesity medications, particularly GLP-1 receptor agonists such as semaglutide and dual GIP/GLP-1 agonists such as tirzepatide. These therapies do far more than suppress appetite. They target the biological systems that regulate hunger, satiety, insulin sensitivity, and energy balance — helping patients achieve weight loss levels once thought possible only through bariatric surgery (Chakhtoura et al., 2023; American Diabetes Association Professional Practice Committee for Obesity, 2026).
Clinical trials have shown that some patients lose 15–22% of their body weight with these newer medications, alongside major improvements in blood pressure, blood sugar control, fatty liver disease, sleep apnoea, and cardiovascular risk (Ciudin et al., 2026). Landmark studies such as SELECT further demonstrated that semaglutide reduced heart attack and stroke risk in adults with obesity, even in those without diabetes — reinforcing that obesity treatment is about far more than appearance alone.
At the same time, experts caution that obesity medications are not “magic injections.” Long-term success still depends on comprehensive care that includes nutrition, resistance training, sleep optimisation, behavioural support, and ongoing medical follow-up. As next-generation therapies continue to evolve, medicine is entering a new era — one where obesity is finally treated with the same scientific seriousness as other chronic diseases (Tchang & Ryan, 2026).
What Is Obesity? Reframing the Conversation
Before diving into medications, it is worth understanding how medical science now defines obesity. The European Association for the Study of Obesity (EASO) — one of the world's leading bodies on this condition — released its updated pharmacological treatment framework in 2026, reinforcing that obesity is a chronic, relapsing, neurobiological disease, not a lifestyle failure (Ciudin et al., 2026).
This is a critical distinction. Obesity involves complex interactions among genetics, hormones, the brain's reward system, gut microbiome, and social environment. Body fat, especially around the abdomen, drives inflammation and increases the risk of more than 200 health complications — including type 2 diabetes, heart disease, sleep apnoea, certain cancers, and joint disorders.
Recognising obesity as a disease means that medical treatment — including pharmacotherapy — is not a "shortcut." It is appropriate, evidence-based care.
STEP Trials (Semaglutide)
The STEP clinical trial programme showed that semaglutide 2.4 mg produced average weight loss of approximately 15% alongside improvements in blood pressure, waist circumference, and cardiometabolic risk factors.
SURMOUNT Trials (Tirzepatide)
The SURMOUNT studies demonstrated that tirzepatide achieved weight reductions exceeding 20% in many participants, establishing dual GIP/GLP-1 agonism as one of the most effective non-surgical obesity treatments available.
SELECT Trial (Cardiovascular Outcomes)
The SELECT trial was a landmark breakthrough because semaglutide reduced major cardiovascular events — including heart attack and stroke — in adults with obesity even without diabetes, confirming that obesity treatment improves more than body weight alone.
The Current Medication Landscape: What's Available Now
First-Line and Established Options
A comprehensive 2023 review published in eClinicalMedicine mapped the full spectrum of available obesity pharmacotherapies (Chakhtoura et al., 2023). At that time, approved options included:
Orlistat — blocks fat absorption in the gut; modest weight loss (~3–5%)
Phentermine/topiramate (Qsymia) — appetite suppression; ~8–10% weight loss
Naltrexone/bupropion (Contrave) — targets food cravings and reward pathways
Liraglutide (Saxenda) — a daily GLP-1 receptor agonist; ~5–8% weight loss
These medications remain relevant and available, particularly for patients who cannot access or tolerate newer agents.
The GLP-1 Revolution: Semaglutide and Tirzepatide
The most significant development in recent years has been the approval of semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) — weekly injectable medications that mimic gut hormones to powerfully reduce hunger and improve metabolic function.
The EASO 2026 framework notes that these agents represent a paradigm shift, with weight reductions of 15–22% observed in clinical trials — numbers previously associated only with surgery (Ciudin et al., 2026). The American Diabetes Association's updated Standards of Care for Overweight and Obesity (2026) similarly positions GLP-1 receptor agonists and dual GIP/GLP-1 agonists (like tirzepatide) as first-line pharmacological options for eligible adults — a major update from previous years (American Diabetes Association Professional Practice Committee for Obesity, 2026).
The Next Frontier: Multi-Receptor Agonists and Metabolic Modulators
Just as patients and doctors were getting used to GLP-1 medications, a new generation of drugs is already in late-stage clinical trials or early approval. Lempesis and Dalamaga (2026), writing in Metabolism Open, describe this as the era of multi-receptor agonists — drugs that simultaneously target multiple hormonal pathways to produce even greater metabolic effects.
What Are Multi-Receptor Agonists?
Traditional GLP-1 medications target one receptor. The new agents aim at two, three, or even more:
Dual agonists (GLP-1 + GIP): Tirzepatide is already approved here. It outperformed semaglutide in head-to-head trials.
Triple agonists (GLP-1 + GIP + glucagon): Retatrutide is the leading candidate. Early data shows weight loss exceeding 24% in some patient groups.
Amylin analogues and combinations: Cagrilintide combined with semaglutide (CagriSema) has shown remarkable results in clinical trials, with some participants losing >25% of body weight.
Oral formulations: Oral semaglutide (Rybelsus) is approved for diabetes; oral versions of newer agents are under investigation for obesity.
Lempesis and Dalamaga (2026) also note important controversies surrounding these agents — including long-term cardiovascular safety beyond existing trial periods, effects on lean muscle mass (muscle loss alongside fat loss), and questions about bone density. These are actively researched areas, and patients should discuss them openly with their physicians.
Why Are Patients Still Not Getting Treatment? A Humbling Reality Check
Despite these breakthroughs, a pointed expert guidance statement from TOS, OMA, and OAC — published in Obesity in 2026 — delivers a sobering message: most people with obesity who could benefit from pharmacotherapy are still not receiving it (Tchang & Ryan, 2026).
The authors describe this as a "humbling call to action," citing:
Persistent prescriber hesitancy rooted in outdated beliefs about patient willpower
Insurance and cost barriers — many insurance plans still do not cover AOMs
Pharmacy shortages — semaglutide and tirzepatide shortages have been an ongoing challenge
Weight stigma — both within healthcare settings and internalised by patients who delay seeking help
If you have been diagnosed with obesity (BMI ≥30, or ≥27 with weight-related health conditions) and have not been offered a discussion about medication, it may be time to proactively bring it up with your doctor. This is your right as a patient. Importantly, South Asian populations often develop visceral adiposity, insulin resistance, and type 2 diabetes at lower BMI levels than Western populations, highlighting the limitations of BMI alone.
Personalising Treatment: The Era of Tailored Pharmacotherapy
One of the most exciting developments is the growing shift toward precision medicine in obesity care. A 2025 review in Frontiers in Endocrinology by Steenackers et al. asks a forward-thinking question: are we ready to select, tailor, and combine anti-obesity pharmacotherapies to achieve more ambitious goals?
The answer, increasingly, is yes — with caveats.
How Is Treatment Personalised?
Doctors are now considering multiple factors when selecting medications:
Biological factors:
Presence of type 2 diabetes (favours GLP-1/GIP agents)
Cardiovascular disease history (semaglutide has proven CV benefits)
Kidney function (affects drug choice and dosing)
Hormonal conditions (e.g., hypothyroidism, PCOS)
Behavioural and psychological factors:
Presence of binge eating disorder
History of depression or anxiety (naltrexone/bupropion may be preferred or avoided)
Food addiction patterns
Practical factors:
Preference for oral vs. injectable medication
Insurance coverage
Tolerance of side effects (nausea is common with GLP-1 agents, especially early on)
Steenackers et al. (2025) also raise the emerging concept of combination pharmacotherapy — using two different medications simultaneously to target multiple pathways, similar to how hypertension or HIV is managed. While still largely investigational, early data are promising.
Obesity Medications and Diabetes: A Special Relationship
For the millions of people living with both obesity and type 2 diabetes, the convergence of treatments is particularly relevant. The American Diabetes Association's Standards of Care in Overweight and Obesity (2026) integrates obesity management directly into diabetes care in a way that marks a significant cultural and clinical shift.
Key recommendations include:
GLP-1 receptor agonists and dual GIP/GLP-1 agonists are now recommended regardless of baseline HbA1c for adults with obesity and established cardiovascular disease or high cardiovascular risk
Weight management goals in people with diabetes should now target ≥10% body weight loss where possible — not just glycaemic control alone
Medication selection should account for both metabolic and cardiorenal benefits
This integrated approach means that if you have diabetes and obesity, your treatment plan can — and should — address both simultaneously.
Managing Side Effects: What Patients Experience
GLP-1-based medications are generally well tolerated, but side effects are real and should be managed proactively.
Common (usually temporary):
Nausea, especially in the first 4–8 weeks
Vomiting or diarrhoea during dose escalation
Reduced appetite (often desired, but can become excessive)
Fatigue
Less common but important:
Muscle loss (sarcopenia) — especially with rapid weight loss; resistance exercise and adequate protein intake are critical
Gallstones — weight loss in general increases gallstone risk
Pancreatitis — rare; discuss personal risk with your doctor
"Ozempic face" — loss of facial fat; largely cosmetic
What helps: Starting at a low dose and escalating slowly, eating smaller meals, avoiding high-fat foods initially, and staying hydrated. Most patients find that nausea significantly improves after the first month.
The Role of Lifestyle: Medications Work Best Alongside Behaviour Change
It is important to be clear: anti-obesity medications are not a substitute for healthy habits — they are a powerful tool that makes those habits more achievable.
The EASO framework (Ciudin et al., 2026) consistently emphasises that pharmacotherapy should be delivered within a comprehensive obesity management program, including:
Medical nutrition therapy (eating patterns tailored to you, not generic diets)
Physical activity guidance appropriate to your fitness level
Psychological support, including cognitive behavioural strategies
Regular medical follow-up and monitoring
Think of medications as levelling the playing field — reducing the biological drive to overeat so that your efforts at lifestyle change can actually succeed and stick.
Practical Applications: 8 Steps You Can Take This Month
Assess your eligibility. If your BMI is ≥30 (or ≥27 with a weight-related health condition such as high blood pressure, pre-diabetes, or sleep apnoea), you may be a candidate for pharmacotherapy. Use a BMI calculator as a starting point, but know that BMI has limitations.
Find an obesity medicine specialist. Your primary care physician is a great starting point, but obesity medicine specialists have dedicated training in this area. Search for board-certified obesity medicine physicians through the Obesity Medicine Association (OMA).
Check your insurance coverage. Costs vary enormously. Some plans cover AOMs; others do not. Manufacturer assistance programmes exist for eligible patients. Ask your pharmacy or benefits manager.
Prepare for your appointment. Write down your weight history, previous diet attempts, current medications, and any weight-related health conditions. Bring questions.
Track your progress beyond the scale. Blood pressure, blood sugar, energy levels, sleep quality, and mobility are all meaningful markers of improvement — even before significant weight loss occurs.
Prioritise protein and resistance training. If you start a GLP-1 medication, aim for 1.2–1.6g of protein per kilogram of body weight daily and include 2–3 strength training sessions per week to preserve muscle mass.
Plan for the long term. Obesity is a chronic condition. Most patients who stop medication regain weight. Discuss a long-term maintenance plan with your doctor from the outset.
Connect with a community. Peer support significantly improves outcomes. Groups like the Obesity Action Coalition (OAC) offer free resources, advocacy tools, and community forums.
Frequently Asked Questions (FAQs)
1. Are weight-loss medications safe for long-term use? The newer GLP-1 agents (semaglutide, tirzepatide) have now been studied for up to 4–5 years in large clinical trials and show a favourable long-term safety profile. Cardiovascular outcomes trials (like SURMOUNT and SELECT) have actually demonstrated reductions in heart attack and stroke risk. That said, "long-term" data beyond 5 years is still accumulating, and your doctor will monitor you regularly.
2. Will I regain weight when I stop the medication? This is one of the most common and valid concerns. The evidence shows that most people do regain a significant portion of weight after stopping GLP-1 medications — because obesity is a chronic, biological condition that medication helps manage rather than cure. This is why current guidelines recommend treating obesity like other chronic diseases: with ongoing, sustained therapy.
3. Can I take these medications if I have heart disease? In many cases, yes — and they may be especially beneficial. Semaglutide received approval specifically for reducing cardiovascular risk in people with obesity and established heart disease. Always disclose your full medical history to your physician.
4. What is the difference between Ozempic and Wegovy? Both contain semaglutide, but at different approved doses. Ozempic (up to 2 mg) is FDA-approved for type 2 diabetes. Wegovy (up to 2.4 mg weekly) is approved specifically for chronic weight management. The higher dose in Wegovy produces greater weight loss. They are not interchangeable without physician guidance.
5. Are these medications suitable for teenagers? Wegovy (semaglutide) is FDA-approved for adolescents aged 12 and older with obesity. Tirzepatide approvals for adolescents are pending. Paediatric obesity is a serious medical concern, and early intervention with appropriate treatments can prevent lifelong complications. Decisions should always involve a paediatrician or adolescent medicine specialist.
6. I've heard about "Ozempic face" — is that real and dangerous? "Ozempic face" refers to facial volume loss that can occur with rapid weight loss on GLP-1 medications. It is a cosmetic concern, not a medical danger, and largely reflects the normal redistribution of body fat during significant weight loss. Slower, gradual weight loss and adequate nutrition can minimise this effect.
7. What if I can't afford these medications? Cost is a genuine barrier. Options to explore include: manufacturer patient assistance programmes (Novo Nordisk and Eli Lilly both offer these), GoodRx and similar discount programmes for some formulations, compounded versions (though quality control varies — discuss with your doctor), and advocacy through your insurance provider. The Obesity Action Coalition also provides advocacy resources to help patients fight insurance denials.
A Note on Weight Stigma and Self-Compassion
Embedded throughout the latest scientific literature is an urgent call to address weight stigma. Tchang and Ryan (2026) explicitly call on healthcare providers to confront their own biases and treat obesity with the same compassion offered to any other chronic disease.
If you have ever felt judged, dismissed, or lectured at a medical appointment, that experience is unfortunately common — and it is not your fault. You deserve evidence-based care delivered with dignity. If your current provider is not providing that, you are entitled to seek a second opinion.
Obesity is not a character flaw. It is a complex biological condition — and in 2026, there are more effective, evidence-based tools than ever before to help you manage it.
Important Considerations
Lean Mass Preservation Matters
Rapid weight loss can reduce not only fat mass but also skeletal muscle mass, which may lower strength, metabolic rate, and long-term functional health.
Why Resistance Training Is Essential
Resistance exercise acts as a biological signal that helps preserve muscle tissue during caloric restriction and GLP-1–mediated weight loss.
Protein Targets
Many obesity specialists now recommend approximately 1.2–1.6 g/kg/day of protein intake during pharmacotherapy to support muscle maintenance and recovery.
Emerging Clinical Concern
Researchers are increasingly studying “sarcopenic weight loss,” where excessive lean tissue loss may occur despite successful fat reduction.
Why Weight Loss Slows
Weight-loss plateaus are biologically normal and occur because the body adapts to lower energy intake by reducing resting metabolic rate and increasing hunger-related hormonal signals.
Metabolic Adaptation
As body weight decreases, the body requires fewer calories for maintenance, meaning early rapid progress often slows over time.
Common Contributors
Reduced physical activity, inadequate protein intake, poor sleep, medication adherence issues, and loss of muscle mass can all contribute to plateaus.
How Clinicians Respond
Strategies may include dose adjustment, resistance training progression, higher protein intake, behavioural coaching, or combination pharmacotherapy in selected patients.
Author’s Note: A Clinician’s Perspective
As a physician working in internal medicine and metabolic health, I have seen firsthand how deeply obesity affects nearly every organ system in the body — from diabetes and cardiovascular disease to fatty liver disease, sleep disorders, joint degeneration, and declining quality of life. Yet for many years, patients were often given overly simplistic advice that failed to reflect the biological complexity of obesity itself.
What makes the current era of obesity medicine so important is that science is finally catching up with patient reality. We now understand that obesity is not merely a problem of motivation or personal discipline. It is a chronic neurohormonal and metabolic disease influenced by genetics, appetite regulation, insulin resistance, inflammation, gut signaling, sleep, stress, medications, and environmental factors.
The emergence of GLP-1 receptor agonists, dual incretin therapies, and next-generation metabolic medications represents one of the most significant advances in preventive medicine and cardiometabolic care in decades. In clinical practice, these therapies are not simply helping patients lose weight — they are improving blood sugar control, reducing cardiovascular risk, enhancing mobility, restoring confidence, and in many cases, helping patients regain a sense of control over their health.
At the same time, medications are not a replacement for comprehensive care. Long-term success still depends on preserving muscle mass, improving nutrition quality, increasing physical activity, optimising sleep, and addressing the psychological burden that often accompanies obesity.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Weight Loss vs Fat Loss: The Critical Difference Every GLP-1 User Must Understand
Visceral Fat Treatment: GLP-1, Semaglutide and SGLT2 Explained
GLP-1 Muscle Loss: You’re Losing Weight But Are You Losing Strength Too?
Why Your Body Resists Weight Loss: Understanding the Science of Weight Regain | DR T S DIDWAL
Obesity 2025: Revolutionary Research Advances in Treatment and Management | DR T S DIDWAL
References
American Diabetes Association Professional Practice Committee for Obesity. (2026). Pharmacologic treatment of obesity in adults: Standards of care in overweight and obesity. Diabetes, Obesity, and CardioMetabolic CARE, 1(1), 5–36. https://doi.org/10.2337/doci25-0008
Chakhtoura, M., Haber, R., Ghezzawi, M., Rhayem, C., & El Masri, D. (2023). Pharmacotherapy of obesity: An update on the available medications and drugs under investigation. eClinicalMedicine, 58, Article 101882. https://doi.org/10.1016/j.eclinm.2023.101882
Ciudin, A., Baker, J. L., Belančić, A., et al. (2026). Framework for the pharmacological treatment of obesity and its complications from the European Association for the Study of Obesity (EASO): 2026 update. Nature Medicine. https://doi.org/10.1038/s41591-026-04397-4
Lempesis, I. G., & Dalamaga, M. (2026). Obesity pharmacotherapy reimagined: The era of multi-receptor agonists and next-generation metabolic modulators, perspectives and controversies. Metabolism Open, 30, Article 100463. https://doi.org/10.1016/j.metop.2026.100463
Steenackers, N., Toumassian, J., Deleus, E., Mertens, A., Lannoo, M., Pazmino, S., van Laar, A. D. E., Van der Schueren, B., & Vangoitsenhoven, R. (2025). Pharmacotherapy for obesity: Are we ready to select, tailor and combine pharmacotherapy to achieve more ambitious goals? Frontiers in Endocrinology, 16, Article 1569468. https://doi.org/10.3389/fendo.2025.1569468
Tchang, B. G., & Ryan, D. H. (2026). TOS/OMA/OAC expert guidance statement on obesity pharmacotherapy: A humbling call to action. Obesity, 34(4), 765–769. https://doi.org/10.1002/oby.70170