Beyond the Low-Fat Myth: 6 New Studies Redefining Dietary Fat and Heart Health
Is fat really bad for your heart? Explore 6 breakthrough studies redefining dietary fat, LDL cholesterol, and cardiovascular risk.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/11/20268 min read
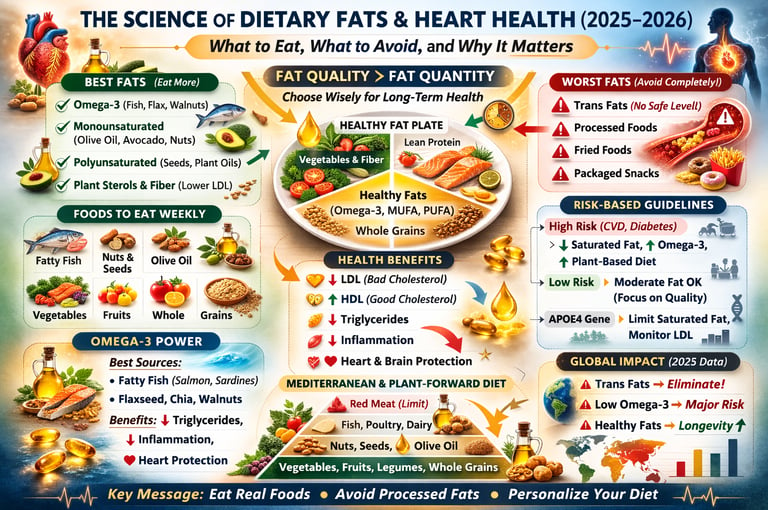
For decades, dietary fat was cast as the villain in the battle against heart disease. Public health campaigns urged us to slash fat intake, leading to a surge in low-fat products that often replaced fats with refined sugars and starches. Yet as we stand in 2026, a wave of sophisticated research is rewriting the narrative. The question is no longer whether fat is “bad,” but which fats, in what contexts, and for whom truly matter for cardiovascular health.
Modern lipid science has moved beyond simplistic “eat less fat” advice. It now emphasizes fat quality, overall dietary patterns, individual risk profiles, and genetic factors. Six landmark studies from 2025–2026 illuminate how strategic choices around dietary fats can meaningfully lower cardiovascular risk while supporting broader metabolic health.
Clinical Pearls: Practical Takeaways for Everyday Heart Health
1. Master the Substitution Rule
Reducing saturated fat only improves outcomes when replaced with polyunsaturated fats (PUFAs), monounsaturated fats (MUFAs), or high-quality carbohydrates. Swapping butter for olive oil or nuts helps; replacing it with sugary snacks or white bread often raises triglycerides and worsens insulin resistance. Always ask: “What am I replacing this with?”
2. Risk-Stratified Approach to Saturated Fat
The benefits of strict saturated fat reduction are most pronounced in individuals with existing heart disease or high cardiovascular risk. For healthy, low-risk people, moderate intake from whole-food sources (like full-fat dairy or unprocessed meat) within a nutrient-rich diet appears far less concerning. One-size-fits-all restrictions are outdated.
3. Address the Omega-3 “Silent Deficiency”
Inadequate intake of EPA and DHA omega-3s ranks as a major global contributor to coronary heart disease. These fats offer anti-inflammatory, triglyceride-lowering, and membrane-stabilizing benefits. Prioritize fatty fish, or consider high-quality supplements if your intake is low—especially if you have elevated triglycerides or high risk.
4. Focus on the Food Matrix, Not Isolated Nutrients
The overall dietary pattern trumps single-nutrient counting. Vegetables, nuts, legumes, olive oil, and fish create synergistic effects through fiber, polyphenols, and healthy fats that modulate lipid absorption and inflammation. Whole-food Mediterranean or plant-forward patterns consistently link to lower mortality, even in people with dyslipidemia.
5. Personalize Based on Genetics
Variants like APOE4 can cause stronger LDL responses to saturated fat. Two people eating the same meal may have dramatically different cholesterol results. As genetic and metabolic testing improve, truly individualized fat recommendations are becoming a practical reality rather than a distant ideal.
6. Zero Tolerance for Industrial Trans Fats
There is no safe threshold for artificial trans fats. They raise LDL, lower HDL, and promote inflammation. Eliminate any product listing “partially hydrogenated oils.” This remains the clearest, most unanimous recommendation in lipid science.
Understanding Lipids: Essential Players in Health
Lipids—including triglycerides, cholesterol, and phospholipids—are vital for life. They form cell membranes, enable hormone production, facilitate vitamin absorption, and regulate inflammation. The issue has never been fat itself, but the types and contexts in which we consume it.
Saturated fatty acids (SFAs), monounsaturated (MUFAs), polyunsaturated (PUFAs, including omega-3s and omega-6s), and trans fats each interact differently with our biology. Quality, food source, and overall diet determine whether fats support or harm cardiovascular health.
Study 1: Risk-Stratified Evidence on Saturated Fat (Steen et al., 2026)
A major systematic review published in Annals of Internal Medicine analyzed 17 randomized controlled trials involving over 66,000 participants. It examined the effects of reducing or modifying saturated fat intake on cholesterol, mortality, and cardiovascular events.
The standout finding: Benefits are strongly risk-dependent. In high-risk individuals (those with established cardiovascular disease or multiple risk factors), lowering saturated fat—particularly when replaced with PUFAs—produced meaningful reductions in all-cause mortality, cardiovascular mortality, nonfatal heart attacks, and strokes over five years.
For low-risk, generally healthy people, the absolute benefits were minimal or below clinically important thresholds. Replacing saturated fat with refined carbohydrates showed little to no advantage and sometimes worsened metabolic markers.
This research supports moving away from blanket population-wide fat restrictions toward personalized, risk-stratified guidance.
Study 2: Personalized Nutrition and Genetic Variability (Lovegrove, 2025)
Traditional guidelines rely on average population responses, but inter-individual variation is enormous. Genetics (especially APOE variants), gut microbiome, age, sex, and metabolic health all influence how dietary fats affect lipid profiles.
People with APOE4 alleles, for example, often show exaggerated LDL increases in response to saturated fat. This review advocates a dual approach: sensible public health guidance to reduce industrial trans fats and excess saturated fat in processed foods, combined with emerging tools for precision nutrition.
Study 3: Dietary Patterns and Mortality in Dyslipidemia (Yin et al., 2025)
In a large prospective cohort from China, researchers tracked dietary patterns in people with dyslipidemia (abnormal blood lipids). Plant-forward patterns rich in vegetables, whole grains, legumes, nuts, and fish were associated with significantly lower all-cause mortality compared to patterns high in refined carbs, processed meats, and fried foods.
This reinforces a crucial principle: In real-world eating, the whole diet matters more than obsessing over individual grams of fat. Synergistic effects of fiber, antioxidants, and healthy fats in minimally processed foods drive superior outcomes.
Study 4: Global Burden of Dietary Fat Risks (Ma et al., 2025 )
Comprehensive analyses of meta-analyses and Global Burden of Disease data highlight regional differences. While excess saturated and trans fats remain problematic in high-income countries, inadequate omega-3 intake represents a widespread, under-addressed risk factor globally, contributing to hundreds of thousands of ischemic heart disease deaths annually.
Industrial trans fats have no safe threshold and should be eliminated. Increasing access to nuts, seeds, fish, and quality plant oils offers high public health returns, especially in lower-resource settings.
Study 5: Updated AACE Guidelines for Dyslipidemia Management (Patel et al., 2025)
The 2025 American Association of Clinical Endocrinology consensus strongly endorses Mediterranean-style and plant-forward diets as first-line interventions. These patterns improve LDL, triglycerides, HDL, and inflammatory markers.
The guidelines emphasize cardiovascular risk stratification over treating isolated numbers. They support replacing saturated fats with unsaturated fats, increasing soluble fiber, and minimizing ultra-processed foods. Omega-3 supplementation (particularly high-dose EPA) earns a role for certain high-risk patients with elevated triglycerides.
Study 6: Lipids in Clinical Nutrition – Mechanisms and Recommendations (Frydrych et al., 2025)
This narrative review underscores that lipids are biologically indispensable. Their effects depend heavily on the type and food matrix. It provides a foundational scientific case against outdated low-fat dogma and for nuanced, food-based guidance.
Practical Dietary Fat Recommendations: What Should You Actually Eat?
End the Low-Fat Obsession
Total fat intake matters less than quality. Focus on intelligent substitutions rather than drastic cuts.
Prioritize These Fats
Extra-virgin olive oil (rich in MUFAs and polyphenols)
Avocados, nuts, and seeds
Fatty fish (salmon, mackerel, sardines) for omega-3s
Moderate full-fat dairy or fermented foods in the context of a high-quality diet
Minimize These
Industrial trans fats (complete elimination)
Excessive saturated fat from ultra-processed sources
Fried foods and commercially baked goods
Build a Heart-Protective Plate
Fill half with non-starchy vegetables, add legumes and whole grains, include high-quality protein, and finish with healthy fats. This Mediterranean-pattern approach consistently outperforms restrictive low-fat regimens in trials.
Lifestyle Synergy
Combine smart fat choices with regular physical activity (as covered in related articles on exercise and mitochondrial health), good sleep, stress management, and—not smoking—for multiplicative benefits.
Timeline of Changes
Weeks 1–4: Improved triglycerides and energy from better omega-3 status and reduced refined carbs.
Months 1–3: Noticeable shifts in lipid panels and inflammatory markers with consistent dietary pattern changes.
Long-term (6+ months): Reduced cardiovascular risk and better overall metabolic resilience.
Frequently Asked Questions
Q: Is saturated fat really bad for you?
A: It depends on context, source, and your personal risk. In high-risk individuals, reducing it (especially replacing with PUFAs) offers clear benefits. For low-risk people eating mostly whole foods, moderate amounts are unlikely to be harmful. Focus on the overall pattern rather than demonizing any single food.
Q: What are the best fats for heart health?
A: Unsaturated fats—particularly MUFAs from olive oil, avocados, and nuts, and omega-3 PUFAs from fish and certain seeds—have the strongest evidence for improving lipid profiles and reducing inflammation.
Q: Should I avoid all fat if I have high cholesterol?
A: No. Emphasizing high-quality fats within a Mediterranean or plant-forward pattern is usually more effective than fat avoidance. Work with your doctor using current risk-stratified guidelines.
Q: Are omega-3 supplements worth it?
A: For people who don’t eat fatty fish regularly or have high triglycerides/cardiovascular risk, yes—evidence supports benefits, especially prescription-strength options. Discuss testing and dosing with your physician.
Q: How much do genetics really matter?
A: Significantly for some people. APOE4 carriers, for instance, may need tighter saturated fat control. Genetic insights are becoming valuable tools for personalization.
Q: Is the Mediterranean diet still the gold standard?
A: Yes—strong evidence from guidelines and cohorts supports it. Flexible plant-forward variations work well too, depending on cultural preferences and sustainability.
Q: Which fats should I eliminate?
A: Artificial trans fats. They offer no benefit and clear harm. Minimize heavily processed sources of saturated fat as well.
The Bottom Line: A Nuanced, Evidence-Based Future
The low-fat era was well-intentioned but oversimplified. Today’s science calls for precision: prioritize fat quality, whole-food dietary patterns, risk stratification, and personalization. Strategic inclusion of anti-inflammatory unsaturated fats—especially omega-3s—while minimizing industrial junk fats offers one of the most powerful levers we have for lifelong heart health.
Your heart doesn’t need fear-based restriction. It needs intelligent, consistent nourishment within a rich, varied, whole-food diet. Start with small, sustainable swaps—drizzle olive oil instead of butter, add a handful of walnuts, choose salmon twice a week—and build from there. Science has evolved. Our plates should too.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Can a Low-Carb Diet Improve Cholesterol and Diabetes? What the Latest Research Really Shows
Can Plant-Based Polyphenols Lower Biological Age? | DR T S DIDWAL
Time-Restricted Eating: Metabolic Advantage or Just Fewer Calories? | DR T S DIDWAL
Can You Revitalize Your Immune System? 7 Science-Backed Longevity Strategies | DR T S DIDWAL
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
References
Frydrych, A., Kulita, K., Jurowski, K., & Piekoszewski, W. (2025). Lipids in clinical nutrition and health: Narrative review and dietary recommendations. Foods (Basel, Switzerland), 14(3), 473. https://doi.org/10.3390/foods14030473
Lovegrove, J. A. (2025). Dietary fats and cardiometabolic health—from public health to personalised nutrition: 'one for all' and 'all for one'. Nutrition Bulletin, 50(1), 132–141. https://doi.org/10.1111/nbu.12722
Ma, J., Hu, D., Li, D., Chen, Y., Chen, Q., Fan, Z., Wang, G., Xu, W., Zhu, G., Xin, Z., Cao, W., Zhang, Z., Wu, J., Ding, J., Yin, L., Chang, Y., & Ren, S. (2025). The impact of dietary fat and fatty acid consumption on human health: A comprehensive review of meta-analyses and the Global Burden of Disease Study 2021. Trends in Food Science & Technology, 160, 105002. ,https://doi.org/10.1016/j.tifs.2025.105002
Patel, S. B., Belalcazar, L. M., Afreen, S., Balderas, R., Hegele, R. A., Karpe, F., Ponte-Negretti, C. I., & Rajpal, A. (2025). American Association of Clinical Endocrinology consensus statement: Algorithm for management of adults with dyslipidemia — 2025 update. Endocrine Practice: Official Journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists, 31(10), 1207–1238. https://doi.org/10.1016/j.eprac.2025.07.014
Steen, J. P., Klatt, K. C., Chang, Y., Guyatt, G. H., Zhu, H., Swierz, M. J., Storman, D., Sun, M., Zhao, Y., Ge, L., Thabane, L., Ghosh, N. R., Karam, G., Alonso-Coello, P., Bala, M. M., & Johnston, B. C. (2026). Effect of interventions aimed at reducing or modifying saturated fat intake on cholesterol, mortality, and major cardiovascular events: A risk stratified systematic review of randomized trials. Annals of Internal Medicine, 179(2), 242–255. https://doi.org/10.7326/ANNALS-25-02229
Yin, L., Yu, L., Wang, Y., et al. (2025). Dietary patterns and risk of all-cause mortality in individuals with dyslipidemia based on a prospective cohort in Guizhou China. Scientific Reports, 15, 7395. https://doi.org/10.1038/s41598-025-88101-5