Weight Cycling (Yo-Yo Dieting): Does Repeated Weight Loss and Regain Really Harm Your Health?
Does yo-yo dieting permanently damage your metabolism? Discover what the latest 2026 research says about weight cycling, muscle loss, inflammation, GLP-1 medications, and long-term health.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/12/202620 min read
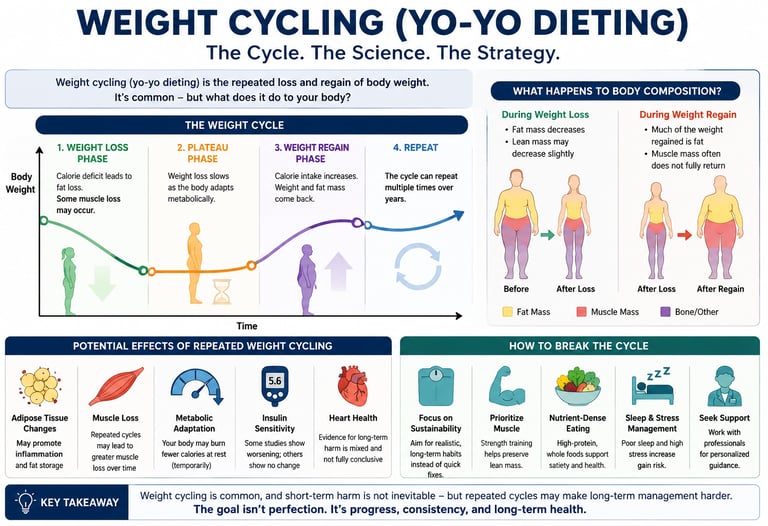
Weight cycling (yo-yo dieting) is the repeated loss and regain of body weight. Current evidence suggests it does not permanently damage metabolism or independently increase disease risk in most people. However, older adults, individuals with low muscle mass, and those discontinuing GLP-1 medications may face greater risks of muscle loss and rapid weight regain, making resistance training and long-term lifestyle support essential.
Key takeaways
1. The "Broken Metabolism" Myth is Largely Debunked
The landmark Lancet Diabetes & Endocrinology review found no convincing clinical evidence that yo-yo dieting permanently damages your resting metabolic rate (Magkos & Stefan, 2026). While your metabolism naturally slows down during active weight loss to conserve energy, it largely bounces back once your weight stabilizes or is regained. Having a history of multiple diet cycles does not mean your metabolism is fundamentally broken.
2. The Danger Lies in the Base, Not the Cycle
Older studies frequently blamed weight cycling for increased risks of type 2 diabetes and cardiovascular disease. However, the 2026 data shows that when researchers properly account for age, baseline health, and how long a person has lived with obesity, the act of weight cycling itself isn't the driver of disease (Magkos & Stefan, 2026). The underlying health risks are tied to the weight itself, not the fluctuations.
3. Your Age and Baseline Muscle Mass Matter Immensely
While population averages show that weight cycling doesn't automatically ruin body composition, individual risks vary. 2025 research emphasizes that older adults and individuals with low initial muscle mass are highly vulnerable to sarcopenic obesity—high fat mass paired with low muscle mass (Zamboni et al., 2025). For these groups, losing muscle during a diet and regaining only fat can gradually compromise physical strength.
4. GLP-1 Medication Cycling is a Distinct, High-Concern Scenario
Weight cycling caused by stopping incretin mimetic drugs (like semaglutide or tirzepatide) behaves differently than traditional dieting. When these medications are discontinued abruptly, weight regain is rapid, and up to 40% of the weight originally lost can be lean muscle mass Alexander, S.E., & Howden, E.J. (2026). This rapid shift can leave your body composition worse off than your baseline, making structured medical tapering essential.
5. Fat Tissue Has a Subclinical "Inflammatory Memory"
Even if your annual physical and standard blood panels look completely normal after weight cycling, changes may be happening at the cellular level. Molecular research reveals that adipose (fat) tissue can retain an epigenetic and immunologic "memory" of a prior obese state, keeping tissue subtly primed for inflammation and less metabolically flexible (Navarro et al., 2026). This helps explain why rapid weight rebound can happen upon re-exposure to a high-calorie environment.
6. Fear of Yo-Yo Dieting Should Not Deter Weight-Loss Attempts
One of the most critical clinical warnings from researchers is directed at diet culture fearmongering: do not remain at a higher weight purely out of fear of yo-yo dieting (Magkos & Stefan, 2026). Staying at a higher weight carries clear, well-established cardiometabolic risks, whereas attempting intentional, medically sound weight loss still offers profound health benefits—even if you have tried and failed before.
7. Resistance Training and Protein are Non-Negotiable Safeguards
The ultimate physiological armor against the potential downsides of weight cycling is muscle preservation. Across recent reviews, engaging in resistance training 2 to 3 times per week and maintaining optimal protein intake are the most effective ways to protect lean tissue and support long-term metabolic flexibility, especially when navigating drug-driven weight cycles (Alexander & Howden, 2026; Zamboni et al., 2025).
8. Clinical Focus is Shifting from the Scale to Composition
The modern scientific consensus treats weight management less as a battle with the scale and more as a mission to optimize body composition. Instead of just tracking total pounds, experts emphasize that obesity research and clinical practice must actively monitor fat-to-muscle ratios and physical strength to prevent long-term functional decline (Hegazi & Halpern, 2025). If you've lost weight and regained it before — maybe more than once — you've probably heard some version of this warning: "Yo-yo dieting wrecks your metabolism and makes you fatter in the long run."
In May 2026, The Lancet Diabetes & Endocrinology published a landmark Personal View by Professors Faidon Magkos (University of Copenhagen) and Norbert Stefan (German Center for Diabetes Research, University Hospital Tübingen, and Helmholtz Munich) that re-examined decades of human and animal research on weight cycling — the repeated loss and regain of body weight, also known as yo-yo dieting. Their conclusion challenges a belief that has shaped obesity treatment guidance for 30 years.
At the same time, a separate and growing body of research — on muscle loss, adipose tissue "inflammatory memory," and rebound weight gain after stopping GLP-1 drugs like semaglutide and tirzepatide — suggests the picture isn't quite as simple as "nothing to worry about."
What Is Weight Cycling?
Weight cycling (also called yo-yo dieting) refers to repeated cycles of intentional weight loss followed by weight regain, typically defined in research as losing and regaining at least 5–10 pounds (or roughly 5% of body weight) more than once.
It's extraordinarily common. Worldwide, roughly half of all adults are actively trying to lose weight at any given time, and the majority of that lost weight is regained within one to five years — often setting the stage for another attempt, and another cycle.
Weight cycling isn't one single phenomenon. Researchers distinguish between several patterns that matter clinically:
Number of cycles — one round of loss/regain versus five or more over a lifetime
Magnitude — losing 5% of body weight versus 20%+
Speed — rapid loss (very low-calorie diets, medication) versus gradual loss
Intentionality — deliberate dieting versus illness-related or medication-related weight loss
Population — people with obesity versus people at a healthy weight who cycle for aesthetic or athletic reasons
This matters because much of the older research lumped all of these together, which is part of why the newest analysis reached different conclusions.
The Old Narrative: Why We Feared Yo-Yo Dieting
The fear of weight cycling isn't irrational — it grew out of real, published research going back to the 1990s. The classic hypothesis proposed three linked mechanisms:
Disproportionate fat regain — that when weight comes back, it returns as more fat and less muscle than the composition of the weight originally lost.
Metabolic adaptation — that with each cycle, resting metabolic rate drops further, making each subsequent weight-loss attempt harder and each regain faster.
Cumulative harm — that repeated cycles progressively worsen insulin resistance, blood pressure, and cardiovascular risk, independent of the obesity itself.
This narrative became so entrenched that it's frequently cited by clinicians, in patient education materials, and across health media as a reason to be cautious about intentional weight loss — sometimes even a reason to avoid dieting altogether.
The problem, according to the 2026 Lancet analysis, is that many of the studies underpinning this narrative didn't adequately separate the effects of weight cycling itself from confounding factors: age, baseline health status, how much time a person had already spent living with obesity, and reverse causation (people with worse metabolic health may be more prone to weight cycling, rather than weight cycling causing the worse health).
The 2026 Lancet Review: What Actually Changed
Magkos and Stefan's Personal View, published online on 14 May 2026, systematically re-examined observational studies, randomized controlled trials, and animal experiments investigating whether weight cycling independently harms body weight regulation, body composition, energy metabolism, and metabolic function.
Their headline conclusion: there is no convincing causal evidence that weight cycling itself leads to long-term clinical harm in people with obesity, once confounding variables are properly accounted for.
As Professor Magkos put it in comments accompanying the publication, many people avoid attempting weight loss because they fear that yo-yo dieting will damage their muscle mass and metabolism — and the review suggests those fears are largely unsupported by rigorous evidence.
Key findings from the review include:
When body composition changes during weight cycling were compared against equivalent first-time weight loss in controlled studies, the proportion of weight lost as fat versus muscle was similar, not meaningfully worse with cycling.
Reductions in resting metabolic rate during weight loss are proportional to the amount of weight lost and largely reverse with regain — there is limited evidence of a cumulative, permanently lowered "metabolic set point" from cycling per se.
Associations between weight cycling and cardiometabolic disease in observational studies were substantially attenuated (weakened) once analyses adjusted for BMI, age, and baseline health status — suggesting that underlying adiposity, not the act of cycling, is driving much of the associated risk.
Clinical importance: This matters enormously for how clinicians counsel patients. If the old narrative were fully correct, a patient who had cycled weight multiple times would need to be warned that further attempts carry compounding physiological risk. The Lancet review instead supports continuing to recommend weight-loss attempts on their clinical merits — you are not necessarily "worse off" metabolically for having tried and regained before.
That said, a Personal View is an expert interpretation of existing evidence, not new primary data — and it does not erase every mechanistic concern raised elsewhere in the literature, several of which we cover next.
Body Composition: Does Weight Cycling Really Cause Disproportionate Muscle Loss?
This is one of the most searched — and most misunderstood — parts of the weight cycling conversation, and it intersects directly with growing concern about sarcopenia (age-related loss of muscle mass and strength) and sarcopenic obesity (low muscle mass combined with high fat mass).
A 2025 review in Reviews in Endocrine & Metabolic Disorders by Zamboni and colleagues specifically examined weight cycling's effects on muscle mass and sarcopenic obesity risk. Their analysis highlights that:
Older adults and people with pre-existing low muscle mass appear to be at higher risk of unfavorable body composition changes with repeated weight cycling than younger, metabolically healthy individuals.
Each weight-loss phase risks muscle loss; if regain phases replace that lost tissue disproportionately with fat, repeated cycles could theoretically compound sarcopenic risk over a lifetime — even if any single cycle looks unremarkable.
Resistance exercise and adequate protein intake during the weight-loss phase are the most consistently effective countermeasures identified across trials.
Clinical interpretation: This is a case where population-level averages (the Lancet review's overall conclusion) can differ from what matters for a specific higher-risk patient. A 30-year-old with normal muscle mass losing 10% of body weight through a supervised program is a very different clinical scenario than a 68-year-old with low baseline muscle mass repeatedly cycling weight without resistance training. The "cycling is not harmful" conclusion applies best to the former; caution is warranted for the latter.
A related 2025 commentary by Hegazi and Halpern in the same journal makes a broader point relevant here: obesity research and clinical practice have historically focused almost entirely on fat mass, while overlooking muscle mass and function — an oversight that becomes especially costly in the context of rapid weight loss and weight cycling.
Metabolic Rate: Does Cycling Slow Your Metabolism Permanently?
The fear that "my metabolism is broken from years of dieting" is one of the most common concerns people raise with clinicians and dietitians. Here's what the evidence actually supports:
Resting metabolic rate does drop during active weight loss — partly explained by reduced body mass, and partly by an additional, disproportionate reduction sometimes called adaptive thermogenesis or "metabolic adaptation."
This adaptation is well-documented (famously demonstrated in reanalyses of the 1944–45 Minnesota Starvation Experiment data), but it largely reverses once weight stabilizes or is regained.
The Lancet review found limited convincing evidence that this adaptation compounds progressively with each additional weight cycle in a way that leaves someone with a permanently slower metabolism than if they'd never dieted at all.
In plain terms: your metabolism adapts during a weight-loss phase and mostly recovers afterward. Having dieted five times in your life does not appear, based on current evidence, to leave you with a fundamentally broken metabolic rate compared to someone who dieted once — though individual variation exists, and the experience of increased hunger and reduced fullness signals after weight loss (which drives regain) is real and well-documented, separate from the metabolic rate question.
The Counter-Evidence: Obesogenic Inflammatory Memory
Here's where the picture gets more nuanced — and where a purely reassuring headline risks oversimplifying real, active areas of concern.
A January 2026 study in Biomolecules by Navarro and colleagues introduced and tested the concept of "obesogenic inflammatory memory" — the idea that fat tissue and the immune system retain a molecular "memory" of a prior obese state, even after weight normalizes.
In their mouse model, animals that underwent two cycles of diet-induced weight gain and loss showed, by 80 weeks of age:
A final body weight and glucose/lipid profile comparable to lean control animals
But impaired metabolic flexibility and a persistently more inflammatory adipose tissue profile than mice that had never been obese
This aligns with a growing line of research (including a widely covered 2024 Nature paper on adipose tissue's epigenetic memory of obesity) showing that fat cells can retain altered gene-expression patterns after weight loss, potentially predisposing formerly obese tissue to faster or more severe rebound weight gain and inflammation on re-exposure to a high-calorie environment.
Related mechanistic work has also implicated:
Lipid-associated macrophages and memory T cells that persist in adipose tissue after weight loss and become more inflammatory upon weight regain
The CD70–CD27 signaling axis, which appears important for forming this kind of immunologic memory — and which, when experimentally blocked in mice, reduced the exaggerated inflammatory response to a subsequent weight-cycling episode
Why this doesn't necessarily contradict the Lancet review: These are largely mechanistic, cellular, and animal-model findings. They demonstrate biologically plausible pathways by which repeated cycling could matter — particularly for inflammation and metabolic flexibility — even in a scenario where final body weight, fasting glucose, and lipids look statistically "normal" on standard clinical bloodwork. The Lancet review's focus was on clinically measurable outcomes in humans; the inflammatory memory research operates at a mechanistic, subclinical level that conventional lab panels may not fully capture yet.
In short: your annual physical might look fine after weight cycling, while your fat tissue may still be running a subtly different, more inflammation-prone program than someone who's never cycled. Whether that translates into measurably worse long-term clinical outcomes in humans is still being actively studied — this is one of the most important open questions in the field heading into 2027.
Weight Cycling and GLP-1 Drugs (Semaglutide, Tirzepatide)
This is arguably the most clinically urgent version of weight cycling in 2026, given how many people are starting and stopping GLP-1/GIP receptor agonist medications.
A 2026 review in Current Opinion in Clinical Nutrition and Metabolic Care by Alexander and Howden focused specifically on this scenario, and the findings are more cautionary than the general weight-cycling literature:
More than half of people prescribed incretin mimetic drugs (IMDs) like semaglutide or tirzepatide discontinue and later restart therapy within two years — creating a drug-driven cycle of loss and regain.
Stopping IMD therapy leads to rapid, near-complete reversal of weight loss and cardiometabolic improvements within about a year, and early discontinuation is linked to increased cardiometabolic risk.
Up to 40% of the weight lost on these medications can be lean (muscle) mass — meaning the regain that follows discontinuation is disproportionately fat, worsening body composition beyond the person's starting point.
This medication-driven cycling "compounds" the effects seen in classic dieting cycles, potentially worsening body composition and metabolic profiles beyond baseline.
Supervised exercise programs, particularly resistance training, both during treatment and after discontinuation, attenuate weight regain and appear to leave a lasting "legacy" benefit on metabolic markers even after the drug is stopped.
Clinical importance: This is the clearest area where the "don't worry about weight cycling" message needs a caveat. Rapid pharmacological weight loss followed by rapid discontinuation-driven regain is a meaningfully different physiological event than gradual, diet-based weight cycling — largely because of the scale of muscle loss involved and the speed of regain. Anyone using or considering stopping a GLP-1 medication should discuss a structured, muscle-preserving maintenance or tapering plan with their prescribing clinician rather than stopping abruptly.
Cardiometabolic Disease Risk: What the Data Actually Shows
Across large observational cohorts, weight cycling has historically been associated with modestly higher rates of:
Type 2 diabetes
Hypertension
Dyslipidemia
All-cause mortality (in some but not all cohorts)
The critical clinical question is whether these associations reflect a causal effect of cycling itself, or whether they largely reflect confounding by indication — i.e., people who weight-cycle tend to have higher baseline BMI, more years lived with obesity, and more pre-existing metabolic dysfunction, all of which independently raise disease risk regardless of whether their weight fluctuated.
The 2026 Lancet review argues strongly for the latter interpretation, noting that associations were substantially weakened after adjusting for these factors. This is consistent with a broader pattern in nutrition epidemiology, where behaviors correlated with poor baseline health (rather than causing it) can appear artificially risky in unadjusted analyses.
However, it's worth being precise about the limits of this reassurance:
Randomized controlled trials of weight cycling in humans (as opposed to observational data) are limited, short, and cannot ethically replicate decades of real-world cycling.
Most trial-based evidence covers one or two cycles over months to a few years — not the 5–10+ cycles some people experience over a lifetime of dieting.
Animal studies, which can control for these variables more precisely, show more consistent — though not universal — evidence of adverse effects with prolonged, repeated cycling, particularly around inflammation and glucose handling.
How to Interpret These Studies Like a Clinician
Given the seemingly conflicting headlines ("yo-yo dieting fears debunked" versus "obesogenic inflammatory memory drives dangerous effects"), here's a practical framework for weighing this evidence, the way an endocrinologist or metabolic researcher would:
1. Distinguish clinical outcomes from mechanistic findings. The Lancet review is strongest on measurable, patient-relevant outcomes: body weight, standard body composition, fasting glucose, blood pressure. The inflammatory memory and epigenetic research is strongest on cellular mechanisms that may not yet show up on a standard lab panel but could matter over a longer horizon.
2. Distinguish population averages from individual risk factors. "No convincing average harm" does not mean "no risk for anyone." Age, baseline muscle mass, number and magnitude of cycles, and how weight is lost (crash dieting versus supervised, structured programs) all modify individual risk.
3. Distinguish diet-driven cycling from drug-driven cycling. The evidence on rapid, large-magnitude, medication-driven cycling (GLP-1 discontinuation) is more concerning than the evidence on gradual, diet-based cycling — mainly because of the scale of lean mass loss involved.
4. Weigh the alternative. Even under a cautious reading of the mechanistic evidence, the comparison that matters clinically is weight cycling versus remaining at a higher, stable weight — not weight cycling versus effortless, permanent weight loss on the first attempt. For most people with obesity-related disease risk, the Lancet review's authors argue that discouraging weight-loss attempts due to cycling fears is not supported and may do more harm than good.
Practical Protocol: Minimizing Any Real Risk
Whether or not weight cycling turns out to carry meaningful long-term harm, the strategies that protect you are the same ones good clinical practice has recommended for years. Here is a practical, evidence-aligned protocol:
Before you start a weight-loss attempt
Get a baseline sense of your body composition, not just weight — a DEXA scan or bioelectrical impedance analysis if accessible, so you can track fat versus lean mass changes over time.
Discuss goals and pace with a clinician or registered dietitian, especially if you have cycled multiple times before or are over age 60.
During active weight loss
Aim for a moderate rate of loss (roughly 0.5–1% of body weight per week) rather than very aggressive restriction, which is associated with greater lean mass loss.
Prioritize protein intake — commonly cited targets in the muscle-preservation literature range from 1.2–1.6 g/kg body weight per day during a calorie deficit (confirm the right target for you with your clinician, especially with kidney disease).
Incorporate resistance training at least 2–3 times per week; this is the single most consistently supported intervention across the muscle-preservation and GLP-1 literature.
During weight maintenance or regain risk periods
Build a specific maintenance plan before you finish losing weight — don't wait until regain starts to think about it.
If you are on or stopping a GLP-1/GIP medication, ask your prescriber about a structured tapering plan and continued resistance training, rather than abrupt discontinuation.
Track strength and function (not just the scale) as a marker that muscle is being preserved through any weight changes.
If you have cycled weight multiple times already
Don't assume damage has been done — per the 2026 Lancet review, there is limited evidence this alone has permanently harmed your metabolism.
Do get a current assessment of muscle mass and metabolic markers (fasting glucose, HbA1c, lipids, blood pressure) so future decisions are based on where you are now, not fear of the past.
Evidence Summary
Magkos & Stefan (2026) — Expert Evidence Review (Lancet Diabetes & Endocrinology)
Main Finding: There is no convincing causal evidence that weight cycling independently harms body composition, metabolic rate, or overall disease risk once confounding factors are controlled.
Clinical Takeaway: Patients should not avoid or delay weight-loss attempts purely out of fear of weight cycling.
Sanaya, Janusaite, Dalamaga & Magkos (2024) — Narrative Review (Current Obesity Reports)
Main Finding: A summary of physiological effects across multiple studies highlights that the findings are inconsistent and highly context-dependent.
Clinical Takeaway: The physical effects of weight cycling vary heavily by population, the specific methods used, and the overall magnitude of the weight changes.
Zamboni et al. (2025) — Review (Reviews in Endocrine & Metabolic Disorders)
Main Finding: Older adults and individuals with low baseline muscle mass are at a significantly higher risk of developing sarcopenia (muscle wasting) or sarcopenic obesity when cycling weight.
Clinical Takeaway: Age and baseline muscle status are critical modifiers of individual patient risk.
Hegazi & Halpern (2025) — Commentary (Reviews in Endocrine & Metabolic Disorders)
Main Finding: Historical and current obesity research has under-prioritized the importance of tracking muscle mass relative to fat mass.
Clinical Takeaway: Clinicians and patients must track muscle preservation, not just scale weight or fat loss, during any period of weight change.
Navarro et al. (2026) — Animal Study (Biomolecules)
Main Finding: An "obesogenic inflammatory memory" lingers within adipose (fat) tissue and immune cells despite the normalization of body weight, glucose, and lipid levels.
Clinical Takeaway: Standard metabolic laboratory panels may look completely normal even while subclinical inflammatory risks persist.
Alexander & Howden (2026) — Review (Curr Opin Clin Nutr Metab Care)
Main Finding: Stopping GLP-1 receptor agonists causes a rapid rebound in weight and metabolic markers; crucially, up to 40% of the weight lost on these injectable medications is lean mass.
Clinical Takeaway: Structured medication tapering combined with strict resistance training is vital around the use of GLP-1 drugs to preserve muscle integrity.Common Myths & Mistakes
Myth: "Every time you yo-yo diet, your metabolism gets permanently slower." Reality: Metabolic rate drops during active weight loss in proportion to weight lost, and largely recovers with weight stabilization or regain. Current evidence doesn't support a progressively "broken" metabolism from repeated cycling alone.
Myth: "It's healthier to just stay at a higher weight than risk yo-yo dieting." Reality: The 2026 Lancet review's authors explicitly caution against this conclusion — discouraging weight-loss attempts due to cycling fears is not supported by the evidence and may forgo real cardiometabolic benefits of successful weight loss.
Myth: "If my bloodwork looks normal after weight cycling, there's no lingering effect." Reality: Emerging inflammatory-memory research suggests subclinical changes in fat tissue and immune cells can persist even when standard labs normalize. This is an active research area, not a settled one.
Myth: "GLP-1 medication weight cycling is basically the same as diet-based yo-yo dieting." Reality: It isn't — the speed of loss, scale of lean mass loss (up to 40%), and speed of regain after discontinuation make medication-driven cycling a distinct, more concerning scenario requiring its own management plan.
Mistake: Judging "success" only by the number on the scale. Fix: Track body composition and strength alongside weight, especially if you have cycled before or are over 60.
Mistake: Stopping a GLP-1 medication abruptly without a plan. Fix: Work with your prescriber on tapering and pair any weight-loss phase (diet or drug-based) with resistance training.
FAQs
1. Is weight cycling (yo-yo dieting) actually bad for you? According to a major 2026 evidence review in The Lancet Diabetes & Endocrinology, there is no convincing evidence that weight cycling itself causes long-term clinical harm once other factors like age and baseline health are accounted for. However, mechanistic research suggests subclinical effects — particularly in adipose tissue inflammation and muscle preservation — may still matter for certain people.
2. Does yo-yo dieting slow down your metabolism permanently? Not according to current evidence. Metabolic rate drops during active weight loss in proportion to the weight lost, and this largely reverses once weight stabilizes or is regained. There's limited support for a cumulative, permanent metabolic slowdown from repeated cycling.
3. Does weight cycling cause more fat gain and less muscle each time? Controlled studies generally show the fat-to-muscle ratio of weight lost during comparable diets is similar whether or not someone has cycled before. However, older adults and people with lower baseline muscle mass appear more vulnerable to unfavorable body composition shifts with repeated cycling.
4. Is it worse to yo-yo diet than to just stay overweight? The authors of the 2026 Lancet review specifically argue against this idea. Discouraging weight-loss attempts due to fear of cycling isn't supported by the evidence, and remaining at a higher weight carries its own well-established cardiometabolic risks.
5. What is "obesogenic inflammatory memory"? It's a concept, tested in a 2026 mouse study, describing how fat tissue and immune cells can retain an inflammatory "memory" of a past obese state even after weight and standard metabolic markers normalize — potentially predisposing the body to faster or worse rebound effects if weight is regained again.
6. Is weight cycling from stopping Ozempic, Wegovy, or Zepbound different from regular yo-yo dieting? Yes. Research specific to GLP-1/GIP medications shows discontinuation leads to rapid, near-complete weight and metabolic rebound within about a year, and up to 40% of weight lost on these drugs can be muscle mass — making the regain disproportionately fat. This is considered a higher-concern pattern than gradual diet-based cycling.
7. How can I protect my muscle mass if I know I might regain weight? Resistance training 2–3 times per week and adequate protein intake during any weight-loss phase are the most consistently supported strategies across the literature, including specifically for people using GLP-1 medications.
8. Should I avoid dieting altogether if I've yo-yo dieted many times before? Not based on current evidence. There's no strong indication that prior cycling has permanently damaged your metabolism. A more useful step is getting a current assessment of your muscle mass and metabolic markers and planning your next attempt with structured support.
9. Does weight cycling increase diabetes or heart disease risk? Observational studies have shown associations, but the 2026 Lancet review found these associations weaken substantially after adjusting for baseline BMI, age, and health status — suggesting underlying adiposity, not cycling itself, may be the main driver in many cases.
10. What should I do if I'm planning to stop a GLP-1 weight-loss medication? Talk to your prescribing clinician about a structured tapering approach rather than stopping abruptly, and consider starting or continuing a resistance-training program to help preserve lean mass and metabolic benefits during the transition.
11. Is weight cycling worse for older adults? Current evidence suggests yes — particularly regarding muscle mass and risk of sarcopenic obesity, because older adults typically start with lower muscle reserves and may recover lean mass less efficiently during regain phases.
12. How much weight loss counts as "weight cycling" in research? Definitions vary, but many studies use a threshold of losing and regaining at least 5–10 pounds, or about 5% of body weight, more than once, as the working definition of clinically relevant weight cycling.
Conclusion & Action Steps
The 2026 Lancet Diabetes & Endocrinology review is a genuinely important shift in how the field understands weight cycling: the specific fear that yo-yo dieting permanently damages your metabolism or body composition is not well-supported by rigorous evidence, and this fear should not, on its own, stop someone with obesity-related health risks from attempting weight loss.
At the same time, this isn't a blanket "don't worry about it" verdict. Mechanistic research on inflammatory memory, the particular vulnerability of older adults and people with low muscle mass, and the distinct risks of rapid weight regain after stopping GLP-1 medications all point to real, active areas where care and structure genuinely matter.
Your action steps:
Don't let fear of "yo-yo dieting" alone stop you from pursuing medically appropriate weight loss — the strongest current evidence doesn't support that fear as a reason to avoid trying.
Track body composition and strength, not just the scale, especially if you're over 60 or have cycled weight multiple times.
Prioritize protein and resistance training during any weight-loss phase, diet-based or medication-based.
If you use a GLP-1 medication, plan any discontinuation with your prescriber — don't stop abruptly.
Talk to your doctor or a registered dietitian about your specific history and risk factors before starting your next attempt — general population findings don't replace individualized care.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Beyond the Scale: Low-Carb vs Low-Fat Diets for Visceral Fat Loss and Muscle Preservation
Visceral Fat Treatment: GLP-1, Semaglutide, and SGLT2 Explained
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Magkos, F., & Stefan, N. (2026). Is weight cycling clinically harmful? The Lancet Diabetes & Endocrinology, 14(7), 594–607. https://doi.org/10.1016/S2213-8587(26)00037-9
Sanaya, N., Janusaite, M., Dalamaga, M., & Magkos, F. (2024). The Physiological Effects of Weight-Cycling: A Review of Current Evidence. Current Obesity Reports.
Zamboni, M., Giani, A., Fantin, F., Rossi, A., Mazzali, G., & Zoico, E. (2025). Weight cycling and its effects on muscle mass, sarcopenia and sarcopenic obesity. Reviews in Endocrine and Metabolic Disorders, 26(4), 767–783.
Navarro, M.D., Hinchado, M.D., Bote, E., Gálvez, I., Otero, E., Palomino-Segura, M., Martín-Cordero, L., & Ortega, E. (2026). Obesogenic Inflammatory Memory: A New Concept Related to the Dangerous Effects of Weight Cycling. Biomolecules, 16(2), 193.
Hegazi, R., & Halpern, B. (2025). Looking beyond fat in obesity: the frequently overlooked importance of muscle mass. Reviews in Endocrine & Metabolic Disorders, 26, 719–721.
Alexander, S.E., & Howden, E.J. (2026). Metabolic rebound and weight cycling following incretin mimetic drug withdrawal: a cause for concern? Current Opinion in Clinical Nutrition and Metabolic Care, 29(4), 395–402.
Hinte, L.C., Castellano-Castillo, D., Ghosh, A., Melrose, K., Gasser, E., Noé, F., et al. (2024). Adipose tissue retains an epigenetic memory of obesity after weight loss. Nature, 636, 457–465.
Blaszczak, A.M., Bernier, M., Wright, V.P., et al. Obesogenic Memory Maintains Adipose Tissue Inflammation and Insulin Resistance. ImmunoMetabolism.
Bernecker, M., Lin, A., Feuchtinger, A., Molenaar, A., Schriever, S.C., & Pfluger, P.T. (2025). Weight cycling exacerbates glucose intolerance and hepatic triglyceride storage in mice with a history of chronic high fat diet exposure. Journal of Translational Medicine.
Grunvald, E., et al. Strategies for minimizing muscle loss during use of incretin-mimetic drugs for treatment of obesity. Obesity Reviews (roundtable consensus paper).
West, S., Scragg, J., Aveyard, P., et al. (2025). Weight regain after cessation of medication for weight management: systematic review and meta-analysis. The Lancet Regional Health – Europe, 52, 101261.
Lean, M.E.J., Leslie, W.S., Barnes, A.C., et al. (2019). Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT trial. Lancet Diabetes & Endocrinology, 7, 344–355.
Bellicha, A., van Baak, M.A., Battista, F., et al. (2021). Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: an overview of 12 systematic reviews and 149 studies. Obesity Reviews, 22(S4), e13256.
Magkos, F., Fraterrigo, G., Yoshino, J., et al. (2016). Effects of moderate and subsequent progressive weight loss on metabolic function and adipose tissue biology in humans with obesity. Cell Metabolism, 23, 591–601.
Gross, K., & Brinkmann, C. (2024). Why you should not skip tailored exercise interventions when using incretin mimetics for weight loss. Frontiers in Endocrinology.