VO₂ Max in Cardiology: The Missing Vital Sign for Cardiovascular Risk and Longevity
Understand VO₂ max, the gold-standard measure of cardiorespiratory fitness, and its role in predicting cardiovascular disease, longevity, and metabolic health.
HEARTEXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/1/202616 min read
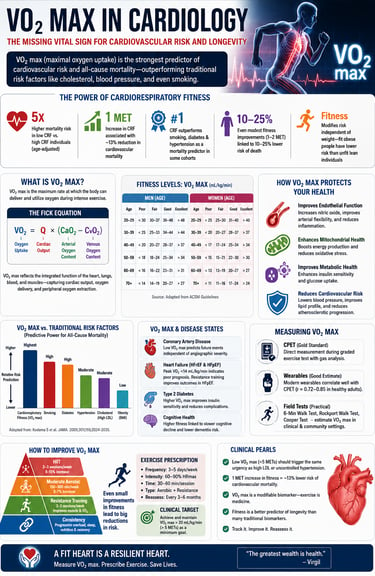
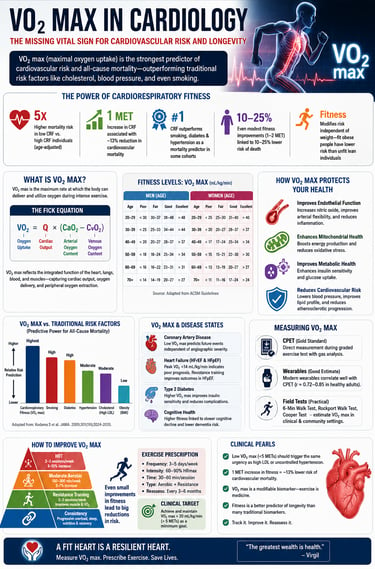
VO₂ max is the most powerful yet underused predictor of cardiovascular risk—outperforming traditional markers like cholesterol, blood pressure, and even smoking in some cohorts. This article explores why cardiorespiratory fitness is the missing vital sign in modern cardiology and how it can be measured, interpreted, and improved in clinical practice.
VO₂ max is a stronger independent predictor of mortality than smoking in multiple large cohort studies.
Even modest fitness improvements (1–2 MET increase) are associated with 10–25% reductions in cardiovascular and all-cause mortality.
Fitness modifies cardiovascular risk independent of body weight — a fit obese person is at lower risk than an unfit normal-weight person.
Low CRF (<5 METs) should trigger the same clinical urgency as high LDL or uncontrolled hypertension.
In HFpEF, peripheral muscle dysfunction drives VO₂ max limitation — resistance training is particularly important in this population.
Wearable VO₂ max estimates in healthy populations now correlate well with CPET results (r ≈ 0.72–0.85).
Exercise prescription is medicine — and it has a dose, a target, and a measurable endpoint.
Elite Clinician Perspective: VO₂ Max as a Missing Vital Sign
We are measuring risk—but not capacity.
Modern cardiology excels at quantifying static biomarkers (LDL, HbA1c, BP), yet fails to routinely assess physiological reserve. VO₂ max fills this gap by capturing what the cardiovascular system can actually deliver under stress.A normal report does not equal a resilient patient.
Patients with optimal lipids and normal angiograms may still have critically low cardiorespiratory fitness (CRF). These individuals often declare themselves only when exposed to physiological stress—frequently as acute coronary events.VO₂ max is the most integrative biomarker we have.
It reflects cardiac output, endothelial function, mitochondrial efficiency, skeletal muscle health, and oxygen delivery—all within a single metric. No traditional biomarker offers this systems-level insight.Low fitness is a high-risk state—clinically equivalent to disease.
A VO₂ max in the lowest quartile confers mortality risk comparable to smoking or diabetes. This should trigger the same clinical urgency as uncontrolled hypertension or dyslipidaemia.Fitness modifies risk independent of weight.
The “fit vs. fat” paradigm is clinically real: an obese patient with moderate-to-high CRF often has lower cardiovascular risk than a lean but sedentary individual. BMI alone is an insufficient risk stratifier.Exercise is not lifestyle advice—it is therapy.
VO₂ max is one of the few biomarkers that is directly modifiable. Structured exercise interventions can produce risk reductions comparable to pharmacological therapies, particularly in high-risk populations.We must start prescribing and tracking fitness.
Incorporating METs or estimated VO₂ max into routine consultations transforms exercise from vague advice into a measurable clinical endpoint—what gets measured gets managed.The future of cardiology is functional, not just biochemical.
Integrating CRF into risk models represents a paradigm shift—from treating numbers to treating physiology.
What Is VO₂ Max? A Deeper Look Beyond the Textbook
VO₂ max — or maximal oxygen uptake — quantifies the maximum rate at which the cardiovascular and muscular systems can deliver and utilise oxygen during peak exercise. It is expressed in millilitres of oxygen per kilogram of body weight per minute (mL/kg/min) and is calculated through the Fick Equation:
The Fick Equation
VO₂ = Cardiac Output (Q) × Arteriovenous Oxygen Difference (CaO₂ − CvO₂)
This elegant equation reveals that VO₂ max is not merely a "lung" or "heart" measurement — it is an integrated physiological measure encompassing cardiac output (how much blood the heart pumps), oxygen delivery (haemoglobin, lung function), and peripheral oxygen extraction (muscle mitochondrial density, capillary networks).
A critical distinction often lost in clinical practice is the difference between VO₂ max (true physiological maximum, limited by central factors), VO₂ peak (the highest value achieved during testing, which may fall short of true maximum), and METs (Metabolic Equivalents — a practical field measurement where 1 MET ≈ 3.5 mL/kg/min resting oxygen consumption).
Recent work using the NASA method for VO₂ estimation has shed new light on how hemodynamic responses — including stroke volume, heart rate trajectory, and oxygen pulse — relate to functional aerobic capacity across different adult populations, underscoring that VO₂ max captures far more than fitness level alone (Arzayus-Patiño et al., 2026).
VO₂ Max as a Predictor of Mortality: The Evidence Is Overwhelming
The epidemiological case for CRF as a mortality predictor is, at this point, compelling beyond a reasonable doubt. Landmark data from the Cooper Clinic cohort and the FRIEND (Fitness Registry and the Importance of Exercise: A National Database) registry consistently demonstrate a steep, graded, dose-response relationship between cardiorespiratory fitness and all-cause and cardiovascular mortality.
5×: Higher mortality risk in low CRF vs. high CRF individuals (age-adjusted)
1 MET: Increase in CRF associated with ~13% reduction in cardiovascular mortality
>#1:CRF outperforms smoking, diabetes & hypertension as a mortality predictor in some cohorts
The comparative context is startling. A seminal analysis published in JAMA demonstrated that when age-adjusted fitness levels were compared head-to-head with traditional cardiovascular risk factors — including smoking, diabetes, and hypertension — low CRF emerged as the most powerful independent predictor of all-cause mortality in both men and women. Abdalla et al. (2025) confirm in their comprehensive review of VO₂ max in clinical cardiology that this evidence extends to contemporary populations and that fitness-related risk is not merely a proxy for other lifestyle factors.
"You cannot medicate your way out of low fitness." — The core clinical challenge of integrating CRF into standard care.
The concept of "fitness vs. fatness" further complicates the standard obesity-risk narrative: metabolically healthy individuals with high VO₂ max demonstrate substantially lower cardiovascular risk than normal-weight individuals with poor fitness. Body weight, it turns out, is a far less reliable signal than the physiological capacity that underlies it (Isath et al., 2023).
The Vascular Biology of VO₂ Max: How Fitness Protects Your Arteries
Understanding why VO₂ max predicts cardiovascular outcomes requires a journey into vascular biology — and it is here that the connection becomes truly remarkable.
Endothelial Function and Nitric Oxide
Regular aerobic exercise increases vascular shear stress — the frictional force of blood flow against arterial walls. This mechanical stimulus upregulates endothelial nitric oxide synthase (eNOS), leading to greater nitric oxide (NO) bioavailability. Nitric oxide is not merely a vasodilator; it is a master regulator of vascular homeostasis that inhibits platelet aggregation, reduces monocyte adhesion, and suppresses vascular smooth muscle proliferation. Individuals with higher VO₂ max consistently demonstrate superior flow-mediated dilation (FMD) — a non-invasive measure of endothelial function — compared to sedentary counterparts.
Arterial Stiffness and Vascular Aging
Aortic stiffness, measured by pulse wave velocity (PWV), is an independent predictor of cardiovascular events and a marker of accelerated vascular aging. Longitudinal data consistently show that individuals with higher CRF maintain more compliant, elastic arteries into later decades of life. Fitness appears to slow the molecular clock of vascular aging — partly through anti-inflammatory mechanisms and partly through preserved smooth muscle cell phenotype.
Microvascular Health
Perhaps most underappreciated is the relationship between VO₂ max and microvascular function. High CRF is associated with greater skeletal muscle capillary density, superior mitochondrial coupling efficiency, and enhanced GLUT-4 transporter expression — enabling more efficient glucose uptake independent of insulin. This is the mechanistic link between fitness and type 2 diabetes prevention.
VO₂ Max Across Cardiometabolic Disease Spectrum
The clinical significance of CRF extends well beyond primary prevention. Across the full spectrum of cardiometabolic disease, VO₂ max functions as both a diagnostic indicator and a therapeutic target.
In insulin resistance and type 2 diabetes, skeletal muscle accounts for approximately 80% of insulin-stimulated glucose disposal — and it is precisely here that fitness exerts its metabolic influence. Higher VO₂ max reflects greater mitochondrial oxidative capacity, reduced intramyocellular lipid accumulation, and improved metabolic flexibility (the ability to switch between fuel sources). These adaptations are partially independent of weight loss, meaning exercise improves glycaemic control through mechanisms beyond caloric expenditure alone.
In hypertension, exercise-induced reductions in vascular resistance operate through multiple parallel pathways: reduced sympathetic nervous system tone, enhanced baroreflex sensitivity, decreased circulating renin-angiotensin system activity, and improved endothelial function — all captured in summary by the VO₂ max metric.
In obesity, VO₂ max serves as a marker of metabolic flexibility and functional health independent of BMI — challenging the simplistic view that body weight alone determines cardiometabolic risk. An obese individual with a VO₂ max above the 50th percentile for age carries substantially lower cardiovascular risk than a normal-weight individual below the 20th percentile.
VO₂ Max vs. Traditional Biomarkers: A Direct Comparison
LDL Cholesterol
Measures: Atherogenic lipid burden in circulation
Limitation: Static value; does not reflect endothelial function or vascular performance
VO₂ Max Advantage: Places lipid risk within the context of overall cardiovascular function and capacity
HbA1c
Measures: Average blood glucose over ~3 months
Limitation: Glucose-centric; fails to capture insulin resistance and metabolic flexibility
VO₂ Max Advantage: Reflects mitochondrial efficiency, substrate utilization, and whole-body metabolic health
Blood Pressure
Measures: Arterial pressure at a single point in time
Limitation: Variable; influenced by environment (e.g., white-coat effect); does not assess physiological reserve
VO₂ Max Advantage: Captures dynamic vascular response and adaptability during physical stress
C-Reactive Protein (CRP)
Measures: Systemic inflammation
Limitation: Non-specific; elevated in multiple unrelated conditions
VO₂ Max Advantage: Integrates inflammatory, endothelial, and metabolic health into a functional outcome
VO₂ Max
Measures: Integrated cardiorespiratory capacity (heart, lungs, muscles)
Limitation: Requires effort, testing protocols, or estimation tools
Clinical Strength: Represents a true “integrated physiologic reserve marker”—capturing how the body performs, not just what it contains
Bottom Line
Traditional biomarkers = static, isolated risk indicators
VO₂ max = dynamic, systems-level measure of functional health and resilience
Measuring VO₂ Max in Clinical Practice
The gold standard for VO₂ max measurement remains Cardiopulmonary Exercise Testing (CPET) — a graded maximal exercise test with breath-by-breath gas analysis providing simultaneous assessment of ventilatory thresholds, cardiac output, heart rate recovery, and exercise capacity. However, CPET requires specialised equipment and trained personnel, limiting its accessibility in routine outpatient settings.
Treadmill-Based Protocols (Bruce, Modified Bruce, Cornell)
Estimate VO₂ max using exercise duration and workload via validated regression equations
Widely used in clinical and stress-testing settings
Modified Bruce Protocol is especially suitable for elderly or deconditioned patients due to its gradual intensity progression
6-Minute Walk Test (6MWT)
Simple, low-cost functional assessment
Particularly useful in patients with heart failure and chronic pulmonary disease
Reflects submaximal functional capacity rather than true VO₂ max
Non-Exercise Prediction Models
Use variables such as age, sex, resting heart rate, and physical activity level
Can be integrated into electronic health records for rapid risk estimation
Useful for large-scale screening and routine outpatient assessment
Consumer Wearables
Utilize optical heart rate monitoring and GPS-derived activity data
Provide reasonably accurate VO₂ max estimates in healthy populations
Accuracy in patients with cardiovascular or metabolic disease remains under investigation (Abdalla et al., 2025)
Clinical Insight
While cardiopulmonary exercise testing (CPET) remains the gold standard, these alternative methods enable scalable, practical assessment of cardiorespiratory fitness across diverse clinical settings.
Clinical Risk Stratification by Metabolic Equivalents (METs)
Understanding your MET capacity is essential for predicting surgical outcomes and long-term cardiac resilience. Here is the clinical breakdown of risk categories:
High Risk (< 5 METs): The "Clinical Red Zone"
Functional Status: Patients are unable to climb a single flight of stairs or walk at a brisk pace without significant shortness of breath (dyspnoea).
Prognosis: This level is associated with a very poor prognosis in both surgical and cardiac settings. It indicates a severe lack of physiologic reserve, making even minor stressors potentially life-threatening.
Moderate Risk (5–8 METs): The "Functional Baseline"
Functional Status: Individuals are generally capable of performing most daily activities, such as light housework or walking on level ground.
Prognosis: While functional, this group remains at elevated risk for future cardiac events. These patients stand to gain the most significant survival benefits from entering a structured exercise programme to migrate toward the "Protective" tier.
Protective (> 10 METs): The "Cardiac Resilience" Tier
Functional Status: Individuals can easily perform vigorous activities, such as jogging, heavy yard work, or climbing multiple flights of stairs without fatigue.
Prognosis: This level exerts a strong cardioprotective effect. Reaching 10+ METs is the "gold standard" for longevity, as it is statistically linked to the lowest rates of all-cause and cardiovascular mortality across all age groups.
Exercise as Medicine: Improving VO₂ Max as a Therapeutic Target
If VO₂ max is a biomarker, it is a uniquely actionable one. Unlike LDL, which requires pharmacological intervention when diet fails, or blood pressure, which may necessitate lifetime medication, VO₂ max is fundamentally modifiable through structured exercise — and the magnitude of improvement carries direct clinical benefit.
High-Intensity Interval Training (HIIT) vs. Moderate-Intensity Continuous Training (MICT)
A comprehensive overview of systematic reviews and meta-analyses by Crowley et al. (2022) evaluated the differential effects of exercise training intensity on VO₂ max in healthy adults. The findings support a clear intensity-response relationship: higher training intensities — particularly HIIT — produce greater improvements in VO₂ max relative to volume-matched MICT. However, the absolute magnitude of improvement and the optimal training modality appear to be population- and context-dependent. For sedentary, deconditioned, or elderly individuals, MICT provides meaningful VO₂ max gains with a more favourable safety profile and greater adherence.
Tamayo Acosta et al. (2022) further investigated aerobic exercise versus HIIT effects on both VO₂ max and blood pressure, finding that both modalities produced statistically significant improvements in VO₂ max, but HIIT demonstrated superior gains alongside comparable blood pressure reductions — suggesting HIIT may be particularly valuable in hypertensive patients who can tolerate the intensity.
A practical exercise prescription framework for VO₂ max improvement in clinical populations might incorporate:
Aerobic Foundation (Weeks 1–4)
3–4 sessions/week at 50–65% heart rate reserve (HRR). Walking, cycling, swimming. Duration 20–30 min. Build aerobic base and compliance.
Progressive Overload (Weeks 5–12)
Increase to 65–75% HRR. Introduce 4×4 min HIIT intervals (85–95% peak HR) 1–2×/week. Expected VO₂ max gain: 8–15%.
Resistance Training Synergy
2×/week compound resistance exercises. Enhances skeletal muscle oxidative capacity and insulin sensitivity independent of aerobic training.
Reassess & Iterate
Re-measure VO₂ max or METs at 12 weeks. Even a 1 MET improvement reduces cardiovascular mortality risk by ~13%. Track as a vital sign.
The dose-response data are clinically encouraging: the greatest relative risk reduction from fitness improvement occurs in the transition from very low to moderate CRF. A previously sedentary individual who achieves even a modest improvement in VO₂ max — moving from below the 20th to the 40th percentile — realises a proportionally larger risk-benefit than an already-fit individual pursuing elite performance.
Special Populations: Tailoring VO₂ Max Assessment
In heart failure, VO₂ max carries particular clinical weight. Peak VO₂ below 14 mL/kg/min has historically been used as a threshold for advanced heart failure therapies including cardiac transplantation listing. Importantly, VO₂ max profiles differ between HFrEF (where central cardiac output limitation predominates) and HFpEF (where peripheral factors — including skeletal muscle dysfunction and impaired oxygen extraction — play an equal or greater role).
In post-MI patients, early cardiac rehabilitation with structured exercise training improves VO₂ max, reduces rehospitalisation, and independently reduces mortality — with effect sizes comparable to pharmacological interventions. In the elderly, where frailty and VO₂ max decline intersect, fitness-targeted exercise programmes demonstrate the potential to compress morbidity and maintain functional independence. In women, hormonal transitions — particularly menopause — produce accelerated declines in VO₂ max and vascular function that are only partially attenuated by hormone replacement, underscoring the critical role of exercise interventions in this demographic.
VO₂ Max, Longevity, and the Biological Age Conversation
The emerging science of biological aging has provided new mechanistic context for the VO₂ max–longevity relationship. Higher CRF is associated with longer telomere length, superior mitochondrial biogenesis (via PGC-1α activation), enhanced autophagic flux, and lower systemic levels of pro-inflammatory cytokines including CRP and IL-6. These are not independent phenomena — they converge on a shared mechanism where physical fitness fundamentally resets the inflammatory and metabolic milieu toward biological youth.
The practical implication is powerful: an individual's VO₂ max, adjusted for age, may represent one of the most accessible proxies for biological age currently available in routine clinical assessment (Isath et al., 2023).
Integrating VO₂ Max into Daily Clinical Practice
A Pragmatic “Fitness Vital Sign” Framework
Non-Exercise VO₂ Max Estimation
Utilises validated algorithms incorporating age, sex, resting heart rate, and physical activity level
Easily embedded within electronic health record (EHR) systems
Enables rapid, scalable assessment in routine outpatient settings
Routine Treadmill Testing
Incorporate during annual cardiovascular risk evaluations
Provides MET-based estimation of functional capacity
Can supplement or, in selected cases, replace standard stress ECG for broader physiological insight
Wearable Data Integration
Consumer devices increasingly provide VO₂ max estimates using heart rate and activity data
Offers continuous, real-world monitoring of fitness trends
Serves as a valuable adjunct to clinical assessment as validation improves
Risk Stratification Models
Integration of cardiorespiratory fitness (CRF) into established tools (e.g., ASCVD, HEART score)
Enhances predictive accuracy by incorporating functional capacity
Represents an emerging frontier in preventive cardiology
Clinical Perspective: A Necessary Paradigm Shift
The limitation is not technological, but conceptual
Traditional cardiology has focused on a cholesterol-centric, biomarker-driven model of risk
Emerging evidence supports a transition toward a physiology-centric approach, where:
Cardiovascular performance is measured, not just risk factors
Functional reserve is tracked longitudinally
Exercise capacity becomes a therapeutic target, not merely a lifestyle variable
Bottom Line
VO₂ max transforms cardiovascular care from static risk estimation to dynamic physiological assessment—bridging the gap between prevention, performance, and long-term health outcomes.
Frequently Asked Questions
What is a "good" VO₂ max for my age?
A "good" VO₂ max varies significantly by age and sex. Generally, for a 40-year-old male, a score above 40 mL/kg/min is considered good; for a 40-year-old female, above 33 mL/kg/min is the benchmark. However, for longevity, clinicians look for individuals to be in the top 25% (upper quartile) of their peer group.
Is VO₂ max a better predictor of death than smoking?
Yes. Peer-reviewed research, including studies published in JAMA, demonstrates that low cardiorespiratory fitness (CRF) is a stronger predictor of all-cause mortality than smoking, diabetes, or hypertension. Moving from the lowest fitness category to a moderate category can reduce your mortality risk by nearly 50%.
How can I increase my VO₂ max fast?
The most efficient way to increase VO₂ max is through High-Intensity Interval Training (HIIT). A proven protocol is the "4x4 method":
4 minutes of high-intensity effort (85–95% max heart rate).
3 minutes of active recovery (light walking).
Repeat 4 times, twice per week.
This method typically yields an 8–15% improvement within 12 weeks.
Can I estimate my VO₂ max without a lab test?
Yes. While a CPET (Cardiopulmonary Exercise Test) is the gold standard, you can estimate your score using:
Wearable Devices: Apple Watch, Garmin, and Fitbit use heart rate and pace data to provide ±5% accuracy.
The Cooper Test: Measuring how far you can run in 12 minutes.
Rockport Walk Test: Measuring heart rate after a brisk 1-mile walk.
Why does VO₂ max matter for heart disease?
VO₂ max measures how well your heart, lungs, and blood vessels work together. A high score indicates superior endothelial function (flexible arteries) and high mitochondrial density. Low VO₂ max is often a "hidden" indicator of vascular stiffness and metabolic dysfunction, even if your cholesterol and blood pressure look normal.
Clinical pearls
1. The "Integrated Reserve" Principle
Scientific Perspective: VO 2 max is an integrated physiological marker of the "oxygen conductant system." It represents the functional synergy of pulmonary diffusion, cardiac stroke volume, haemoglobin affinity, and mitochondrial oxidative phosphorylation. Unlike static biomarkers (like LDL), it measures dynamic physiologic reserve.
Think of your body like a car. Your cholesterol is like the quality of the fuel, but VO2 max is the horsepower of the engine. Even if you have "clean fuel," a weak engine won't handle a steep hill (physical stress) well. Improving this score makes your "engine" more efficient and harder to break.
2. The "Smoker’s Paradox" of Fitness
Scientific Perspective: Low cardiorespiratory fitness (CRF), defined as being in the lowest 20th percentile for one's age/sex, carries a hazard ratio for all-cause mortality that exceeds that of current smoking, type 2 diabetes, and end-stage renal disease.
Being extremely "out of shape" is actually riskier for your heart than smoking. If you’re worried about your health but only focus on your blood test results while staying sedentary, you’re missing the biggest danger signal your body has.
3. The Endothelial "Shear Stress" Benefit
Scientific Perspective: Aerobic exercise induces laminar shear stress on the vascular endothelium, upregulating endothelial nitric oxide synthase (eNOS). This improves nitric oxide bioavailability, which prevents arterial stiffening and inhibits the pro-atherogenic processes of leukocyte adhesion and smooth muscle proliferation.
When you exercise, and your heart rate goes up, the blood rushing through your arteries acts like a "power wash" for your blood vessels. It signals your arteries to release a gas (nitric oxide) that keeps them flexible and slippery, preventing "clogs" from forming in the first place.
4. Metabolic Flexibility and the Mitochondria
Scientific Perspective: VO 2 max is a proxy for mitochondrial density and efficiency. High CRF is associated with enhanced metabolic flexibility—the ability to seamlessly switch between lipid and glucose oxidation. This reduces "lipotoxicity" (fat buildup in the wrong places) and improves systemic insulin sensitivity.
Fitness isn't just about burning calories; it’s about upgrading your cells' batteries (mitochondria). A fit person's body is much better at switching between burning sugar and burning fat. This keeps your blood sugar stable and prevents fat from "leaking" into your organs and causing damage.
5. The "1 MET" Milestone
Scientific Perspective: For every 1 MET (3.5 mL/kg/min) increase in VO 2 max, there is a documented 12–15% reduction in all-cause mortality. This dose-response relationship is most profound in the transition from "Least Fit" to "Below Average," suggesting that the greatest clinical gains occur in the most deconditioned patients.
You don’t need to become an Olympic athlete to see massive benefits. Improving your fitness by just one "level"—for example, going from getting winded on a flight of stairs to being able to walk briskly for 10 minutes—can slash your risk of an early death by over 10%. Every little bit of extra "huff and puff" counts.
Author’s Note
This article was written with a single purpose: to challenge a deeply ingrained assumption in modern cardiology—that cardiovascular risk can be adequately assessed through static biomarkers alone. While cholesterol, blood pressure, and glycaemic indices remain essential, they do not fully capture the dynamic physiological capacity that ultimately determines how the human body responds to stress, illness, and aging.
Cardiorespiratory fitness, expressed as VO₂ max, represents a convergence point of multiple systems—cardiac, vascular, metabolic, and muscular. It is both a reflection of current health and a powerful predictor of future outcomes. Yet, despite decades of compelling evidence, it remains underutilised in routine clinical practice. This gap is not due to lack of data, but rather a lag in translating physiology into everyday decision-making.
As a clinician, I have encountered patients whose laboratory profiles suggested low risk, yet whose functional capacity told a very different story—often revealed only after a cardiac event. These experiences underscore a critical lesson: health cannot be fully understood without assessing what the body can do, not just what its numbers show.
The goal of this work is not to replace traditional risk factors, but to complement and strengthen them by reintroducing a physiology-centred perspective. VO₂ max is not merely a fitness metric; it is a clinically actionable biomarker—one that can be measured, improved, and tracked over time.
If this article encourages even a small shift—prompting clinicians to measure fitness, or patients to value it as a core component of health—then it has served its purpose.
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
Share this article: Send it to a friend or family member who has been told they're "healthy" based solely on blood tests. VO₂ max is the missing piece of their picture.
Ready to Make Fitness Your Most Powerful Biomarker?
Whether you're a patient looking to understand your cardiovascular risk, a clinician considering CRF integration, or a health enthusiast optimising longevity, VO₂ max is where the conversation starts.
Related Articles
You Don't Need 10,000 Steps: How Many Steps Per Day for Heart Health
HIIT vs Moderate Cardio: Which Improves Cardiovascular Fitness Faster?
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
References
Abdalla, H. M., Dreher, L., VanDolah, H., et al. (2025). VO2 Max in clinical cardiology: Clinical applications, evidence gaps, and future directions. Current Cardiology Reports, 27, 130. https://doi.org/10.1007/s11886-025-02289-6
Arzayus-Patiño, L., Rodriguez-Castro, J., Betancourt-Peña, J., Avila-Valencia, J. C., & Benavides-Cordoba, V. (2026). Hemodynamic responses and functional aerobic capacity in adults: Insights from NASA method estimated VO₂. Frontiers in Rehabilitation Sciences, 7, 1731940. https://doi.org/10.3389/fresc.2026.1731940
Crowley, E., Powell, C., Carson, B. P., & Davies, R. W. (2022). The effect of exercise training intensity on VO2max in healthy adults: An overview of systematic reviews and meta-analyses. Translational Sports Medicine, 2022, 9310710. https://doi.org/10.1155/2022/9310710
Isath, A., Koziol, K. J., Martinez, M. W., Garber, C. E., Martinez, M. N., Emery, M. S., Baggish, A. L., Naidu, S. S., Lavie, C. J., Arena, R., & Krittanawong, C. (2023). Exercise and cardiovascular health: A state-of-the-art review. Progress in Cardiovascular Diseases, 79, 44–52. https://doi.org/10.1016/j.pcad.2023.04.008
Tamayo Acosta, J., Sosa Gomez, A. E., Samuel, S., Pelenyi, S., Acosta, R. E., & Acosta, M. (2022). Effects of aerobic exercise versus high-intensity interval training on V̇O2max and blood pressure. Cureus, 14(10), e30322. https://doi.org/10.7759/cureus.30322