Therapeutic Advances in Sarcopenia Management: From Muscle Loss to Recovery
Discover the latest science-backed treatments for sarcopenia. Learn how resistance training, protein, vitamin D, creatine, and emerging therapies can help prevent muscle loss and rebuild strength.
SARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/1/202623 min read
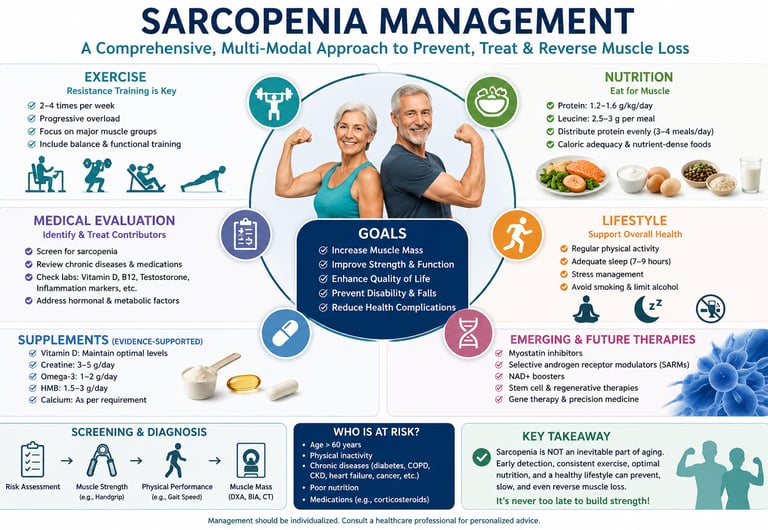
The best way to treat sarcopenia is through progressive resistance training combined with adequate protein intake. Experts recommend strength training 2–3 times weekly and consuming 1.2–1.5 grams of protein per kilogram of body weight daily. Additional measures such as vitamin D optimization, regular physical activity, and management of chronic diseases can further improve muscle strength, physical function, and healthy aging. This multimodal approach remains the gold standard for preventing and treating age-related muscle loss.
Sarcopenia: You Can Fight Back and Win Strength Back
Losing muscle as you get older isn’t something you just have to accept. Doctors now recognize sarcopenia as a real, treatable medical condition — not an unavoidable part of aging. It’s listed as ICD-10 M62.84, and it affects 10–27% of adults over 60. It also costs the U.S. healthcare system $40.4 billion each year in hospital stays alone.
So what’s actually happening? Starting around age 30, your muscles slowly start to lose their ability to grow and repair. After 60, that loss speeds up. Inflammation, hormone changes, low energy in your muscle cells, and fewer muscle stem cells all team up to break muscle down faster than your body can rebuild it [Nguyen et al., 2026; Tan et al., 2026].
The good news from 2024–2026 research: this process can be slowed, stopped, and even partially reversed. The most important marker isn’t just muscle size — it’s strength [Tan et al., 2026].
Here’s what works best:
1. Strength training is your #1 tool. Lifting weights or doing resistance exercises 2–3 times per week tells your muscles to grow. Using weights that feel challenging — about 70–85% of your max — gives the strongest signal [Liu et al., 2025]. You’ll likely notice strength gains in 4–8 weeks.
2. Eat enough protein, at every meal. Older muscles need more protein to grow: 1.2–1.5 g per kg of body weight daily. That’s 25–30 g of high-quality protein at breakfast, lunch, and dinner, with leucine-rich foods like eggs, dairy, fish, or whey [Kuzuya et al., 2025; Kalra et al., 2025].
3. Check vitamin D and inflammation. Vitamin D levels above 30 ng/mL help muscles contract better. Omega-3s from fish or supplements help calm the low-grade inflammation that drives muscle loss [Kalra et al., 2025].
New medicines like SARMs and myostatin blockers are being tested and show promise — adding 1–3 kg of lean mass in studies — but they aren’t approved yet [Liu et al., 2025]. Therapies that repair muscle stem cells and boost cell energy are also on the horizon [Nguyen et al., 2026].
Don’t wait for a fall or fracture to act. Simple checks like the SARC-F questionnaire, grip strength, and walking speed can catch sarcopenia early [Cruz-Jentoft et al., 2019]. Remember: muscle isn’t just for movement. It controls blood sugar, metabolism, and heart health. When muscle fails, your whole body feels it [Tan et al., 2026].
Muscle loss speaks quietly, but you can answer loudly. With the right exercise, food, and medical support, you can protect your strength, independence, and health for years to come.
Key Takeaways
Sarcopenia is a treatable disease, not inevitable aging. Officially recognized as ICD-10 M62.84, it’s progressive muscle failure that can be prevented and partially reversed with targeted action.
Resistance training is the single most effective intervention. Progressive resistance training 2–3x/week at 70–85% 1RM is the gold standard for restoring muscle mass, strength, and function. Strength gains appear in 4–8 weeks.
Protein timing and quality matter as much as quantity. Aim for 1.2–1.5 g/kg/day, with 25–30 g of high-quality protein + 2.5–3 g leucine per meal to overcome age-related anabolic resistance. Early detection changes outcomes. Simple tools like SARC-F, grip strength (<27 kg for men, <16 kg for women), and gait speed <0.8 m/s can flag sarcopenia years before disability sets in.
Muscle is an endocrine organ. Loss of muscle disrupts myokine signalling, worsening insulin resistance, fatty liver, and cardiovascular risk. Treating sarcopenia improves whole-body metabolism.
Drugs and regenerative therapies are adjuncts, not replacements. SARMs, myostatin inhibitors, and NAD⁺ precursors show promise in trials, but none replace exercise + nutrition. They work best combined with lifestyle intervention.
What Is Sarcopenia?
Sarcopenia is the progressive, age-related loss of skeletal muscle mass, strength, and physical function. It begins as early as age 30, accelerates after 60, and significantly increases the risk of falls, disability, metabolic disease, and early death. Recognized since 2016 as an official disease (ICD-10: M62.84), it is now understood to be both preventable and partially reversible with targeted intervention.
The word itself comes from the Greek sarx (flesh) and penia (loss). But it took decades for medicine to treat it as more than an aging footnote. A landmark conceptual definition from the Global Leadership Initiative in Sarcopenia (GLIS) — highlighted in the 2026 Annals of the Academy of Medicine Singapore review — now frames sarcopenia as progressive muscle failure, with strength decline as the primary marker, not mass alone.
There are two main types:
Primary sarcopenia: Driven purely by aging — the gradual hormonal, cellular, and molecular decline that comes with time.
Secondary sarcopenia: Triggered or accelerated by chronic illness (cancer, heart failure, kidney disease), malnutrition, or prolonged physical inactivity. This can occur at any age.
Critically, skeletal muscle is no longer seen as merely a contractile organ. A 2026 review in Annals of the Academy of Medicine Singapore emphasizes that muscle functions as a major endocrine organ, secreting signaling proteins called myokines that regulate systemic metabolism, inflammation, insulin sensitivity, and cardiovascular health. When muscle deteriorates, the ripple effects are system-wide.
Prevalence, Risk & Economic Impact
10–27% of adults over 60 are affected globally
$40.4B Annual U.S. hospitalization costs
~30 Age when muscle decline begins
3–8% Muscle mass lost per decade after 30
Beyond the direct physical consequences, sarcopenia drives a cascade of cardiometabolic harm. The 2026 Singapore review reports that muscle loss exacerbates insulin resistance, impairs glucose utilization, and alters lipid metabolism — directly raising the risk of type 2 diabetes, obesity, metabolic syndrome, fatty liver disease, and cardiovascular disease.
High-risk groups include:
Adults over 60, especially women post-menopause
Patients with type 2 diabetes, chronic kidney disease, COPD, or cancer
Individuals with prolonged bed rest or physical inactivity
Those with poor protein intake or malnutrition
Patients on long-term corticosteroids
The Biology of Muscle Loss: What Goes Wrong?
Understanding sarcopenia requires looking inside the muscle cell. Multiple converging mechanisms drive the condition, which is why no single intervention works alone.
Anabolic Resistance
The mTORC1 pathway — the master switch for muscle growth — stops responding to protein and exercise signals, blunting muscle protein synthesis.
Inflammaging
Chronic low-grade inflammation driven by elevated IL-6 and TNF-α accelerates the ubiquitin-proteasome pathway, tagging healthy muscle proteins for destruction.
Mitochondrial Failure
Aging mitochondria produce excess reactive oxygen species (ROS), creating oxidative stress that damages muscle fibers and perpetuates inflammation.
Satellite Cell Depletion
Muscle-resident stem cells (satellite cells) decline in number and function, destroying the tissue's natural repair capacity.
Hormonal Decline
Falling testosterone, growth hormone, and IGF-1 levels reduce protein synthesis while rising cortisol promotes breakdown.
NAD⁺ Decline
A 2026 review in Endocrinology and Metabolism highlights NAD⁺ depletion as a key driver of mitochondrial dysfunction and impaired cellular energy production in aging muscle.
The Proteostasis Collapse
At the heart of sarcopenia is a failure of proteostasis — the balance between muscle protein synthesis (MPS) and degradation. In aging muscle, two key degradation systems become overactive:
Ubiquitin-proteasome system (UPS): Muscle-specific E3 ligases MuRF1 and atrogin-1 tag proteins for destruction, accelerated by inflammation and hormone decline.
Autophagy-lysosome pathway: The cellular recycling system that is intended to clear damaged components becomes dysregulated, consuming healthy tissue.
The Myokine Connection
Healthy muscle secretes beneficial myokines — including irisin, IL-6 (in its acute exercise-induced form), and BDNF — that support metabolism, brain health, and anti-inflammatory signaling. In sarcopenia, this myokine secretome becomes disrupted, compounding whole-body consequences well beyond simple muscle weakness.
Diagnosing Sarcopenia: The Modern Approach
Early detection is critical, because prevention is dramatically more effective than reversal of advanced disease.
Clinical Screening Tools
SARC-F questionnaire: A validated 5-item screening tool for primary care. Scores ≥4 indicate high sarcopenia risk.
Grip strength testing: Low grip strength (below 27 kg in men, 16 kg in women per EWGSOP2 criteria) is the primary diagnostic signal in modern frameworks.
Gait speed: Walking speed below 0.8 m/s signals poor physical performance, a key sarcopenia outcome measure.
Chair stand test: Inability to complete 5 stands from a chair in under 15 seconds indicates functional impairment.
Muscle Mass Quantification
DXA (dual-energy X-ray absorptiometry): The clinical standard for measuring appendicular lean mass index (ALMI).
Bioelectrical impedance analysis (BIA): Practical, accessible, less precise but suitable for monitoring.
CT/MRI-based radiomics + AI: A rapidly emerging tool highlighted by the Singapore consortium — AI-enabled body composition analysis from routine CT scans shows promise for opportunistic, population-level sarcopenia detection.
Emerging Biomarkers (2025–2026)
The 2026 Endocrinology and Metabolism review by Nguyen et al. identifies several biomarker categories under active investigation:
Creatinine-to-cystatin C ratio (a surrogate for muscle mass)
Circulating myokines (irisin, myostatin, follistatin levels)
Composite multi-marker panels combining inflammatory, hormonal, and metabolic signals
Epigenomic and transcriptomic signatures from multi-omics profiling
Clinical Note
Biomarker-based sarcopenia detection remains a research tool. Widespread clinical use requires large-scale validation and cost-effectiveness assessment — a key priority of Singapore's new national sarcopenia consortium (2026).
Resistance Training: The Undisputed Gold Standard
If sarcopenia treatment had a single non-negotiable cornerstone, it is this: progressive resistance training (PRT). Every major review published in 2024–2026 confirms it. No drug, supplement, or therapy has yet matched its ability to simultaneously improve muscle mass, strength, and function.
Why Resistance Training Works at the Molecular Level
Mechanical stress on muscle fibers triggers mechanotransduction — the conversion of physical force into biochemical signals. This activates the mTORC1 pathway (the master regulator of protein synthesis), stimulates satellite cell proliferation, and improves neuromuscular coordination. In essence, PRT is the most potent pharmacological-equivalent stimulus available without a prescription.
Evidence-Based Resistance Training Protocol for Sarcopenia
Frequency: 2–3 sessions per week, non-consecutive days
Intensity 70–85% of 1-repetition maximum (1RM) for superior hypertrophy and strength
Volume 3–4 sets of 8–12 repetitions per exercise
Progression: Increase load by 5–10% when target reps are achieved with proper form
Exercise Selection: Multi-joint compound movements: squats, leg press, rows, chest press, overhead press
Rest Periods 60–120 seconds between sets
Expected Timeline: Strength gains: 4–8 weeks. Measurable mass gains: 12–16 weeks. Functional improvement: 6–8 weeks.
What About Lighter Weights?
A common clinical question is whether older adults can benefit from lighter resistance. The evidence is nuanced. Research consistently shows that high-intensity PRT (70–85% 1RM) is required for superior hypertrophic and strength outcomes. However, lower-intensity training (40–60% 1RM taken to near-failure) can also stimulate meaningful muscle protein synthesis and is a useful entry point for deconditioned patients, those with joint pain, or those in early rehabilitation settings. The key principle is progressive overload — the muscle must be challenged beyond its current capacity.
Aerobic Exercise: Necessary but Insufficient
Aerobic exercise improves cardiovascular health, endurance, and metabolic function, and should be included for overall health. However, it does not significantly increase muscle mass or strength. For sarcopenia management, it must be combined with resistance training, not used as a substitute. A well-rounded program includes 150 minutes per week of moderate aerobic activity alongside 2–3 resistance sessions.
Nutrition Strategies: Feeding the Anabolic Signal
Exercise provides the anabolic stimulus. Nutrition provides the raw materials. Without adequate protein and key micronutrients, even an optimally designed training program yields suboptimal results.
Protein Intake: How Much, What Kind, and When
The 2025 expert consensus published in the Geriatrics & Gerontology International (Kuzuya et al.) and the Journal of the Association of Physicians India (Kalra et al.) converge on clear recommendations for older adults:
✅ Protein Recommendation for Sarcopenia
1.2–1.5 g of protein per kg of body weight per day — significantly higher than the general adult RDA of 0.8 g/kg/day. For a 70 kg person, that is 84–105 g of protein daily. Patients with active resistance training, illness, or cachexia may need up to 1.6–2.0 g/kg/day.
The Per-Meal Threshold
Quantity alone is not enough. Distributing protein evenly across meals — with at least 25–30 grams of high-quality protein per meal — is essential to overcome anabolic resistance. A single high-protein dinner while breakfast and lunch remain protein-light is an ineffective strategy.
The Leucine Spark Plug
Among all amino acids, leucine acts as the metabolic trigger for mTOR activation. Without sufficient leucine, the muscle-building process may not initiate regardless of total protein intake. The expert consensus recommends:
2.5–3 g of leucine per meal as the minimum threshold for anabolic signaling
High-leucine foods: whey protein (~10–11% leucine), eggs, dairy, meat, fish, soy
Plant-based eaters may need higher total protein intake or leucine-enriched supplements to reach the threshold, as most plant proteins have lower leucine density
Protein Source Quality Comparison
Here is the same information broken down into clear, structured points to help you compare the protein sources quickly:
Whey Protein
Leucine: ~2.7 g
DIAAS Score: 1.09 (Excellent)
Sarcopenia Takeaway: Highly Recommended. It is the fastest-digesting protein available, making it incredibly effective at spiking muscle protein synthesis.
Eggs (Whole)
Leucine: ~2.1 g
DIAAS Score: 1.13 (Excellent)
Sarcopenia Takeaway: Highly Recommended. It ranks as one of the highest-quality whole foods available with exceptional biological value.
Chicken / Fish
Leucine: ~2.0–2.3 g
DIAAS Score: >1.0 (Excellent)
Sarcopenia Takeaway: Highly Recommended. A versatile, lean whole-food animal protein that easily fits into core lunch and dinner meals.
Dairy (Greek Yogurt)
Leucine: ~2.0 g
DIAAS Score: ~1.08 (Excellent)
Sarcopenia Takeaway: Highly Recommended. Contains casein, which digests more slowly to provide a sustained, steady release of amino acids.
Soy Protein
Leucine: ~1.9 g
DIAAS Score: 0.91 (Good)
Sarcopenia Takeaway: Good Plant Option. It is the highest-quality single plant source available, though you may need slightly larger portions than whey.
Peas / Legumes
Leucine: ~1.4–1.7 g
DIAAS Score: 0.6–0.8 (Moderate)
Sarcopenia Takeaway: Moderate Option. You will need to consume significantly larger portions to hit the necessary leucine threshold to trigger muscle growth.
Rice / Wheat
Leucine: ~0.9–1.2 g
DIAAS Score: <0.6 (Low)
Sarcopenia Takeaway: Poor Alone. Low in essential amino acids (like lysine). Must be paired intentionally with legumes to patch up the nutritional gaps.DIAAS = Digestible Indispensable Amino Acid Score; values are approximate and vary by preparation method.
Vitamin D: The Neuromuscular Wire
Vitamin D deficiency correlates strongly with sarcopenia risk, muscle weakness, and fall incidence. It plays a direct role in muscle fiber contraction speed and efficiency, and supports satellite cell function. Key points:
Optimal serum level: ≥30 ng/mL (75 nmol/L)
Deficiency threshold: <20 ng/mL — at this level, muscle performance is significantly compromised regardless of exercise effort
Supplementation: 1,000–2,000 IU/day of vitamin D3, or up to 4,000 IU/day in deficiency (discuss with your physician)
Test fasting 25-OH vitamin D blood levels before supplementing
Omega-3 Fatty Acids: Cooling the Inflammatory Fire
EPA and DHA (found in fatty fish like salmon, sardines, and mackerel, as well as fish oil supplements) exert anti-inflammatory effects that directly counter inflammaging. They may also enhance muscle protein synthesis and improve insulin sensitivity in muscle tissue. Recommended intake: 2–3 g combined EPA + DHA daily, ideally from dietary sources or high-quality fish oil.
Emerging Nutritional Agents
Creatine monohydrate: Growing evidence supports 3–5 g/day combined with resistance training for enhanced strength gains in older adults.
HMB (β-hydroxy β-methylbutyrate): A leucine metabolite that reduces muscle protein breakdown; 3 g/day may benefit those with very low activity levels or during hospitalization.
NAD⁺ precursors (NMN, NR): Early-phase evidence from Nguyen et al. (2026) suggests these may restore mitochondrial function in aging muscle, though large clinical trials are ongoing.
Emerging Pharmacological Therapies
No pharmaceutical agent is currently approved specifically for sarcopenia, but the pipeline is active. Liu et al.'s 2025 Clinical Nutrition review and Najm et al.'s 2024 International Journal of Molecular Sciences review provide the most current landscape.
⚠️ Important Disclaimer
All pharmacological agents discussed in this section are investigational or off-label. They should not be used outside of approved clinical trials or specialist supervision. They carry significant legal, ethical, and safety risks when used without medical oversight.
SARMs (e.g., Enobosarm)
Mechanism: Selectively activates androgen receptors specifically in muscle and bone tissue.
Status: Phase II/III clinical trials.
Key Findings: Demonstrates a 1 to 3 kg gain in lean mass over 12 to 24 weeks, while significantly reducing the typical androgenic side effects associated with traditional steroids.
Bimagrumab (Anti-ActRIIB)
Mechanism: Blocks the myostatin and activin pathways to remove the "brakes" on muscle growth.
Status: Phase II trials complete.
Key Findings: Produced a 3.6% increase in lean mass over 24 weeks, alongside a dual benefit of reduced fat mass.
Landogrozumab
Mechanism: An antibody designed to specifically target and inhibit anti-myostatin.
Status: Phase II trials ongoing.
Key Findings: Shows a favorable early safety profile; definitive efficacy data is still pending.
Anamorelin
Mechanism: Acts as a ghrelin receptor agonist to simultaneously stimulate appetite and anabolic pathways.
Status: Approved in Japan (specifically for cancer cachexia/muscle wasting).
Key Findings: Effectively improves lean body mass and appetite in patients suffering from cancer-associated sarcopenia.
ACE-031 / REGN1033
Mechanism: ActRIIB antagonists that block both myostatin and Growth Differentiation Factors (GDFs).
Status: Paused / Suspended.
Key Findings: Showed strong preclinical promise, but clinical development is currently suspended pending a resolution of safety concerns regarding off-target effects.
Testosterone Replacement Therapy (TRT)
Mechanism: Traditional androgen receptor agonist.
Status: Approved (strictly for confirmed hypogonadism).
Key Findings: Successfully increases lean mass in hypogonadal men, though cardiovascular and prostate risks require highly careful medical evaluation.
Senolytics (Dasatinib + Quercetin)
Mechanism: Clears age-related senescent "zombie" cells that secrete chronic inflammatory factors.
Status: Early clinical trials.
Key Findings: Highly promising preclinical data; the very first human clinical trials for sarcopenia applications are now underway.
SARMs: The Promise and the Problem
Selective androgen receptor modulators represent the most clinically advanced drug class for sarcopenia. Unlike anabolic steroids, they activate androgen receptors in muscle and bone tissue with high tissue selectivity, minimizing effects on the prostate, cardiovascular system, and endogenous hormone production. Phase II trials have consistently demonstrated meaningful lean mass gains. However, long-term safety data on prostate cancer risk, cardiovascular outcomes, and hormonal suppression are not yet available. Regulatory approval remains pending globally.
Myostatin Inhibitors: Removing the Growth Brake
Myostatin is a protein that naturally limits muscle mass — an evolutionary safeguard against energetically costly muscle growth. Blocking it pharmacologically allows for greater hypertrophy potential. Bimagrumab, the leading candidate, showed a 3.6% increase in lean mass over 24 weeks in Phase II trials, with an additional benefit of fat mass reduction. The challenge is dose calibration: complete myostatin blockade may have unintended metabolic consequences in the long term.
Regenerative Medicine & Gene Therapy
These approaches address the root cause of advanced sarcopenia — depleted regenerative capacity — rather than its symptoms. They represent the frontier of the field.
Stem Cell Therapies
Two primary approaches are under investigation:
Satellite cell therapies: Direct transplantation of expanded muscle-resident stem cells, or pharmacological activation of endogenous satellite cells via growth factors (IGF-1, HGF) and anti-inflammatory agents to restore the satellite cell niche.
Mesenchymal stem cell (MSC) therapy: Multipotent cells that can differentiate into muscle and secrete anti-inflammatory paracrine factors. Early clinical trials show improved muscle function and reduced systemic inflammatory markers.
Gene Therapy Approaches
Several gene-based strategies are being explored in preclinical and early clinical settings:
Overexpression of IGF-1 or follistatin (a natural myostatin inhibitor) in muscle tissue using viral vectors
Delivery of mitochondrial rescue genes to restore bioenergetic function
CRISPR-Cas9 editing of genes associated with accelerated muscle wasting (e.g., ACVR2B, MSTN)
Realistic Timeline
Regenerative and gene-based therapies remain largely experimental. They are not available outside of regulated clinical trials. Based on current development trajectories, limited clinical availability for specific indications is plausible within 5–10 years.
Microbiome Modulation: An Emerging Frontier
A growing body of evidence now links the gut microbiome to muscle health. The gut microbiome influences sarcopenia through short-chain fatty acid (SCFA) production (anti-inflammatory), amino acid metabolism, and immune system modulation. Nguyen et al. (2026) identify gut microbiota as a promising therapeutic target, with probiotic and prebiotic interventions under investigation as adjuncts to standard sarcopenia care.
Precision Medicine: The Future of Sarcopenia Care
Liu et al.'s 2025 Clinical Nutrition review champions a shift toward personalized, biomarker-guided sarcopenia management. This mirrors oncology's precision approach — where molecular profiling guides individualized treatment algorithms.
Biomarker-Guided Intervention Selection
Here is the biomarker profile information broken down into clear, structured points:
High CRP / IL-6
What It Signals: A dominant inflammaging phenotype (chronic, low-grade inflammation driven by aging).
Priority Intervention: Optimize Omega-3 intake, implement a strict anti-inflammatory diet, and consider potential senolytic therapies.
Low Testosterone / IGF-1
What It Signals: Hormonal insufficiency that directly drives an anabolic deficit (inability to build or maintain muscle).
Priority Intervention: Seek an endocrinology referral; implement hormone replacement therapy if true hypogonadism is clinically confirmed.
Low 25-OH Vitamin D (<20 ng/mL)
What It Signals: Impairment in neuromuscular signaling, which directly weakens muscle function and coordination.
Priority Intervention: Initiate aggressive Vitamin D3 correction as a baseline priority before deploying other interventions.
Elevated Myostatin / Low Follistatin
What It Signals: An overactive muscle growth "brake" system in the body that naturally limits muscle hypertrophy.
Priority Intervention: Prioritize progressive resistance training; consider experimental myostatin inhibitors if participating in a clinical trial setting.
Mitochondrial Dysfunction Markers
What It Signals: Bioenergetic failure, meaning the muscle cells are struggling to efficiently produce cellular energy.
Priority Intervention: Support with NAD⁺ precursors (such as NMN or NR) and Coenzyme Q10, combined with structured aerobic training.Phenotype Classification
Not all sarcopenia is the same. Treatment priorities differ by phenotype:
Sarcopenic obesity ("fat frailty"): Requires simultaneous fat loss and muscle gain — a delicate balance where caloric restriction must not exceed protein needs
Acute sarcopenia (hospitalisation-related): Requires urgent nutritional support and early mobility to prevent rapid accelerated loss during inactivity
Cancer-associated sarcopenia (cachexia): Ghrelin mimetics like anamorelin + anti-cachexia interventions + disease-directed therapy
Chronic disease-related sarcopenia (CKD, COPD, heart failure): Requires optimisation of the underlying disease as the primary target alongside muscle interventions
Practical Protocols: What to Do Starting Monday
The Comprehensive Sarcopenia Prevention Checklist
Begin resistance training 2–3x per week, progressing load every 1–2 weeks
Hit 25–30 g of high-quality protein at breakfast — not just dinner
Distribute total protein intake across 3–4 meals, not one large evening meal
Get a 25-OH vitamin D blood test; supplement if below 30 ng/mL
Include 2–3 servings of fatty fish per week or use a fish oil supplement (2+ g EPA+DHA/day)
Fill half your plate with colorful vegetables to dampen inflammaging
Walk 7,000–10,000 steps daily as aerobic base; this is not a substitute for resistance training
Screen for sarcopenia with SARC-F if over 60 or managing a chronic condition
Request grip strength and gait speed testing at your next clinical appointment
Manage comorbidities aggressively — uncontrolled diabetes, heart failure, or inflammation accelerates muscle loss
Consider creatine monohydrate (3–5 g/day) in combination with resistance training
Track progress every 3–6 months with functional measures (grip strength, timed sit-to-stand, walking speed)
Weekly Meal Protein Target (75 kg Adult)
🍽 Sample Protein Distribution — 90–110 g/day Target
Breakfast3 eggs + Greek yogurt (170g) + whey shake → ~35 g protein
Lunch150g chicken breast + legumes → ~35–40 g protein
SnackCottage cheese + handful of nuts → ~15 g protein
Dinner150g salmon or lean beef + vegetables → ~30–35 g protein
Daily Total~115–125 g ≈ 1.5 g/kg for a 75 kg person ✓
Common Myths & Mistakes in Sarcopenia Management
❌ Myth: Walking is enough to prevent muscle loss.
✅ Reality Walking preserves cardiovascular health but does not produce the mechanical overload needed to maintain muscle mass or reverse sarcopenia. Resistance training is essential.
❌ Myth: Older adults don't need as much protein as younger people.
✅ Reality: Older adults need more protein (1.2–1.5 g/kg/day) than young adults due to anabolic resistance. The standard RDA of 0.8 g/kg is inadequate for muscle preservation after 60.
❌ Myth: Sarcopenia is inevitable — there's nothing you can do.
✅ Reality: While some age-related decline is unavoidable, the rate and severity of sarcopenia are highly modifiable. Multiple interventions can significantly preserve, maintain, or partially restore muscle mass and strength.
❌ Myth: Light resistance exercise is ineffective — you have to lift heavy.
✅ Reality: While high-intensity training (70–85% 1RM) produces superior results, lower-intensity training taken to near-failure can also stimulate meaningful adaptations. Start where you can and progress gradually.
❌ Myth: Protein supplements are just for bodybuilders.
✅ Reality Protein supplements (whey, casein, plant-based) are practical, evidence-based tools for meeting the elevated protein requirements in older adults with poor appetite, dietary restrictions, or high protein needs.
❌ Myth: Sarcopenia only affects underweight or frail-looking people.
✅ Reality: "Sarcopenic obesity" — the simultaneous presence of excess fat and muscle loss — is increasingly common and more metabolically dangerous than either condition alone. Normal or high body weight does not rule out sarcopenia.
Frequently Asked Questions
At what age should I start worrying about sarcopenia?
Muscle mass begins declining around age 30, typically at 3–8% per decade. The rate accelerates significantly after age 60. However, the optimal time to intervene is before significant loss occurs — ideally in your 40s and 50s with established resistance training habits and adequate protein intake. If you are over 60 and experiencing unexplained weakness, difficulty climbing stairs, or frequent falls, see your physician promptly.
Can sarcopenia be reversed?
Early-stage sarcopenia is substantially reversible with intensive multimodal treatment. Advanced sarcopenia can be improved — with measurable gains in strength and function — though restoration to youthful baseline is unlikely. A 2025 review in Clinical Nutrition shows that personalized, combined interventions can restore functional independence in many cases. Early detection and consistent treatment produce the best outcomes.
How much protein do older adults actually need?
The 2025 Nutritional Management Guidelines for Sarcopenia (Kuzuya et al.) recommend 1.2–1.5 g of protein per kilogram of body weight daily for older adults — roughly 50–90% more than the standard adult RDA. For a 70 kg person, that is 84–105 g/day. Divide this evenly across 3–4 meals, aiming for 25–30 g per sitting to overcome anabolic resistance.
Is it safe for older adults with joint pain or osteoporosis to do resistance training?
Yes — with appropriate modifications and supervision. Resistance training is actually beneficial for bone density and is recommended alongside sarcopenia treatment. Begin with lower loads, focus on proper technique, and work with a physical therapist or certified exercise specialist. Machine-based exercises, water resistance training, and elastic bands reduce joint stress while still providing the anabolic stimulus needed.
What is the difference between sarcopenia and cachexia?
Both involve muscle loss, but cachexia is a complex metabolic syndrome defined by underlying illness (cancer, heart failure, COPD), systemic inflammation, anorexia, and involuntary weight loss. Sarcopenia is primarily age-related (or inactivity/malnutrition-driven) and does not necessarily involve overall weight loss. The conditions overlap significantly — cancer patients commonly have cachexia-driven sarcopenia — and treatment approaches share elements but must address the underlying disease in cachexia.
How do SARMs differ from anabolic steroids, and are they legal?
SARMs selectively activate androgen receptors in muscle and bone tissue, producing anabolic effects with significantly fewer androgenic side effects (e.g., prostate enlargement, cardiovascular stress) compared to anabolic steroids. However, SARMs are not approved for human use by the FDA or EMA for any indication, including sarcopenia. They are investigational compounds in clinical trials. Purchasing or using SARMs outside a clinical trial context is legally and medically risky.
Does testosterone replacement help with sarcopenia?
In men with confirmed hypogonadism (clinically low testosterone), testosterone replacement therapy (TRT) increases lean muscle mass and strength and is an appropriate medical intervention. It is not recommended for men with normal testosterone levels due to cardiovascular risks (erythrocytosis, thromboembolic risk) and potential prostate health concerns. Women with sarcopenia may benefit from low-dose testosterone in specific cases — discuss with an endocrinologist. TRT should always be part of a comprehensive management program, not used in isolation.
Are there specific foods that fight sarcopenia?
No single "superfood" cures sarcopenia, but a pattern of dietary choices strongly supports muscle health. Prioritize: leucine-rich proteins (eggs, dairy, meat, fish, whey), fatty fish rich in EPA/DHA omega-3s (salmon, sardines, mackerel), vitamin D-rich foods (fortified dairy, egg yolk, fatty fish), colorful vegetables and fruits for antioxidant and anti-inflammatory support, and creatine from red meat. Overall dietary quality — Mediterranean-style patterns combining these elements — consistently outperforms single-food interventions.
How long does it take to see results from sarcopenia treatment?
Strength improvements typically appear within 4–8 weeks of consistent resistance training. Measurable muscle mass gains require 12–16 weeks. Functional improvements such as faster gait speed and easier stair climbing usually manifest within 6–8 weeks. Nutritional optimization alone (without exercise) can reduce further loss but yields smaller gains. Consistency is the critical variable — intermittent effort produces minimal benefit.
Can gut health affect sarcopenia?
Yes — emerging evidence increasingly connects gut microbiome composition to muscle health. A healthy microbiome produces short-chain fatty acids with anti-inflammatory effects, influences amino acid bioavailability, and modulates immune function. Dysbiosis (microbiome imbalance) may amplify inflammaging and reduce the anabolic response to nutrition. Probiotic and prebiotic interventions are being studied as potential adjuncts, though this field is still in the early stages.
Clinical Pearls
1. Exercise is the "Volume Knob" for Your DNA
Science shows that resistance training (lifting weights or using bands) does more than just build bulk; it sends a signal to your genes to stay young.
The Pearl: When you challenge your muscles, you activate a pathway called mTOR. Think of this as the "master switch" for growth.
The Action: You don't need to be a bodybuilder, but you do need "progressive overload"—gradually increasing the weight or resistance so your muscles never get too comfortable.
2. Protein Needs a "Threshold" to Work
As we age, our muscles become "hard of hearing" when it comes to protein. This is called anabolic resistance. To get the muscle to listen, you have to hit a specific amount in one sitting.
The Pearl: Eating a little protein throughout the day isn't enough. You need about 25–30 grams of protein in a single meal to "trigger" muscle building.
The Action: Focus on your breakfast. Most people get enough protein at dinner, but very little in the morning. Adding eggs or Greek yogurt to your breakfast can flip the building switch earlier in the day.
3. Leucine is the "Spark Plug"
Not all proteins are created equal. One specific amino acid called Leucine acts like a spark plug that starts the muscle-building engine.
The Pearl: Even if you eat enough protein, if it is low in Leucine, the muscle-building process (synthesis) might not start.
The Action: Prioritise "high-quality" proteins like whey, dairy, eggs, or soy. If you are plant-based, you may need to eat slightly more or look for Leucine-enriched supplements to get that "spark."
4. Vitamin D is the "Communication Wire"
You can have the best engine in the world, but it won't run if the wiring is faulty. Vitamin D acts as a bridge between your nerves and your muscles.
The Pearl: Low Vitamin D is directly linked to muscle weakness and a higher risk of falling. It helps your muscles contract faster and more efficiently.
The Action: Ask your doctor for a blood test. If you are below 30 ng/mL, your muscles are likely struggling to perform, regardless of how much you exercise.
5. "Inflammaging" is the Silent Muscle Thief
Chronic, low-grade inflammation (often called "inflammaging") acts like rust on your muscle fibers, breaking them down faster than you can repair them.
The Pearl: High levels of inflammatory markers (like CRP or IL-6) act as a signal for the body to "recycle" muscle tissue for energy.
The Action: Combat this "rust" with Omega-3 fatty acids (found in fish oil) and a diet rich in colorful vegetables. These help "cool down" the system so your exercise efforts actually stick.
Conclusion: Your Muscle Health Action Plan
Sarcopenia is not a sentence — it is a signal. And like all biological signals, it responds to the right intervention. The science of 2025–2026 has made one thing abundantly clear: the combination of progressive resistance training, optimized protein intake, targeted micronutrient correction, and management of underlying conditions is more powerful than any single drug, supplement, or therapy yet developed.
Your key action steps:
Start resistance training this week — 2 sessions is sufficient to begin
Add protein to your breakfast immediately; this single shift creates the most impact for most people
Get your vitamin D and grip strength measured at your next medical appointment
If you are over 60 or managing a chronic disease, ask your physician about formal sarcopenia screening using the SARC-F questionnaire
Be consistent — muscle health is built in months and years, not days
If you are a clinician: screen routinely, prescribe specifically, and monitor objectively. Sarcopenia is now an ICD-coded disease with effective, evidence-based treatments. Treating it with the same rigor as diabetes or hypertension saves independence, reduces hospitalizations, and extends healthy years.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Emerging therapies discussed — including SARMs, myostatin inhibitors, gene therapy, and stem cell interventions — are investigational and not approved for routine clinical use. They carry significant medical, ethical, and legal risks when used outside approved research settings. Individual circumstances vary; all treatment decisions should be made in consultation with qualified healthcare professionals. Always consult your physician before starting a new exercise program, supplement, or medication.
Related Articles
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
Sarcopenia in Diabetes: Managing Muscle Loss with Chronic Disease | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
Best Exercises for Sarcopenia: Strength Training Guide for Older Adults | DR T S DIDWAL
Best Supplements for Sarcopenia: Vitamin D, Creatine, and HMB Explained | DR T S DIDWAL
References & Sources
Bauer, J., Morley, J. E., Schols, A. M. W. J., Ferrucci, L., Cruz-Jentoft, A. J., Dent, E., Baracos, V. E., Crawford, J. A., Doehner, W., Heymsfield, S. B., Anker, S. D., Coates, P. M., Fielding, R. A., Guenette, J., Landi, F., Lane, N. E., von Haehling, S., & Muscaritoli, M. (2019). Sarcopenia: A time for action. An SCWD position paper. Journal of Cachexia, Sarcopenia and Muscle, 10(5), 956–961. https://doi.org/10.1002/jcsm.12483
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., Cooper, C., Landi, F., Rolland, Y., Sayer, A. A., Schneider, S. M., Sieber, C. C., Topinkova, E., Vandewoude, M., Visser, M., Zamboni, M., & Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Dent, E., Morley, J. E., Cruz-Jentoft, A. J., Woodhouse, L., Rodríguez-Mañas, L., Fried, L. P., Woo, J., Aprahamian, I., Sanford, A., Lundy, J., Landi, F., Beilby, J., Martin, F. C., Merchant, R. A., Fielding, R. A., Hoogendijk, E. O., Won, C. W., Abbatecola, A., Cederholm, T., ... Vellas, B. (2018). International clinical practice guidelines for sarcopenia (ICFSR): Screening, diagnosis and management. The Journal of Nutrition, Health & Aging, 22(10), 1148–1161. https://doi.org/10.1007/s12603-018-1139-9
Frontera, W. R., & Ochala, J. (2015). Skeletal muscle: A brief review of structure and function. Calcified Tissue International, 96(3), 183–195. https://doi.org/10.1007/s00223-014-9915-y
Kalra, S., Das, A., Kotwal, N., Baruah, M. P., Sahay, R., Tiwaskar, M., Saboo, B., Chadha, M., Bantwal, G., Chawla, R., & Agrawal, N. (2025). Expert opinion on management advancements in sarcopenia: From muscle wasting to recovery. Journal of Association of Physicians of India, 73(6), 50–60.
Kuzuya, M., Kanno, Y., Arai, H., Akishita, M., Kozaki, K., Kojima, T., Satake, S., Shamoto, H., Takahashi, T., Tokuda, H., Maeda, K., Wakabayashi, H., Makizako, H., Shimada, H., Umegaki, H., & Rakugi, H. (2025). Nutritional management guidelines for sarcopenia and frailty 2025. Geriatrics & Gerontology International, 25(1), 5–53. https://doi.org/10.1111/ggi.70275
Liu, X., Chen, X., & Cui, J. (2025). Therapeutic advances in sarcopenia management: From traditional interventions to personalized medicine. Clinical Nutrition, 51, 187–197.
Lo, J. H., U, K. P., Yiu, T., Ong, M. T., & Lee, W. Y. (2020). Sarcopenia: Current treatments and new regenerative therapeutic approaches. Journal of Orthopaedic Translation, 23, 38–52. https://doi.org/10.1016/j.jot.2020.04.002
Mao, X., Lv, K., Qi, W., Wang, Y., Zhang, L., Liu, H., & Zhou, Y. (2025). Research progress on sarcopenia in the musculoskeletal system. Bone Research, 13, Article 78. https://doi.org/10.1038/s41413-025-00455-8
Moore, D. R., Churchward-Venne, T. A., Witard, O., Breen, L., Burd, N. A., Tipton, K. D., & Phillips, S. M. (2015). Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. Journals of Gerontology: Series A, 70(1), 57–62. https://doi.org/10.1093/gerona/glu103
Najm, A., Niculescu, A. G., Grumezescu, A. M., & Beuran, M. (2024). Emerging therapeutic strategies in sarcopenia: An updated review on pathogenesis and treatment advances. International Journal of Molecular Sciences, 25(8), Article 4300. https://doi.org/10.3390/ijms25084300
Nguyen, T. T., Dao, T., Nguyen, H. T., Le, Q. G., Kim, J. H., & Park, S. W. (2026). Sarcopenia and muscle aging: Updated insights into molecular mechanisms and translational therapeutics. Endocrinology and Metabolism, 41(1), 57–85. https://doi.org/10.3803/EnM.2025.2656
Papadopoulou, S. K. (2020). Sarcopenia: A contemporary health problem among older adult populations. Nutrients, 12(5), Article 1293. https://doi.org/10.3390/nu12051293
Tan, L. F., Koh, F. H., Lim, W. S., Chew, J., Tay, L., Merchant, R. A., Ng, T. P., & Wee, S. L. (2026). Sarcopenia: Current evidence, advances in assessment, clinical implementation and future directions. Annals of the Academy of Medicine, Singapore, 55(1), 26–37. https://doi.org/10.47102/annals-acadmedsg.2025287
Zheng, Y., Feng, J., Yu, Y., Wang, X., & Zhang, J. (2024). Advances in sarcopenia: Mechanisms, therapeutic targets, and intervention strategies. Archives of Pharmacological Research, 47, 301–324. https://doi.org/10.1007/s12263-024-00712-w