The Vitamin D–K2 Axis: A Precision Strategy for Bone, Muscle, and Vascular Integrity
Explore the science behind the Vitamin D–K2 axis and how this synergistic pathway supports bone density, muscle strength, and vascular health.
NUTRITIONHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
3/6/202615 min read
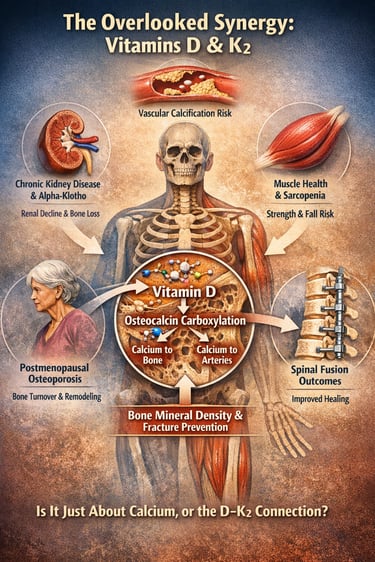
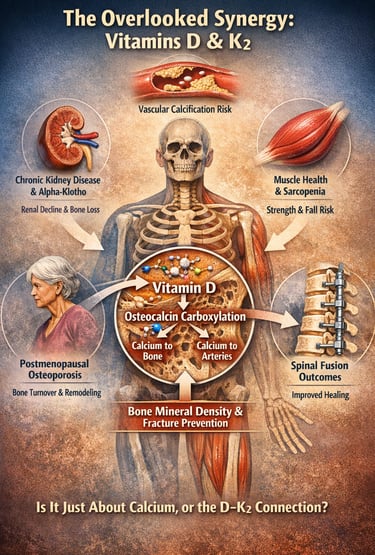
The Overlooked Synergy in Calcium Metabolism and Bone Health
What if the real problem in osteoporosis, sarcopenia, and even vascular calcification is not simply calcium deficiency — but a breakdown in how calcium is regulated, activated, and directed within the body?
For decades, Vitamin D has been prescribed almost reflexively to improve bone mineral density and reduce fracture risk. Yet emerging research suggests that Vitamin D alone may represent only half of the physiological equation. Calcium metabolism is not merely about absorption — it is about precision targeting. While Vitamin D enhances intestinal calcium uptake and increases circulating calcium levels, it is Vitamin K2 that activates osteocalcin through carboxylation, enabling calcium to bind effectively to hydroxyapatite in the bone matrix (Khandelwal et al., 2025). Without sufficient Vitamin K2, undercarboxylated osteocalcin accumulates, potentially allowing calcium to deposit in soft tissues rather than strengthening skeletal structure.
This mechanistic synergy has implications far beyond traditional osteoporosis management. In postmenopausal osteoporosis, Vitamin K2 supplementation significantly improves bone turnover markers and shifts remodeling toward formation (Zhang et al., 2025b). In chronic kidney disease, declining alpha-klotho levels impair Vitamin D metabolism and accelerate bone loss, linking renal physiology directly to skeletal fragility (Zhang et al., 2025a). Even in orthopedic surgery, combined Vitamin D3 and K2 supplementation has demonstrated improved spinal fusion outcomes and reduced implant subsidence in osteoporotic patients (Wang et al., 2025).
Meanwhile, Vitamin D’s role extends into skeletal muscle, where vitamin D receptor activation influences protein synthesis, mitochondrial function, and fall risk reduction — key factors in preventing osteosarcopenia (Kuwabara et al., 2024).
The emerging message is clear: optimizing bone, muscle, and metabolic health may require rethinking Vitamin D as a standalone intervention — and embracing a more integrated D–K axis model.
Distilling the synergistic relationship between Vitamin D and K2 into "clinical pearls" requires balancing the complex biochemistry for providers with the practical, "so what?" outcomes for patients.
Clinical pearls
1. The "Traffic Cop" Mechanism
Scientific Perspective: Vitamin D upregulates the synthesis of osteocalcin, but Vitamin K2 is the essential cofactor for its carboxylation. Only carboxylated osteocalcin has the high affinity for hydroxyapatite required to bind calcium to the bone matrix.
Think of Vitamin D as the loader that puts calcium into your "delivery truck" (the bloodstream). Without Vitamin K2, the truck doesn't have a GPS—the calcium might end up "parked" in your arteries (causing stiffness) instead of your bones.
2. Guarding the "Longevity Protein" (Alpha-Klotho)
Scientific Perspective: In Chronic Kidney Disease (CKD), the decline of the Alpha-Klotho protein disrupts FGF23 signaling and Vitamin D metabolism. Higher serum Alpha-Klotho is a positive predictor of Bone Mineral Density (BMD), regardless of the CKD stage.
For those with kidney concerns, bone health isn't just about calcium; it's about protecting a specific protein (Alpha-Klotho) that keeps your bones and kidneys "communicating." Monitoring this can help predict and prevent bone loss early.
3. Shifting the Bone Balance (The Anabolic Switch)
Scientific Perspective: Meta-analyses show Vitamin K2 (specifically MK-7) significantly reduces the ratio of undercarboxylated osteocalcin This shifts the biochemical environment from bone resorption (loss) toward bone formation (gain).
Menopause often acts like a "drain" on bone density. Adding K2 helps "plug the drain" by making sure your body’s bone-building cells are actually active and effective, rather than just floating around.
4. The "Internal Splint" for Surgery
Scientific Perspective: Combined D3 and K2 therapy improves endoscopic spinal fusion rates. The synergy creates a superior anabolic environment that prevents "cage subsidence" (the implant sinking into soft bone) and promotes faster mineral bridge formation.
If you are undergoing back surgery, your bones are the foundation for the hardware. Supplementing with both vitamins acts like an "internal splint," helping your bone grow into the implants faster and more securely.
5. Muscle Fiber "Quality Control"
Scientific Perspective: Vitamin D receptors (VDR) in skeletal muscle modulate mitochondrial function and protein synthesis. Correcting deficiency (aiming for 30–40 ng/mL) is critical for maintaining Type II (fast-twitch) muscle fibers, which are the first to atrophy in aging.
Strong bones are useless if you fall. Vitamin D helps your muscles "fire" faster and stay strong, which improves your balance and prevents the falls that lead to fractures in the first place.
6. Bioavailability Matters (MK-7 vs. MK-4)
Scientific Perspective: Vitamin K2 as MK-7 has a much longer half-life (approx. 72 hours) compared to MK-4 (approx. 1–2 hours). This leads to more stable serum levels and better extra-hepatic (bone and vascular) tissue distribution with once-daily dosing.
Not all Vitamin K is created equal. When looking at labels, "MK-7" is the gold standard because it stays in your system longer, meaning you only need to take it once a day to get the 24-hour bone-protecting benefits.
Part I: Understanding the Synergy — What the Science Says
Vitamins D and K: Biochemically Inseparable
At the molecular level, the connection between Vitamins D and K is not coincidental — it is mechanistic. Khandelwal, Ahmed, and Dikshit (2025), writing in the Journal of Mid-life Health, provide perhaps the most comprehensive recent overview of this biochemical synergy. Their review establishes that Vitamin D is primarily responsible for upregulating calcium absorption from the gut and facilitating its transport into the bloodstream. However, without adequate Vitamin K — specifically Vitamin K2 (menaquinone) — that calcium has no reliable mechanism to reach the bone matrix where it is needed most.
The critical intermediary here is a protein called osteocalcin, synthesized by osteoblasts (bone-forming cells) but dependent on Vitamin K2 for its carboxylation. In its carboxylated form, osteocalcin has a high affinity for hydroxyapatite, the mineral compound that gives bone its rigidity. Without sufficient Vitamin K2, osteocalcin remains undercarboxylated — circulating and non-functional — and calcium may instead deposit in arterial walls, a process associated with cardiovascular risk.
This creates a compelling paradox: high-dose Vitamin D supplementation without concurrent Vitamin K2 may inadvertently increase calcium loading in soft tissues. Khandelwal et al. (2025) highlight that this interaction has significant implications for midlife adults, particularly postmenopausal women and aging men whose bone turnover accelerates and whose dietary intake of both vitamins tends to decline simultaneously. The authors argue that combined supplementation protocols are not only rational but may be essential for populations at risk of osteoporosis, arterial calcification, and metabolic decline.
Key Takeaway: Vitamin D drives calcium absorption; Vitamin K2 directs that calcium into bone rather than arteries. The two vitamins must work in concert for optimal skeletal and cardiovascular protection.
Part II: Bone Mineral Density and the Kidney Connection
Alpha-Klotho, Chronic Kidney Disease, and Bone Loss
One of the most intriguing findings in recent bone health research comes from a large-scale analysis of NHANES (National Health and Nutrition Examination Survey) data conducted by Zhang, Qi, Luo, et al. (2025) and published in Scientific Reports. Their study examined serum alpha-klotho levels — a longevity-associated protein produced primarily in the kidneys — and their relationship with bone mineral density (BMD) in patients with chronic kidney disease (CKD).
Alpha-klotho is a protein with wide-ranging anti-aging and organ-protective properties. It acts as a co-receptor for fibroblast growth factor 23 (FGF23), a hormone that regulates phosphate metabolism and Vitamin D activation. In CKD, alpha-klotho levels decline sharply, contributing to impaired Vitamin D metabolism, dysregulated calcium-phosphorus balance, and accelerated bone loss — a condition known as renal osteodystrophy.
Analyzing data from 2011 to 2016, Zhang et al. (2025) found a statistically significant positive association between serum alpha-klotho levels and BMD across multiple skeletal sites in CKD patients. Higher alpha-klotho levels were associated with better bone density, even after adjusting for age, sex, body mass index, and kidney function. Importantly, this relationship persisted across different stages of CKD, suggesting that alpha-klotho serves as both a biomarker and a potential therapeutic target.
The clinical implication is profound: in patients where Vitamin D metabolism is already compromised by kidney disease, supporting the alpha-klotho pathway may amplify the skeletal benefits of any supplementation strategy — including combined Vitamin D and K2 protocols.
Key Takeaway: In chronic kidney disease, alpha-klotho decline disrupts Vitamin D metabolism and accelerates bone loss. Higher serum alpha-klotho is associated with better bone mineral density, making it a valuable biomarker and target in CKD-related osteoporosis management.
Part III: Vitamin K2 and Postmenopausal Bone Health
What the Meta-Analysis Tells Us About Bone Turnover
Among the populations most vulnerable to osteoporosis-related fractures are postmenopausal women, for whom the decline in estrogen sharply increases the rate of bone resorption. A 2025 systematic review and meta-analysis by Zhang, Li, Li, Yuan, Liu, and Shi, published in Frontiers in Endocrinology, provides the most rigorous current synthesis of evidence on Vitamin K2 supplementation and bone turnover biochemical markers in this population.
The meta-analysis pooled data from multiple randomized controlled trials and evaluated the effect of Vitamin K2 (primarily in the form of menaquinone-7, or MK-7) on markers of bone formation and resorption. The key markers examined included osteocalcin (a marker of bone formation), undercarboxylated osteocalcin (ucOC, a functional indicator of Vitamin K2 status), and N-terminal telopeptide (NTX), a marker of bone resorption.
The findings were clinically meaningful. Vitamin K2 supplementation significantly increased the ratio of carboxylated to undercarboxylated osteocalcin, indicating improved bone-forming activity. It also showed a trend toward reducing markers of bone resorption, suggesting a net anabolic effect on the skeleton. Importantly, these effects were observed independent of concurrent calcium or Vitamin D supplementation in some trials, though the authors noted that the magnitude of benefit was likely enhanced when Vitamin K2 was combined with Vitamin D — consistent with the mechanistic synergy described by Khandelwal et al. (2025).
The authors conclude that Vitamin K2 supplementation represents a clinically viable, well-tolerated adjunct to standard osteoporosis management in postmenopausal women, with biochemical evidence supporting its role in shifting the bone turnover balance toward formation over resorption.
Key Takeaway: Vitamin K2 supplementation in postmenopausal women significantly improves carboxylated osteocalcin ratios and favourably shifts bone turnover markers toward formation over resorption — supporting its role as a meaningful adjunct in osteoporosis management.
Part IV: Vitamin D and Skeletal Muscle Health
Beyond Bone — The Muscular Case for Vitamin D
While most discussions of Vitamin D focus on calcium metabolism and bone density, a growing body of literature highlights its equally important role in skeletal muscle function. A 2024 review by Kuwabara, Matsumoto, Hatamoto, and Fujita, published in Current Opinion in Clinical Nutrition and Metabolic Care, synthesizes the most recent evidence on how Vitamin D influences muscle physiology.
Vitamin D receptors (VDR) are expressed in skeletal muscle cells, and Vitamin D modulates gene expression related to protein synthesis, calcium handling within myocytes, and mitochondrial function. The clinical consequences of Vitamin D deficiency in muscle tissue include reduced grip strength, impaired balance, increased fall risk, and sarcopenia — the age-related loss of muscle mass and function that dramatically increases fracture risk in older adults.
Kuwabara et al. (2024) review intervention studies demonstrating that Vitamin D supplementation — particularly when correcting deficiency — improves muscle strength, physical performance, and reduces fall incidence in older populations. The review also highlights that the threshold for adequate Vitamin D levels relevant to muscle health may be higher than the minimum required to prevent rickets, with some evidence suggesting that optimal muscle function may require serum 25-hydroxyvitamin D levels of at least 30–40 ng/mL.
The authors further explore the interaction between Vitamin D and insulin-like growth factor 1 (IGF-1), a key anabolic hormone in muscle tissue, and the potential role of Vitamin D in attenuating muscle inflammation — both of which carry significant implications for rehabilitation, athletic performance, and healthy aging.
This muscle-health dimension adds yet another layer to the rationale for ensuring adequate Vitamin D status, particularly in older adults who are simultaneously at risk for both osteoporosis and sarcopenia — a clinical syndrome sometimes called osteosarcopenia.
Key Takeaway: Vitamin D acts directly on skeletal muscle via its nuclear receptor, supporting protein synthesis, calcium handling, and mitochondrial function. Correcting deficiency in older adults demonstrably improves muscle strength and reduces fall and fracture risk — making Vitamin D optimization central to healthy aging.
Part V: Clinical Proof of Concept — Spinal Fusion Outcomes
When D and K2 Work Together in Surgical Settings
Perhaps the most compelling clinical evidence for combined Vitamin D and K2 supplementation comes from a 2025 prospective study by Wang, Wang, Wang, et al., published in Scientific Reports. The study examined the effect of combined Vitamin K2 and D3 therapy on endoscopic fusion outcomes in patients with osteoporotic lumbar degenerative disease — a population for whom poor bone quality dramatically complicates surgical success.
Lumbar spinal fusion in osteoporotic patients is notoriously challenging. Pedicle screws and interbody cages require adequate bone density for proper anchoring and healing; in osteoporotic bone, hardware failure, cage subsidence (sinking of the implant), and nonunion are common complications. The study by Wang et al. (2025) enrolled patients with osteoporotic lumbar degenerative disease who underwent endoscopic spinal fusion, randomizing them to receive combined Vitamin K2 and D3 supplementation versus standard of care.
The results were striking. Patients receiving combined K2 and D3 supplementation demonstrated significantly improved endoscopic fusion rates, reduced cage subsidence, and better clinical outcomes at follow-up compared to controls. Bone mineral density at the lumbar spine showed greater improvement in the supplemented group, and markers of bone turnover were more favorably modulated. The authors propose that the synergistic action of D3 (enhancing calcium availability and osteoblast activity) and K2 (improving osteocalcin carboxylation and directing mineral to the bone matrix) creates an anabolic environment conducive to accelerated and more complete fusion.
This study moves the conversation from basic science and population epidemiology into direct clinical application — demonstrating that combined supplementation produces measurable, patient-centered improvements in one of the most demanding clinical scenarios for bone health.
Key Takeaway: Combined Vitamin K2 and D3 supplementation significantly improved spinal fusion rates, reduced implant subsidence, and enhanced bone mineral density recovery in osteoporotic patients undergoing lumbar surgery — providing powerful clinical validation of the D-K2 synergy hypothesis.
Part VI: Connecting the Dots — An Integrated Model
The Vitamin D–K2 Axis: A Precision Model for Bone, Muscle, and Renal Health
Calcium Is Not the Problem — Calcium Misplacement Is.
Modern bone discourse has overemphasized calcium intake while underexamining calcium regulation. Vitamin D increases intestinal calcium absorption, but without adequate Vitamin K2–mediated osteocalcin carboxylation, that calcium lacks precise skeletal targeting. The issue is not deficiency alone — it is biological directionality.Vitamin D Is a Hormone, Not Just a Vitamin.
Through vitamin D receptor (VDR) activation, it regulates gene transcription in osteoblasts, skeletal muscle fibers, and immune cells. Its influence spans bone mineral density, mitochondrial function, and fall risk. Yet its anabolic skeletal effects require downstream protein activation — a step dependent on Vitamin K2.Vitamin K2 Is the Biochemical Gatekeeper.
Menaquinone-7 (MK-7) activates osteocalcin and matrix Gla protein, enabling calcium binding to hydroxyapatite while potentially limiting vascular deposition. Without sufficient K2, undercarboxylated osteocalcin circulates functionally inert — a molecular inefficiency with systemic consequences.The Kidney–Bone Axis Cannot Be Ignored.
In chronic kidney disease, declining alpha-klotho impairs Vitamin D activation and disrupts phosphate homeostasis. The resulting skeletal fragility reflects endocrine cross-talk failure. Any serious discussion of osteoporosis must now include renal physiology.Postmenopausal Osteoporosis Is a Remodeling Crisis.
Estrogen decline accelerates bone resorption. Emerging meta-analytic data suggest Vitamin K2 shifts turnover markers toward formation, especially when paired with adequate Vitamin D. This represents modulation of remodeling dynamics rather than simple mineral supplementation.Muscle Is Part of the Fracture Equation.
Sarcopenia increases fall risk — the proximal cause of many fragility fractures. Vitamin D sufficiency improves muscle strength and neuromuscular coordination, integrating bone and muscle into a single functional unit: osteosarcopenia.Surgical Evidence Strengthens the Case.
Prospective spinal fusion data demonstrate improved fusion rates and reduced implant subsidence with combined D3 and K2 therapy in osteoporotic patients. This is translational proof that biochemical synergy yields structural outcomes.Clinical Implication: Move From Supplementation to Strategy.
Vitamin D alone is incomplete. Vitamin K2 alone is insufficient. Together, they represent a coordinated endocrine–nutritional axis.The Future Is Precision Micronutrition.
As longevity medicine evolves, the D–K2 partnership may redefine foundational care in bone, muscle, and metabolic health — not as alternative therapy, but as physiological optimization grounded in mechanistic science.
Part VII: Practical Considerations for Supplementation
What Doses, What Forms, and Who Should Consider Combined Therapy?
While personalized medical advice requires individual clinical assessment, the literature supports several general principles:
Vitamin D3 (cholecalciferol) is the preferred supplemental form, as it more effectively raises serum 25-hydroxyvitamin D levels than D2 (ergocalciferol). Dosing typically ranges from 1,000–4,000 IU daily for maintenance, with higher doses under medical supervision for correction of deficiency.
Vitamin K2 as MK-7 (menaquinone-7) has superior bioavailability and a longer half-life compared to MK-4, making once-daily dosing practical. Evidence supporting bone and vascular benefits typically involves doses in the range of 90–360 micrograms daily.
Individuals most likely to benefit from combined supplementation include postmenopausal women with reduced BMD, older adults with sarcopenia or fall risk, patients with CKD and evidence of bone disease, individuals on long-term anticoagulant therapy (though K2 use should be discussed with a physician in these cases), and those with documented deficiency in either vitamin.
Key Dietary Sources of Vitamin K2
Natto (fermented soybeans) – the richest known source, especially high in menaquinone-7 (MK-7).
Hard and aged cheeses (Gouda, Edam, Jarlsberg) – good sources of MK-8 and MK-9.
Egg yolks – contain small amounts of MK-4.
Butter and full-fat dairy from grass-fed animals – moderate K2 content.
Chicken and goose liver – provide MK-4, a short-chain form of K2.
Fermented foods such as sauerkraut and kefir – smaller but useful amounts.
Frequently Asked Questions (FAQs)
Q1. Can I take Vitamin D and Vitamin K2 together, or will they interfere with each other?
Not only can you take them together — the evidence suggests you probably should. Vitamins D and K2 work synergistically rather than competitively. Vitamin D enhances calcium absorption, while K2 ensures that calcium is directed to the bone matrix through osteocalcin carboxylation rather than depositing in soft tissues. There is no known pharmacological antagonism between the two vitamins, and combined formulations are widely available and supported by the literature reviewed in this article (Khandelwal et al., 2025; Wang et al., 2025).
Q2. I have been told I have low Vitamin D. Should I also be checked for Vitamin K2 status?
This is a clinically important question. While routine serum Vitamin K2 testing is not universally standardized, a functional proxy — the ratio of undercarboxylated to carboxylated osteocalcin — provides a reliable indicator of K2 status. Individuals with low Vitamin D are frequently also inadequate in K2, particularly older adults, those with limited dietary variety, and people who avoid fermented foods (a primary dietary source of MK-7). If your clinician is managing Vitamin D deficiency, it is reasonable to discuss Vitamin K2 status as well.
Q3. Does Vitamin D supplementation alone put me at risk for arterial calcification?
The concern is theoretically valid. Vitamin D increases intestinal calcium absorption, and without sufficient Vitamin K2 to carboxylate osteocalcin, that calcium may not be effectively incorporated into bone. Some observational data suggest that high-dose Vitamin D without adequate K2 may be associated with increased vascular calcification risk, though causality remains under active investigation. The prudent approach, supported by the mechanistic rationale outlined by Khandelwal et al. (2025), is to ensure adequate K2 status when undertaking Vitamin D supplementation — particularly at higher doses.
Q4. I have chronic kidney disease. What does the research say about bone health for me specifically?
CKD fundamentally impairs Vitamin D metabolism because the kidney is responsible for converting 25-hydroxyvitamin D into its active form, 1,25-dihydroxyvitamin D (calcitriol). Zhang et al. (2025) found that alpha-klotho — a protein whose production declines with kidney disease — is significantly associated with bone mineral density in CKD patients. This means that CKD patients face a compounded skeletal risk: impaired Vitamin D activation, reduced alpha-klotho, and dysregulated mineral metabolism. Management of bone health in CKD should be individualized and guided by a nephrologist, but awareness of the D-K2 interplay and alpha-klotho biomarker is increasingly relevant to this population.
Q5. Is Vitamin K2 safe for people on blood thinners like warfarin?
This requires individual medical evaluation. Warfarin works by inhibiting Vitamin K-dependent clotting factor carboxylation, and Vitamin K supplementation can indeed alter warfarin's anticoagulant effect. However, it is important to note that Vitamin K2 (particularly MK-7) at low, consistent doses may actually stabilize INR (the measure of anticoagulant effect) in some patients rather than simply antagonizing warfarin. Nevertheless, any changes to Vitamin K intake in individuals on warfarin should be discussed with a prescribing physician and monitored accordingly. This is not an area for self-management.
Q6. As a postmenopausal woman, which form of Vitamin K2 is best for bone health?
The meta-analysis by Zhang et al. (2025) and the broader literature most consistently support Vitamin K2 in the form of menaquinone-7 (MK-7) for bone health applications. MK-7 has a biological half-life of approximately 72 hours, allowing for stable once-daily supplementation and more consistent tissue levels compared to MK-4, which is cleared from the bloodstream more rapidly. Doses of MK-7 used in clinical trials for bone outcomes typically range from 90 to 200 micrograms daily. As with any supplement, quality sourcing and combined use with adequate Vitamin D3 and calcium (where appropriate) is advisable.
Q7. Can Vitamin D and K2 supplementation replace my osteoporosis medication?
No — and this distinction is important. Vitamins D and K2 are supportive nutritional interventions with meaningful evidence for improving bone turnover markers, enhancing bone mineral density, and reducing fracture risk when used appropriately. However, they do not replicate the mechanism of action of pharmacological agents such as bisphosphonates, denosumab, or teriparatide, which are the evidence-based standard of care for established osteoporosis with high fracture risk. Vitamins D and K2 are best understood as foundational nutritional support — optimizing the substrate and cellular environment for bone health — rather than as standalone treatments for diagnosed osteoporosis. Discuss any supplementation strategy with your healthcare provider before altering your treatment plan.
Author’s Note
As a clinician trained in internal medicine and deeply engaged in metabolic and musculoskeletal research, I have long been struck by how often Vitamin D is prescribed in isolation — almost reflexively — while the broader physiology of calcium regulation receives far less attention. The emerging literature on the Vitamin D–K2 partnership challenges that reductionist approach. It compels us to think beyond nutrient replacement and toward coordinated biological systems.
This article was written not to promote supplementation indiscriminately, but to encourage a more mechanistic understanding of bone, muscle, and renal health. The interaction between Vitamin D, Vitamin K2, osteocalcin carboxylation, alpha-klotho signaling, and skeletal remodeling represents a convergence of endocrinology, nephrology, and geriatric medicine. In my view, this convergence is precisely where modern preventive medicine must focus — at the level of molecular orchestration rather than isolated biomarkers.
Importantly, the evidence continues to evolve. While the mechanistic rationale for combined Vitamin D and K2 optimization is compelling, clinical decisions must remain individualized. Patients with chronic kidney disease, those on anticoagulant therapy, individuals with established osteoporosis, or those undergoing orthopedic surgery require tailored evaluation and specialist guidance. Nutritional interventions should complement — not replace — evidence-based pharmacotherapy when indicated.
My goal in synthesizing this material is to bridge scientific rigor with clinical practicality. As our understanding of osteosarcopenia, vascular calcification, and metabolic aging deepens, it becomes increasingly clear that micronutrients operate within interconnected biological networks. Recognizing and respecting those networks is not alternative medicine — it is physiology.
I hope this discussion contributes to a more integrated and thoughtful approach to bone and metabolic health across the lifespan. lifespan.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Can Omega-3 Boost Muscle Protein Synthesis? What the Latest Research Reveals | DR T S DIDWAL
Beyond the Low-Fat Myth: 6 New Studies Redefining Dietary Fat and Heart Health | DR T S DIDWAL
Can Plant-Based Polyphenols Lower Biological Age? | DR T S DIDWAL
References
Khandelwal, A., Ahmed, K. A., & Dikshit, P. (2025). Vitamin D and Vitamin K: Synergistic roles and emerging evidence for combined supplementation. Journal of Mid-life Health, 16(4), 505–508. https://doi.org/10.4103/jmh.jmh_169_25
Kuwabara, A., Matsumoto, M., Hatamoto, Y., & Fujita, S. (2024). Vitamin D and muscle health: Insights from recent studies. Current Opinion in Clinical Nutrition and Metabolic Care, 27(6), 499–506. https://doi.org/10.1097/MCO.0000000000001071
Wang, Y., Wang, Y., Wang, F., et al. (2025). Combined vitamin K2 and D3 therapy improves endoscopic fusion outcomes in osteoporotic lumbar degenerative disease: A prospective study. Scientific Reports, 15, 15422. https://doi.org/10.1038/s41598-025-99922-9
Zhang, Y., Qi, R., Luo, X., et al. (2025). Serum alpha-klotho levels associate with bone mineral density in chronic kidney disease patients from NHANES 2011 to 2016. Scientific Reports, 15, 18760. https://doi.org/10.1038/s41598-025-04024-1
Zhang, Z., Li, Y., Li, J., Yuan, Y., Liu, K., & Shi, X. (2025). The effect of vitamin K2 supplementation on bone turnover biochemical markers in postmenopausal osteoporosis patients: A systematic review and meta-analysis. Frontiers in Endocrinology, 16, 1703116. https://doi.org/10.3389/fendo.2025.1703116