Resistance Circuit Training: The Science-Backed Workout That Improves Blood Pressure, Cholesterol, and Blood Sugar
Can resistance circuit training improve heart and metabolic health? Discover what the latest clinical trials and meta-analyses reveal about blood pressure, cholesterol, insulin resistance, body fat, and muscle.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/27/202628 min read
Resistance circuit training can meaningfully improve your blood pressure, cholesterol, blood sugar control, and body composition in as little as 6 weeks — with just three 45-minute sessions per week.
A growing body of clinical evidence shows this hybrid approach (compound lifts performed back-to-back with short rests) delivers both strength gains and cardiovascular benefits in one efficient workout. From large drops in insulin resistance and LDL cholesterol to better functional strength in older adults, RCT offers a practical, muscle-preserving path to cardiometabolic health — no marathon cardio sessions required.
Key Points: Resistance Circuit Training for Cardiometabolic Health
1. Hybrid Powerhouse Protocol: Resistance circuit training (RCT) — compound lifts performed back-to-back with 1–2 minute rests at 60–70% 1RM — uniquely delivers both muscular hypertrophy/strength gains and sustained cardiovascular stimulus in one 45-minute session, three times weekly. It bridges traditional lifting and aerobic work without forcing a choice.
2. Rapid, Clinically Meaningful Results: In just 6 weeks, overweight men doing RCT saw large-effect improvements: –2.5 kg body weight, –3.5% body fat, –0.91 HOMA-IR, –9.6 mg/dL LDL, +3.8 mg/dL HDL, and substantial METRNL elevation — all without dietary intervention. Effect sizes for insulin sensitivity markers exceeded 2.0 (very large).
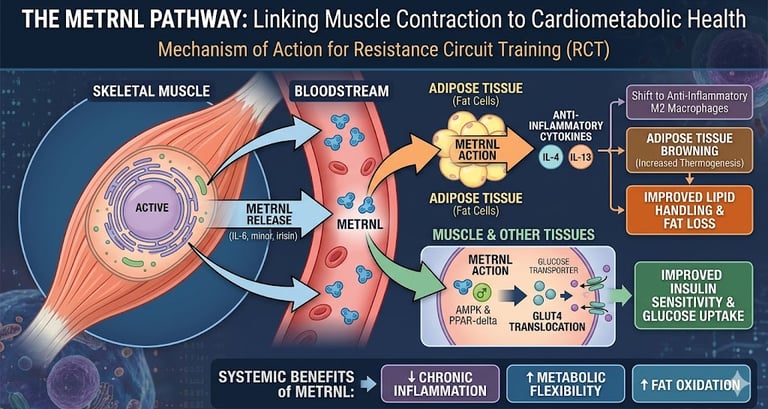
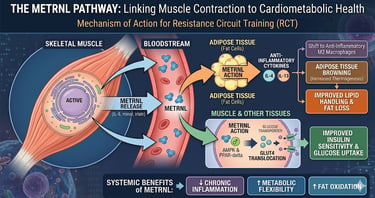
3. METRNL as a Key Myokine Mediator: Skeletal muscle releases METRNL during contractions, promoting anti-inflammatory cytokines (IL-4/IL-13), insulin sensitivity, fat oxidation, and adipose browning. Human RCT data shows strong correlations between METRNL rises and metabolic improvements, positioning muscle as a potent endocrine organ.
4. Strong Benefits for Older Adults: Meta-analyses show RCT reduces systolic BP by ~9.8 mmHg (moderate intensity superior), cuts fat mass (~5.4 kg), adds lean mass (+1.4 kg), boosts strength (large effects), improves functional autonomy, and lowers arterial stiffness — directly supporting independence and cardiovascular risk reduction.
5. Superior Body Composition Across Studies: Large-scale meta-analysis (45 studies) confirms RCT increases muscle mass (+1.9%) while decreasing fat mass (–4.3%). Unlike pure cardio, it builds rather than risks sacrificing lean tissue, making it ideal for sustainable recomposition.
6. Complementary to HIIT, Not Competitive: HIIT excels at VO₂max gains, but RCT delivers more consistent strength, functional mobility, and blood pressure benefits — especially valuable for adults over 50. The smartest approach blends both or leverages RCT’s built-in cardio element for time efficiency.
7. Contextual Cardiovascular Protection: While RCT meaningfully improves risk factors (BP, lipids, glucose, inflammation), long-term data emphasize combining resistance with aerobic elements for maximal CVD risk reduction. Short rests in circuits provide the missing aerobic stimulus pure heavy lifting lacks.
8. Actionable, Evidence-Based Prescription: Train 3 non-consecutive days (8–12 reps, 3 sets, progressive overload every 2 weeks). Prioritize form, moderate intensity for BP goals, medical clearance if at risk, and pair with some dedicated aerobic activity. Expect measurable cardiometabolic shifts in 6 weeks with consistency — an efficient, muscle-preserving path to better heart and metabolic health.
Introduction
If you've got 45 minutes, three days a week, and a few dumbbells, you have enough to meaningfully change your cardiometabolic risk profile — and you don't need to choose between lifting weights and protecting your heart.
Resistance circuit training (RCT) — moving through a sequence of strength exercises with short rest periods, so you get a strength stimulus and an elevated heart rate in the same session — sits at an unusual intersection in exercise science. It builds muscle like traditional resistance training. It challenges your cardiovascular system more like aerobic exercise. And a wave of recent trials, including a 2025 study that measured an actual exercise hormone in human blood before and after training, shows it does both at once.
This isn't another "lift weights, it's good for you" article. We're going to walk through what happened, biologically, inside the bodies of real study participants — overweight men, older adults, postmenopausal women — when they did circuit resistance training for six weeks, eight weeks, or longer. We'll show you the actual numbers: how much their blood pressure dropped, how much their LDL cholesterol fell, what happened to a newly discovered "exercise hormone" called METRNL, and — critically — what those numbers mean for your actual health risk, not just your spreadsheet of gym stats.
1. What Is Resistance Circuit Training, Exactly?
Resistance circuit training is exactly what it sounds like: a "circuit" of resistance exercises performed back-to-back, or with short rest periods, targeting different muscle groups in sequence. Instead of resting 2–3 minutes between sets of the same exercise (as in traditional bodybuilding-style training), you keep moving — squats, then a chest press, then rows, then a core exercise — often completing the whole sequence two or three times.
The defining features, based on the protocols actually used in clinical research, are:
Compound, multi-joint exercises: squats, lunges, leg presses, bench presses, rows, shoulder presses. Programs commonly target major muscle groups using squats, lunges, and leg presses for the lower body, bench presses, rows, and shoulder presses for the upper body, and planks, Russian twists, and leg raises for the core.
Moderate intensity: typically 60–70% of your one-repetition maximum (1RM) — challenging, but not maximal effort, with participants performing each exercise for 8–12 repetitions across three sets.
Short rest periods: 1–2 minutes between sets, which is what keeps your heart rate elevated and adds a cardiovascular component that traditional heavy lifting (with its longer rests) doesn't provide.
Progressive overload: load is increased every couple of weeks as you adapt, the same principle used in traditional strength training
.
How RCT differs from traditional strength training and steady-state cardio
Feature Traditional Resistance Training Resistance Circuit Training (RCT) Steady-State Cardio Rest between sets 2–5 minutes 1–2 minutes (or less) N/A (continuous) Heart rate during session Mild elevation, spikes Sustained moderate elevation Sustained moderate-high Primary stimulus Muscle hypertrophy/strength Strength + cardiovascular Cardiorespiratory fitness Session time efficiency Lower (more total time for same volume) Higher Moderate Effect on lean mass Strong Strong Minimal/negative in some contexts Effect on VO₂max Modest Moderate Strong
This hybrid nature is precisely why researchers have gotten interested in RCT for cardiometabolic health — a term that covers the cluster of risk factors (blood pressure, blood lipids, blood glucose, body fat, systemic inflammation) that together predict your risk of heart disease, stroke, and type 2 diabetes.
2. The Biology: How Lifting Weights in a Circuit Changes Your Blood Chemistry
Your muscles are an endocrine organ
Skeletal muscle doesn't just move your skeleton — it secretes signaling proteins called myokines directly into your bloodstream during and after contraction. These myokines travel to your fat tissue, liver, immune cells, and blood vessels and change how those tissues behave. This field is called exercise immunometabolism, and it's one of the more important advances in exercise science over the past decade.
One myokine getting serious research attention is METRNL (Meteorin-like protein), sometimes called Metrnl. In animal studies, METRNL has been shown to do several things relevant to your heart and metabolism:
Push immune cells in fat tissue toward an anti-inflammatory M2 phenotype, which calms the chronic low-grade inflammation that drives metabolic disease.
Improve insulin sensitivity and fat oxidation in peripheral tissues.
Stimulate adipose tissue browning — converting some white fat (pure storage) toward a more metabolically active, heat-generating "beige fat" phenotype.
Trigger the release of two specific anti-inflammatory cytokines, IL-4 and IL-13, which help maintain healthy fat tissue function.
The catch: most of this mechanistic detail comes from animal and cell studies. Until recently, we didn't have strong human evidence that resistance circuit training specifically — as opposed to aerobic exercise or HIIT — could move this hormone and have it correlate with real metabolic improvements in actual people. That's exactly the gap the 2025 Alizadeh and Safarzade study was designed to fill, and it's where we're heading next.
The cardiovascular side: why short-rest circuits stress your heart differently
When you keep rest periods short, your heart rate doesn't fully recover between exercises. Over a full circuit, this creates a sustained cardiovascular load that's different from either heavy traditional lifting (brief spikes, long recovery) or steady cardio (continuous but lower-intensity). Repeated over weeks, this pattern appears to drive adaptations in vascular function, blood pressure regulation, and autonomic nervous system balance — the same systems targeted by aerobic training, but achieved through a strength-training format. Emerging mechanistic and intervention evidence demonstrates that resistance training favorably modifies vascular function, metabolic health, autonomic regulation, and functional capacity.
3. Clinical Evidence #1: METRNL, Inflammation, and Metabolic Markers in Overweight Adults
This is the centerpiece study for understanding the mechanism, and it's worth walking through carefully because the numbers are genuinely striking for a 6-week intervention.
The study design
Alizadeh and Safarzade (2025) ran a randomized controlled trial with 30 overweight, untrained male university students (BMI 25–30 kg/m², age ~25). Fifteen participants did 6 weeks of circuit resistance training — three 45-minute sessions per week at 60–70% of their 1RM — while fifteen served as a no-intervention control group eating the same cafeteria diet.
The researchers measured serum METRNL, two anti-inflammatory cytokines (IL-4, IL-13), insulin resistance (via HOMA-IR), full lipid panel, and body composition before and after the program.
Body composition
Body weight: Participants in the resistance circuit training (CRT) group lost an average of 2.5 kg, whereas the control group gained 0.9 kg, demonstrating a statistically significant reduction in body weight after six weeks.
Body mass index (BMI): BMI decreased by 2.0 kg/m² in the CRT group, while it increased by 0.4 kg/m² in the control group. This represented a large treatment effect (Cohen's d = −1.14).
Body fat percentage: Participants performing CRT reduced their body fat by 3.5%, compared with a 0.7% increase in the control group. This improvement also showed a large effect size (d = −0.96).
Lean body mass: Lean body mass increased by 1.07 kg in the CRT group compared with 0.07 kg in controls. Although the between-group difference was not statistically significant, participants maintained (and slightly increased) muscle mass despite substantial fat loss.
Overall interpretation: Six weeks of resistance circuit training produced clinically meaningful improvements in body composition, characterized by significant reductions in body weight, BMI, and body fat while preserving lean muscle mass.
.Clinical importance: A BMI drop of 2 points in 6 weeks, driven primarily by fat loss rather than muscle loss, is a clinically meaningful change — particularly because it happened without any prescribed diet change. For context, even modest sustained weight loss (5–10% of body weight) is associated with measurable reductions in diabetes and cardiovascular risk in the broader literature. This study suggests RCT can produce a meaningful chunk of that change in just six weeks.
Glucose and Insulin
Key Findings
Fasting blood glucose: The CRT group reduced fasting blood glucose by 0.9 mmol/L, while the control group showed a slight increase of 0.05 mmol/L, with a very large effect size (d = −2.38).
Fasting insulin: Participants undergoing CRT experienced a 2.1 µU/mL reduction in fasting insulin, compared with a 0.4 µU/mL increase in the control group. The effect size was very large (d = −1.67).
Insulin resistance (HOMA-IR): HOMA-IR decreased by 0.91 in the CRT group but increased by 0.12 in controls. The reduction corresponded to a very large effect size (d = −2.39).
Significant improvement in insulin sensitivity: HOMA-IR fell from 2.85 to 1.94 in the CRT group, representing a statistically significant improvement compared with the control group.
Clinical Importance
Reduced insulin resistance: The decline in HOMA-IR suggests that the body required less insulin to maintain normal blood glucose, indicating markedly improved insulin sensitivity.
Large treatment effects: Effect sizes exceeding 2.0 are considered exceptionally large in exercise science, substantially greater than the 0.2–0.8 effect sizes typically reported for most lifestyle interventions.
Clinical implication: Although resistance circuit training is not a replacement for diabetes medication when pharmacological treatment is indicated, these findings suggest that it can be a highly effective strategy for improving insulin sensitivity within a relatively short period.
Lipid Profile
Key Findings
Total cholesterol: Decreased by 14.1 mg/dL in the CRT group, while increasing by 2 mg/dL in controls.
Triglycerides: Declined by 12.8 mg/dL following CRT, compared with a 1 mg/dL increase in the control group.
LDL ("bad") cholesterol: Fell by 9.6 mg/dL in the CRT group but increased by 2.4 mg/dL in controls.
HDL ("good") cholesterol: Increased by 3.8 mg/dL after CRT, whereas the control group experienced a 1 mg/dL decrease.
Overall lipid response: Every lipid parameter improved significantly more in the resistance circuit training group than in the control group.
Clinical Importance
Favorable lipid remodeling: CRT produced the classic cardioprotective lipid profile characterized by lower LDL cholesterol and triglycerides together with higher HDL cholesterol.
Potential cardiovascular benefit: A sustained ~10 mg/dL reduction in LDL cholesterol may contribute to lower cardiovascular risk and is comparable to improvements achieved through moderate dietary modification, although it remains smaller than the LDL reductions typically produced by statin therapy.
Long-term perspective: Because this intervention lasted only six weeks, additional studies are needed to determine whether these lipid improvements are maintained over longer periods.
METRNL and Inflammation
Key Findings
METRNL levels: Serum METRNL increased by 0.60 ng/mL in the CRT group compared with only 0.04 ng/mL in controls, representing a very large effect size (d = 2.6).
Anti-inflammatory cytokines: Levels of IL-4 and IL-13 increased significantly following resistance circuit training.
Strong positive correlations: Increases in METRNL were strongly associated with:
IL-4 (r = 0.91)
IL-13 (r = 0.91)
HDL cholesterol (r = 0.87)
Strong negative correlations: Higher METRNL levels were associated with lower:
Fasting glucose
Fasting insulin
HOMA-IR
Triglycerides
Total cholesterol
LDL cholesterol
BMI
Body fat percentage
Correlation strength: Most correlation coefficients ranged from 0.70 to 0.96, indicating very strong associations.
Clinical Importance
Potential biological mechanism: The findings support the hypothesis that METRNL may act as an exercise-induced myokine linking skeletal muscle contraction with improved metabolic and inflammatory health.
Evidence remains preliminary: Although the correlations are compelling, they do not establish cause and effect.
Important limitation: Because the study involved a small sample of young overweight men and lasted only six weeks, it cannot determine whether METRNL directly mediates these metabolic improvements or simply reflects broader physiological adaptations to exercise.
Future research: Larger, longer-term, and tissue-specific studies are required before METRNL can be considered a confirmed therapeutic target rather than a promising biomarker of exercise adaptation.
4. Clinical Evidence #2: What Happens to Older Adults Who Do Circuit Resistance Training
Aging brings a predictable cluster of problems: loss of muscle mass (sarcopenia), rising blood pressure, declining cardiorespiratory fitness, and reduced ability to do daily tasks independently. A major 2024 systematic review and meta-analysis pooled data across multiple randomized controlled trials specifically to answer: does resistance circuit training meaningfully change this trajectory?
The findings, pooled across studies
Resistance circuit training reduces body fat (mean difference = −5.39 kg), BMI (mean difference = −1.22), and body weight (mean difference = −1.28 kg), while increasing lean body mass (mean difference = +1.42 kg) in older adults.
On strength and function:
RCT improves upper limb strength (standardized mean difference = 2.09) and lower limb strength (standardized mean difference = 2.03), cardiorespiratory endurance (mean difference = +94 meters on a walking test), and functional autonomy.
On blood pressure — arguably the most clinically important cardiovascular finding here:
Across the pooled trials, systolic blood pressure dropped by a mean of 9.8 mmHg (95% CI −13.26 to −6.31) compared to control groups. Interestingly, the intensity mattered: systolic blood pressure dropped more with moderate-to-low intensity exercise (mean difference = −13.8 mmHg) than with high-intensity exercise, which showed no significant change, and moderate-to-low intensity training similarly produced a larger drop in diastolic blood pressure (mean difference = −6.8 mmHg).
Clinical importance: A 9.8 mmHg drop in systolic blood pressure is not a trivial number. In the cardiovascular epidemiology literature, sustained reductions of this magnitude are associated with meaningfully lower risk of stroke and cardiovascular events at a population level — comparable to what some single antihypertensive medications achieve. The finding that moderate intensity outperformed high intensity for blood pressure is also clinically actionable: it suggests older adults (and anyone concerned about blood pressure specifically) don't need to push to exhaustion to get the cardiovascular benefit, and in fact may do better training at a more moderate, sustainable effort level.
Here is the breakdown of the findings from the 2025 meta-analysis on community-dwelling older adults,
Blood Pressure
Systolic blood pressure: Circuit-based resistance training reduced systolic blood pressure by an average of 6.10 mmHg.
Diastolic blood pressure: Participants also experienced a significant reduction in diastolic blood pressure of 2.88 mmHg.
Arterial Stiffness
Improved vascular health: Circuit-based resistance training reduced brachial-ankle pulse wave velocity (baPWV) by 101.81 cm/s, indicating a significant improvement in arterial stiffness.
Body Composition
Lower body fat: Participants showed significant reductions in body fat percentage and total fat mass.
Greater lean mass: Lean body mass increased following the training intervention, reflecting improvements in muscle preservation and overall body composition.
Bone Health
Improved bone mineral content: Resistance circuit training increased femoral neck bone mineral content, suggesting potential benefits for skeletal health and osteoporosis prevention.
Impact of Training Frequency
More than three sessions per week: Training more than three times weekly produced a greater reduction in systolic blood pressure than training twice a week or less.
Diastolic blood pressure: Improvements in diastolic blood pressure were similar regardless of weekly training frequency, indicating that this benefit was less dependent on exercise frequency.
Clinical Importance
Reduced cardiovascular risk: Improvements in both blood pressure and arterial stiffness suggest that resistance circuit training enhances vascular function, not merely lowers blood pressure.
Healthier blood vessels: Because arterial stiffness is an independent predictor of cardiovascular events, reducing brachial-ankle pulse wave velocity indicates meaningful improvements in blood vessel health that may contribute to lower long-term cardiovascular risk.
Comprehensive health benefits: In addition to improving vascular function, circuit-based resistance training simultaneously enhances body composition, muscle mass, and bone health, making it an effective strategy for promoting healthy aging and cardiometabolic health.Functional autonomy: why this matters beyond the lab
The meta-analysis of included studies reporting functional autonomy demonstrated that RCT interventions led to meaningful improvement among older adults, and the broader literature notes that high-intensity resistance circuit training has been shown to increase muscle strength, muscle mass, and bone mineral density in older adults, and has been associated with reductions in cardiovascular risk factors including blood pressure.
In plain terms: this isn't just about lab numbers. Functional autonomy measures — things like how fast someone can get up from a chair, walk a set distance, or climb stairs — predict whether an older adult can live independently and avoid falls. Improvements here have a direct line to quality of life and reduced disability risk, not just abstract "fitness."
5. Clinical Evidence #3: The Big-Picture Meta-Analysis on Body Composition, Strength, and Cardiorespiratory Fitness
Zooming out from any single population, Ramos-Campo and colleagues (2021) conducted a comprehensive systematic review and meta-analysis pooling data from 45 studies, encompassing 58 exercise groups (897 participants) and 34 control groups (474 participants) — one of the largest aggregations of resistance circuit training data available.
Circuit-based resistance training interventions led to increases in muscle mass of 1.9% and decreases in fat mass of 4.3%, both statistically significant.
Clinical importance: Because this pools data across dozens of trials with different populations (young, old, healthy, overweight) and different protocols, it gives us confidence that the body composition benefits seen in individual trials (like the METRNL study above) aren't a fluke of one small sample — they replicate at scale. A 4.3% average reduction in fat mass with a simultaneous increase in muscle mass is the body composition outcome most people are actually trying to achieve, and it's notable that resistance circuit training delivers both at once rather than trading one for the other (a common concern with pure-cardio approaches, which can sometimes reduce both fat and muscle).
This meta-analysis is frequently cited as foundational evidence in the more specific, mechanism-focused studies we've already covered — both the METRNL trial and the older-adult meta-analysis reference it directly, underscoring that the field has converged on circuit-based resistance training as a genuinely distinct, evidence-backed training modality rather than a fitness trend.
6. Clinical Evidence #4: How Circuit Resistance Training Compares to HIIT
A natural question: if you only have time for one type of time-efficient workout, should it be resistance circuit training or high-intensity interval training (HIIT)? A 2026 systematic review and meta-analysis focused specifically on middle-aged and older women gives us a useful comparison point — not against RCT directly, but against the same outcomes RCT trials measure, which lets us put the two modalities side by side.
Across 19 randomized controlled trials, HIIT significantly improved VO2max compared with control interventions, with a large effect size (SMD = 1.20) and high certainty of evidence.
However, HIIT's advantages were concentrated almost entirely in cardiorespiratory fitness, not in the broader functional and strength outcomes where circuit resistance training excels:
Flexibility showed no significant improvement after HIIT (SMD = 0.17, not statistically significant).
The Timed Up and Go test, a functional mobility measure, showed a large but statistically non-significant effect favoring HIIT, with very high heterogeneity between studies (I² = 94%).
A composite physical function measure showed only a borderline significant improvement with HIIT (SMD = 0.49, p = 0.05).
Clinical importance: This is a meaningful distinction. HIIT reliably and robustly improves cardiorespiratory fitness (VO2max) — arguably more reliably than RCT does, since aerobic capacity is its primary training target. But for the strength, functional mobility, and musculoskeletal outcomes that matter enormously for older adults' independence and fall risk, the evidence for HIIT is weaker and less consistent, while resistance circuit training's strength and functional-autonomy effects (covered in Section 4) are large and consistent.
The practical takeaway: these aren't really competing modalities — they're complementary. If your primary goal is maximizing aerobic capacity, HIIT has an edge. If your goals include preserving muscle, bone density, functional independence, and blood pressure control alongside cardiovascular benefit, resistance circuit training — which blends both stimuli in one session — may be the more time-efficient single choice, particularly for anyone over 50 or managing several cardiometabolic risk factors at once.
7. Clinical Evidence #5: The Bigger Cardiovascular Picture — Why Sedentary Time Matters Even If You Exercise
A 2026 narrative review provides important context for why resistance training deserves a bigger seat at the table in cardiovascular prevention, beyond just the direct biomarker changes covered above.
Sedentary behavior is increasingly recognized as an independent risk factor for cardiovascular disease, yet prevention efforts continue to emphasize aerobic exercise while underutilizing resistance training. The review synthesizes evidence showing that large-scale epidemiologic studies consistently link prolonged sedentary time to increased cardiovascular morbidity and mortality, even among physically active adults — meaning your 45-minute circuit session doesn't fully cancel out 10 hours of sitting, but resistance training specifically appears to counteract some of that risk through different pathways than aerobic exercise alone.
Community- and clinic-based resistance training interventions show particular promise in reducing sedentary-related cardiovascular risk among older adults and high-risk populations.
Clinical importance — and a necessary dose of nuance: It would be easy to read this section and conclude resistance training alone solves cardiovascular risk. The evidence doesn't support going that far. A 20-year cohort study (the ATTICA study, n≈2,000) found that participants in a combined aerobic-and-resistance training group had a 59% lower risk of atherosclerotic cardiovascular disease compared to inactive participants, and those doing aerobic exercise alone had a 46% lower risk — but resistance training alone, without a meaningful aerobic component, showed no statistically significant association with reduced cardiovascular risk over two decades.
This is an important corrective to keep in mind throughout this article: the strongest, most consistent long-term cardiovascular protection comes from combining aerobic and resistance work, which is exactly what resistance circuit training is designed to do — it's not "pure" resistance training in the powerlifting sense, precisely because the short rest periods add the cardiovascular component that pure strength training lacks. This is likely part of why RCT performs so well across the biomarker studies above: it isn't choosing between the two approaches, it's blending them in a single session.
A separate randomized trial comparing aerobic, resistance, and combined training head-to-head over 8 weeks found that combined training produced significant reductions in both peripheral and central diastolic blood pressure (−4 mmHg each), an increase in cardiorespiratory fitness of 4.9 mL/kg/min, and increases in upper body strength (4 kg), lower body strength (11 kg), and lean body mass (0.8 kg) — outperforming either modality alone on several measures.
8. Evidence Summary Table
Alizadeh & Safarzade (2025): Mechanistic Randomized Controlled Trial
Conducted in 30 overweight young men over 6 weeks.
Resistance circuit training significantly:
Reduced BMI by 2.0 kg/m².
Decreased body fat by 3.5%.
Improved insulin resistance (HOMA-IR) from 2.85 to 1.94.
Lowered LDL cholesterol by approximately 10 mg/dL.
Increased HDL cholesterol by approximately 4 mg/dL.
Increased circulating METRNL, an exercise-induced myokine linked to metabolic health.
Evidence strength: A well-designed randomized controlled trial that provides valuable mechanistic insights, although its small sample size and short duration limit generalizability.
Hu, Xia, Zeng et al. (2024): Systematic Review and Meta-analysis
Pooled data from studies involving older adults.
Resistance circuit training significantly:
Reduced systolic blood pressure by 9.8 mmHg.
Decreased body fat by 5.39 kg.
Increased lean body mass by 1.42 kg.
Produced large improvements in upper- and lower-limb strength.
Evidence strength: High-quality evidence based on pooled results from multiple clinical trials, providing strong support for the cardiovascular and body composition benefits of resistance circuit training.
Ramos-Campo et al. (2021): Large Meta-analysis
Combined results from 45 studies involving 1,371 participants.
Reported:
1.9% increase in muscle mass.
4.3% reduction in fat mass.
Evidence strength: One of the strongest sources of evidence demonstrating consistent improvements in body composition across diverse adult populations.
Cai, Guo, Zhang et al. (2026): HIIT Meta-analysis
Examined middle-aged and older women.
High-intensity interval training (HIIT) significantly:
Improved cardiorespiratory fitness (VO₂max) with a large effect size.
Produced less consistent improvements in functional outcomes.
Evidence strength: Strong evidence supporting HIIT for improving aerobic fitness, although benefits for broader physical function were less robust than those observed for resistance circuit training.
Johnson (2026): Narrative Review
Reviewed evidence across general adult populations.
Concluded that resistance training:
Improves vascular function.
Enhances metabolic health.
Supports autonomic nervous system regulation.
Helps counteract the harmful cardiovascular effects of prolonged sedentary behavior.
Evidence strength: A narrative review provides valuable physiological context but is considered lower on the evidence hierarchy than systematic reviews and meta-analyses.
Evidence Hierarchy: How Strong Is the Overall Evidence?
Systematic reviews and meta-analyses provide the strongest level of evidence because they combine findings from multiple independent studies, reducing the influence of chance and study-specific bias.
The Hu et al. (2024) and Ramos-Campo et al. (2021) meta-analyses consistently demonstrate that resistance circuit training improves blood pressure, body composition, muscle mass, and physical function across diverse populations.
The Alizadeh & Safarzade (2025) randomized controlled trial complements these findings by offering detailed mechanistic evidence, including improvements in METRNL, insulin sensitivity, lipid metabolism, and inflammatory markers.
However, because the METRNL study involved a small sample of young overweight men and lasted only six weeks, its mechanistic findings—particularly the observed correlations between METRNL and metabolic outcomes—should be viewed as promising but preliminary rather than definitive proof of causality.
Taken together, the evidence indicates that resistance circuit training is an effective strategy for improving cardiometabolic health, while ongoing research will help clarify the precise biological mechanisms underlying these benefits.
9. How to Build Your Own Resistance Circuit Training Program
Based on the protocols actually used in these clinical trials, here's how to structure a program that mirrors what's been shown to work.
The core framework
Frequency: 3 non-consecutive days per week (e.g., Monday/Wednesday/Friday), matching the protocol used in the METRNL trial.
Session structure: 5-minute warm-up → 30–35 minutes of circuit work → 5-minute cool-down.
Intensity: 60–70% of your one-rep max — challenging but sustainable, rated roughly 13–15 ("moderate to somewhat hard") on a 6–20 perceived exertion scale.
Volume: 8–12 reps per exercise, 3 sets, with 1–2 minutes rest between sets — the short rest is what makes it a "circuit" rather than traditional lifting.
Progressive overload: Increase load by 5–10% every 2 weeks once you can comfortably complete more than 12 reps with good form.
A note on intensity for blood pressure goals specifically
If lowering blood pressure is a primary goal — particularly relevant if you're over 50 or already have elevated readings — remember the finding from Section 4: moderate-to-low intensity outperformed high intensity for both systolic and diastolic blood pressure reduction in the older-adult meta-analysis. You don't need to chase maximal effort to get this particular benefit, and pushing too hard may even blunt it.
Exercise selection checklist
Build your circuit from one exercise per category, rotating selections every few weeks to keep things engaging and to challenge muscles from different angles:
Lower body push: squats, leg press
Lower body unilateral: lunges, step-ups
Upper body push: bench press, shoulder press, push-ups
Upper body pull: rows (any variation), lat pulldowns
Core: planks, Russian twists, leg raises
10. A Sample 6-Week Beginner Protocol
This mirrors the structure used in the clinical trials above, adapted for someone starting from a general fitness base. Always get medical clearance first if you have any cardiovascular risk factors (see Section 12).
Sample 6-Week Resistance Circuit Training Program
Weeks 1–2: Build the Foundation
Goal: Learn proper exercise technique, establish movement patterns, and prepare the body for progressive overload.
Bodyweight or Goblet Squat: 3 sets × 10–12 reps (60–90 seconds rest)
Push-Up (Knee or Full): 3 sets × 8–12 reps (60–90 seconds rest)
Dumbbell Row: 3 sets × 10–12 reps (60–90 seconds rest)
Walking Lunge: 3 sets × 10 repetitions per leg (60–90 seconds rest)
Plank: 3 sets × 30–45-second hold (60 seconds rest)
Weeks 3–4: Progressive Overload
Goal: Increase training intensity while maintaining good exercise technique.
Increase the training load by 5–10% on any exercise if you comfortably completed 12 repetitions with proper form during Week 2.
If recovery is adequate, consider adding one additional circuit round.
Exercise Program
Goblet or Barbell Squat: 3 sets × 8–12 reps (60–90 seconds rest)
Bench Press or Dumbbell Chest Press: 3 sets × 8–12 reps (60–90 seconds rest)
Seated or Standing Row: 3 sets × 8–12 reps (60–90 seconds rest)
Step-Up: 3 sets × 10 repetitions per leg (60–90 seconds rest)
Russian Twist: 3 sets × 15 repetitions per side (60 seconds rest)
Weeks 5–6: Full Resistance Circuit
Goal: Maximize cardiovascular and metabolic adaptations by completing a full resistance circuit.
If recovery remains good, perform two complete circuit rounds, following the study protocol of three sets per exercise during the session.
Exercise Program
Loaded Squat: 3 sets × 8–12 reps (60–90 seconds rest)
Shoulder Press: 3 sets × 8–12 reps (60–90 seconds rest)
Bent-Over Row: 3 sets × 8–12 reps (60–90 seconds rest)
Loaded Lunge: 3 sets × 8–10 repetitions per leg (60–90 seconds rest)
Leg Raise: 3 sets × 12–15 reps (60 seconds rest)
Practical Tips
Perform a 5–10 minute warm-up before each session using light aerobic activity and dynamic mobility exercises.
Complete the program 2–3 times per week, allowing at least 48 hours between sessions for recovery.
Prioritize proper exercise technique before increasing resistance.
Progress weights gradually while maintaining good form throughout every repetition.
Finish each workout with a 5-minute cool-down and gentle stretching to promote recovery and flexibility.
11. Common Myths and Mistakes
Myth: "Circuit training is just cardio with weights — it won't build real strength." The meta-analysis data directly contradicts this: pooled across 45 studies, RCT produced significant increases in muscle mass (1.9%) alongside fat loss, and in older adults produced large effect sizes for both upper and lower limb strength.
Myth: "You need to train at high intensity to get cardiovascular benefits." The opposite was true for blood pressure specifically in the older-adult meta-analysis — moderate-to-low intensity outperformed high intensity for both systolic and diastolic blood pressure reduction. Don't assume "harder is always better" — for some markers, sustainable moderate effort wins.
Mistake: Skipping the short rest periods. If you rest 3+ minutes between exercises "to be safe," you've effectively converted your circuit back into traditional strength training and may lose the cardiovascular adaptation that distinguishes RCT. The 1–2 minute rest window used across these trials is part of the active ingredient, not an incidental detail.
Mistake: Treating resistance training as a total substitute for aerobic exercise. The 20-year ATTICA cohort data is a useful reality check: resistance training alone, without any aerobic component, showed no significant association with reduced cardiovascular disease risk over two decades, while combined aerobic-plus-resistance training showed the strongest protection. Circuit-style training, with its built-in cardiovascular component, is a good way to get both — but if you're doing zero other aerobic activity, it's worth knowing that the longest-term evidence favors a combined approach.
Mistake: Expecting METRNL or any single myokine to be "the" mechanism. It's tempting to treat a hormone like METRNL as the full explanation for why exercise works. The researchers behind the human METRNL trial were explicit that their findings show correlation, not proven causation, and called for more mechanistic research before drawing firm conclusions. The real story is almost certainly multiple overlapping pathways (myokines, vascular adaptations, autonomic changes) working together.
Mistake: Assuming results from a 6-week trial in young men apply identically to you. The METRNL study is genuinely useful, but it was conducted in 30 young, overweight, untrained men over six weeks. If you're older, female, already metabolically healthy, or training for years rather than weeks, your physiological response may differ — which is exactly why we've included the older-adult and broader meta-analysis data above for a fuller picture.
12. Safety Considerations and When to Talk to Your Doctor
Resistance circuit training is generally well-tolerated, including in older and clinical populations, but a few safety notes are worth taking seriously:
Get cleared first if you have known cardiovascular disease, uncontrolled high blood pressure, recent cardiac events, or musculoskeletal conditions. The clinical trials cited here specifically excluded people with cardiometabolic disease, acute illness, or conditions precluding safe exercise participation. That exclusion exists for a reason — these populations need individualized medical guidance before starting.
If you're on blood pressure or diabetes medication, monitor for symptoms of overcorrection (lightheadedness, unusually low readings) as your fitness improves, since exercise-induced improvements in blood pressure and insulin sensitivity can sometimes require medication adjustments — something only your physician should manage.
Form before load. The trials used supervised sessions with trainers providing real-time feedback and form correction. If you're newer to resistance training, consider at least a few sessions with a qualified trainer to learn proper technique before circuit-style training at higher intensities.
Progress gradually. The 5–10% load increase every two weeks used in these trialsis a reasonable, evidence-based pace — resist the urge to progress faster, especially in the first few weeks.
This article is for educational purposes and does not replace personalized medical advice. If you have existing heart disease, diabetes, uncontrolled hypertension, or any condition affecting exercise safety, talk to your doctor or a qualified exercise physiologist before starting a new training program.
13. Frequently Asked Questions
How quickly can I expect to see cardiometabolic changes from circuit resistance training? In the clinical trial reviewed here, measurable changes in body fat, blood glucose, insulin resistance, and lipid profile were detected after just 6 weeks of training, three sessions per week. Individual results vary, and longer programs generally produce larger, more durable changes.
Is resistance circuit training better than HIIT for heart health? They're not directly competing — they excel at different things. HIIT shows a strong, well-established effect on cardiorespiratory fitness (VO2max), while resistance circuit training shows stronger, more consistent effects on strength, functional mobility, and blood pressure in older adults. Many experts would suggest combining both rather than choosing one exclusively.
Can resistance circuit training lower blood pressure on its own? Yes — pooled data from older-adult trials found systolic blood pressure dropped by an average of 9.8 mmHg compared to control groups, with moderate-intensity programs producing the largest effect. That said, if you have hypertension, this should complement — not replace — your prescribed treatment plan.
Do I need to do circuit training at high intensity to get results? Not necessarily, and for blood pressure specifically, the evidence suggests otherwise: moderate-to-low intensity training outperformed high-intensity training for both systolic and diastolic blood pressure reduction in a major meta-analysis of older adults.
What is METRNL and why does it matter? METRNL (Meteorin-like protein) is a hormone released by muscle during exercise that, in lab studies, has anti-inflammatory and metabolism-improving effects. A 2025 human trial found that six weeks of circuit resistance training significantly raised METRNL levels, and those increases correlated strongly with improvements in blood sugar, cholesterol, and body fat— though the researchers caution this shows correlation, not proven cause-and-effect.
Will circuit resistance training make me lose muscle while losing fat? The opposite tends to happen. Across a large pooled meta-analysis of 45 studies, RCT produced an average 1.9% increase in muscle mass alongside a 4.3% decrease in fat mass, and the METRNL trial found lean body mass was unaffected (slightly increased, though not significantly) even as participants lost substantial fat.
Is resistance circuit training safe for older adults? The evidence base specifically supports this population: meta-analyses focused on older adults found significant improvements in strength, body composition, blood pressure, and functional autonomy, with appropriately designed, often supervised programs. That said, medical clearance and proper supervision are especially important for older adults or those with existing health conditions.
How does resistance circuit training compare to just lifting weights normally? The short rest periods (1–2 minutes) used in circuit-style programs add a cardiovascular stimulus that traditional, longer-rest strength training doesn't provide to the same degree, which may explain why RCT shows such consistent effects across both strength and cardiometabolic markers like blood pressure and lipids.
Can resistance circuit training replace cardio entirely? Probably not optimally. Long-term cohort data (20 years of follow-up) found that resistance training alone, without an aerobic component, wasn't significantly associated with reduced cardiovascular disease risk, while combined aerobic-and-resistance activity showed the strongest protective association. Circuit-style resistance training's built-in cardiovascular component may help bridge this gap, but pairing it with some dedicated aerobic activity is still the most evidence-backed approach.
How many days per week should I do circuit resistance training? The clinical trials reviewed here used three non-consecutive sessions per week (e.g., Monday/Wednesday/Friday), allowing recovery days between sessions. This frequency appears in multiple trials and is a reasonable, evidence-aligned starting point.
What's a realistic body fat percentage change I could expect? In the 6-week trial, the exercise group's body fat percentage dropped by 3.5 percentage points compared to controls, while pooled older-adult data showed an average reduction of 5.39 kg of body fat mass. Individual results depend heavily on starting point, diet, consistency, and program duration.
14. Conclusion and Your Next Steps
The evidence reviewed here points to a consistent picture: resistance circuit training isn't just a time-efficient way to build muscle — it produces measurable, clinically relevant changes in the specific markers that predict cardiovascular and metabolic disease risk. Blood pressure drops by an amount comparable to some medications. LDL cholesterol falls and HDL rises in the same favorable direction cardiologists look for. Insulin resistance improves with some of the largest effect sizes reported in exercise research. And it does all this while building, not sacrificing, lean muscle mass.
It's not a magic bullet, and the honest caveats matter: most individual trials are short and modest in size, the mechanistic claims around hormones like METRNL are still being established, and the strongest long-term cardiovascular protection appears to come from combining resistance work with some aerobic activity rather than relying on resistance training alone.
Your action steps:
Get medical clearance if you have existing cardiovascular risk factors, are over 50 and haven't exercised regularly, or have any condition that affects exercise safety.
Start with the Weeks 1–2 protocol above, focusing on form before load.
Train three non-consecutive days per week, keeping rest periods to 1–2 minutes to preserve the cardiovascular benefit.
Progress load by 5–10% every two weeks once you can comfortably exceed 12 reps with good form.
Pair it with some aerobic activity — even brisk walking — rather than relying on resistance training alone for cardiovascular protection.
Track what matters: not just the scale, but blood pressure, waist circumference, and — if accessible — periodic lipid panels with your doctor, since these are the markers the research above actually measured.
You don't need a gym membership, hours of free time, or perfect genetics to move these numbers. You need a structured plan, consistency, and roughly 45 minutes, three days a week — and six weeks from now, your blood work could look meaningfully different.
Medical Disclaimer
The information in this article, including the research findings, is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Before starting a resistance exercise program, you must consult with a qualified healthcare professional, especially if you have existing health conditions (such as cardiovascular disease, uncontrolled hypertension, or advanced metabolic disease). Exercise carries inherent risks, and you assume full responsibility for your actions. This article does not establish a doctor-patient relationship.
Related Articles
References
Alizadeh, H., Safarzade, A. (2025). Effects of circuit resistance training on serum myokine METRNL and cardiometabolic health markers in overweight participants: a 6-week intervention study. Sport Sciences for Health, 21, 1127–1138. https://doi.org/10.1007/s11332-025-01350-9
Hu, C., Xia, Y., Zeng, D., Ye, M., Mei, T. (2024). Effect of resistance circuit training on comprehensive health indicators in older adults: a systematic review and meta-analysis. Scientific Reports, 14, 8823. https://doi.org/10.1038/s41598-024-59386-9
Ramos-Campo, D. J., Andreu Caravaca, L., Martínez-Rodríguez, A., Rubio-Arias, J. Á. (2021). Effects of Resistance Circuit-Based Training on Body Composition, Strength and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Biology, 10(5), 377. https://doi.org/10.3390/biology10050377
Cai, L., Guo, J., Zhang, R., Gu, J., Zhao, L., Wu, J., Yu, Y., Chen, S. (2026). Effects of high intensity interval training (HIIT) on cardiopulmonary fitness and physical function in middle-aged and elderly women: a systematic review and meta-analysis. Frontiers in Physiology, 17:1778052. https://doi.org/10.3389/fphys.2026.1778052
Johnson, M. A. (2026). Breaking the Sedentary Cycle: The Role of Resistance Training in Cardiovascular Health and Disease Prevention. Current Epidemiology Reports, 13, 10. https://doi.org/10.1007/s40471-026-00390-0
Hu, Z., Jiang, S., Hu, C., Shen, B., Gu, J. (2025). The effects of circuit-based resistance training on blood pressure, arterial stiffness, and body composition in community-dwelling older adults: a systematic review and meta-analysis. Frontiers in Physiology. PMID: 40464000.
Panagiotakos, D. et al. Assessment of Long-Term Engagement in Aerobic Versus Resistance Exercise on 20-Year Cardiovascular Disease Incidence (2002–2024): The ATTICA Epidemiological Cohort Study. PMC11765820.
Comparative effectiveness of aerobic, resistance, and combined training on cardiovascular disease risk factors: A randomized controlled trial. PMC6322789.
Silva, J. G., Rodrigues, L. F., Torres, T., Improta-Caria, A. C., Oliveira, E. M., Fernandes, T. (2026). Resistance training and cardiovascular health: epigenetic regulation. Frontiers in Physiology. PMC12851980.
Tayebi, S. M., Golmohammadi, M., Eslami, R., Shakiba, N., Costa, P. B. (2023). The effects of eight weeks of circuit resistance training on serum METRNL levels and insulin resistance in individuals with type 2 diabetes. Journal of Diabetes & Metabolic Disorders, 22, 1151–1158.
Rao, R. R., Long, J. Z., White, J. P., et al. (2014). Meteorin-like is a hormone that regulates immune-adipose interactions to increase beige fat thermogenesis. Cell, 157(6), 1279-1291.
Li, Z., Gao, Z., Sun, T., et al. (2023). Meteorin-like/Metrnl, a novel secreted protein implicated in inflammation, immunology, and metabolism: A comprehensive review of preclinical and clinical studies. Frontiers in Immunology, 14:1098570.
Lee, J. O., Byun, W. S., Kang, M. J., et al. (2020). The myokine meteorin-like (metrnl) improves glucose tolerance in both skeletal muscle cells and mice by targeting AMPKα2. FEBS Journal, 287, 2087-2104.
Jung, T. W., Lee, S. H., Kim, H-C., et al. (2018). METRNL attenuates lipid-induced inflammation and insulin resistance via AMPK or PPARδ-dependent pathways in skeletal muscle of mice. Experimental & Molecular Medicine, 50, 1-11.
American College of Sports Medicine (ACSM). Guidelines for Exercise Testing and Prescription. (Referenced standard for exercise intensity and prescription frameworks.)
American Heart Association (AHA). Recommendations on physical activity and resistance training for cardiovascular health. (Referenced standard for general exercise guidance.)
This article synthesizes peer-reviewed research for educational purposes. It is not a substitute for individualized medical advice. Always consult your physician before beginning a new exercise program, particularly if you have cardiovascular disease, diabetes, or other chronic health conditions.