Obesity as a Neuroendocrine Disease: Brain, Leptin Resistance & Appetite Control (2026)
Is obesity a brain disease? Discover how leptin resistance, hypothalamic inflammation, dopamine dysfunction, and the gut-brain axis drive weight gain—and learn the latest science-backed treatments for lasting weight loss.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/3/202620 min read
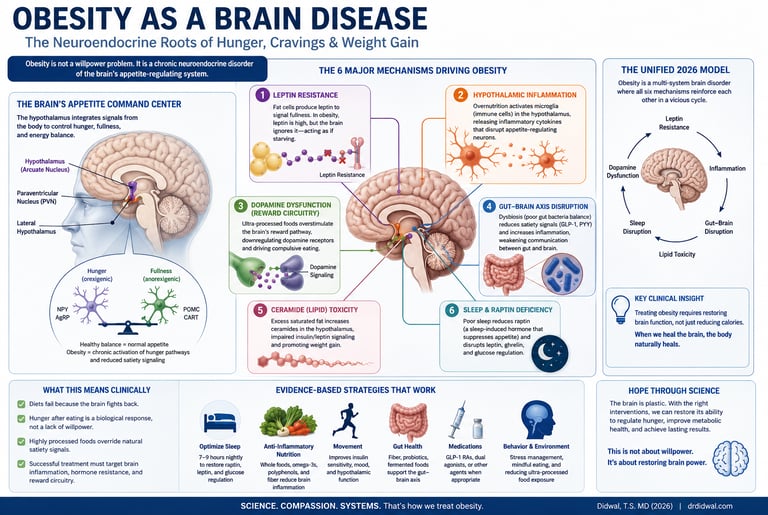
Obesity is increasingly recognized as a brain-based neuroendocrine disorder rather than simply a problem of overeating. Leptin resistance, hypothalamic inflammation, dopamine dysfunction, gut-brain signaling abnormalities, and sleep disruption can impair appetite regulation, leading to persistent hunger, weight gain, and difficulty maintaining long-term weight loss despite adequate energy stores.
Key Takeaways
Obesity is not simply a willpower problem. Modern research increasingly recognizes obesity as a complex neuroendocrine disorder involving the brain, hormones, metabolism, and environment.
The hypothalamus acts as the body's appetite control center. Dysfunction within this region can impair hunger regulation, satiety signaling, and energy balance.
Leptin resistance is a central driver of obesity. Despite high levels of leptin, the brain may fail to recognize that adequate energy stores exist, resulting in persistent hunger and reduced energy expenditure.
Hypothalamic inflammation may precede significant weight gain. Chronic overnutrition can activate brain immune cells, disrupting normal appetite-regulating pathways.
Ceramides and lipid toxicity contribute to brain dysfunction. These bioactive lipids can impair leptin and insulin signaling within appetite-control centers of the brain.
Ultra-processed foods affect reward pathways. Repeated exposure can alter dopamine signaling, increase cravings, and promote compulsive overeating behaviors.
The gut microbiome influences appetite and metabolism. Gut-derived metabolites and vagal signaling play important roles in regulating hunger, satiety, and inflammation.
Sleep is a critical metabolic regulator. Sleep deprivation disrupts leptin, ghrelin, and other neuroendocrine pathways, increasing hunger and promoting weight gain.
Obesity results from multiple interconnected biological systems. Brain dysfunction, hormonal resistance, reward-circuit changes, and peripheral metabolic abnormalities reinforce one another in a self-perpetuating cycle.
Effective treatment requires a multimodal approach. High-quality sleep, regular exercise, protein- and fiber-rich nutrition, reduction of ultra-processed foods, behavioral support, and appropriate pharmacotherapy work synergistically to restore metabolic health.
GLP-1 receptor agonists represent a major therapeutic advance. These medications act directly on brain and metabolic pathways to reduce appetite and improve weight regulation.
The future of obesity medicine lies in precision neuroendocrinology. Emerging therapies targeting hypothalamic inflammation, leptin sensitivity, oxytocin pathways, and gut-brain signaling may enable more personalized obesity treatment in the coming years
.For decades, obesity was viewed primarily as a problem of willpower, personal responsibility, and excessive calorie consumption. The prevailing advice was simple: eat less, move more, and the weight would come off. Yet this explanation fails to account for a striking reality—most individuals who lose weight eventually regain it, often despite extraordinary efforts to maintain healthy habits. If obesity were merely a matter of self-control, why would long-term weight loss prove so difficult for millions of people worldwide?
Modern neuroscience and endocrinology now offer a very different explanation. Emerging evidence suggests that obesity is not simply a disorder of excess body fat but a complex neuroendocrine disease involving dysfunction of the brain’s appetite-regulating systems. The hypothalamus, the brain region responsible for monitoring energy stores and controlling hunger, can become resistant to critical hormonal signals such as leptin and insulin. As a result, the brain may behave as though the body is starving even when energy reserves are abundant, driving persistent hunger, food cravings, and reduced energy expenditure (Tan et al., 2025; Argente et al., 2025).
At the same time, chronic consumption of ultra-processed foods, sleep deprivation, gut microbiome disturbances, and hypothalamic inflammation can disrupt the delicate neural circuits that regulate appetite and reward. These biological changes help explain why obesity often behaves like a chronic relapsing disease rather than a simple lifestyle choice (Maqsood et al., 2025; Zhang et al., 2025).
Understanding obesity through the lens of brain biology represents one of the most important paradigm shifts in modern medicine. By recognizing how the brain, hormones, metabolism, and environment interact, we can move beyond blame and toward more effective, evidence-based strategies for long-term weight management and metabolic health.
1 in 8 Adults worldwide live with obesity (WHO 2024)
95% of dieters regain weight within 5 years without addressing neuroendocrine factors
2.8M Deaths annually attributable to overweight & obesity (WHO)
4 Key systems disrupted in the unified 2026 model of obesity
The Paradigm Shift: Why "Calories In, Calories Out" Is Incomplete
For most of the 20th century, obesity was treated as a simple math problem: eat less, move more, and the weight will come off. This model is not wrong — energy balance does matter — but it is radically incomplete. It is like saying that pneumonia is caused by "not enough oxygen" and that the treatment is to breathe harder.
A pivotal shift has occurred in the last decade. Leading endocrinologists, neuroscientists, and clinical researchers now recognize obesity as a disorder of the neuroendocrine system — specifically, a failure of the brain's ability to accurately sense and regulate energy stores (Argente et al., 2025; Sun et al., 2025).
This reframe matters enormously in practice. It explains:
Why weight regain after calorie restriction is so common — the brain adapts by increasing hunger and slowing metabolism
Why do some people feel genuinely hungry even after eating a full meal
Why highly processed foods can override the body's natural satiety signals
Why shame-based approaches to obesity treatment consistently fail
Key Clinical Insight According to a landmark 2025 paper in Cell Metabolism (Tan et al., 2025), leptin resistance — not simply overeating — is the central biological mechanism driving persistent weight gain and failed dieting. Treating obesity without addressing this neurological dysfunction is like treating high blood pressure by telling someone to "just relax."
The Hypothalamus: Your Brain's Metabolic Command Center
The Architecture of Hunger
The hypothalamus may be small — roughly the size of an almond — but it processes an enormous volume of metabolic information every second. At its core, the arcuate nucleus (ARC) contains two opposing sets of neurons whose balance determines whether you feel hungry or full:
Orexigenic neurons (hunger-promoting): release Neuropeptide Y (NPY) and Agouti-related peptide (AgRP), driving you to seek food
Anorexigenic neurons (satiety-promoting): release Pro-opiomelanocortin (POMC) and CART, signaling fullness and suppressing intake
These neurons act like an internal congress, constantly debating: eat or stop? Under healthy conditions, signals from circulating hormones — leptin, insulin, ghrelin, and gut peptides — keep this debate balanced. In obesity, the orexigenic side wins chronically.
The ARC sends its decisions downstream to the paraventricular nucleus (PVN) and the lateral hypothalamus, which in turn control autonomic nervous system output, cortisol release, and physical activity levels — all relevant to energy balance (Sun et al., 2025).
Novel Regulators: Raptin and Sleep Physiology
One of the most exciting discoveries in appetite neuroscience is the 2025 identification of raptin — a sleep-induced hypothalamic hormone that actively suppresses appetite and body weight. Research published in Cell Research (Xie et al., 2025) demonstrated that raptin is produced primarily during deep sleep and acts directly on hypothalamic circuits to dampen hunger signals.
The clinical implication is striking: sleep deprivation doesn't just leave you tired — it specifically shuts down a powerful neurological appetite suppressant, creating a biochemical environment that drives overeating the next day.
Hypothalamic Inflammation: The Early Lesion
Perhaps the most important paradigm-shifting finding of the last decade is that hypothalamic inflammation precedes significant weight gain. Even a few days of high-fat, high-sugar feeding triggers an innate immune response in the brain's microglia (resident immune cells), causing localized neuroinflammation (Argente et al., 2025).
This "gliosis" — the brain equivalent of an inflamed joint — disrupts the delicate signaling between POMC and NPY neurons. The hunger switch gets jammed in the "on" position. And because the inflammation itself perpetuates the dysfunction, it creates a vicious cycle that becomes harder to break over time.
"Early hypothalamic inflammation — triggered by nutrient excess — impairs neuronal plasticity and disrupts anorexigenic signaling pathways, often preceding overt weight gain." — Argente et al., The Lancet Diabetes & Endocrinology, 2025
Leptin Resistance: Why Your Brain Thinks You're Starving
What Is Leptin, and Why Does It Matter?
Leptin is the body's primary long-term energy status signal. Produced by adipose (fat) tissue in proportion to fat mass, it travels through the bloodstream to the hypothalamus, where it tells the brain: "We have enough energy stored. You can stop eating now."
Under normal physiology, this system works elegantly: more fat → more leptin → less appetite → less eating → less fat. It's a self-correcting feedback loop.
In obesity, this loop breaks down in a paradoxical way. People with obesity don't have too little leptin — they have too much. But despite sky-high leptin levels, the brain doesn't register the signal. This is leptin resistance, and it is arguably the single most important biological mechanism explaining why obesity is so hard to treat (Tan et al., 2025).
Four Mechanisms of Leptin Resistance
A landmark 2025 study in Cell Metabolism (Tan et al., 2025) mapped the cellular and molecular basis of leptin resistance with unprecedented detail. Four primary mechanisms have been identified:
Here is the information rewritten into clear, structured bullet points for better readability:
Mechanisms of Leptin Resistance
1. Impaired Transport
What Happens: Less leptin can cross the blood–brain barrier into the hypothalamus.
Result: The brain receives only a fraction of the actual leptin signal circulating in the body.
2. SOCS3 Overactivation
What Happens: Suppressor of cytokine signaling 3 (SOCS3) blocks the intracellular JAK-STAT signaling pathway inside neurons.
Result: Leptin molecules successfully reach the brain but are completely blocked from triggering a cellular response.
3. Ceramide Lipid Toxicity
What Happens: An accumulation of ceramides disrupts the normal function of the neuronal membrane.
Result: POMC (pro-opiomelanocortin) neurons become impaired, which directly drives hyperphagia (extreme overeating).
4. ER Stress
What Happens: Chronic overnutrition causes endoplasmic reticulum (ER) stress within hypothalamic neurons.
Result: Protein folding errors occur, which further impair and degrade downstream leptin signaling.The practical consequence: the hypothalamus behaves as if the body is in a state of starvation, even when fat stores are at their highest. NPY/AgRP neurons remain active, hunger persists, and metabolism slows — a metabolic illusion that makes weight loss both physiologically and psychologically exhausting.
Is Leptin Resistance Reversible?
Importantly, leptin resistance is not permanent. Evidence suggests it can be partially reversed through interventions that reduce hypothalamic inflammation:
Sustained weight loss re-sensitizes leptin receptors over time
Regular aerobic exercise reduces hypothalamic inflammation and improves leptin signaling
High-quality sleep restores hypothalamic receptor sensitivity
Reducing saturated fats and ultra-processed foods decreases ceramide accumulation in the hypothalamus (Le Stunff et al., 2025; Argente et al., 2025)
Ceramides: The Neurotoxic Fat You've Never Heard Of
Among the emerging mechanisms in obesity science, the role of ceramides deserves special attention. These bioactive sphingolipids — a class of fat molecules — accumulate in the hypothalamus when dietary saturated fat intake is chronically elevated.
A 2025 review in Reviews in Endocrine and Metabolic Disorders (Le Stunff et al., 2025) described ceramides as a critical link between overnutrition and neurological dysfunction. In the hypothalamus, ceramide accumulation:
Directly impairs POMC neuron function, removing the brain's satiety signal
Disrupts insulin signaling pathways in the brain
Promotes chronic hyperphagia (persistent overeating)
Impairs glucose homeostasis independently of peripheral insulin resistance
Think of ceramides as a kind of neurological rust — they build up slowly with chronic exposure to certain fats and sugars, corroding the machinery of appetite regulation from within. The good news: dietary changes that reduce saturated fat intake can lower ceramide levels and partially restore hypothalamic function.
Clinical Insight: Ceramides as a Biomarker? Researchers are actively investigating whether plasma ceramide levels could serve as a biomarker for hypothalamic dysfunction and leptin resistance — potentially enabling earlier, more targeted obesity interventions before significant weight gain occurs.
Reward Pathways, Dopamine, and Food Addiction Biology
The Dopamine System and Hedonic Eating
The hypothalamus regulates hunger based on the body's need for energy — this is called homeostatic eating. But humans also eat for pleasure, comfort, and habit — this is hedonic eating, and it is governed by an entirely different brain circuit.
The mesolimbic dopamine system — stretching from the ventral tegmental area (VTA) to the nucleus accumbens — evolved to reward survival behaviors: eating, sex, and social bonding. Every bite of pleasurable food triggers a dopamine release that reinforces the behavior, creating a powerful memory: "Do that again."
This system worked beautifully when food was scarce and nutritionally diverse. It is poorly adapted to the modern food environment.
How Ultra-Processed Foods Hijack the Brain
Ultra-processed foods are engineered to hit what food scientists call the "bliss point" — the optimal combination of sugar, fat, and salt that maximizes palatability and dopamine release, while bypassing natural satiety signals. Unlike whole foods, which trigger gut peptide release that gradually signals fullness, ultra-processed foods can be consumed far past satiety before the brain catches up.
A comprehensive 2025 review (Maqsood et al., 2025) found that chronic consumption of highly palatable foods leads to:
Dopamine receptor downregulation: Fewer D2 receptors mean less pleasure from the same food, driving escalating consumption
Elevated reward threshold: Normal, whole foods become comparatively less rewarding — "broccoli doesn't taste like anything anymore"
Behavioral reinforcement loops that closely mirror those seen in substance use disorders
Is Food Addiction Real?
The concept of food addiction remains debated in academic circles, but the neurobiological evidence is increasingly compelling. The same brain regions, the same receptor changes, and the same behavioral patterns that characterize alcohol or cocaine addiction are observed in individuals with compulsive overeating of ultra-processed foods (Maqsood et al., 2025).
❌ Common Belief"Food addiction is just an excuse for lack of willpower."
✅ The ScienceDopamine receptor downregulation from chronic hyper-palatable food exposure creates genuine neuroadaptive changes identical to substance addiction pathways.
This does not mean that everyone who overeats is "addicted" to food, but it does mean that treating compulsive overeating requires addressing the neurological changes driving it — not simply telling someone to eat less.
The Gut–Brain Axis: Your Microbiome's Role in Appetite
The gut and brain are in constant two-way communication via the vagus nerve, enteric nervous system, and a rich array of signaling molecules. The trillion-strong community of microorganisms in your gut — the microbiome — plays an increasingly recognized role in this dialogue.
A 2025 review in the Journal of Diabetes Investigation (Zhang et al., 2025) outlined the key mechanisms by which gut microbiota influence obesity and appetite:
Short-chain fatty acids (SCFAs): Beneficial bacteria ferment dietary fiber into butyrate, propionate, and acetate. These SCFAs cross the blood–brain barrier and modulate hypothalamic NPY/AgRP activity — essentially, they carry the "I'm full" message from the gut to the brain
Bile acid signaling: Microbiota-modified bile acids activate receptors in both the gut and brain that influence satiety and energy expenditure
Inflammatory mediators: A dysbiotic microbiome (disrupted by ultra-processed food, antibiotics, or low-fiber diets) produces lipopolysaccharides that trigger systemic inflammation — which in turn worsens leptin resistance
In practical terms, a diet rich in diverse plant fibers feeds the beneficial bacteria that keep this communication clear. A diet heavy in ultra-processed foods creates static on the line — the "I'm full" message never reaches the brain reliably.
⚠ Important Note: Probiotic supplements alone are unlikely to reverse obesity-related gut dysbiosis. The evidence strongly favors dietary change — particularly increased fiber intake from diverse plant sources — as the most effective way to restore beneficial microbiota composition.
Sleep Deprivation as a Metabolic Disruptor
Most people know that poor sleep makes them feel worse. Fewer people know that it fundamentally alters their hormonal environment in ways that almost guarantee overeating the next day.
Sleep deprivation disrupts appetite regulation through multiple simultaneous mechanisms:
Raptin suppression: The newly identified hypothalamic hormone raptin — which suppresses appetite and promotes energy expenditure — is primarily secreted during deep sleep. Even partial sleep restriction significantly reduces raptin output (Xie et al., 2025)
Ghrelin elevation: The "hunger hormone" ghrelin rises significantly with sleep loss, driving cravings for calorie-dense, high-sugar foods
Leptin reduction: Even a few nights of poor sleep decrease circulating leptin, compounding the satiety deficit
Endocannabinoid system activation: Sleep loss activates the endocannabinoid system in ways that enhance the rewarding properties of food — the equivalent of physiological "munchies"
The combined result: after a bad night's sleep, you will be hormonally primed to consume roughly 300–400 additional calories the next day, according to controlled research. This is not a character flaw. It is biochemistry.
Body Weight Set Point Theory: Why Weight Regain Is So Common
One of the most important concepts in modern obesity research is the body weight set point theory. According to this model, the brain—particularly the hypothalamus—defends a biologically preferred range of body fat and body weight. When weight falls below this defended level, powerful compensatory mechanisms are activated to restore lost weight.
This phenomenon is known as defended adiposity. In many individuals with obesity, chronic leptin resistance, hypothalamic inflammation, and neuroendocrine dysfunction may cause the brain to defend a higher-than-normal level of body fat. As a result, weight loss is often met with increased hunger, reduced satiety, and a decline in energy expenditure.
An alternative but related concept is the settling point theory, which proposes that body weight is not regulated by a fixed biological set point alone. Instead, weight "settles" at the level determined by the interaction between genetics, appetite regulation, food environment, physical activity, sleep, stress, and metabolic health. Modern environments rich in ultra-processed foods may shift this settling point upward over time.
A key mechanism underlying weight regain is adaptive thermogenesis. After weight loss, the body often burns fewer calories than expected for its new size. Resting metabolic rate declines, movement efficiency improves, and hunger-promoting hormones increase. This metabolic adaptation can persist for months or even years, making long-term weight maintenance challenging.
Together, set point theory, settling point theory, and adaptive thermogenesis help explain why obesity is more than a simple calorie imbalance. They reinforce the modern view that obesity is a chronic neuroendocrine condition in which the brain actively defends body weight, often resisting efforts to lose and maintain weight loss.
The 2026 Unified Neuroendocrine Model of Obesity
Modern obesity can be understood as a four-system communication breakdown that becomes self-reinforcing over time. Each disrupted system feeds back into the others, creating a biological lock that simple calorie restriction cannot reliably open.
The Breakdown of Obesity's Communication Loop
1. Hypothalamic System (The Command Center)
Primary Dysfunction: Impaired energy sensing and neuroinflammation (brain inflammation).
Clinical Impact: Creates a persistent biological drive to eat and an inability to accurately register fullness.
2. Hormonal System (The Signaling Network)
Primary Dysfunction: Leptin resistance and insulin resistance.
Clinical Impact: The brain completely ignores "I'm full" signals, causing a perception of internal starvation despite having adequate energy stores.
3. Reward System (The Hedonic Drive)
Primary Dysfunction: Dopamine receptor downregulation (fewer active pleasure receptors).
Clinical Impact: Drives compulsive overeating of ultra-processed foods, while reducing the pleasure derived from whole foods.
4. Peripheral Metabolism (The Target Organs)
Primary Dysfunction: Metabolic dysfunction-associated steatotic liver disease (MAFLD), systemic insulin resistance, and ceramide lipid accumulation.
Clinical Impact: Generates a pro-inflammatory environment that feeds back to the hypothalamus, perpetually restarting and reinforcing the cycle.
The 2025 Liver-Brain Connection (Cao et al., 2025):
Fatty liver disease (MAFLD) plays an aggressive role in this cycle. It amplifies systemic inflammation and disrupts lipid metabolism, which directly damages hypothalamic function. This creates a destructive feedback loop between peripheral organ damage and central appetite dysregulation.
Takeaway:
"Obesity isn't a single problem — it's a 'communication breakdown' between your brain's hunger switch, your hormones, your pleasure centers, and your liver. When these four systems stop talking to each other properly, your body defaults to storing fat rather than burning it."
Evidence Summary: Key 2025–2026 Studies
Here is the recent research evidence broken down into clear, structured bullet points, organized by the study's overall impact:
High-Quality Studies (Major Breakthroughs & Pathophysiology)
Leptin Resistance Mechanisms (Tan et al., 2025 | Cell Metabolism)
Finding: Uncovered the precise cellular and molecular foundations of leptin resistance, pinning it on SOCS3 overactivation, ceramide accumulation, ER stress, and impaired transport across the blood–brain barrier.
Obesity as a Brain Disorder (Argente et al., 2025 | Lancet Diabetes & Endocrinology)
Finding: Proved that hypothalamic inflammation actually precedes weight gain, firmly establishing obesity as a primary neuroendocrine disorder rather than just a metabolic consequence.
Discovery of "Raptin" (Xie et al., 2025 | Cell Research)
Finding: Discovered a brand-new, sleep-induced hypothalamic hormone named raptin that actively suppresses appetite and counteracts obesity.
The Ceramide Effect (Le Stunff et al., 2025 | Rev. Endocrine Metab. Disorders)
Finding: Demonstrated that the accumulation of ceramides (toxic lipids) in the hypothalamus directly impairs both glucose balance and leptin signaling.
The Liver-Brain Loop (Cao et al., 2025 | Clinical & Translational Medicine)
Finding: Showed that metabolic dysfunction-associated steatotic liver disease (MAFLD) releases systemic inflammatory signals that worsen hypothalamic dysfunction, creating a destructive feedback loop.
Gut-Brain Signaling (Zhang et al., 2025 | J. Diabetes Investigation)
Finding: Found that short-chain fatty acids (SCFAs) produced by gut microbiota directly modulate appetite signaling in the hypothalamus via the vagus nerve.
Systems Review (Sun et al., 2025 | Frontiers in Nutrition)
Finding: Provided a comprehensive, high-quality systems review detailing the interconnected neural and hormonal mechanisms that regulate human appetite.
Moderate-Quality Studies (Emerging & Specialized Research)
Food Addiction & Dopamine (Maqsood et al., 2025 | Food Science & Nutrition)
Finding: Highlighted the neurobiological overlap between food addiction and substance use disorders, driven heavily by the downregulation of D2 dopamine receptors.
Future Treatment Frontiers (Tiwari et al., 2026 | Biological Rhythm Research)
Finding: Evaluated emerging neuroendocrine and cutting-edge neurotechnological approaches for the future treatment of obesity.
The Role of Oxytocin (Liu et al., 2026 | Clinical Endocrinology)
Finding: Identified that oxytocinergic pathways play a significant, distinct neuroendocrine role in how the body regulates obesity.
Cognitive and Mental Health Impacts (Mugisha, 2026 | IDOSR J. Experimental Sciences)
Finding: Demonstrated that obesity-driven neuroinflammation spreads beyond appetite centers, accelerating cognitive decline and increasing psychiatric comorbidities.
Common Myths and Mistakes About Obesity
❌ Myth: Obesity is caused by laziness and lack of discipline.
✅ Fact: Obesity is a neuroendocrine disorder. Leptin resistance, hypothalamic inflammation, and dopamine dysfunction drive overeating at a biological level independent of willpower.
❌ Myth: If you just eat less and move more, weight will stay off.
✅ Fact: Caloric restriction triggers compensatory increases in hunger hormones and metabolic slowdown. Without addressing leptin resistance and reward circuit dysfunction, weight regain is the biologically expected outcome.
❌ Myth: All calories are equal — a calorie of broccoli is the same as a calorie of cookies.
✅ Fact: Ultra-processed foods trigger far greater dopamine release, faster gastric emptying, weaker gut peptide satiety signals, and blood sugar volatility — making them neurologically and metabolically distinct from whole foods of equivalent caloric value.
❌ Myth: Sleep is a luxury — you can function fine on 5–6 hours.
✅ Fact: Even modest sleep restriction suppresses raptin, elevates ghrelin, and reduces leptin — creating a hormonal profile almost identical to deliberate caloric restriction, but in the direction of increased appetite and fat storage.
❌ Myth: Probiotics can fix your gut and help you lose weight.
✅ Fact: While the gut–brain axis is real and important, evidence for probiotic supplements as an obesity treatment remains weak. Dietary fiber diversity is the most evidence-based way to support a healthy microbiome.
Evidence-Based Treatment Protocol: A Multimodal Approach
Given that obesity involves dysregulation across at least four interconnected biological systems, effective treatment must be multimodal — targeting the hypothalamus, hormonal signaling, reward circuits, and peripheral metabolism simultaneously.
1 Sleep Optimization
7–9 hours per night. Supports raptin secretion, normalizes ghrelin/leptin balance, and improves hypothalamic leptin sensitivity.
2 Protein & Fiber Priority
1.2–1.6 g protein/kg/day + 30+ g fiber. Maximises satiety signaling via POMC/CART activation and gut–brain axis function.
3 Ultra-Processed Food Reduction
Reduce UPF to <10% of calories. Allows dopamine receptor recovery and natural appetite threshold restoration.
4 Aerobic Exercise
150+ min/week moderate intensity. Reduces hypothalamic inflammation, improves leptin sensitivity, enhances BDNF for neuroplasticity.
5 Pharmacotherapy
GLP-1 receptor agonists (semaglutide, tirzepatide) work centrally to suppress appetite and peripherally to improve insulin sensitivity.
6 Behavioral Support
Cognitive behavioral strategies to manage food environment, emotional triggers, and compulsive eating patterns driven by reward dysfunction.
Anti-Inflammatory Nutrition: Targeting the Hypothalamus
Given the role of hypothalamic inflammation in initiating and sustaining leptin resistance, an anti-inflammatory dietary pattern is not merely beneficial — it is mechanistically targeted treatment. Key elements include:
Omega-3 fatty acids (EPA/DHA from oily fish or algae) — reduce microglial activation in the hypothalamus
Extra-virgin olive oil — polyphenols reduce ceramide synthesis and neuroinflammation
Diverse colored vegetables — antioxidants counter oxidative stress from overnutrition
Fermented foods (yogurt, kefir, kimchi) — support SCFA-producing microbiota and gut–brain signaling
Minimizing saturated fats from ultra-processed sources reduces ceramide accumulation in the hypothalamus
Limiting refined sugars and high-fructose corn syrup prevents blood–brain barrier inflammation
Pharmacological Approaches: The 2026 Landscape
The most significant advance in obesity pharmacotherapy is the validation that GLP-1 receptor agonists (semaglutide, tirzepatide) work primarily through central mechanisms — they activate receptors in the hypothalamus, brainstem, and reward circuits to reduce appetite, slow gastric emptying, and improve leptin sensitivity. They do not simply make you feel nauseous — they genuinely recalibrate the neuroendocrine set point for body weight.
Emerging targets in 2026 research include oxytocin receptor agonists (Liu et al., 2026) and novel hypothalamic neuropeptide analogs that may offer more targeted approaches with fewer systemic side effects (Tiwari et al., 2026).
⚠ Medical DisclaimerThis article is for educational purposes only. Pharmacological treatment for obesity should always be prescribed and monitored by a qualified healthcare professional. Individual responses to medications vary, and treatment must be personalized to your specific medical history, comorbidities, and goals.
Faqs
Is obesity truly a brain disease, or is it mainly a metabolic issue?
Obesity is both a metabolic and neuroendocrine disorder, but modern research increasingly recognizes the central role of the brain. The hypothalamus regulates hunger, satiety, and energy expenditure through complex hormonal signals. In obesity, leptin resistance, hypothalamic inflammation, and reward-circuit dysfunction impair the brain's ability to accurately regulate body weight, leading to persistent hunger and weight regain despite adequate energy stores (Argente et al., 2025; Tan et al., 2025).
Why do I feel hungry immediately after eating a large meal?
Persistent hunger after eating may occur when the brain fails to properly interpret satiety signals. Leptin resistance, insulin resistance, inadequate protein intake, rapid consumption of ultra-processed foods, poor sleep, and disruptions in gut-derived hormones such as GLP-1 and peptide YY can all contribute to continued hunger despite sufficient caloric intake (Sun et al., 2025).
Can leptin resistance be reversed?
Leptin resistance appears to be partially reversible. Sustained weight loss, regular physical activity, improved sleep quality, reduction in ultra-processed foods, and anti-inflammatory dietary patterns can improve leptin signaling and hypothalamic function over time. However, recovery is often gradual and varies among individuals (Tan et al., 2025).
Are ultra-processed foods genuinely addictive?
While food addiction remains scientifically debated, growing evidence suggests that ultra-processed foods can trigger neurobiological changes similar to those seen in substance use disorders. Chronic exposure may reduce dopamine receptor sensitivity, increase cravings, and reinforce compulsive eating behaviors, particularly in susceptible individuals (Maqsood et al., 2025).
How does sleep deprivation cause weight gain?
Sleep deprivation alters several appetite-regulating hormones. It increases ghrelin, decreases leptin, suppresses the sleep-associated hormone raptin, and enhances activity within reward pathways. These changes promote hunger, cravings for calorie-dense foods, and increased caloric intake the following day (Xie et al., 2025).
What is the gut–brain axis and how does it affect my weight?
The gut–brain axis is a bidirectional communication network linking the gastrointestinal tract, microbiome, vagus nerve, immune system, and brain. Beneficial gut bacteria produce metabolites such as short-chain fatty acids that influence appetite regulation and energy balance. Disruptions in this system can promote inflammation, leptin resistance, and overeating (Zhang et al., 2025).
What role do GLP-1 receptor agonists play in treating neuroendocrine obesity?
GLP-1 receptor agonists such as semaglutide and tirzepatide work by targeting both the brain and peripheral metabolism. They reduce appetite, enhance satiety, slow gastric emptying, improve insulin sensitivity, and influence reward pathways involved in food intake. Their effectiveness supports the concept that obesity is fundamentally a neuroendocrine disorder rather than simply a problem of excess calorie consumption.
What emerging treatments are on the horizon for 2026 and beyond?
Researchers are investigating novel therapies targeting leptin sensitization, hypothalamic inflammation, oxytocin pathways, gut-derived hormones, and neurotechnological approaches that directly modulate appetite-regulating brain circuits. These precision therapies may allow treatment to be tailored to the specific biological drivers of obesity in individual patients (Tiwari et al., 2026; Liu et al., 2026).
How does obesity affect cognitive function and mental health?
Chronic obesity is associated with systemic inflammation, insulin resistance, vascular dysfunction, and neuroinflammation. These processes may increase the risk of cognitive decline, depression, anxiety, and impaired executive function. Emerging evidence suggests that obesity-related inflammation can adversely affect brain health long before neurological symptoms become apparent (Mugisha, 2026).
Is childhood obesity different from adult obesity neurologically?
Yes. Childhood obesity occurs during critical periods of brain development and may produce long-lasting changes in hypothalamic circuitry, reward processing, and appetite regulation. Early-life exposure to excessive nutrition, maternal obesity, and ultra-processed foods may influence lifelong body-weight regulation, making prevention during childhood particularly important.
Conclusion: Treating the Brain, Not Just the Body
The science of obesity has been fundamentally transformed. What was once understood as a simple imbalance of intake versus expenditure is now recognized as a complex, multi-system neuroendocrine disorder — one that begins in the brain, is sustained by hormonal dysregulation, and is amplified by the modern food environment.
Leptin resistance explains why hunger persists despite adequate calories. Hypothalamic inflammation explains why the problem compounds over time. Dopamine dysfunction explains the compulsive pull of ultra-processed foods. And the gut–brain axis explains why what you eat affects not just your gut, but your brain's ability to regulate itself.
This understanding has three critical implications for clinicians and patients alike:
Stop blaming willpower. Persistent hunger in obesity is a symptom of neurological dysfunction — as real and involuntary as the chest pain of cardiac disease.
Treat the brain first. Sleep optimization, anti-inflammatory nutrition, exercise, and behavioral strategies targeting reward circuits are not lifestyle "add-ons" — they are mechanistically targeted treatments.
Use the full pharmacological toolkit. GLP-1 receptor agonists and emerging neuroendocrine therapies offer the most evidence-based path to recalibrating a dysregulated appetite system when lifestyle changes alone are insufficient.
The future of obesity medicine lies in precision neuroendocrinology — matching the right intervention to the right biological mechanism in the right patient. That future is not far off. But it starts with accepting the biological reality of what obesity actually is.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Managing Diabesity: A Complete Guide to Weight Loss and Blood Sugar Control | DR T S DIDWAL
Weight Loss as Immunotherapy: The Science Behind Reversing Chronic Inflammation | DR T S DIDWAL
Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health | DR T S DIDWAL
References
Argente, J., Farooqi, I. S., Chowen, J. A., Kühnen, P., López, M., Morselli, E., et al. (2025). Hypothalamic obesity: From basic mechanisms to clinical perspectives. The Lancet Diabetes & Endocrinology. Advance online publication. https://doi.org/10.1016/S2213-8587(24)00283-3
Cao, Y., Liu, Z., Zhang, H., Wang, X., & Li, S. (2025). Metabolic dysfunction–associated fatty liver disease and its cardiometabolic implications. Clinical and Translational Medicine. Advance online publication. https://doi.org/10.1016/j.s2049-3614(25)00142-x
Cassataro, M. A., et al. (2026). Dual incretin therapies in obesity: Mechanisms and clinical outcomes. Diabetes, Obesity and Metabolism. Advance online publication.
Caturano, A., et al. (2025). Beyond weight loss: Neuroendocrine effects of GLP-1 receptor agonists. Endocrine Reviews. Advance online publication.
Le Stunff, H., Brasilio Villalta, P., & Magnan, C. (2025). Hypothalamic ceramide metabolism in obesity and dysregulation of glucose homeostasis. Reviews in Endocrine and Metabolic Disorders. Advance online publication. https://doi.org/10.1007/s11154-025-10003-8
Liu, X., Chen, Y., Huang, Y., Xiao, X., & Zhong, X. (2026). The neuroendocrine role of oxytocinergic pathways in obesity. Clinical Endocrinology, 104, 556–566. https://doi.org/10.1111/cen.70111
Maqsood, S., Ahmed, F., Arshad, M. T., Ikram, A., & Abdullahi, M. A. (2025). Comparative analysis of food addiction and obesity: A critical review. Food Science & Nutrition, 13(8), e70799. https://doi.org/10.1002/fsn3.70799
Mugisha, E. K. (2026). Obesity and neuroinflammation: Mechanisms, evidence, and implications for health. IDOSR Journal of Experimental Sciences, 12(1), 20–27. https://doi.org/10.59298/IDOSR/JES/06/1212027
Sun, X., Liu, B., Yuan, Y., Rong, Y., Pang, R., & Li, Q. (2025). Neural and hormonal mechanisms of appetite regulation during eating. Frontiers in Nutrition, 12, Article 1484827. https://doi.org/10.3389/fnut.2025.1484827
Tan, B., Hedbacker, K., Kelly, L., Zhang, Z., Moura-Assis, A., Luo, J. D., et al. (2025). A cellular and molecular basis of leptin resistance. Cell Metabolism, 37(3), 723–737. https://doi.org/10.1016/j.cmet.2025.01.001
Tiwari, G., Mundada, A. B., Mundada, P. A., Maheshwari, R., Singh, S., Kumar, R., et al. (2026). Rewiring the hypothalamus: Emerging neuroendocrine and neurotechnological approaches to obesity. Biological Rhythm Research, 1–30. Advance online publication. https://doi.org/10.1080/09291016.2026.2635609
World Health Organization. (2024). Obesity and overweight: Key facts. WHO Global Health Observatory.
Xie, L. Q., Hu, B., Lu, R. B., et al. (2025). Raptin, a sleep-induced hypothalamic hormone, suppresses appetite and obesity. Cell Research, 35, 165–185. https://doi.org/10.1038/s41422-025-01078-8
Zhang, Y., Liu, X., Wang, Y., Li, M., Chen, H., & Sun, Q. (2025). Gut microbiota–derived metabolites and metabolic diseases: Mechanisms and therapeutic implications. Journal of Diabetes Investigation. Advance online publication. https://doi.org/10.1016/j.jdiacomp.2025.100008