Muscle Loss and Cardiovascular Disease: The Overlooked Connection You Need to Know
Discover the emerging science linking muscle loss with heart disease and declining cardiorespiratory fitness. Evidence-based strategies for prevention, early detection, exercise, and nutrition.
SARCOPENIAHEART
Dr. T.S. Didwal, M.D. {Internal Medicine}.
5/5/202613 min read
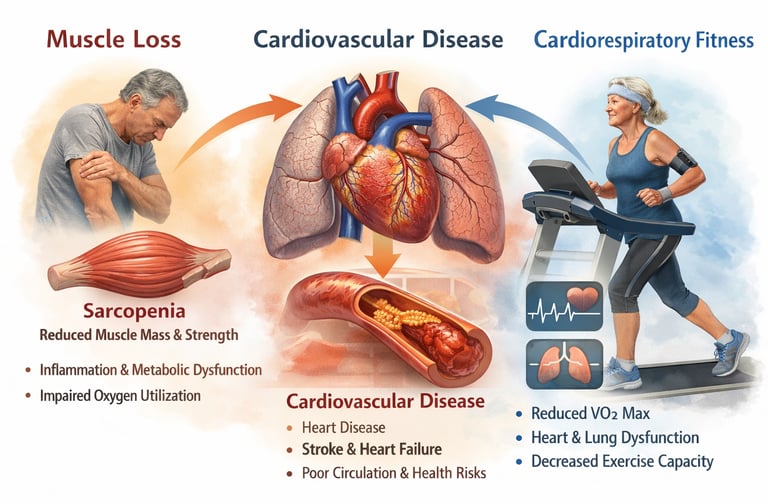
Sarcopenia (age-related muscle loss) is now recognized as an independent cardiovascular risk factor. Emerging evidence from 2025–2026 shows that reduced muscle mass and strength are strongly associated with higher risks of heart disease, stroke, heart failure, and premature death—independent of traditional risk factors like hypertension, diabetes, or obesity.
Randomized controlled trials show that resistance and combined exercise training significantly improve muscle mass, insulin sensitivity, and cardiorespiratory fitness, with parallel reductions in key cardiovascular risk markers. These findings support a causal, modifiable link between improving muscle health and lowering cardiometabolic risk.
Skeletal muscle is not just for movement—it is a metabolic and cardiovascular organ. When muscle declines, multiple systems that protect the heart begin to fail.
Why Muscle Loss Increases Heart Risk
Research across meta-analyses and cohort studies shows that sarcopenia contributes to cardiovascular disease through several interconnected mechanisms:
↓ VO₂ max (cardiorespiratory fitness): Less muscle reduces oxygen utilization, a major predictor of survival
Insulin resistance: Muscle is the primary site for glucose disposal
Chronic inflammation: Elevated IL-6 and TNF-α accelerate atherosclerosis
Mitochondrial dysfunction: Reduced energy production and increased oxidative stress
Cardiac deconditioning: Lower demand leads to reduced cardiac efficiency
Large-scale data (e.g., NHANES analyses and longitudinal cohorts) confirm that muscle loss predicts cardiovascular events even after adjusting for obesity and lifestyle factors.
Who Is at Risk?
Adults >60 years (risk rises sharply with age)
Individuals with a sedentary lifestyle, diabetes, or chronic disease
Those with unintentional weight loss or reduced strength
Early decline often begins in the mid-30s, long before symptoms appear.
Early Warning Signs
Difficulty rising from a chair
Reduced grip strength
Fatigue or breathlessness with mild activity
Slower walking speed
Loss of muscle mass or unexplained weight loss
Muscle health is cardiovascular health.
Preventing or reversing sarcopenia is not just about strength or mobility—it is a powerful, modifiable strategy to reduce cardiovascular risk and improve longevity.
Sarcopenia increases cardiovascular risk independently of traditional factors
Muscle loss drives insulin resistance, inflammation, and reduced fitness
Strength training + adequate protein are the most effective interventions
Early detection using simple clinical tests can prevent long-term complications
What Is Sarcopenia — and Why Should Your Cardiologist Care?
Sarcopenia (from the Greek sarx, flesh, and penia, poverty) is defined as the progressive, generalized loss of skeletal muscle mass, strength, and physical performance. It is not merely feeling weak with age. It is a clinically measurable condition with its own diagnostic criteria, measurable biomarkers, and now — a well-established cardiovascular risk profile.
While the condition typically accelerates after age 60, muscle mass quietly declines from your mid-thirties onward. By the time most people notice symptoms, years of subclinical loss have already occurred. The condition affects roughly 10% of adults over 60, rising sharply to nearly half of those in their eighties.
For decades, sarcopenia was treated as a mobility and falls issue — something orthopedic teams and physiotherapists dealt with. The stunning re-framing offered by the 2025–2026 literature is this: sarcopenia belongs on the cardiology agenda, right alongside hypertension, dyslipidemia, and diabetes. A landmark editorial by Hanon (2025) in the European Journal of Preventive Cardiology explicitly argues that sarcopenia deserves recognition as a new cardiovascular risk factor, calling for systematic screening and integrated cardiac-muscle management protocols.
What the 2025–2026 Research Actually Found
Six major peer-reviewed studies and expert statements now form the backbone of our understanding. Let us walk through each one clearly.
Sarcopenia and Risk of Cardiovascular Events and Mortality
Wang et al. (2026) conducted the most comprehensive meta-analysis to date, pooling data from longitudinal observational studies. Their findings confirmed that individuals with sarcopenia face a significantly elevated risk of major cardiovascular events and all-cause mortality. The dose-response relationship was clear: greater muscle loss predicted worse cardiac outcomes, independent of traditional risk factors like age, blood pressure, and cholesterol levels.:
Greater severity of sarcopenia is dose-dependently associated with higher cardiovascular events and mortality, independent of traditional risk factors.
Sarcopenia as an Independent CVD Risk Factor
Yu et al. (2025) analysed data from the U.S. National Health and Nutrition Examination Survey — one of the most representative health databases in the world. Using this large, rigorously collected sample, they confirmed sarcopenia as an independent risk factor for coronary artery disease, heart failure, and stroke. Critically, the association held even after controlling for obesity, diabetes, and sedentary behaviour, signalling that muscle loss carries its own cardiovascular danger signal.
Sarcopenia acts as an independent cardiovascular risk factor, even after adjusting for obesity, diabetes, and physical inactivity.
Lean Mass Trajectories and Cardiovascular Risk
Liu et al.(2026) took a dynamic, longitudinal approach by tracking changes in predicted lean mass over time rather than taking a single snapshot. Their prospective cohort study demonstrated that individuals whose lean mass trajectories declined over follow-up carried a substantially higher cardiovascular disease risk — emphasising that the direction of change matters as much as current muscle mass. Maintaining or building lean mass was protective; losing it was a warning signal measurable years before cardiac events occurred.
Declining lean mass over time (trajectory) predicts cardiovascular risk more strongly than a single baseline measurement.
Long-Term Burden of Sarcopenia and Cardiorespiratory Multimorbidity
Lu et al. (2025) examined what happens when sarcopenia persists over time rather than appearing briefly. Their study in The Journal of Nutrition, Health & Aging found that sustained sarcopenia — measured by its severity and duration — dramatically increases the risk of cardiorespiratory multimorbidity: the simultaneous presence of multiple heart and lung conditions. The takeaway was striking: the longer muscle loss goes unaddressed, the more the entire cardiovascular-respiratory unit degrades together
Chronic, persistent sarcopenia amplifies cardiorespiratory multimorbidity, with risk increasing with duration and severity
Getting to the Heart of Sarcopenia and CVD
Nezafati, P. et al. (2025) published a comprehensive mechanistic review in Ageing that maps the precise biological pathways through which muscle loss translates into cardiovascular damage. Their analysis covered mitochondrial dysfunction, pro-inflammatory cytokine release, metabolic dysregulation, autonomic nervous system changes, and endothelial dysfunction — providing the mechanistic explanation for why the epidemiological associations above are not coincidental but causal.
Sarcopenia contributes to cardiovascular disease through multiple causal biological pathways, including inflammation, mitochondrial dysfunction, and metabolic dysregulation.
Lean Body Mass and Hypertensive Cardiovascular Phenotype
Gunawardana et al.(2025) introduced an important nuance: the cardiovascular consequences of lean body mass may differ by sex. Their research found that lower lean body mass was associated with a hypertensive cardiovascular phenotype — elevated blood pressure, increased left ventricular mass, and stiffer arteries — specifically in men but not in women at the same muscle mass levels. This suggests that cardiovascular screening and intervention thresholds may need to be sex-tailored in future guidelines.
Low lean mass is linked to a hypertensive cardiovascular phenotype primarily in men, suggesting sex-specific risk thresholds.
How Exactly Does Muscle Loss Damage Your Heart?
Understanding the mechanisms transforms sarcopenia from an abstract statistic into something you can visualise — and motivates you to prevent it. The pathways are multiple and interconnected.
Reduced Oxygen Utilisation & VO2 Max Decline
Muscles are the primary consumers of oxygen during activity. Less muscle mass means lower VO2 max — the single strongest predictor of long-term survival. Your heart and lungs become undertrained.
Cardiac Deconditioning
When less muscle demands blood flow, the heart is challenged less. Like any muscle it atrophies from under-use, becoming less efficient. Cardiac output capacity shrinks silently.
Respiratory Muscle Weakness
The diaphragm and intercostal muscles are skeletal muscles too. Sarcopenia weakens them, reducing lung capacity and making every breath require more effort — a hidden driver of breathlessness.
Metabolic Dysfunction
Muscle is the body's primary site of glucose disposal. Loss of muscle mass drives insulin resistance, dyslipidaemia, and metabolic syndrome — all established cardiovascular risk multipliers.
Chronic Systemic Inflammation
Sarcopenic muscle releases excess pro-inflammatory cytokines (IL-6, TNF-α) that damage arterial walls, accelerate atherosclerosis, and impair cardiac function over time.
Mitochondrial Dysfunction
Fewer, less functional mitochondria in sarcopenic muscle mean reduced aerobic capacity, increased oxidative stress, and impaired energy production — accelerating cardiovascular ageing.
Nezafati et al. (2025) documented how these pathways converge into a self-reinforcing cycle: reduced physical capacity leads to inactivity, which worsens inflammation and metabolic dysfunction, which further accelerates muscle loss. Breaking this cycle early is the key clinical challenge.
Recognising the Warning Signs — Early Detection Saves Lives
Sarcopenia rarely announces itself dramatically. It creeps in gradually, often mistaken for "just getting older." Knowing what to watch for — in yourself or someone you care for — can prompt life-changing early intervention.
Muscle & Strength Signals
Difficulty rising from a chair without using your arms
Reduced grip strength — struggling with jars, bags, or handshakes
Unexplained reduction in muscle definition or body weight
Feeling weaker during activities that used to feel easy
Recurrent falls or near-falls
Cardiorespiratory Signals
Getting winded climbing one flight of stairs
Needing more rest during walks than a year ago
Disproportionate fatigue after light physical effort
Longer recovery after exercise than previously
Reduced tolerance for aerobic activities you enjoyed before
If any combination of these warning signs is present — especially alongside cardiovascular risk factors such as hypertension, diabetes, or a family history of heart disease — raise the question of sarcopenia screening with your doctor. Objective tests include grip-strength dynamometry, a simple five-times chair-stand test, gait speed assessment, DEXA body composition scanning, and cardiopulmonary exercise testing for VO2 max.
The Evidence-Based Action Plan: What You Can Do Starting Today
This is where research empowers rather than alarms. The European Association of Preventive Cardiology's 2025 Scientific Statement, led by Cornelissen et al., and the expert consensus from Moretti et al. (2025) give us a clear, safe, and practical roadmap — one that is effective even for people who already have cardiovascular disease.
Your Practical Action Plan
Based on the 2025–2026 consensus evidence, here is what works — concretely and measurably.
Resistance Training (Non-Negotiable)
2–3 sessions per week targeting all major muscle groups
Progressive overload: gradually increase weights or resistance
Bodyweight squats, push-ups, and planks are valid starting points
Resistance bands are excellent for beginners and cardiac patients
Moretti et al. (2025): start before significant loss occurs for best results
Aerobic Exercise for Heart-Lung Health
150 minutes of moderate aerobic activity per week, minimum
Brisk walking, swimming, cycling, or dancing all qualify
HIIT (short intense bursts + recovery) is superior for VO2 max gains
Aerobic exercise strengthens the heart and improves lung capacity
Combine with resistance training for the gold-standard outcome
Protein Strategy — Timing Matters
Target 1.2–1.5 g of protein per kg body weight daily
Distribute protein across all meals — not just dinner
Quality sources: lean meats, fish, eggs, dairy, legumes, tofu
Post-exercise protein window (within 30–60 min) enhances synthesis
Vitamin D, omega-3s, and antioxidants provide complementary support
Lifestyle Pillars
Sleep 7–9 hours nightly — muscle repair is largely nocturnal
Break prolonged sitting every 30–45 minutes with movement
Manage chronic conditions: diabetes and hypertension accelerate muscle loss
Control stress — cortisol is catabolic (muscle-destroying) when chronically elevated
Mediterranean-style dietary pattern benefits both muscle and arteries
Special Note for Cardiac Patients
Resistance training and aerobic exercise are safe and beneficial even with established heart disease — when supervised appropriately (Cornelissen et al., 2025)
Always consult your cardiologist before beginning a new exercise programme
Cardiac rehabilitation programmes are the ideal setting to integrate sarcopenia management
Begin gradually — progress is the goal, not speed
Monitor for chest pain, severe breathlessness, or dizziness during exercise
Cardiopulmonary exercise testing can establish your baseline VO2 max and track improvements safely
Frequently Asked Questions
1. At what age should I start worrying about sarcopenia and heart risk?
Muscle mass begins to decline as early as your mid-30s, but clinically significant sarcopenia becomes more common after age 60. However, cardiovascular risk linked to muscle loss can start much earlier. Preventive strategies—especially resistance training and adequate protein intake—should ideally begin in midlife to reduce long-term cardiometabolic risk.
2. Can sarcopenia actually cause heart attacks or strokes?
Sarcopenia does not directly “cause” a heart attack, but it significantly increases risk. Studies show that muscle loss promotes insulin resistance, chronic inflammation, endothelial dysfunction, and reduced cardiorespiratory fitness—all of which are established drivers of atherosclerosis, heart failure, and stroke. This makes sarcopenia an independent and clinically relevant cardiovascular risk factor.
3. How much protein do I really need, and does timing matter?
Most adults aiming to preserve or build muscle should consume 1.2–1.5 g/kg/day of protein, especially after age 50. Distributing protein evenly across meals (rather than consuming most at dinner) improves muscle protein synthesis. Consuming protein within 30–60 minutes after resistance exercise may further enhance muscle repair and growth.
4. I have heart disease. Is resistance training safe for me?
Yes—when appropriately prescribed. Current cardiology guidelines support resistance training as safe and beneficial for most patients with stable cardiovascular disease. It improves muscle strength, functional capacity, and metabolic health. Ideally, training should begin under supervision (e.g., cardiac rehabilitation), with gradual progression and monitoring for symptoms.
5. Does sarcopenia affect men and women differently in terms of heart risk?
Emerging evidence suggests there may be sex-specific differences. Some studies indicate that low lean mass is more strongly associated with hypertensive cardiovascular changes in men, while women may have different thresholds or protective factors. However, both men and women experience increased overall cardiovascular risk when muscle mass and strength decline.
6. What tests should I ask my doctor for if I suspect sarcopenia?
Simple, validated screening tools include:
Grip strength measurement
Five-times chair stand test
Gait speed assessment
For more detailed evaluation:
DEXA scan (body composition)
Bioimpedance analysis
Cardiopulmonary exercise testing (VO₂ max)
These help assess both muscle health and cardiovascular fitness.
7. Can sarcopenia be reversed, and will that reduce heart risk?
Yes—especially in early and moderate stages. Resistance training combined with adequate protein intake can significantly improve muscle mass and strength. Evidence shows that improving muscle health enhances insulin sensitivity, reduces inflammation, and improves cardiorespiratory fitness—key pathways that lower cardiovascular risk.
Sarcopenia is modifiable and clinically actionable. Early detection and targeted lifestyle interventions can simultaneously improve muscle health and reduce cardiovascular disease risk.
Clinical Pearls
1. The "Metabolic Sink" Principle
Scientific Perspective: Skeletal muscle is the body’s primary site for glucose disposal and insulin-mediated metabolism. Sarcopenia reduces this "metabolic sink," leading to insulin resistance and systemic inflammation ($IL-6$ and $TNF-\alpha$ elevation), which directly damages the vascular endothelium.
Think of your muscles as a sponge for blood sugar. When you lose muscle, that "sponge" gets smaller, leaving excess sugar and inflammation to circulate in your blood, eventually "rusting" your arteries and putting extra strain on your heart.
2. VO2 Max as the "Survival Currency"
Scientific Perspective: Sarcopenia directly limits VO2 max (maximal oxygen consumption). Since muscles are the end-users of the oxygen the heart pumps, a reduction in muscle quality creates a bottleneck. New research shows this "peripheral limitation" is as dangerous as a weak heart itself.
Your heart can only pump as much oxygen as your muscles are capable of using. If your muscles are weak, your heart loses its training partner. Keeping your muscles strong ensures your heart doesn't have to work twice as hard to move you through your daily life.
3. The "Silent Atrophy" of the Heart
Scientific Perspective: The 2025 research suggests a "cross-talk" between skeletal muscle and cardiac tissue. When skeletal muscles atrophy, the heart undergoes cardiac deconditioning—becoming smaller and less compliant because the "demand signal" from the rest of the body has gone quiet.
Your heart follows the "Use It or Lose It" rule. If your leg and arm muscles aren't demanding blood flow through exercise, your heart muscle actually gets "out of shape" and weaker because it’s not being challenged. Strong limbs lead to a strong, thick heart wall.
4. Protein Thresholds & The "Anabolic Window"
Scientific Perspective: Older adults require higher leucine concentrations to trigger muscle protein synthesis (MPS). The 2026 guidelines recommend 1.2–1.5g of protein per kg/day, specifically timed within 30–60 minutes post-exercise to overcome "anabolic resistance."
Just eating protein isn't enough; you have to give your body a reason to use it. By eating high-quality protein (like eggs, Greek yogurt, or lean meat) right after a walk or a strength session, you "unlock" your body’s ability to repair your muscles and protect your heart.
5. The "Sex-Specific" Risk Warning
Scientific Perspective: 2025 studies (Gunawardana et al.) found that men are more susceptible to a "hypertensive phenotype" when lean mass drops. In men, low muscle mass is more aggressively linked to stiff arteries and high blood pressure than it is in women at the same age.
While muscle is vital for everyone, men need to be extra vigilant. For men, losing muscle doesn't just make you "weaker"—it is directly tied to your blood pressure spiking and your arteries becoming stiff like old pipes. Strength training is essentially a blood pressure medication you perform in the gym.
Author’s Note
As a physician and clinician deeply engaged with the science of aging, metabolism, and cardiovascular health, my goal in writing this article is to bridge the gap between emerging research and practical, real-world application. Sarcopenia is often overlooked or dismissed as a natural part of aging, yet the latest scientific evidence clearly shows that muscle loss has profound consequences—not only for strength and mobility, but also for heart health, lung function, and overall longevity.
I wrote this piece to empower readers with knowledge that can change outcomes. The research published in 2025 marks a turning point in how we understand the interconnectedness of muscle, cardiovascular function, and respiratory capacity. By highlighting these findings in a clear and patient-friendly way, I hope to encourage early screening, proactive lifestyle changes, and a more integrated approach to preventive health.
Most importantly, I want to emphasize that sarcopenia is not inevitable. With the right combination of resistance training, aerobic exercise, and optimal nutrition, meaningful improvements are possible at any age. Your muscles are not just for movement—they are a cornerstone of metabolic, cardiovascular, and respiratory health. Taking action today can protect your strength, your independence, and your future wellbeing.
While most current evidence is derived from observational and longitudinal studies, the consistency of associations across populations, dose-response relationships, and strong mechanistic pathways collectively support a likely causal link. However, residual confounding and reverse causation cannot be fully excluded.
Medical Disclaimer: This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. All exercise and nutritional strategies discussed should be evaluated in the context of your individual health circumstances in consultation with a qualified healthcare provider. People with established cardiovascular disease should seek clearance from their cardiologist before beginning any new exercise programme.
Related Articles
Is Resistance Training Safe and Effective for Cardiovascular Patients? A Clinical Guide
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
Best Exercises for Sarcopenia: Strength Training Guide for Older Adults | DR T S DIDWAL
References
Cornelissen, V., Neunhäuserer, D., Niebauer, J., Papadakis, M., Wilhelm, M., & Hansen, D. (2025). Influence of exercise and nutrition on sarcopenia in cardiovascular disease: A scientific statement of the European Association of Preventive Cardiology of the ESC. European Journal of Preventive Cardiology, Article zwaf432. https://doi.org/10.1093/eurjpc/zwaf432
Gunawardana, D., Guo, M., & Montero, D. (2025). Lean body mass associates with a hypertensive cardiovascular phenotype in men but not in women. Journal of Cachexia, Sarcopenia and Muscle, 16(6), Article e70125. https://doi.org/10.1002/jcsm.70125
Hanon, O. (2025). Sarcopenia: A new cardiovascular risk factor? European Journal of Preventive Cardiology, Article zwaf282. https://doi.org/10.1093/eurjpc/zwaf282
Liu, Q., Cui, H., & Wu, Y. (2026). Association of trajectories of sex-specific quintiles of predicted lean mass and risk of cardiovascular disease: A prospective cohort study. Nutrition, Metabolism and Cardiovascular Diseases, 36(3), Article 104467. https://doi.org/10.1016/j.numecd.2025.104467
Lu, Z., Kong, Y., Shao, W., Ke, J., Wang, Y., Wei, X., Hou, Y., & Shao, R. (2025). Association between long-term burden of sarcopenia and cardiorespiratory multimorbidity. The Journal of Nutrition, Health & Aging, 29(11), Article 100670. https://doi.org/10.1016/j.jnha.2025.100670
Moretti, A., Paoletta, M., Liguori, S., Bertone, M., Toro, G., & Iolascon, G. (2025). Physical exercise for primary sarcopenia: An expert opinion. Frontiers in Rehabilitation Sciences, 6, Article 1538336. https://doi.org/10.3389/fresc.2025.1538336
Nezafati, P., Saxena, P., Raman, J., Hebbard, L., & McFarlane, C. (2025). Getting to the heart of sarcopenia and cardiovascular disease. Aging, 17(8), 2212–2239. https://doi.org/10.18632/aging.206296
Patnaik, A. (2025). Sarcopenia: Emerging role in cardiovascular disorders. Indian Journal of Clinical Cardiology, 6(1), 7–8. https://doi.org/10.1177/26324636241309973
Wang, N., Xiao, Y., Chen, Z., & Liu, Y. (2026). Sarcopenia and risk of cardiovascular events and mortality: A meta-analysis of longitudinal observational studies. Canadian Journal of Cardiology. Advance online publication. https://doi.org/10.1016/j.cjca.2025.XX.XXX
Yu, Z., Zhao, Z., Ding, C., Liu, Q., Ma, T., Han, X., Lu, D., & Zhang, L. (2025). The association between sarcopenia and cardiovascular disease: An investigative analysis from the NHANES. Nutrition, Metabolism and Cardiovascular Diseases, 35(7), 103864. https://doi.org/10.1016/j.numecd.2025.104467