Metabolically Healthy Obesity: Why "Healthy" Doesn't Mean Safe
Think "metabolically healthy obesity" means you're safe? New 2025 research says otherwise. Discover the hidden cardiovascular risks, who's truly at risk, and what to do now.
OBESITY
Dr. T.S. Didwal, M.D.
5/26/202623 min read
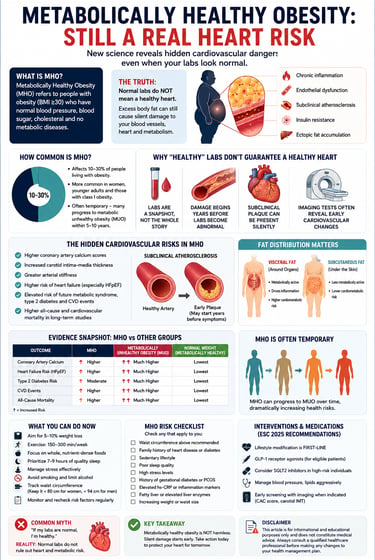
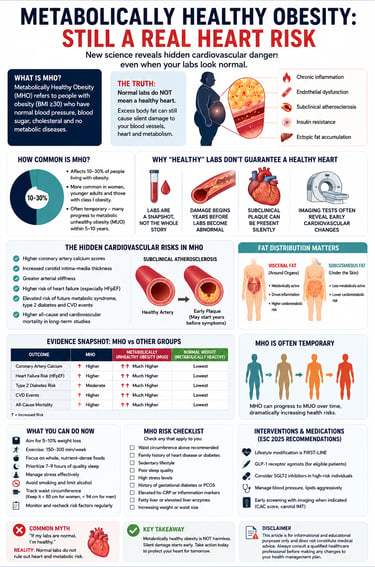
No, metabolically healthy obesity is not as safe as it sounds.
Even if your blood sugar, cholesterol, and blood pressure look completely normal, carrying extra weight — especially around the belly — can still quietly raise your risk of heart disease, clogged arteries, and future diabetes. New 2025–2026 research shows this “healthy obesity” state is often temporary and hides early heart damage. The good news? Taking action now with modest weight loss (just 5–10%), regular walking, better sleep, and the right diet can significantly protect your heart. Talk to your doctor about a full check-up beyond standard labs.
Key Takeaways
1. MHO Confers Intermediate Cardiovascular Risk
Individuals with MHO exhibit a moderately elevated risk of coronary artery disease (approximately 50% higher) and cardiometabolic multimorbidity compared to metabolically healthy normal-weight (MHNW) individuals, despite normal standard metabolic parameters. This risk stems from subclinical endothelial dysfunction, low-grade inflammation, and early atherosclerotic processes independent of overt dysglycemia or dyslipidemia (Shuey et al., 2025; Koskinas et al., 2025).
2. MHO Represents a Transient Phenotype
Longitudinal cohort data indicate that MHO is frequently unstable, with a substantial proportion of individuals transitioning to metabolically unhealthy obesity (MUO) within 5–10 years. This transition is associated with a >100% increase in cardiometabolic multimorbidity risk, driven by progressive visceral adiposity, epigenetic modifications, and declining mitochondrial function (Cai et al., 2025; Tsuchiya & Tsutsumi, 2025).
3. Visceral Fat Distribution is the Primary Determinant
Cardiovascular risk in obesity is more strongly mediated by ectopic and visceral adipose tissue accumulation than by total adiposity (BMI). Even in MHO, preferential visceral fat storage promotes adipose tissue hypoxia, macrophage polarization toward pro-inflammatory phenotypes, and reduced adiponectin signaling, accelerating vascular remodeling (Schulze & Stefan, 2024).
4. Standard Metabolic Panels Lack Sensitivity for Risk Stratification
Routine biomarkers (fasting glucose, HbA1c, lipids, blood pressure) are lagging indicators that fail to detect ongoing subclinical atherosclerosis, elevated hs-CRP, hyperinsulinemia, and coronary artery calcium burden frequently present in MHO. Advanced phenotyping incorporating waist circumference, HOMA-IR, and imaging is required for accurate risk assessment (Koskinas et al., 2025).
5. Weight Reduction and Physical Activity Yield Independent Benefits
Modest weight loss (5–10% of body weight) and regular aerobic/resistance exercise confer cardiovascular protection in MHO through improvements in endothelial function, reduction of systemic inflammation, and enhanced mitochondrial oxidative capacity — effects that are partially independent of changes in metabolic laboratory parameters (Chen et al., 2025; Zhang et al., 2025).
6. Early Intervention is Supported by Major Guidelines
The 2025 ESC Clinical Consensus Statement recommends comprehensive obesity management—including lifestyle modification, consideration of GLP-1 receptor agonists, and evaluation of bariatric surgery—for all individuals with obesity, irrespective of current metabolic health classification. Delaying intervention based on MHO status is inconsistent with current evidence (Koskinas et al., 2025).
What Is Metabolically Healthy Obesity — And Why Does It Matter?
Imagine stepping off the scale, having a BMI over 30, and then hearing your doctor say: "Your blood tests look perfect. Everything is normal."
For millions of people, this scenario feels like a win. And for years, the medical community used a reassuring label for it: metabolically healthy obesity (MHO). The idea was simple — if your blood sugar, blood pressure, cholesterol, and insulin sensitivity all fell within normal ranges despite excess body weight, your cardiovascular risk was considered low.
But that idea is being dismantled by some of the most rigorous research of the decade.
New evidence from 2024–2026 makes one thing unmistakably clear: metabolically healthy obesity is not cardiovascularly safe. Even when your routine lab work looks perfectly normal, excess body fat creates a cascade of silent, systemic damage — subclinical atherosclerosis, vascular inflammation, and cardiometabolic disease — long before any blood test catches it.
This article gives you the complete, evidence-based picture of what MHO actually is, what the latest science reveals about its risks, and — most importantly — exactly what you and your healthcare provider should do about it right now.
How Common Is MHO? The Prevalence Data
Metabolically healthy obesity is more common than most people realize — yet less stable than anyone would hope.
A 2025 review published in Biomolecules by researchers from the University of Yamanashi reported that MHO affects roughly 10–30% of people living with obesity globally, with significant variation by sex, age, BMI level, and ethnicity. Women, younger individuals, and those with Class I obesity (BMI 30–34.9) are most likely to meet MHO criteria at any given moment.
However — and this is critical — that "metabolically healthy" status is often temporary. Studies consistently show that a substantial proportion of people classified as MHO will develop metabolic abnormalities within 5–10 years, at which point their cardiovascular risk escalates sharply.
Key prevalence facts:
Approximately 1 in 5 to 1 in 3 obese adults meets MHO criteria at any given time
MHO prevalence declines with age — older adults with obesity are far more likely to be metabolically unhealthy
Ethnicity significantly affects metabolic risk thresholds; Asian populations, for example, experience metabolic dysfunction at lower BMI levels than European populations
MHO prevalence has been decreasing in recent decades as obesity severity has increased across populations
Why "Healthy" Labs Don't Guarantee a Healthy Heart
Here is the core problem with the MHO concept: standard metabolic labs are a snapshot, not a safety certificate.
The tests most clinicians use to define metabolic health — fasting glucose, HbA1c, fasting lipids, blood pressure, and waist circumference — are all lagging indicators. They reveal metabolic dysfunction only after it has already been present for some time. What they miss completely is the subclinical damage that excess adipose tissue causes in the years before markers shift.
Several biological processes running quietly beneath your normal lab values include:
Endothelial dysfunction: The inner lining of your blood vessels loses flexibility and responsiveness, impairing blood flow regulation even when blood pressure appears normal.
Low-grade chronic inflammation: Excess adipose tissue — particularly visceral fat — secretes inflammatory cytokines including TNF-alpha, IL-6, and CRP, which promote atherosclerosis independent of lipid levels.
Subclinical atherosclerosis: Carotid intima-media thickness and coronary artery calcium scores — more sensitive markers of vascular disease — are often elevated in MHO individuals even when LDL cholesterol is perfectly normal.
Adipose tissue hypoxia: As fat cells expand, they outgrow their oxygen supply, triggering local inflammation and fibrosis — processes invisible on a standard blood panel.
Hyperinsulinemia without frank hyperglycemia: Insulin levels can be elevated (and damaging) even when fasting glucose remains in the normal range.
As the 2025 ESC Clinical Consensus Statement explicitly states, excess adipose tissue itself — independent of traditional metabolic markers — is an independent risk factor for cardiovascular events. This fundamentally changes how we should interpret "normal" metabolic labs in someone with obesity.
The Hidden Cardiovascular Risks in MHO
The cardiovascular risks lurking beneath a "metabolically healthy" label are now well-documented. Here is what the research consistently finds:
Subclinical Atherosclerosis
Studies using carotid ultrasound and coronary calcium CT consistently detect measurable plaque burden in MHO individuals — plaque that hasn't caused symptoms yet but represents genuine cardiovascular disease in progress. In multiple imaging studies, coronary artery calcium scores in MHO individuals fall between those of metabolically healthy normal-weight individuals and those with metabolically unhealthy obesity — significantly above zero.
Elevated Coronary Artery Disease Risk
A landmark cohort study published in the Journal of the American Heart Association in 2025, examining 69,272 patients, found that even individuals who remained metabolically healthy while obese carried elevated coronary artery disease risk compared to normal-weight metabolically healthy individuals. Those who transitioned from metabolically healthy to metabolically unhealthy obesity experienced a dramatic further escalation in risk.
Cardiometabolic Multimorbidity
A 2025 nationwide prospective cohort study published in Frontiers in Nutrition — using data from the China Health and Retirement Longitudinal Study — examined 5,850 participants and tracked cardiometabolic multimorbidity (CMM), defined as the simultaneous presence of two or more of the following: diabetes, hypertension, and cardiovascular disease. Among all BMI-metabolic phenotypes, the metabolically unhealthy obese group carried the highest CMM risk (OR = 3.31). But critically, the MHO group also showed significantly elevated CMM risk compared to metabolically healthy normal-weight individuals — confirming that even "healthy" obesity accelerates multi-organ disease.
Heart Failure Risk
Recent data, including studies cited in the 2025 ESC consensus statement, demonstrate elevated risk of heart failure with preserved ejection fraction (HFpEF) in MHO individuals — a form of heart failure increasingly linked to obesity and visceral fat accumulation independent of traditional metabolic markers. HFpEF is particularly difficult to treat and strongly impairs quality of life.
Sleep Apnea and Autonomic Dysfunction
Even without dyslipidemia or hypertension, obese individuals frequently experience obstructive sleep apnea, which triggers nocturnal hypoxia, intermittent sympathetic activation, and oxidative stress — all of which accelerate cardiovascular aging.
Why Fat Distribution Matters More Than Your BMI
One of the most important advances in obesity science over the past decade is the recognition that where fat is stored matters as much as — and possibly more than — how much fat you carry.
A landmark 2024 review in Nature Reviews Endocrinology by Schulze and Stefan from the German Institute of Human Nutrition and the German Center for Diabetes Research found that fat distribution is central to understanding metabolic risk in obesity. Specifically:
Visceral adipose tissue (VAT) — fat stored around internal organs — is metabolically active and highly inflammatory. High VAT is strongly associated with cardiovascular risk even when total BMI is only modestly elevated.
Subcutaneous adipose tissue (SAT) — fat stored just beneath the skin, particularly in the lower body — is metabolically more benign and may even have some protective cardiovascular properties.
Ectopic fat deposits — in the liver (hepatic steatosis), around the heart (pericardial fat), and within skeletal muscle — are particularly damaging and associated with insulin resistance, arrhythmias, and cardiac dysfunction.
People with MHO typically have lower visceral fat and more favorable fat distribution compared to metabolically unhealthy obese individuals. This is likely the primary structural reason their standard metabolic markers remain normal for longer. However — and this is the critical nuance — visceral fat accumulation progresses with time, aging, and lifestyle factors. The metabolically favorable fat distribution that characterizes MHO today is often not the distribution that person will have a decade from now.
Body fat distribution assessment tools:
Tool What It Measures Clinical Use Waist circumference Proxy for central adiposity Routine clinical screening Waist-to-height ratio Central fat relative to height Better predictor than BMI alone DEXA scan Total and regional body composition Research and specialty clinics CT/MRI Precise visceral vs. subcutaneous fat Research standard Liver ultrasound Hepatic steatosis (ectopic fat) Widely available clinically
The Cellular and Molecular Science Behind MHO
Why do some people with obesity maintain better metabolic health than others? The answer lies at the cellular and molecular level — and the science here is genuinely fascinating.
A 2025 paper in Biomolecules by Tsuchiya and Tsutsumi from the University of Yamanashi provides the most comprehensive recent synthesis. Several biological mechanisms distinguish MHO from metabolically unhealthy obesity (MUO):
Adipose Tissue Inflammation
In MUO, adipose tissue undergoes a dramatic transformation: macrophages infiltrate fat depots, shifting from anti-inflammatory M2 to pro-inflammatory M1 phenotypes. Crown-like structures — clusters of dead adipocytes surrounded by inflammatory macrophages — accumulate. This creates a chronic inflammatory microenvironment.
In MHO, adipose tissue tends to maintain healthier inflammatory profiles with lower macrophage infiltration and higher proportions of regulatory T-cells (Tregs), which suppress inflammation.
Adiponectin: The Protective Hormone
MHO individuals typically have higher circulating adiponectin — an insulin-sensitising, anti-inflammatory adipokine secreted by fat cells. Adiponectin protects blood vessels, improves lipid metabolism, and reduces hepatic glucose production. As obesity progresses toward the metabolically unhealthy phenotype, adiponectin levels drop and leptin levels rise — a shift that is measurable and clinically significant.
Mesothelial Cells: A New Discovery
A remarkable finding from recent single-cell transcriptomic analyses identified mesothelial cells lining the visceral peritoneum as potentially key drivers of metabolic health in visceral adipose tissue. These cells appear to create a metabolically protective barrier around visceral fat in MHO individuals. Their dysfunction or loss may be a tipping point in the transition to MUO.
Epigenetic Memory of Obesity
Among the most consequential discoveries in this field is persistent epigenetic memory of obesity — molecular changes to gene expression patterns that persist even after weight is lost. This provides a molecular explanation for why MHO often represents a transient state and why weight regain is so common: the body's gene expression machinery retains a "memory" of the obese state, making metabolic deterioration more likely over time.
Mitochondrial Function
MHO individuals typically demonstrate better mitochondrial biogenesis and oxidative capacity in skeletal muscle compared to MUO individuals. This improved energy metabolism capacity — partly explained by higher physical activity levels in MHO individuals — contributes to better insulin sensitivity and lipid handling.
Key Studies: What the Research Actually Shows
Study 1: The 69,272-Patient CAD Cohort (JAHA, 2025)
Reference: Shuey et al., Journal of the American Heart Association, 2025
Design: Large clinical cohort study tracking metabolic health transitions
Key Finding: Even individuals who maintained metabolically healthy status while obese showed elevated coronary artery disease risk compared to normal-weight metabolically healthy individuals. Those transitioning from metabolically healthy to unhealthy obesity experienced dramatically higher risk. The study powerfully illustrates that metabolic health classification is dynamic, not static.
Clinical Implication: Even if your labs are normal today, staying obese increases your cumulative cardiovascular risk with each passing year.
Study 2: Cardiometabolic Multimorbidity Nationwide Cohort (Frontiers in Nutrition, 2025)
Reference: Cai, Zhang, Ding et al., Frontiers in Nutrition, 2025
Design: Nationwide prospective cohort study; 5,850 Chinese adults followed longitudinally
Key Finding: Both overweight/obesity and metabolically unhealthy status significantly accelerated cardiometabolic multimorbidity progression. Metabolically unhealthy obese individuals had the highest risk (OR = 3.31). Critically, individuals who transitioned from MHO to metabolically unhealthy obesity (MUO) showed a 107% increase in CMM risk compared to those who remained metabolically healthy and normal weight.
Clinical Implication: The transition from MHO to MUO is a major cardiac event in slow motion. Preventing that transition through early lifestyle intervention is a high-value clinical target.
Study 3: Weight Changes and Cardiovascular Outcomes (Heart, 2025)
Reference: Zhang, Schutte & Pierscionek, Heart, 2025
Design: Prospective cohort study; 454 obese patients with existing cardiovascular disease
Key Finding: Weight reduction correlated with improved cardiovascular outcomes across the metabolic health spectrum — including among metabolically healthy obese participants. Weight gain predicted a worse cardiovascular prognosis.
Clinical Implication: Even if you are currently metabolically healthy, weight loss delivers measurable cardiovascular benefit. This argues definitively against a "watch and wait" approach in MHO.
Study 4: Fat Distribution and MHO Definition (Nature Reviews Endocrinology, 2024)
Reference: Schulze & Stefan, Nature Reviews Endocrinology, 2024
Design: Comprehensive review of MHO epidemiology, mechanisms, and clinical implications
Key Finding: Studies support the MHO concept but emphasize that fat distribution — particularly the ratio of visceral to subcutaneous fat — is central to risk stratification. MHO individuals have a moderately elevated cardiovascular risk compared to metabolically healthy normal-weight individuals. This elevation should not be dismissed as clinically insignificant.
Clinical Implication: Body fat distribution assessment (waist circumference, waist-to-height ratio, or imaging) should be standard in all obese patients regardless of metabolic marker status.
Study 5: Cellular Mechanisms of MHO (Biomolecules, 2025)
Reference: Tsuchiya & Tsutsumi, Biomolecules, 2025
Design: Comprehensive molecular review
Key Finding: MHO individuals with obesity have a 50% increased risk of coronary heart disease compared to metabolically healthy normal-weight individuals — even before any metabolic markers deteriorate. Epigenetic memory of obesity provides a molecular basis for why MHO is typically a transient rather than stable state.
Clinical Implication: The molecular machinery driving cardiovascular damage in obesity is already running at diagnosis of MHO. Waiting for metabolic markers to become abnormal is too late.
Study 6: ESC Consensus Statement (European Journal of Preventive Cardiology, 2025)
Reference: Koskinas et al., European Journal of Preventive Cardiology, 2025
Design: Clinical consensus statement from Europe's leading cardiology society
Key Finding: Metabolic health phenotypes should not guide clinical decision-making regarding obesity management. All individuals with obesity — regardless of current metabolic profile — merit comprehensive lifestyle intervention, pharmacotherapy consideration, and in appropriate cases, bariatric surgery referral. Clinicians should avoid falsely reassuring patients that favorable metabolic markers protect against cardiovascular disease.
Clinical Implication: This is the most authoritative cardiovascular organization in Europe explicitly endorsing aggressive intervention regardless of MHO status.
Study 7: Weight Control and Cardiovascular Outcomes — Umbrella Review
Reference: Chen et al., International Journal of Obesity, 2025
Design: Umbrella review of systematic reviews and meta-analyses — hundreds of studies, hundreds of thousands of participants
Key Finding: Structured weight loss interventions consistently reduce cardiovascular event risk and mortality. Even 5–10% weight reduction produces measurable cardiovascular benefit — ideal body weight is not required.
Clinical Implication: Modest, achievable weight loss is clinically meaningful. This is one of the most patient-empowering findings in the literature.
Evidence Summary Table: MHO vs. Other Phenotypes
Understanding Metabolic Phenotypes and Health Risks
Metabolic health is not determined by weight alone. Researchers categorize individuals into four distinct metabolic phenotypes based on their Body Mass Index (BMI) and metabolic markers (like blood pressure, blood sugar, and cholesterol).
1. Metabolically Healthy Normal Weight (MHNW)
Definition: Individuals with a normal BMI and optimal metabolic health markers.
Cardiovascular Disease (CVD) Risk: Baseline / Lowest risk.
Diabetes Risk: Baseline / Lowest risk.
Cardiometabolic Mortality (CMM) Risk: Baseline / Lowest risk.
Stability Over Time: Highest stability. This is the healthiest reference group and tends to remain stable over time.
2. Metabolically Healthy Obesity (MHO)
Definition: Individuals with a BMI in the obesity range who currently maintain healthy metabolic markers.
Cardiovascular Disease (CVD) Risk: Moderately elevated (~50% higher than MHNW).
Diabetes Risk: Elevated.
Cardiometabolic Mortality (CMM) Risk: Elevated.
Stability Over Time: Often transient. This state is frequently temporary, as many individuals eventually progress to Metabolically Unhealthy Obesity (MUO).
3. Metabolically Unhealthy Normal Weight (MUNW)
Definition: Individuals with a normal BMI who exhibit poor metabolic health markers (sometimes referred to as "skinny fat").
Cardiovascular Disease (CVD) Risk: Moderately elevated.
Diabetes Risk: High risk.
Cardiometabolic Mortality (CMM) Risk: High risk (Odds Ratio ~1.91 compared to MHNW).
Stability Over Time: Moderate stability.
4. Metabolically Unhealthy Obesity (MUO)
Definition: Individuals with both a BMI in the obesity range and poor metabolic health markers.
Cardiovascular Disease (CVD) Risk: Highest risk.
Diabetes Risk: Highest risk.
Cardiometabolic Mortality (CMM) Risk: Highest risk (Odds Ratio ~3.31 compared to MHNW).
Stability Over Time: Most stable. This profile rarely improves without targeted clinical or lifestyle interventions.
Key Takeaway: Normal weight does not guarantee metabolic health (as seen in MUNW), and obesity is rarely permanently benign (as seen in MHO). Managing metabolic markers is critical regardless of the scale.
MHO Is Temporary: The Transition Problem
Perhaps the most clinically important — and least discussed — aspect of MHO is its inherent instability.
The 2025 Frontiers in Nutrition cohort study quantified it starkly: individuals who transitioned from MHO to MUO (metabolically unhealthy obesity) experienced a 107% increase in cardiometabolic multimorbidity risk. That is more than a doubling of risk — triggered not by a dramatic health event, but simply by the natural progression of untreated obesity.
What drives this transition? Several well-established factors:
Aging: Hormonal changes, decreased physical activity, and altered fat distribution with age accelerate the shift from subcutaneous to visceral fat storage, eroding metabolic health.
Progressive weight gain: Even modest additional weight gain in an already obese individual can tip the balance from metabolically healthy to unhealthy.
Declining physical activity: The cardiovascular and metabolic benefits of physical activity — which significantly buffer the effects of excess fat mass — diminish when activity levels fall.
Stress and sleep disruption: Chronic psychological stress and poor sleep quality both elevate cortisol, which promotes visceral fat accumulation and insulin resistance.
Dietary quality deterioration: Even without weight gain, diets high in ultra-processed foods, refined carbohydrates, and added sugars drive inflammation and metabolic dysfunction independent of caloric intake.
The clinical implication is sobering: Telling a patient with MHO that they are "fine for now" sets them up for a future crisis. The responsible clinical message is: you are in a better position than someone with metabolically unhealthy obesity, but that position is fragile and actively requires maintenance through lifestyle intervention.
Common Myths and Dangerous Misconceptions
Myth 1: "My labs are perfect, so my heart must be healthy."
Reality: Standard metabolic labs do not measure endothelial function, arterial stiffness, or subclinical atherosclerosis. People with MHO frequently have measurable cardiovascular disease on imaging, even with perfectly normal blood tests. Normal labs are a good starting point, not a finish line.
Myth 2: "I don't need to lose weight unless my metabolic markers get worse."
Reality: Weight reduction produces cardiovascular benefits even in metabolically healthy individuals. Multiple studies confirm that waiting until metabolic dysfunction develops forfeits significant preventive opportunity. By the time markers shift, subclinical cardiovascular damage has already been accumulating for years.
Myth 3: "Exercise only helps if it leads to weight loss."
Reality: Physical activity provides powerful, independent cardiovascular benefits completely separate from its effects on body weight. Regular exercise improves endothelial function, reduces systemic inflammation, enhances mitochondrial function, and improves insulin sensitivity — all of which directly protect the heart regardless of what the scale says.
Myth 4: "MHO is a stable, long-term state."
Reality: MHO is frequently a transitional phenotype. Large cohort studies consistently demonstrate progression to metabolically unhealthy obesity over 5–10 years in a substantial proportion of individuals currently classified as MHO, particularly without lifestyle intervention.
Myth 5: "If I'm metabolically healthy, newer weight loss medications don't apply to me."
Reality: The 2025 ESC consensus statement supports considering GLP-1 receptor agonists and other weight management pharmacotherapies in all individuals with obesity who have cardiovascular risk factors — regardless of current metabolic health status. These medications offer cardiovascular benefits extending beyond weight loss alone.
Myth 6: "BMI is the best measure of obesity-related risk."
Reality: BMI is a population-level tool with well-documented limitations at the individual level. Fat distribution — particularly visceral vs. subcutaneous fat — is a more accurate predictor of cardiometabolic risk than BMI alone. Waist circumference and waist-to-height ratio should be assessed in every clinical encounter.
Practical Action Plan: What to Do If You Have MHO
Being classified as metabolically healthy with obesity is not a diagnosis of safety — it is a window of opportunity. Here is exactly how to use it:
Step 1: Get a Comprehensive Cardiovascular Assessment
Don't settle for routine blood work alone. Ask your doctor about:
Waist circumference and waist-to-height ratio (assess visceral fat accumulation)
High-sensitivity C-reactive protein (hs-CRP) (marker of systemic inflammation)
Fasting insulin and HOMA-IR (detect insulin resistance before glucose rises)
Liver ultrasound (screen for hepatic steatosis/ectopic fat)
Coronary artery calcium (CAC) score — especially if you are over 40, have a family history of heart disease, or have multiple borderline risk factors
Carotid intima-media thickness (CIMT) in select cases
Step 2: Set a Weight Loss Target of 5–10%
You do not need to reach your "ideal body weight." Evidence from multiple systematic reviews and meta-analyses confirms that 5–10% weight reduction produces measurable cardiovascular benefits — improved blood pressure, better lipid profiles, reduced inflammation, and lower event risk. Focus on this achievable, meaningful goal rather than a distant ideal weight.
Step 3: Prioritize Physical Activity — Even Without Weight Loss
Current guidelines recommend:
150–300 minutes of moderate-intensity aerobic activity per week (brisk walking, cycling, swimming)
At least 2 sessions of resistance/strength training per week
Reduce prolonged sitting: Break up sedentary time with movement every 30–60 minutes
Physical activity improves vascular health, reduces inflammation, and protects your heart through mechanisms completely independent of weight loss. This is not optional — it is medicine.
Step 4: Optimize Your Diet for Vascular Health
Evidence-based dietary strategies that protect cardiovascular health regardless of caloric restriction:
Mediterranean-style eating pattern: Olive oil, vegetables, legumes, whole grains, fish, and moderate nuts. Consistently associated with cardiovascular risk reduction across populations.
Minimize ultra-processed foods and added sugars: These drive inflammation independent of caloric intake.
Adequate dietary fiber (25–30g/day): Supports gut microbiome health, reduces LDL cholesterol, and improves insulin sensitivity.
Limit sodium: Particularly important for blood pressure control even in the absence of hypertension.
Step 5: Address Sleep and Stress
Screen for obstructive sleep apnea (highly prevalent in obesity; STOP-BANG questionnaire)
Target 7–9 hours of quality sleep per night
Implement evidence-based stress management: mindfulness, cognitive behavioral techniques, or structured relaxation
Step 6: Discuss Pharmacotherapy Openly
Do not dismiss weight management medications as a "last resort." The 2025 ESC consensus statement and supporting evidence support discussing:
GLP-1 receptor agonists (e.g., semaglutide): Demonstrate cardiovascular risk reduction independent of weight loss mechanisms. Now considered cardioprotective in high-risk individuals.
GLP-1/GIP dual agonists (e.g., tirzepatide): Show even greater weight reduction and metabolic improvements in recent trials.
These are appropriate tools for appropriate candidates — not admissions of failure.
Step 7: Monitor, Don't Assume Stability
Annual metabolic panel including fasting glucose, HbA1c, full lipids, and liver enzymes
Blood pressure at every clinical encounter
Reassess cardiovascular risk comprehensively every 1–2 years
Repeat advanced testing (e.g., CAC score) if clinically indicated
MHO Risk Assessment Checklist
Use this checklist to discuss your personal risk profile with your healthcare provider:
Lifestyle Factors (higher risk if present):
Sedentary lifestyle (< 150 minutes/week of moderate physical activity)
Regular consumption of ultra-processed foods or added sugars
Poor sleep quality or duration < 7 hours/night
High chronic stress levels
Current smoker or significant smoking history
Clinical Factors (higher risk if present):
Waist circumference > 88 cm (women) or > 102 cm (men)
Family history of premature cardiovascular disease (< 55 in males, < 65 in females)
Age > 45 (men) or > 55 (women) or post-menopausal
Elevated hs-CRP (> 2.0 mg/L)
Fasting insulin > 15 µIU/mL (or HOMA-IR > 2.5)
Fatty liver disease on ultrasound
Obstructive sleep apnea
Weight/BMI Factors:
BMI > 35 (higher absolute risk)
BMI has been trending upward over the past 2–5 years
Predominantly central/abdominal weight distribution
If you have 3 or more of the above, discuss comprehensive cardiovascular risk assessment and early intervention with your doctor — regardless of your standard metabolic labs.
Medications and Interventions: What the ESC Now Recommends
The 2025 European Society of Cardiology Clinical Consensus Statement on obesity and cardiovascular disease — the most authoritative document in this space — provides unambiguous guidance:
Lifestyle Intervention: Universal recommendation for all individuals with obesity, regardless of metabolic phenotype. Not a suggestion to consider — a baseline standard of care.
Pharmacotherapy: Clinicians should actively consider weight management pharmacotherapy in all obese individuals with cardiovascular risk factors, including those currently classified as metabolically healthy. The ESC specifically highlights:
GLP-1 receptor agonists for obesity with established cardiovascular disease or high risk
Emerging combination agents demonstrating cardiovascular benefits beyond weight reduction alone
Bariatric Surgery: Should be discussed and offered for appropriate candidates:
BMI ≥ 40 kg/m²
BMI ≥ 35 kg/m² with significant obesity-related comorbidities
Consider in BMI 30–35 in specific contexts (e.g., type 2 diabetes not well-controlled)
Advanced Monitoring: The ESC recommends incorporating biomarker and imaging-based assessments — not just standard metabolic panels — in higher-risk individuals with obesity.
What the ESC explicitly says to stop doing: Using metabolically healthy status to delay or forego obesity management interventions. This practice — once common — is now characterized as inconsistent with best evidence.
FAQs: Metabolically Healthy Obesity Answered
Q1: What exactly qualifies as "metabolically healthy obesity"?
There is no universally agreed-upon definition, which is part of what makes MHO research challenging. Most studies require a BMI ≥ 30 kg/m² plus the absence of two or more metabolic abnormalities from the following: elevated fasting glucose, high blood pressure, high triglycerides, low HDL cholesterol, and elevated waist circumference. Some definitions also require normal insulin sensitivity (HOMA-IR) and absence of inflammation (normal CRP). The Tsuchiya and Tsutsumi 2025 Biomolecules review comprehensively summarizes the variation in definitions used across major studies from 2006 to 2023.
Q2: Does having MHO mean I don't need to see a doctor about my weight?
Absolutely not. The 2025 ESC Clinical Consensus Statement explicitly recommends that all individuals with obesity — regardless of current metabolic profile — should be offered comprehensive obesity management. MHO is an indication for proactive intervention, not reassurance and surveillance.
Q3: Can MHO become metabolically unhealthy, and how quickly?
Yes — and faster than most people expect. Multiple large cohort studies demonstrate that a significant proportion of individuals classified as MHO transition to metabolically unhealthy obesity within 5–10 years, particularly without lifestyle intervention. The 2025 Frontiers in Nutrition study showed that this transition is associated with a 107% increase in cardiometabolic multimorbidity risk. The transition can be slowed and sometimes prevented through sustained lifestyle intervention.
Q4: How much weight do I need to lose to see real cardiovascular benefit?
Research is clear and reassuring here: you don't need to reach an "ideal" BMI. A 2025 umbrella review of hundreds of studies found that even 5–10% weight reduction produces measurable cardiovascular improvements — better blood pressure, improved lipid profiles, reduced inflammation, and lower event rates. For a 100 kg individual, that is just 5–10 kg. This is a realistic, achievable target.
Q5: Is exercise worth doing if my weight doesn't change much?
Emphatically yes. Physical activity provides cardiovascular protection through mechanisms entirely independent of weight loss — improved endothelial function, reduced systemic inflammation, better glycemic control, enhanced cardiac autonomic tone, and improved mitochondrial function. Multiple studies confirm that fit, obese individuals have significantly better cardiovascular outcomes than unfit, obese individuals at identical body weights.
Q6: Are GLP-1 medications appropriate for metabolically healthy obese individuals?
This requires an individual discussion with your healthcare provider. The current evidence supports considering GLP-1 receptor agonists in obese individuals with cardiovascular risk factors, even those with currently normal metabolic markers. These medications reduce cardiovascular events through mechanisms beyond weight loss alone. Your doctor will weigh your specific risk profile, comorbidities, and individual circumstances.
Q7: What tests should I ask my doctor for if I have MHO?
Beyond standard metabolic panels, consider discussing: high-sensitivity CRP, fasting insulin/HOMA-IR, liver ultrasound (for fatty liver), coronary artery calcium score (especially if > 40 with risk factors), and STOP-BANG questionnaire for sleep apnea screening. Waist circumference and waist-to-height ratio should be assessed at every visit.
Q8: Does MHO in women differ from men?
Yes, in several important ways. Women with obesity are more likely to be classified as MHO than men, partly because premenopausal estrogen promotes more favorable fat distribution (subcutaneous rather than visceral). However, after menopause, this protection diminishes rapidly — fat distribution shifts toward visceral depots, and metabolic markers often deteriorate over a relatively short period. Perimenopausal women with MHO should be followed particularly closely.
Q9: Can my children inherit MHO?
Obesity and metabolic health have both genetic and epigenetic components. Children of parents with obesity have higher risk of obesity themselves, and emerging research on epigenetic memory of obesity suggests that the metabolic environment established in utero and early childhood has lasting effects on metabolic health. This is a powerful motivation for parents to pursue their own metabolic health — both for their own benefit and as modeling for their children.
Q10: Is MHO the same as the "obesity paradox"?
Not exactly, though they are related concepts. The obesity paradox specifically refers to observations in some datasets where obese individuals with existing cardiovascular disease appeared to have better short-term survival outcomes than lean individuals — a finding that has been largely attributed to methodological confounding. MHO refers to the metabolic phenotyping of obese individuals without existing disease. The 2025 ESC consensus statement explicitly cautions against using either concept to delay intervention.
Q11: How often should I have my cardiovascular risk reassessed if I have MHO?
Annual assessment is appropriate for most individuals with MHO. This should include standard metabolic markers plus waist circumference and blood pressure at a minimum. More comprehensive assessment — including advanced biomarkers and potentially imaging — may be warranted every 2–3 years or sooner if new risk factors emerge, metabolic markers shift toward abnormality, or weight continues to increase.
Q12: Is bariatric surgery appropriate for MHO?
For individuals meeting BMI criteria (generally ≥ 40, or ≥ 35 with significant comorbidities), bariatric surgery delivers the most durable, significant cardiovascular risk reduction of any available intervention — and evidence supports this benefit regardless of pre-surgical metabolic health status. If you meet criteria and have not responded adequately to lifestyle and pharmacological intervention, a surgical consultation is appropriate and recommended by the 2025 ESC guidelines.
Conclusion and Key Takeaways
The science has spoken — and the message is clearer than ever before:
Metabolically healthy obesity is not cardiovascularly safe. It is a state of reduced but still meaningfully elevated risk, with a tendency to deteriorate over time and with increasing age. The apparent protection of normal metabolic markers masks real, measurable disease processes — subclinical atherosclerosis, endothelial dysfunction, chronic inflammation, and ectopic fat accumulation — that progress silently toward clinical cardiovascular events.
The good news is equally clear: intervention works, and you don't need to achieve perfection to benefit.
Even 5–10% weight loss delivers measurable cardiovascular protection
Exercise protects your heart independently of weight change
Modern pharmacological tools offer cardiovascular risk reduction beyond their weight-loss effects
Early, proactive intervention now prevents far more difficult clinical problems later
If you have been told your labs look good despite obesity, take that as an opportunity, not a permission slip to do nothing. You are ahead of where many people are — use that advantage.
Work with your healthcare provider to develop a comprehensive, personalized plan. Address your weight. Move your body. Optimize your diet. Screen for hidden risks. Monitor your status over time.
The window is open. The evidence is clear. The time to act is now.
Next Steps:
Schedule a comprehensive cardiovascular risk assessment with your doctor
Ask about waist circumference, hs-CRP, fasting insulin, and liver health screening
Start a sustainable physical activity plan this week — even 20 minutes daily matters
Discuss whether pharmacotherapy is appropriate for your situation
Return for annual metabolic reassessment
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Weight Loss vs Fat Loss: The Critical Difference Every GLP-1 User Must Understand
Visceral Fat Treatment: GLP-1, Semaglutide and SGLT2 Explained
GLP-1 Muscle Loss: You’re Losing Weight But Are You Losing Strength Too?
Obesity 2025: Revolutionary Research Advances in Treatment and Management | DR T S DIDWAL
References
Cai, N., Zhang, L., Ding, S., Tian, X., Mo, L., & Yu, B. (2025). Associations of metabolic heterogeneity of obesity with the progression of cardiometabolic multimorbidity — a nationwide prospective cohort study. Frontiers in Nutrition, 12, Article 1617929. https://doi.org/10.3389/fnut.2025.1617929
Chen, X., Zhang, X., Xiang, X., et al. (2025). Effects of weight control interventions on cardiovascular outcomes: An umbrella review of systematic reviews and meta-analyses. International Journal of Obesity, 49, 1911–1920. https://doi.org/10.1038/s41366-025-01860-z
Di Angelantonio, E., Kaptoge, S., Wormser, D., Willeit, P., Butterworth, A. S., Bansal, N., et al. (2015). Association of cardiometabolic multimorbidity with mortality. JAMA, 314(1), 52–60. https://doi.org/10.1001/jama.2015.7008
Janić, M., Janež, A., El-Tanani, M., & Rizzo, M. (2025). Obesity: Recent advances and future perspectives. Biomedicines, 13(2), Article 368. https://doi.org/10.3390/biomedicines13020368
Koskinas, K. C., Van Craenenbroeck, E. M., Antoniades, C., Blüher, M., Gorter, T. M., Hanssen, H., Marx, N., McDonagh, T. A., Mingrone, G., Rosengren, A., & Prescott, E. B. (2025). Obesity and cardiovascular disease: An ESC clinical consensus statement. European Journal of Preventive Cardiology, 32(3), 184–220. https://doi.org/10.1093/eurjpc/zwae279
Magkos, F. (2019). Metabolically healthy obesity: What's in a name? American Journal of Clinical Nutrition, 110, 533–539. https://doi.org/10.1093/ajcn/nqz133
Neeland, I. J., Poirier, P., & Despres, J. P. (2018). Cardiovascular and metabolic heterogeneity of obesity: Clinical challenges and implications for management. Circulation, 137, 1391–1406. https://doi.org/10.1161/CIRCULATIONAHA.117.029617
Perone, F., Spadafora, L., Pratesi, A., Nicolaio, G., Pala, B., Franco, G., Ruzzolini, M., & Ambrosetti, M. (2024). Obesity and cardiovascular disease: Risk assessment, physical activity, and management of complications. International Journal of Cardiology. Cardiovascular Risk and Prevention, 23, Article 200331. https://doi.org/10.1016/j.ijcrp.2024.200331
Petersen, M. C., et al. (2024). Cardiometabolic characteristics of people with metabolically healthy and unhealthy obesity. Cell Metabolism, 36, 745–761.e5.
Schulze, M. B., & Stefan, N. (2024). Metabolically healthy obesity: From epidemiology and mechanisms to clinical implications. Nature Reviews Endocrinology, 20, 633–646. https://doi.org/10.1038/s41574-024-01008-5
Shuey, M. M., Levinson, R. T., Vogel, M. E., Farber-Eger, E., Huang, S., Harrel, F. E., Jr., Hasty, A. H., Brown, J. D., Silver, H. J., Koethe, J. R., Beckman, J. A., Brown, N. J., Niswender, K. D., Cox, N. J., & Wells, Q. S. (2025). Risk of coronary artery disease associated with transitions in metabolic health in a clinical cohort of 69,272. Journal of the American Heart Association, Article e037597. https://doi.org/10.1161/JAHA.124.037597
Stefan, N., Haring, H. U., Hu, F. B., & Schulze, M. B. (2013). Metabolically healthy obesity: Epidemiology, mechanisms, and clinical implications. Lancet Diabetes & Endocrinology, 1, 152–162. https://doi.org/10.1016/S2213-8587(13)70062-7
Stefan, N., Haring, H. U., & Schulze, M. B. (2018). Metabolically healthy obesity: The low-hanging fruit in obesity treatment? Lancet Diabetes & Endocrinology, 6, 249–258. https://doi.org/10.1016/S2213-8587(17)30292-9
Tsuchiya, K., & Tsutsumi, T. (2025). Beyond the BMI paradox: Unraveling the cellular and molecular determinants of metabolic health in obesity. Biomolecules, 15(9), Article 1278. https://doi.org/10.3390/biom15091278
Zhang, J., Schutte, R., & Pierscionek, B. (2025). Association of weight change with cardiovascular events and all-cause mortality in obese participants with cardiovascular disease: A prospective cohort study. Heart (British Cardiac Society), 111(10), 454–461. https://doi.org/10.1136/heartjnl-2024-324383
Article reviewed and updated: May 2026. All studies cited are from peer-reviewed, high-impact publications. This article does not constitute medical advice. Readers should consult qualified healthcare professionals for personalized guidance.