Metabolic Plasticity: Epigenetic Adaptations to Calorie Restriction
Discover the latest science on calorie restriction, longevity, metabolism, autophagy, and healthy aging. Learn the benefits, risks, and safest evidence-based strategies for sustainable weight loss and metabolic health.
METABOLISMNUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/27/202623 min read
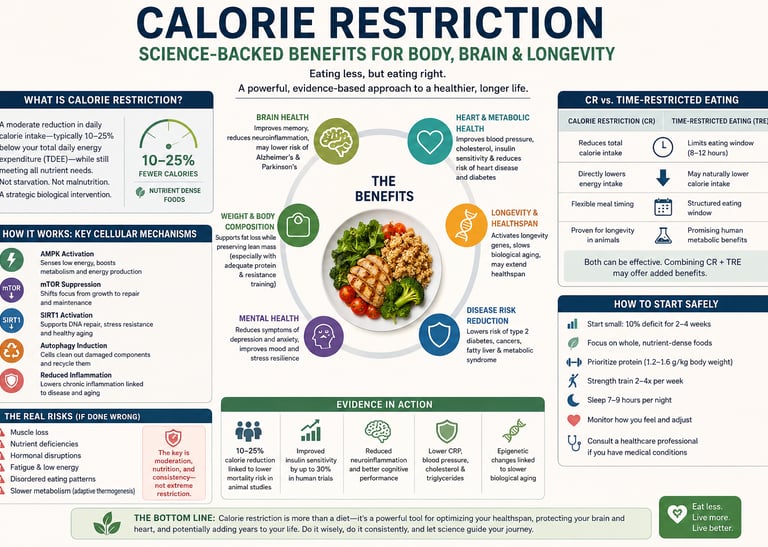
Calorie restriction (CR) is a dietary intervention that reduces daily caloric intake by 10% to 40% without causing malnutrition or depriving the body of essential nutrients. Unlike starvation, calorie restriction focuses on maintaining high nutrient density to activate longevity pathways, reduce systemic inflammation, and optimise metabolic health.
If you've ever tried calorie restriction and hit a wall—or watched someone else sail through the same diet—you already know the frustrating truth: calories in versus calories out is not the whole story.
The good news? Science in 2025 and 2026 has finally caught up with that frustration. Calorie restriction is no longer viewed as a blunt dieting tool. A wave of landmark studies now reveals it as a sophisticated biological intervention—one that reshapes your genes, rewires your brain, slows cellular aging, and may even reduce your risk of heart disease and type 2 diabetes.
In this comprehensive, evidence-based guide, you'll discover:
What the latest genomic research says about why calorie restriction works differently for different people
The brain health and mental health benefits most people never hear about
How time-restricted eating compares head-to-head with traditional calorie counting
The real risks of calorie restriction—and exactly how to avoid them
A practical, safe protocol for getting started today
Whether you're exploring calorie restriction for weight loss, longevity, metabolic health, or mental clarity, this guide covers everything you need to make an informed, personalized decision.
1. What Is Calorie Restriction? A Modern Definition
Calorie restriction (CR) refers to a reduction in daily caloric intake—typically by 10–40%—without causing malnutrition. Critically, this is not starvation. The goal is to consume fewer calories while maintaining adequate levels of protein, micronutrients, and essential fats.
For decades, calorie restriction was framed purely as a weight-loss strategy. Today, researchers understand it as a metabolic and epigenetic intervention with far-reaching effects on inflammation, aging, brain function, and disease risk.
The distinction matters. When calorie restriction is done correctly:
It activates longevity-associated pathways (SIRT1, AMPK, mTOR suppression)
It reduces systemic and neuroinflammation
It improves insulin sensitivity and metabolic flexibility
It triggers autophagy—your body's cellular "self-cleaning" process
It may slow biological aging at the genomic level
When it's done incorrectly—too aggressively, without adequate nutrition, or without professional oversight—it becomes counterproductive and even harmful.
Clinical definition to know: A moderate calorie restriction is generally defined as a 10–25% reduction below an individual's total daily energy expenditure (TDEE), sustained over weeks to months, while meeting all micronutrient requirements.
2. The Genomics Revolution: Why Your DNA Shapes Your Response
The CALERIE™ Genomic Data Resource
One of the most consequential advances in calorie restriction research came from the CALERIE™ Genomic Data Resource, a landmark dataset that documented molecular-level responses to sustained caloric reduction in humans (Ryan et al., 2024).
This resource identified specific genetic markers and epigenetic signatures associated with how individuals respond to calorie restriction. The core finding: your biology, not your willpower, determines a large part of your response to dietary restriction.
What Epigenetics Has to Do With Your Diet
Epigenetics refers to changes in gene expression that don't alter your DNA sequence itself but do change how your genes behave. Calorie restriction appears to trigger measurable epigenetic adaptations—including changes to DNA methylation patterns—that influence:
Metabolic rate regulation (how fast your body burns energy at rest)
Fat storage versus fat burning tendencies
Inflammatory signaling throughout the body
Biological age markers (separate from your chronological age)
Practical Implication: One-Size Dieting Is Obsolete
The CALERIE™ data makes one thing clear: the "calories in, calories out" equation is real but incomplete. Two people on identical caloric deficits can have dramatically different outcomes because of genetic and epigenetic variation.
This has enormous clinical implications. We are entering an era where genetic testing may one day tell you not just whether to restrict calories, but by how much, through which dietary approach, and for how long to generate the best metabolic outcomes for your specific biology.
3. How Calorie Restriction Works: The Cellular Mechanisms
Understanding the "why" behind calorie restriction demystifies the science—and helps you make better decisions about implementation.
3.1 AMPK and SIRT1 Activation
When calorie intake drops, cellular energy sensing changes. Two key regulators are activated:
AMPK (AMP-activated protein kinase): Often called the body's "energy gauge," AMPK signals a low-energy state and shifts the body toward fat burning, autophagy, and mitochondrial biogenesis.
SIRT1 (Sirtuin 1): A longevity-associated protein that regulates DNA repair, inflammation reduction, and metabolic adaptation.
Together, AMPK and SIRT1 activation are considered central to the anti-aging and metabolic benefits of calorie restriction.
3.2 mTOR Suppression
mTOR (mechanistic target of rapamycin) is a growth-promoting signaling pathway. Chronically elevated mTOR—common in overeating and sedentary lifestyles—is linked to accelerated aging, cancer risk, and metabolic dysfunction. Calorie restriction suppresses mTOR activity, shifting cellular resources from growth toward maintenance and repair.
3.3 Autophagy: Cellular Housekeeping
One of calorie restriction's most celebrated effects is the induction of autophagy—a process by which cells break down and recycle damaged proteins and organelles. Think of it as the body's internal "cellular cleaning crew."
Impaired autophagy is linked to neurodegeneration, cancer, and accelerated aging. Calorie restriction is one of the most reliable ways to stimulate autophagy in humans.
3.4 Improved Insulin Sensitivity
Calorie restriction reliably improves insulin sensitivity—the ability of your cells to respond appropriately to insulin. This has downstream benefits for blood sugar regulation, fat storage, and cardiovascular health.
3.5 Reduced Systemic Inflammation
Chronic low-grade inflammation underlies most modern chronic diseases. Calorie restriction reduces inflammatory markers including CRP, TNF-alpha, and IL-6—offering broad-spectrum protection against inflammation-driven disease.
4. Calorie Restriction and Weight Loss: What the Evidence Actually Shows
The Fundamentals Still Hold
The core mechanism of weight loss through calorie restriction is an energy deficit—consuming fewer calories than you expend. This reliably produces weight loss across populations when adherence is maintained.
However, the rate, composition, and sustainability of that weight loss vary enormously based on:
The size of the caloric deficit
Protein intake
Concurrent exercise (especially resistance training)
Hormonal status
Gut microbiome composition
Genetic variation in metabolic rate
Metabolic Adaptation: The Plateau Problem
One of the most clinically important phenomena in calorie restriction is metabolic adaptation—the body's tendency to downregulate energy expenditure in response to sustained caloric reduction.
When you eat significantly less, your body responds by:
Lowering resting metabolic rate (RMR)
Reducing thyroid hormone output (particularly T3)
Increasing hunger hormones (ghrelin)
Decreasing satiety hormones (leptin)
This is sometimes called the "hormonal hibernation" or "starvation response." It's not a moral failing—it's evolutionary survival biology.
The solution: Moderate deficits (10–20% below TDEE), adequate protein (1.2–1.5 g/kg body weight), and strategic diet breaks or refeeds help preserve metabolic rate during sustained calorie restriction.
Muscle Loss: The Silent Risk
A critical but often ignored consequence of calorie restriction without resistance training is sarcopenic weight loss—losing muscle alongside fat. Muscle tissue is metabolically expensive to maintain; the body readily breaks it down during caloric deficits.
Why this matters: muscle is your primary metabolic tissue. Losing it during a diet actively slows your metabolism, making future weight maintenance harder and increasing long-term health risks.
Non-negotiable protocol: Resistance training 2–3 times per week combined with protein intake of 1.2–1.5 g/kg/day is essential to preserve lean mass during calorie restriction.
5. Brain Health and Mental Health: The Surprising Benefits
Calorie Restriction as a Psychiatric Intervention
Perhaps the most surprising development in recent calorie restriction research is its potential as a therapeutic tool for mental health. A 2025 review by Nguyen et al. published in Frontiers in Psychiatry argued that "less is more" when it comes to caloric intake and brain function.
The paper reviewed evidence suggesting calorie restriction may benefit:
Depression and anxiety — through reduced neuroinflammation and improved metabolic flexibility
Cognitive function — via enhanced autophagy and mitochondrial efficiency in neurons
Emotional regulation — through modulation of the gut-brain axis and neurotransmitter systems
Critically, these benefits appear to be partially independent of weight loss itself—meaning the metabolic changes triggered by caloric reduction may directly benefit brain function regardless of how much weight is lost.
The Neuroinflammation Mechanism
Modern psychiatry increasingly recognizes neuroinflammation—chronic low-grade inflammation within the brain—as a driver of depression, anxiety, cognitive decline, and even certain psychotic disorders.
Calorie restriction combats neuroinflammation through:
Reduced systemic inflammatory cytokines crossing the blood-brain barrier
Activation of ketone metabolism, which provides anti-inflammatory fuel for neurons
Autophagy-mediated clearance of damaged proteins that trigger inflammatory cascades
Brain Aging: The Monkey Data
A 2026 study published in Aging Cell (Vitantonio et al.) examined calorie restriction's effects on brain aging in non-human primates—the closest animal model to humans. The findings were striking: calorie restriction significantly attenuated transcriptional aging signatures in white matter oligodendrocytes and brain immune cells (microglia) of the monkey brain.
In practical terms, calorie restriction appeared to slow the molecular aging of critical brain cells, particularly those responsible for myelin maintenance and neuroinflammatory regulation. These findings extend previous rodent data to a primate context, strengthening the case for calorie restriction's neuroprotective effects.
6. Cardiovascular and Metabolic Disease Risk Reduction
The CALERIE 2 Trial: Landmark Human Evidence
One of the most important pieces of human evidence comes from the CALERIE 2 trial, a rigorous randomized controlled trial examining calorie restriction in non-obese adults. A 2026 analysis by Chang et al. published in Diabetes, Obesity & Metabolism assessed the effect of calorie restriction on predicted cardiovascular and type 2 diabetes risk in young adults.
The findings were clinically meaningful: sustained calorie restriction produced measurable reductions in predicted risk for both cardiovascular disease and type 2 diabetes—even in participants who were not obese at baseline.
This is significant because it suggests calorie restriction's metabolic benefits extend beyond weight loss and may independently modify cardiometabolic risk factors including:
Blood pressure
LDL cholesterol and triglycerides
Fasting insulin and glucose
Inflammatory markers
Insulin Sensitivity: A Central Benefit
Improved insulin sensitivity may be the single most impactful metabolic change produced by calorie restriction. Greater insulin sensitivity reduces the risk of type 2 diabetes, reduces cardiovascular disease risk, improves energy utilization, and helps regulate body fat distribution.
7. Longevity and Aging: What Animal and Human Studies Tell Us
The Science of Dietary Restriction and Lifespan
A comprehensive 2026 review in Nature Aging (Schmauck-Medina et al.) synthesized decades of evidence on dietary restriction and longevity across species. Key findings:
Calorie restriction extends lifespan in multiple model organisms including yeast, worms, flies, and rodents
In non-human primates, calorie restriction reduces age-related disease and improves metabolic markers
In humans, it reliably improves biomarkers associated with healthy aging, though direct lifespan data is not yet available
The review also highlighted that how you restrict matters: severe restriction produces different effects than moderate restriction, and the timing of food intake interacts with caloric quantity in complex ways.
Biological Age vs. Chronological Age
One of the most compelling findings from the CALERIE trial program is that calorie restriction appears to slow biological aging—as measured by epigenetic clocks and other aging biomarkers—even when chronological age continues to advance.
This distinction matters clinically: a person who is 50 years old chronologically but has biological markers more consistent with a 42-year-old faces a very different disease trajectory than someone whose biological age matches their chronological age.
8. Calorie Restriction vs. Time-Restricted Eating: Head-to-Head
The 2025 Randomized Trial
A major 2025 randomized controlled trial by Oldenburg et al. published in Obesity directly compared three approaches:
Time-restricted eating (TRE) — eating within a defined window (typically 8–10 hours), without explicit calorie counting
Caloric reduction (CR) — deliberate reduction of daily caloric intake by 25%
Unrestricted eating — no dietary constraints (control group)
Key Findings
Outcome Time-Restricted Eating Caloric Reduction Unrestricted Weight loss Significant Greater Minimal Metabolic improvement Yes Yes No Adherence Higher Moderate N/A Calorie counting required No Yes No Mechanism Circadian alignment + mild deficit Energy deficit None
Bottom line from the trial: Both TRE and CR produce meaningful weight loss and metabolic improvements compared to unrestricted eating. CR produces slightly greater weight loss, but TRE shows significantly higher long-term adherence for many people—and since the best diet is the one you actually maintain, TRE may be more effective in real-world practice.
Who Should Choose Which?
Caloric restriction may be better for:
People who respond well to structured plans and tracking
Those with specific, time-sensitive weight loss goals
Individuals working closely with a registered dietitian
Time-restricted eating may be better for:
People who find calorie counting psychologically burdensome
Those with irregular schedules who can control their eating window more easily than their portion sizes
Individuals primarily seeking metabolic benefits rather than rapid weight loss
9. Plant-Based Calorie Restriction: A Smarter Alternative?
A New 2026 Clinical Trial
A 12-week randomized, open-label, non-inferiority trial published in Frontiers in Nutrition (Mutailipu et al., 2026) compared plant-based calorie-restricted diets against conventional calorie-restricted diets for weight loss and metabolic health in adults with obesity.
The plant-based approach was found to be non-inferior to conventional CR for weight loss—meaning it worked just as well—while offering additional advantages:
Higher fiber intake supports gut microbiome diversity
Lower saturated fat, benefiting cardiovascular risk
Greater antioxidant intake, reduces oxidative stress
Higher satiety per calorie, potentially improving adherence
The Enhanced Mediterranean Diet Angle
Separately, a 2026 study from the Universidad de Navarra reported that an optimized, "smarter" Mediterranean diet was associated with a 31% reduction in type 2 diabetes risk. While not a calorie restriction study per se, the findings underscore the importance of diet quality, not just caloric quantity, in metabolic outcomes.
Combining calorie restriction principles with Mediterranean or plant-forward dietary patterns may represent the most evidence-backed approach to simultaneous weight loss, metabolic improvement, and long-term disease prevention.
10. Calorie Restriction Mimetics: The Future of Fasting Without Fasting
Calorie restriction mimetics (CRMs) are compounds—pharmaceutical or nutraceutical—that activate the same cellular pathways triggered by actual caloric reduction, without requiring dietary restriction. A 2025 review by Chaudhary et al. in Biogerontology catalogued the current state of evidence.
Key pathways targeted by CRMs include:
SIRT1 activation (resveratrol, NAD+ precursors like NMN and NR)
AMPK activation (metformin, berberine)
mTOR inhibition (rapamycin, spermidine)
Autophagy induction (spermidine, urolithin A)
What the Evidence Currently Shows
Resveratrol
Target pathway: SIRT1 activation
Human evidence: Mixed results
Status: Widely available supplement
NMN / NR (Nicotinamide Mononucleotide / Nicotinamide Riboside)
Target pathway: NAD+ / SIRT1 activation
Human evidence: Promising but still early
Status: Dietary supplements
Metformin
Target pathway: AMPK activation
Human evidence: Strong evidence in diabetes and metabolic disease
Status: Prescription medication
Berberine
Target pathway: AMPK activation
Human evidence: Moderate evidence
Status: Natural supplement
Spermidine
Target pathway: Autophagy induction
Human evidence: Promising but early-stage
Status: Supplement
Rapamycin
Target pathway: mTOR inhibition
Human evidence: Strong animal data; emerging human evidence
Status: Investigational drug for longevity research
The Honest Caveat
CRMs are not a replacement for actual dietary change. The most honest summary of the current evidence is that they may complement calorie restriction—providing additional pathway activation on days when dietary adherence is imperfect—but they are unlikely to replicate the full breadth of benefits achieved through sustained calorie restriction in well-nourished individuals.
They represent a genuine and exciting frontier in longevity medicine, but should be approached with appropriate evidence-based caution.
11. The Real Risks and Downsides You Need to Know
A 2025 review in Nature Reviews Endocrinology (Wang & Speakman) provided a critical counterbalance to calorie restriction enthusiasm by comprehensively documenting its potential downsides. This is essential reading for anyone considering a prolonged caloric deficit.
Key Risks of Calorie Restriction
1. Muscle Loss (Sarcopenia) Without sufficient protein and resistance exercise, calorie restriction produces lean mass loss alongside fat loss. This undermines metabolic rate and long-term health outcomes.
Mitigation: Protein intake of 1.2–1.5 g/kg body weight daily + resistance training 2–3x/week.
2. Hormonal Disruption Extreme caloric restriction can suppress the hypothalamic-pituitary-thyroid (HPT) axis, reducing T3 output and effectively lowering metabolic rate. In women, it can disrupt the menstrual cycle and reproductive hormones.
Mitigation: Keep deficits moderate (10–20% below TDEE). Avoid deficits below 1,200 kcal/day for women and 1,500 kcal/day for men without medical supervision.
3. Bone Density Reduction Long-term calorie restriction, particularly in women, is associated with reduced bone mineral density—a risk factor for osteoporosis and fracture. This risk is amplified when calcium and vitamin D intake is inadequate.
Mitigation: Ensure adequate calcium (1,000–1,200 mg/day) and vitamin D. Include weight-bearing exercise.
4. Immune Function Compromise Severe calorie restriction can impair immune cell production and function, increasing susceptibility to infection and reducing vaccine response efficacy.
Mitigation: Ensure adequate micronutrient intake (zinc, vitamin C, vitamin D, iron). Avoid extreme deficits.
5. Disordered Eating Risk For individuals with a history of—or vulnerability to—eating disorders, calorie restriction protocols involving tracking and restriction can trigger or exacerbate disordered eating patterns.
Mitigation: A thorough clinical assessment before starting. Anyone with a history of eating disorders should work only with a multidisciplinary team including a registered dietitian and mental health professional.
6. Psychological Stress Even in individuals without eating disorder history, sustained calorie restriction can increase preoccupation with food, social anxiety around eating, and emotional relationship with meals.
Mitigation: Consider time-restricted eating as an alternative that achieves similar metabolic goals with less cognitive burden. Build in planned "diet breaks."
⚠️ Safety Warning: Always consult a qualified healthcare professional before beginning any calorie restriction protocol, particularly if you have a history of eating disorders, are pregnant or breastfeeding, have a chronic metabolic condition, or take medications that interact with dietary changes.
12. How to Start Calorie Restriction Safely: A Practical Protocol
Step 1: Calculate Your Baseline
Before restricting anything, know your numbers:
TDEE (Total Daily Energy Expenditure): Use a validated online calculator incorporating your age, sex, height, weight, and activity level
Target deficit: Start with 10–15% below TDEE for most people; 20% for those under close medical supervision
Minimum safe floor: Do not go below 1,200 kcal/day (women) or 1,500 kcal/day (men) without medical oversight
Step 2: Prioritize Protein
Set your protein target first—then fill remaining calories with carbohydrates and fats:
General population: 1.2–1.5 g/kg body weight per day
Active individuals or those over 60: 1.5–2.0 g/kg body weight per day
Sources: Lean meats, fish, eggs, legumes, Greek yogurt, tofu, tempeh
Step 3: Focus on Nutrient Density
Every calorie should earn its place. During restriction, food quality matters more, not less:
Prioritize vegetables, fruits, legumes, whole grains, and lean proteins
Minimize ultra-processed foods, refined carbohydrates, and liquid calories
Consider a high-quality multivitamin to fill micronutrient gaps
Step 4: Add Resistance Training
Minimum: 2 sessions per week targeting major muscle groups
Ideal: 3 sessions per week with progressive overload
This is not optional for preserving metabolic rate and lean mass
Step 5: Track, Adjust, and Monitor
Use a food tracking app for the first 4–8 weeks to calibrate portion awareness
Reassess weight and body composition (not just scale weight) every 4 weeks
Watch for signs of excessive restriction: fatigue, hair loss, cold intolerance, menstrual irregularity, persistent irritability
Schedule check-ins with your doctor or dietitian every 8–12 weeks
Beginner-Friendly Weekly Template
Monday: Track calories + resistance training
Tuesday: Track calories + light activity (walk, yoga)
Wednesday: Track calories + resistance training
Thursday: Flexible tracking (stay within calorie target)
Friday: Track calories + resistance training
Saturday: Social eating (stay within weekly calorie budget)
Sunday: Rest, meal prep + plan the week ahead
13. Common Myths and Mistakes
Myth 1: "Eating Less Is Always Better"
Reality: Extreme restriction triggers hormonal adaptations that make weight loss harder, not easier. The evidence consistently supports moderate deficits (10–20% below TDEE) over aggressive ones. Eating too little can paradoxically stall fat loss while accelerating muscle loss.
Myth 2: "All Calories Are Equal"
Reality: While a caloric deficit drives weight loss, the composition of those calories profoundly affects body composition, metabolic health, hormonal balance, and satiety. 500 calories of salmon and vegetables produces very different physiological outcomes than 500 calories of ultra-processed snacks.
Myth 3: "Calorie Restriction Destroys Your Metabolism Permanently"
Reality: Metabolic adaptation during calorie restriction is real but not permanent. Metabolic rate largely recovers when adequate calories are restored—particularly when muscle mass is preserved through protein and resistance training. Long-term "metabolic damage" is largely a myth unsupported by current evidence.
Myth 4: "Time-Restricted Eating Is Just Skipping Breakfast"
Reality: TRE produces distinct metabolic effects through circadian biology, independent of calorie reduction. Aligning food intake with circadian rhythms improves insulin sensitivity, fat oxidation, and gut microbiome health through mechanisms beyond simple caloric restriction.
Myth 5: "Supplements Can Replace Calorie Restriction"
Reality: Calorie restriction mimetics show promise, but no supplement currently replicates the full spectrum of benefits produced by actual sustained caloric reduction in properly nourished individuals. Supplements may complement CR; they do not replace it.
Myth 6: "Calorie Restriction Is Only for Overweight People"
Reality: The CALERIE 2 trial demonstrated meaningful cardiometabolic benefits from calorie restriction in non-obese young adults—suggesting that metabolic improvements accrue independently of starting weight or obesity status.
14. Evidence Summary Table
Ryan et al. (2024 | Genomic): Individual responses to calorie restriction are heavily shaped by unique genetic and epigenetic profiles.
Nguyen et al. (2025 | Review): Calorie restriction demonstrates notable therapeutic potential for mitigating depression, anxiety, and cognitive decline.
Oldenburg et al. (2025 | RCT): Both traditional calorie restriction and time-restricted eating drive weight loss, but time-restricted eating yields higher long-term adherence.
Wang & Speakman (2025 | Review): Documented risks of prolonged calorie restriction include sarcopenia (muscle loss), hormonal disruption, and compromised immune function.
Chaudhary et al. (2025 | Review): Calorie restriction mimetics targeting SIRT1 and AMPK pathways show early anti-aging and anti-inflammatory promise.
Chang et al. (2026 | RCT Analysis): Sustained calorie restriction significantly reduces predicted cardiovascular disease and type 2 diabetes risk, even in non-obese young adults.
Vitantonio et al. (2026 | Primate Study): Calorie restriction protects the central nervous system by slowing down transcriptional brain aging in white matter and immune cells.
Mutailipu et al. (2026 | RCT): Plant-based calorie restriction is clinically non-inferior to conventional approaches for weight loss and metabolic optimization.
Schmauck-Medina et al. (2026 | Review): Dietary restriction reliably extends healthspan across multiple species, with supportive human biological marker trends emerging.
Universidad de Navarra (2026 | Epidemiological): Adherence to an optimized, "smarter" Mediterranean diet pattern reduces type 2 diabetes risk by 31%
15. Frequently Asked Questions
Q1: How much should I restrict calories to lose weight without losing muscle?
A moderate deficit of 10–20% below your TDEE is the evidence-based starting point for preserving lean mass. Pair this with a protein intake of 1.2–1.5 g/kg body weight and resistance training 2–3 times per week. Expect weight loss of approximately 0.5–1 lb (0.25–0.5 kg) per week. Faster loss typically comes at the cost of muscle tissue and metabolic rate.
Q2: Is time-restricted eating as effective as counting calories?
According to the 2025 Oldenburg et al. randomized trial, caloric restriction produces slightly greater weight loss than time-restricted eating alone. However, TRE achieves comparable metabolic improvements and demonstrates significantly higher long-term adherence in many people. If counting calories feels unsustainable, TRE is a clinically valid alternative.
Q3: Can calorie restriction improve depression or anxiety?
Emerging evidence—including a 2025 Frontiers in Psychiatry review—suggests moderate calorie restriction may reduce neuroinflammation and improve mood, cognitive function, and emotional regulation. These effects appear to be partially independent of weight loss. However, calorie restriction is not a replacement for established psychiatric care, and those with mental health conditions should discuss any dietary changes with their doctor.
Q4: What are the warning signs that my calorie restriction has gone too far?
Warning signs of excessive restriction include persistent fatigue, hair loss or thinning, feeling cold all the time, irregular or absent menstrual cycles, significant mood changes or irritability, difficulty concentrating, frequent illness, and loss of strength. If you experience these, increase caloric intake and consult a healthcare provider.
Q5: Does calorie restriction slow aging?
The 2026 Nature Aging review (Schmauck-Medina et al.) confirms that calorie restriction reliably extends lifespan and healthspan in multiple animal models. In primates, it reduces age-related disease. In humans, it measurably slows biological aging biomarkers. Direct human longevity data is not yet available, but the mechanistic and biomarker evidence is compelling.
Q6: Is a plant-based calorie-restricted diet better than a conventional one?
A 2026 randomized trial found plant-based CR to be non-inferior to conventional CR for weight loss, with potential advantages in fiber intake, cardiovascular markers, and gut microbiome health. Plant-based approaches can be highly effective when planned to include adequate protein and vitamin B12, iron, zinc, and omega-3 fatty acids.
Q7: Are calorie restriction mimetics like resveratrol worth taking?
Current evidence suggests CRMs like resveratrol, NMN, and berberine activate some relevant pathways but do not fully replicate actual calorie restriction benefits. Berberine and metformin show the strongest AMPK-activating evidence in humans. These compounds may be useful adjuncts to dietary restriction, but should not replace it. Consult your doctor before starting any supplementation.
Q8: Is calorie restriction safe for older adults?
Older adults face heightened risk of sarcopenia (muscle loss) during calorie restriction, which can significantly impact function and longevity. If calorie restriction is appropriate for an older adult, it must be coupled with higher protein targets (1.5–2.0 g/kg body weight) and consistent resistance training. Medical supervision is particularly important in this population.
Q9: How long does it take to see metabolic benefits from calorie restriction?
Improvements in insulin sensitivity and inflammatory markers can appear within 2–4 weeks of moderate calorie restriction. More substantial changes in body composition, blood lipids, and biological aging markers typically emerge over 12–24 weeks. The CALERIE trials used 2-year sustained restriction to assess long-term effects.
Q10: Who should NOT try calorie restriction?
Calorie restriction is not appropriate—without close medical and nutritional supervision—for: pregnant or breastfeeding individuals; children and adolescents; those with active eating disorders or eating disorder history; individuals who are already underweight; people with certain chronic diseases (kidney disease, liver disease, cancer); and those on medications that interact with significant dietary changes (e.g., certain diabetes medications, blood thinners).
Q11: Can I combine time-restricted eating with calorie restriction?
Yes, and the combination may be synergistic. Restricting both when and how much you eat addresses both circadian biology and energy balance simultaneously. However, combining approaches increases cognitive and behavioral demands, so it's wise to implement one at a time before combining.
Q12: Does gut health affect how I respond to calorie restriction?
The gut microbiome significantly influences metabolic health, inflammation, and weight regulation. Emerging evidence suggests that microbiome composition partially determines individual responses to calorie restriction. High-fiber, plant-forward calorie restriction diets may enhance gut microbiome diversity while achieving a caloric deficit—a potential "two birds, one stone" approach.
Clinical pearls
1. The "Metabolic Thermostat"
Sustained caloric deficits trigger adaptive thermogenesis—a survival-driven downregulation of the resting metabolic rate (RMR) mediated by decreased circulating triiodothyronine (T3), leptin, and sympathetic nervous system activity. This biological adaptation often outpaces mass-dependent metabolic declines, resulting in early weight-loss plateaus. To preserve metabolic rate, employ a conservative deficit (10\% to 15\%) and consider structured diet breaks (e.g., 1–2 weeks at calculated maintenance every 8–12 weeks) to transiently restore leptin signaling and thyroid hormone expression.
"Think of your metabolism like a smart home thermostat. If you suddenly cut your food intake too drastically, your body thinks there is a shortage outside, so it turns down its energy thermostat to save power. This is why crashing your calories stops weight loss and leaves you feeling exhausted and cold. By taking a slow, gentle approach and inserting brief, planned 'rest weeks' where you eat at your normal baseline, we keep your internal thermostat running hot."
2. The Sarcopenia / Lean Mass Retention
Calorie restriction without targeted interventions induces a catabolic state where up to 25% of total weight lost can derive from skeletal muscle and lean tissue, accelerating age-related sarcopenia. This loss impairs glucose disposal (as skeletal muscle is the primary site for insulin-stimulated glucose uptake) and reduces baseline energy expenditure. Mitigating this requires a non-negotiable dual protocol: progressive resistance hyper-loading to stimulate muscle protein synthesis via mechanical tension, paired with an elevated protein intake
"When you eat less, your body looks inside for extra fuel. If you aren't actively lifting weights, your body will actually burn muscle tissue for energy instead of just burning fat. Muscle is your body's main engine; losing it permanently slows your metabolism and weakens your body. To protect it, we treat strength training and eating high-quality protein as a mandatory medicine, not an optional hobby, while you're on fewer calories."
3. The Neuroinflammation & Cognitive Clarity
The cognitive and mood-stabilizing benefits of moderate calorie restriction are largely independent of weight loss and are driven by a reduction in neuroinflammation. Caloric restriction downregulates circulating systemic pro-inflammatory cytokines (such as IL-6 and TNF \alpha) that cross the blood-brain barrier. Furthermore, it shifts the central nervous system toward ketone utilization and stimulates brain-derived neurotrophic factor ($\text{BDNF}$), protecting white matter oligodendrocytes and modulating microglial activation.
"Most people think eating less is just about changing your waistline, but it actually changes your brain chemistry. Chronic overeating causes low-grade, silent inflammation in the brain, which can cloud your thinking and worsen anxiety or low mood. A clean, moderate reduction in food clears out that cellular smoke, acts like an anti-inflammatory for your brain cells, and gives you a level of mental clarity and steady energy that most people don't expect."
4. The Circadian Alignment / Compliance
When comparing traditional calorie restriction (CR) to time-restricted eating (TRE) head-to-head, clinical trials show that while CR yields slightly higher absolute fat loss, TRE demonstrates significantly higher patient adherence. TRE leverages circadian biology to optimize insulin sensitivity during daylight hours without requiring meticulous macronutrient logging. For patients with high psychological resistance to calorie counting or those prone to food tracking anxiety, prescribing a consistent 10-hour eating window serves as a highly effective surrogate that naturally creates a passive caloric deficit.
"The absolute best nutrition plan is the one you can actually stick to long-term. If counting numbers and weighing food every day sounds stressful to you, we can focus on the clock instead of the numbers. By simply eating all of your meals within a steady 10-hour daytime window and letting your digestive system rest for the remaining 14 hours, you get almost all the same health and metabolic benefits without the mental exhaustion of tracking every single bite."
5. The Bone Mineral Density (BMD)
Long-term calorie restriction introduces an understated risk of accelerating bone mineral density loss, particularly in postmenopausal women and individuals with low baseline body mass index. This occurs due to mechanical unloading (carrying less mass) and potential reductions in systemic estrogen and IGF-1 levels. Clinical screening should include a baseline risk assessment, strict monitoring of mechanical axial-loading exercise, and optimization of nutritional cofactors, ensuring a minimum daily intake of 1,000–1,200 mg of elemental calcium along with therapeutic levels of Vitamin D
"As you lose weight, your bones carry less load, and your body naturally changes how it builds bone tissue. If we aren't careful, eating fewer calories can inadvertently thin your bones, raising your risk of fractures later in life. We prevent this by doing two things: making sure you get plenty of calcium and Vitamin D, and doing weight-bearing exercises—like walking or resistance training—which signal your bones to stay dense, thick, and strong."
6. The "Nutrient Density Floor"
As total daily energy intake decreases, the margin for nutritional error narrows drastically. In a calorie-restricted state, the dietary pattern must shift strictly toward high nutrient-density to avoid subclinical micronutrient deficiencies (such as zinc, magnesium, iron, and B-vitamins) that impair mitochondrial efficiency and immune function. A plant-forward or enhanced Mediterranean framework is ideal because its volumetric properties maintain gastric distension (stimulating satiety via mechanoreceptors) while providing superior micronutrient-to-calorie ratios compared to conventional restrictive patterns.
"When you lower your daily food budget, every single calorie has to work twice as hard for you. You can't afford to waste calories on 'empty' foods that don't offer vitamins or minerals. We want to pack your plate with colourful vegetables, lean proteins, and healthy fats. This fills up your stomach physically so you don't feel hungry, while giving your cells the exact tools they need to protect your immune system and keep your energy high."
16. Conclusion and Action Steps
The science of calorie restriction in 2026 tells a story that is simultaneously more nuanced and more exciting than the simple "eat less, weigh less" narrative that dominated for decades.
We now know that calorie restriction:
Triggers sophisticated epigenetic adaptations that vary meaningfully between individuals
Produces measurable reductions in cardiovascular and diabetes risk, even in non-obese young adults
Slows brain aging and may serve as a therapeutic tool for neuroinflammation, depression, and anxiety
Extends healthspan markers across species, including non-human primates
Can be achieved through multiple dietary architectures—classical caloric reduction, time-restricted eating, or plant-based CR—with adherence determining success more than method
It also carries real risks—muscle loss, hormonal disruption, bone density reduction, and psychological harm—that demand evidence-based management and appropriate medical oversight.
Your Next Steps
Calculate your TDEE using a validated online tool and set a moderate deficit target of 10–15%
Set your protein target first: 1.2–1.5 g/kg body weight daily
Choose your approach: Classical CR, time-restricted eating, or a plant-forward combination based on your lifestyle and preferences
Add resistance training: Minimum 2 sessions per week—non-negotiable for metabolic preservation
Monitor progress holistically: Body composition, energy, mood, and lab markers—not just scale weight
Consult a healthcare professional before beginning, especially if you have any existing health conditions or medication concerns
Build in sustainability: Diet breaks, flexible social eating, and long-term habit formation matter more than short-term perfection
Calorie restriction, done thoughtfully and with appropriate support, is one of the most evidence-backed tools available for weight management, metabolic health, and healthy aging. The key is informed, individualized application—not rigid, universal prescription.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Beyond Glucose: Lipotoxicity as the Central Mechanism of Metabolic Disease | DR T S DIDWAL
Time-Restricted Eating: Metabolic Advantage or Just Fewer Calories? | DR T S DIDWAL
Can You Revitalize Your Immune System? 7 Science-Backed Longevity Strategies | DR T S DIDWAL
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
Light and Longevity: Can Sunlight Slow Cellular Aging? | DR T S DIDWAL
References
Chang, R., Claggett, B. L., Redman, L. M., Ravussin, E., Apovian, C. M., & Ostrominski, J. W. (2026). Effect of caloric restriction on predicted risk of incident cardiovascular disease and type 2 diabetes in young adults: Findings from the CALERIE 2 trial. Diabetes, Obesity and Metabolism, 28(2), 1565–1568. https://doi.org/10.1111/dom.70308
Chaudhary, S., Chaudhary, M. R., & Jena, M. K. (2025). Calorie restriction mimetics against aging and inflammation. Biogerontology, 26(1), 126. https://doi.org/10.1007/s10522-025-10269-0
Mutailipu, K., Yang, L., Fang, Y., Lei, S., Guo, J., Yuan, H., Liu, S., Chen, Y., Zhu, C., Qu, S., Zhao, F., & Bu, L. (2026). Plant-based caloric restriction diets versus conventional calorie-restricted diets for weight loss and metabolic health in obese adults: A 12-week randomized, open-label, non-inferiority trial. Frontiers in Nutrition, 13, Article 1805225. https://doi.org/10.3389/fnut.2026.1805225
Nguyen, J. C. D., Govic, A., Levay, E. A., Zelko, M. D., Arumugam, T. V., Penman, J., Johns, T. G., & Boskovic, Z. (2025). Less is more: Calorie restriction as a therapeutic for mental health disorders. Frontiers in Psychiatry, 16, Article 1584890. https://doi.org/10.3389/fpsyt.2025.1584890
Oldenburg, N., Mashek, D. G., Harnack, L., Wang, Q., Manoogian, E. N. C., Evanoff, N., Dengel, D. R., Taddese, A., Yentzer, B. P., Lysne, L., Wong, A., Hanson, M., Anderson, J. D., Alvear, A., LaPage, N., Ryder, J., Varady, K., Gao, Z., Ryu, S., & Chow, L. S. (2025). Time-restricted eating, caloric reduction, and unrestricted eating effects on weight and metabolism: A randomized trial. Obesity, 33(4), 671–684. https://doi.org/10.1002/oby.24252
Ryan, C. P., Corcoran, D. L., Banskota, N., Indik, C. E., Floratos, A., Friedman, R. A., Kobor, M. S., Kraus, V. B., Kraus, W., MacIsaac, J. L., Orenduff, M. C., Pieper, C. F., White, J. P., Ferrucci, L., Horvath, S., Huffman, K. M., & Belsky, D. W. (2024). The CALERIE™ genomic data resource [Preprint]. bioRxiv. https://doi.org/10.1101/2024.05.17.594714
Schmauck-Medina, T., Lautrup, S., Di Francesco, A., Mitchell, S. J., Clemmensen, C., Partridge, L., Roth, G. S., Anderson, R. M., Mattison, J. A., de Cabo, R., Speakman, J. R., Richardson, A., Ingram, D. K., Weindruch, R., Mattson, M. P., & Fang, E. F. (2026). Dietary restriction in aging and longevity. Nature Aging, 6(3), 485–505. https://doi.org/10.1038/s43587-026-01091-5
Universidad de Navarra. (2026, May 19). Scientists found a smarter Mediterranean diet that slashes diabetes risk by 31%. ScienceDaily. https://www.sciencedaily.com/releases/2026/05/260519003103.htm
Vitantonio, A. T., Dimovasili, C., Liu, Y., Wang, Z., Zhang, B., Bennett, D. A., & Shubin, A. V. (2026). Calorie restriction attenuates transcriptional aging signatures in white matter oligodendrocytes and immune cells of the monkey brain. Aging Cell, 25(1), e70298. https://doi.org/10.1111/acel.70298
Wang, A., & Speakman, J. R. (2025). Potential downsides of calorie restriction. Nature Reviews Endocrinology, 21(7), 427–440. https://doi.org/10.1038/s41574-025-01111-1
This article is intended for informational and educational purposes only and does not constitute medical advice. Individual health circumstances vary significantly, and any dietary intervention—including calorie restriction—should be discussed with a qualified healthcare professional before implementation. The author and publisher are not liable for decisions made based on information in this article.
Author: Dr. T.S. Didwal, M.D. (Internal Medicine) Last updated: May 2026 Reviewed against peer-reviewed literature current as of May 2026