Losing Muscle With Age? Here's How Nutrition Can Help Protect Your Strength
Muscle loss isn't inevitable. Learn the best foods, protein targets, supplements, and dietary patterns to preserve muscle and independence as you age.
NUTRITIONSARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/2/202614 min read
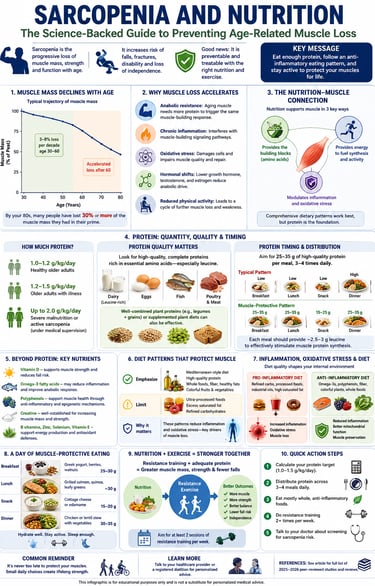
Sarcopenia is the age-related loss of muscle mass, strength, and physical function. The best evidence shows it can be slowed or partially reversed with adequate protein (1.0–1.5 g/kg/day for most older adults), resistance training, and an anti-inflammatory, nutrient-rich diet that supports muscle protein synthesis and reduces chronic inflammation.
Key takeaways:
Sarcopenia is a Clinical Pathology, Not an Inevitable Fate
Sarcopenia has moved past the vague category of "getting old" and is formally recognized as a distinct medical disease. While normal aging includes minor muscle loss, sarcopenia crosses a dangerous threshold that directly spikes the risk of falls, physical disability, and early mortality—meaning it requires proactive, targeted clinical treatment rather than passive acceptance.
The Baseline RDA for Protein is Completely Inadequate for Aging Muscle
The standard Recommended Dietary Allowance (RDA) of $0.8\text{ g/kg/day}$ was calculated to prevent basic nutritional deficiency in young adults, not to maintain muscle tissue in an aging body. To fight off age-related decline, healthy older adults require a significantly higher baseline of $1.0\text{ to }1.2\text{ g/kg/day}$, escalating up to $1.5\text{ g/kg/day}$ during illness or active muscle loss.
Anabolic Resistance Rewrites the Rules of Protein Timing
Aging muscle suffers from "anabolic resistance"—a cellular blunting where the body requires a much stronger signal to trigger Muscle Protein Synthesis (MPS). To bypass this, protein cannot simply be dumped into a single large dinner; it must be evenly distributed across 3 to 4 daily meals, ensuring each meal hits a threshold of 25 to 35 grams of protein to successfully switch on the muscle-building machinery.
Leucine Acts as the Indispensable Molecular Trigger
Total protein volume matters, but its amino acid profile dictates its success. The essential amino acid leucine acts as the definitive metabolic trigger for building muscle tissue. Because animal-based proteins (dairy, eggs, poultry, fish) are naturally dense in highly digestible leucine, they hold a slight efficiency edge, requiring plant-based diets to be highly intentional with food combinations to match the same muscle-building signal.
Systemic Inflammation Actively Derails Muscle Construction
Simply meeting protein quotas is not enough if your systemic environment is highly inflamed. Chronic low-grade inflammation ("inflammaging") actively disrupts the critical mTOR signaling pathway responsible for synthesizing new muscle. A diet high in ultra-processed foods and saturated fats creates an internal environment that functionally blocks the body from using dietary protein to repair its muscles.
Isolated Nutrient Supplementation Falls Short of Whole-Diet Synergy
Chasing single "magic bullets" like isolated Vitamin D or protein powders delivers inferior clinical outcomes compared to structured, whole-diet frameworks. While targeted supplements play a valuable supporting role (especially creatine and correcting verified Vitamin D deficiencies), the strongest evidence favors multi-layered, Mediterranean-style dietary patterns rich in anti-inflammatory omega-3s, fiber, and polyphenols.
Nutrition and Resistance Training are Muscular Co-Dependencies
Dietary interventions hit a hard physiological ceiling without physical stimulation. Mechanical tension from progressive resistance training is the single most powerful trigger for muscle synthesis. Umbrella reviews confirm that combining targeted nutrition with at least two weekly resistance-training sessions outperforms any single-domain strategy for reversing frailty and lowering fall risks.
Proactive Intervention Must Shift Down to the 40s and 50s
Skeletal muscle mass and functional strength peak in a person's 30s, followed by a steady decline of 3% to 8% per decade that aggressively accelerates after age 60. The optimal window for high-yield preventative nutrition and strength habits begins in your 40s and 50s, building a structural "buffer" before severe metabolic and hormonal shifts take hold.
Somewhere around age 40, your body starts a quiet process that most people never notice until it's already cost them strength, balance, or independence. It's called sarcopenia — the progressive loss of skeletal muscle mass, strength, and function that comes with aging.
The encouraging news: sarcopenia is not an unstoppable fate. A growing body of nutrition science shows that what you eat — and specifically how much protein, which nutrients, and in what pattern — can meaningfully slow, prevent, or even partially reverse this decline.
1. What Is Sarcopenia?
Sarcopenia is a progressive, generalized skeletal muscle disorder characterized by accelerated loss of muscle mass and function. Unlike the gradual, near-invisible muscle loss everyone experiences with age, sarcopenia crosses a clinical threshold — one associated with a much higher risk of falls, fractures, physical disability, loss of independence, and mortality.
Muscle mass typically peaks in your 30s, then declines by roughly 3–8% per decade after age 30, with the rate accelerating after 60. By your 80s, many people have lost 30% or more of the muscle mass they had in their prime.
Key point: Sarcopenia is now formally recognized as a disease (with its own diagnostic code), not simply an inevitable byproduct of "getting old." That distinction matters — it means it can be screened for, diagnosed, and treated, and nutrition is one of the primary treatment levers available.
2. Why Muscle Loss Accelerates With Age
Several overlapping mechanisms drive sarcopenia:
Anabolic resistance — aging muscle becomes less responsive to the same amount of dietary protein, requiring a higher per-meal dose to trigger the same muscle-protein-synthesis response as in younger adults.
Chronic low-grade inflammation ("inflammaging") — elevated inflammatory markers interfere with the signaling pathways that build and maintain muscle tissue.
Oxidative stress — accumulated cellular damage impairs mitochondrial function within muscle fibers, reducing both muscle quality and capacity for repair.
Hormonal shifts — declining growth hormone, testosterone, and estrogen (post-menopause) all reduce the anabolic environment needed for muscle maintenance.
Reduced physical activity — sedentary behavior compounds all of the above, creating a feedback loop of further muscle loss.
Recent research increasingly points to genetic susceptibility interacting with dietary protein intake and inflammatory status, suggesting sarcopenia risk isn't just about what you eat, but how your individual biology responds to it. This is an area of active investigation and personalized nutrition research.
3. The Nutrition–Muscle Connection: What the Science Shows
Muscle tissue is in a constant state of turnover — being broken down and rebuilt continuously. Whether you gain, maintain, or lose muscle over time depends on the net balance between muscle protein synthesis (MPS) and muscle protein breakdown (MPB).
Nutrition influences this balance in three major ways:
Providing the raw materials (amino acids) needed to build new muscle protein
Supplying the energy needed to fuel the synthesis process and daily activity
Modulating the inflammatory and oxidative environment in which muscle tissue lives
Recent nutrition-science frameworks distinguish between three complementary approaches to muscle-protective eating: a single-nutrient approach (e.g., focusing on protein or vitamin D alone), a whole-food approach (e.g., emphasizing specific protein-rich or anti-inflammatory foods), and a whole-diet approach (e.g., Mediterranean-style eating patterns). The strongest current evidence suggests these approaches are not mutually exclusive — comprehensive dietary patterns tend to outperform single-nutrient interventions, but individual nutrients like protein remain a critical, non-negotiable foundation within any pattern.
4. Protein: Quantity, Quality, and Timing
How Much Protein Do You Actually Need?
The standard RDA of 0.8 g/kg/day was designed to prevent deficiency in young adults — not to preserve muscle in aging populations. Most current geriatric nutrition guidance recommends:
1.0–1.2 g/kg/day for healthy older adults
1.2–1.5 g/kg/day for older adults with acute or chronic illness
Up to 2.0 g/kg/day for those with severe malnutrition or active sarcopenia, under medical supervision
Protein Quality Matters as Much as Quantity
Not all protein is equal when it comes to stimulating muscle protein synthesis. Protein quality is largely determined by:
Essential amino acid (EAA) content, particularly leucine, which acts as a metabolic trigger for MPS
Digestibility and absorption rate
Amino acid completeness relative to human requirements
High-quality, complete protein sources — dairy, eggs, fish, poultry, and meat — tend to outperform many plant proteins on a per-gram basis for muscle protein synthesis, largely due to leucine content and digestibility. However, well-combined plant proteins (e.g., legumes plus grains) or supplemented plant diets can close much of this gap, which is encouraging news for vegetarians and vegans concerned about sarcopenia risk.
Protein Timing and Distribution
Emerging evidence favors distributing protein evenly across meals rather than concentrating it at dinner (the typical Western eating pattern). A practical target is 25–35 grams of high-quality protein per meal, three to four times daily, each containing roughly 2.5–3 grams of leucine — enough to meaningfully stimulate MPS in older, anabolic-resistant muscle.
5. Beyond Protein: Micronutrients and Bioactive Compounds
Protein isn't the whole story. Several other nutritional factors have accumulating support:
Vitamin D — low status is consistently associated with reduced muscle strength and higher fall risk; supplementation is often recommended for those who are deficient.
Omega-3 fatty acids — may help offset anabolic resistance and reduce inflammatory signaling that interferes with muscle maintenance.
Polyphenols (found in berries, green tea, olive oil, and other plant foods) — increasingly studied for their potential to influence muscle-related gene expression and reduce oxidative damage through epigenetic and anti-inflammatory mechanisms.
Creatine — one of the more well-established supplements for supporting muscle mass and strength, particularly when combined with resistance training.
B vitamins and antioxidant micronutrients (vitamin E, selenium, zinc) — support the broader metabolic and mitochondrial environment muscle depends on.
6. Diet Patterns: Single Nutrient vs. Whole Food vs. Whole Diet Approaches
Rather than chasing one "magic nutrient," current research supports layering interventions:
Here is the breakdown of the dietary approaches and their corresponding strength of evidence, rewritten as clear, actionable points:
Single-Nutrient Approach (Protein or Vitamin D Supplementation Alone)
Example: Taking isolated protein powders or Vitamin D capsules without altering other dietary habits.
Strength of Evidence: Strong for targeted protein supplementation to stimulate muscle synthesis; Moderate for Vitamin D, showing clear benefits primarily in clinically deficient individuals.
Whole-Food Approach (Food Group Optimization)
Example: Actively prioritizing whole, nutrient-dense foods such as dairy, eggs, fatty fish, legumes, and vibrant, colorful produce.
Strength of Evidence: Moderate to Strong, and Growing, as this method provides natural matrices of co-factors, healthy fats, and minerals that isolated supplements lack.
Whole-Diet Pattern Approach (Comprehensive Lifestyle Synergy)
Example: Adopting a structured Mediterranean-style eating pattern characterized by high protein intake and rich levels of plant-based polyphenols.
Strength of Evidence: Strong and Accumulating, yielding the absolute highest clinical efficacy for preventing muscle decline, especially when seamlessly paired with a regular resistance exercise program.
Diets high in ultra-processed foods and saturated fat — a pattern often described as a "Western" or high-fat diet — have been associated in recent research with accelerated markers of age-related muscle decline, likely mediated through increased oxidative stress and systemic inflammation. This reinforces that what you avoid matters nearly as much as what you add.
7. Inflammation, Oxidative Stress, and Diet
Chronic inflammation is one of the central mechanistic links between poor diet and sarcopenia. Diets high in refined carbohydrates, industrial seed oils, and saturated fat tend to promote a pro-inflammatory internal environment, while diets rich in polyphenols, omega-3s, fiber, and antioxidant micronutrients tend to counter it.
Clinically, this matters because inflammation doesn't just correlate with muscle loss — it appears to actively interfere with the molecular signaling pathways (such as the mTOR pathway) responsible for building new muscle tissue. This is one reason why simply "eating enough protein" isn't always sufficient in someone with an inflammatory diet pattern working against them.
8. Practical Application: Building a Sarcopenia-Protective Diet
Here is a practical framework you can start applying today:
Daily Protein Checklist
[ ] Hit your target g/kg/day (1.0–1.5 g/kg for most older adults)
[ ] Distribute protein across 3–4 meals (25–35g each)
[ ] Include at least one leucine-rich source per meal (dairy, eggs, meat, fish, soy)
Weekly Food Targets
[ ] 2–3 servings of fatty fish (omega-3s)
[ ] Daily servings of legumes, nuts, or seeds
[ ] 5+ servings of colorful fruits and vegetables daily (polyphenols, antioxidants)
[ ] Limit ultra-processed, high-saturated-fat foods
Sample One-Day Meal Framework
Here is the sample one-day meal framework rewritten as clear, actionable points:
Breakfast
Example: Greek yogurt topped with fresh berries and walnuts.
Protein Content: 25–30g
Lunch
Example: Grilled salmon served alongside quinoa and a bed of leafy greens.
Protein Content: 30g
Snack
Example: A serving of cottage cheese or a bowl of steamed edamame.
Protein Content: 15–20g
Dinner
Example: A hearty chicken breast or thick lentil stew packed with assorted vegetables.
Protein Content: 30–35g
9. Exercise and Nutrition Together: Why You Need Both
Nutrition alone has meaningful but limited effects on muscle preservation. Resistance training is the strongest known stimulus for muscle protein synthesis, and its combination with adequate protein intake produces substantially better outcomes than either intervention alone. Recent umbrella reviews on fall prevention in older adults consistently find that combined exercise-and-nutrition interventions outperform single-domain approaches for reducing sarcopenia-related fall risk. If you take one action step from this entire article, let it be this: pair your dietary changes with at least two sessions of resistance exercise per week.
10. Evidence Summary Table
Whole-Diet Synergy Outperforms Isolated Elements
Focus & Design: Nutrition in sarcopenia prevention/treatment (Literature Review).
Key Finding: Comprehensive dietary strategies that look at whole-food patterns yield far superior clinical outcomes for aging muscle compared to isolated, single-nutrient supplementation (Granic et al., 2025).
Combined Interventions Deliver Exponential Protection
Focus & Design: Exercise and nutritional strategies for fall prevention (Umbrella Review).
Key Finding: Dual-domain approaches—simultaneously pairing physical training with targeted nutritional adjustments—reduce sarcopenia-related fall risks exponentially more than deploying either intervention on its own (Dharmansyah et al., 2026).
Leucine Architecture Dictates the Anabolic Response
Focus & Design: Protein quality and amino acid composition (Literature Review).
Key Finding: An aging body’s capacity to initiate Muscle Protein Synthesis (MPS) is fundamentally driven by a protein source's total leucine content and its overall amino acid completeness (Calderón et al., 2026).
Genetics and Inflammation Modulate Dietary Success
Focus & Design: Dietary protein intake, inflammatory biomarkers, and sarcopenia incidence (Prospective Cohort Study).
Key Finding: An individual's underlying genetic susceptibility actively intersects with their baseline systemic inflammation and daily protein volume to dictate real-world muscle-loss trajectories (Xia et al., 2026).
Nutrition Competes Directly with Emerging Therapeutics
Focus & Design: Nutritional vs. pharmacological treatments for muscle loss (Systematic Review + Network Meta-Analysis).
Key Finding: High-quality, structured nutritional interventions display robust, clinically meaningful efficacy that holds its own when measured comparatively against emerging medical and pharmacological therapies (Zhang et al., 2025).
Poor-Quality Fats Actively Degrade Muscle Integrity
Focus & Design: High-fat diets and accelerated muscle aging (Mechanistic Study).
Key Finding: Eating habits saturated with ultra-processed foods and poor-quality fats create a cascade of cellular oxidative stress and chronic inflammation, actively accelerating the onset and severity of sarcopenia (Cimmino et al., 2026).
The Protein-Polyphenol Matrix Works at the Cellular Level
Focus & Design: Dual protein and polyphenol clinical interventions (Mechanistic Review).
Key Finding: Intentionally pairing premium protein sources with antioxidant-rich plant polyphenols offers a promising, multi-layered defense system that protects delicate muscle signaling pathways at a deep molecular level (Aragón-Espinosa et al., 2026).
Protein Adequacy Remains the Non-Negotiable Baseline
Focus & Design: Macro-nutritional treatment overview (Clinical Review).
Key Finding: While micro-nutrients and lifestyle patterns dictate outcomes, securing a baseline of highly bioavailable, adequate daily protein remains the absolute foundational pillar of any successful anti-sarcopenia protocol (Barone et al., 2025).
Plant Compounds Influence Muscle via Epigenetic Modulation
Focus & Design: Dietary polyphenols and muscle health (Literature Review).
Key Finding: Beyond standard cellular protection, plant-based polyphenols are increasingly shown to positively influence aging muscle health by directly interacting with critical epigenetic mechanisms and gene expressions (Da Silva Rodrigues et al., 2026).
Methodology Note: Because these clinical study designs span a wide spectrum of scientific strength—ranging from exploratory cellular mechanisms to massive population cohorts and rigorous systematic reviews—this data should be viewed as a converging, highly complementary body of evidence rather than standalone, isolated proof.
11. Common Myths and Mistakes
Myth: "Muscle loss is just an inevitable part of aging — nothing to be done." False. While some decline is normal, the rate and severity of that decline is highly modifiable through diet and exercise.
Myth: "More protein is always better." Not necessarily — excessive protein without adequate energy, hydration, or kidney function monitoring (especially in those with pre-existing kidney disease) isn't automatically beneficial and should be personalized.
Myth: "Plant-based diets can't support muscle health in older age." Overstated. With attention to protein quantity, variety, and leucine content, plant-forward diets can support muscle health — though they typically require more intentional planning than omnivorous diets.
Mistake: Concentrating all protein at dinner. This is the most common pattern in Western diets and works against the "spread it out" principle anabolic-resistant muscle needs.
Mistake: Focusing only on protein and ignoring inflammation. A high-protein diet loaded with ultra-processed foods and saturated fat may partially undercut its own benefits.
12. Frequently Asked Questions
What is the best diet for preventing sarcopenia? No single "best" diet exists, but Mediterranean-style eating patterns combined with adequate, evenly distributed protein intake (1.0–1.5 g/kg/day) and regular resistance exercise show the strongest combined evidence.
How much protein do I need per day to prevent muscle loss? Most older adults benefit from 1.0–1.2 g/kg/day, rising to 1.2–1.5 g/kg/day if managing illness or active muscle loss — always personalized with a healthcare provider.
Can sarcopenia be reversed? Early-stage sarcopenia can often be significantly improved, and in some cases substantially reversed, through combined nutrition and resistance training interventions. Advanced sarcopenia is harder to fully reverse but can still be slowed.
Is whey protein better than plant protein for muscle aging? Whey has a favorable leucine content and rapid digestibility, giving it a practical edge for stimulating muscle protein synthesis. Well-planned plant protein combinations can still be effective, just often requiring larger portions or supplementation.
Does vitamin D help with sarcopenia? In people who are vitamin D deficient, correcting that deficiency is associated with improved muscle strength and reduced fall risk. Supplementing beyond sufficiency shows less clear additional benefit.
What foods should I avoid to protect my muscles as I age? Ultra-processed foods, excess saturated fat, and diets consistently high in refined carbohydrates are associated with increased inflammation and oxidative stress that may accelerate muscle decline.
At what age should I start worrying about sarcopenia? Muscle mass peaks around the 30s and begins a slow decline afterward. Proactive nutrition and strength-training habits are most effective when started in your 40s and 50s, before significant decline occurs — though it's never too late to benefit.
Can supplements alone prevent sarcopenia? Supplements (protein powder, creatine, vitamin D, omega-3s) can support muscle health but are most effective as an addition to — not a replacement for — a well-rounded diet and resistance exercise.
How is sarcopenia diagnosed? Diagnosis typically involves assessing muscle strength (e.g., grip strength), muscle mass (via imaging or bioelectrical impedance), and physical performance (e.g., gait speed), following criteria set by clinical working groups.
Does inflammation really affect muscle mass? Yes. Chronic low-grade inflammation interferes with the cellular signaling pathways responsible for building and maintaining muscle tissue, independent of protein intake.
13. Conclusion and Action Steps
Sarcopenia is not a life sentence handed down by aging alone — it's a modifiable condition with nutrition sitting at the center of the solution. The clinical importance here can't be overstated: the difference between an inflammatory, low-protein diet and a protein-adequate, polyphenol-rich, anti-inflammatory eating pattern can meaningfully shape whether you maintain independence, mobility, and strength in your later decades.
Your next three steps:
Calculate your target protein intake (1.0–1.5 g/kg/day) and distribute it across your meals.
Add two resistance-training sessions to your week — nutrition and exercise work best together.
Talk to your doctor about screening for sarcopenia risk factors, especially if you're over 50 or have noticed declining strength.
This article is for educational purposes and is not a substitute for personalized medical advice. Please consult your physician or a registered dietitian before making significant dietary or supplement changes.
Related Articles
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
Sarcopenia in Diabetes: Managing Muscle Loss with Chronic Disease | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
Best Exercises for Sarcopenia: Strength Training Guide for Older Adults | DR T S DIDWAL
Best Supplements for Sarcopenia: Vitamin D, Creatine, and HMB Explained | DR T S DIDWAL
14. Sources and References
Aragón-Espinosa, P., Pérez-Matute, P., Bompart, C., & et al. (2026). From molecular mechanisms to nutritional applications: Protein and polyphenol interventions in sarcopenia. Journal of Physiology and Biochemistry, 82(1), 12. https://doi.org/10.1007/s13105-026-01154-6
Barone, M., Baccaro, P., & Molfino, A. (2025). An overview of sarcopenia: Focusing on nutritional treatment approaches. Nutrients, 17(7), 1237. https://doi.org/10.3390/nu17071237
Calderón, P., Jima Gavilanes, D., Vivanco-Zárate, A. S., & Sarango-González, K. P. (2026). The role of protein quality and amino acid composition in preventing sarcopenia and functional decline in older adults. Frontiers in Nutrition, 13, Article 1817891. https://doi.org/10.3389/fnut.2026.1817891
Cimmino, F., Petrella, L., Cavaliere, G., & et al. (2026). High-fat diet anticipates age-related sarcopenia through increased oxidative stress and inflammation. British Journal of Biomedical Science, 83, Article 15743. https://doi.org/10.3389/bjbs.2026.15743
Da Silva Rodrigues, G., Lopes da Silva, L. S., Crystine da Silva Sobrinho, A., & et al. (2026). Dietary polyphenols and sarcopenia: Epigenetic mechanisms and geroscience perspectives for muscle health in aging. Frontiers in Aging, 6, Article 1696473. https://doi.org/10.3389/fragi.2025.1696473
Dharmansyah, D., Rahayuwati, L., Pramukti, I., & Mutyara, K. (2026). Exercise and nutritional interventions for sarcopenia-related fall prevention in older adults: An umbrella review. The Journal of Nutrition, Health & Aging, Article 100862. https://doi.org/10.1016/j.jnha.2026.100862
Granic, A., Sayer, A. A., Cooper, R., & Robinson, M. (2025). Nutrition in the prevention and treatment of skeletal muscle ageing and sarcopenia: A single nutrient, a whole food and a whole diet approach. Proceedings of the Nutrition Society, 84(4), 340–355. https://doi.org/10.1017/S0029665124007432
Xia, H., Xiang, R., Song, X., & et al. (2026). Dietary protein intake, inflammatory biomarkers, genetic susceptibility, and the incidence of sarcopenia: A prospective population-based study. Frontiers in Nutrition, 13, Article 1821758. https://doi.org/10.3389/fnut.2026.1821758
Zhang, M., Shen, Y., Gao, Y., Jiang, X., Yue, J., & Hao, Q. (2025). Nutritional and pharmacological interventions for sarcopenia in older adults: A systematic review and network meta-analysis. Journal of the American Medical Directors Association. Advance online publication. https://doi.org/10.1016/j.jamda.2025.106038