High BCAA Levels Could Signal Dangerous Visceral Fat—Here's What New Research Shows
Discover why scientists are studying branched-chain amino acids as emerging biomarkers for visceral fat, obesity, and cardiometabolic risk.
OBESITYMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/28/202621 min read
What do BCAA levels reveal about visceral fat?
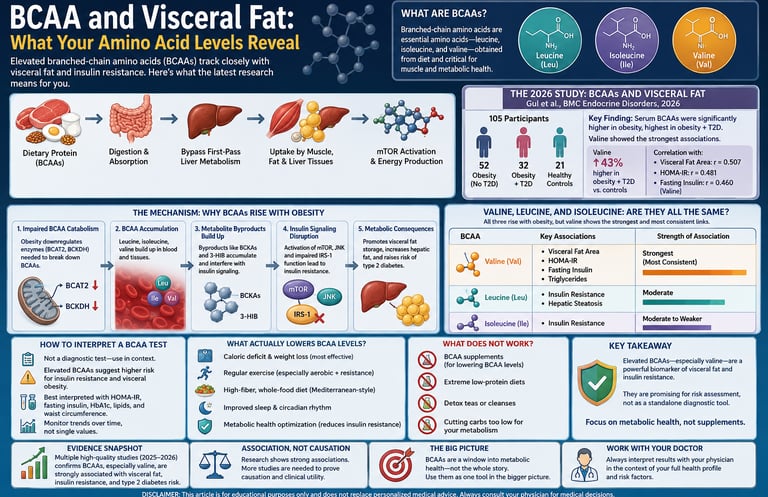
Elevated branched-chain amino acids, especially valine, are strongly linked to visceral fat and insulin resistance. A 2026 clinical study found valine was 20% higher in people with obesity and 43% higher in those with obesity plus type 2 diabetes compared to healthy controls. The rise reflects impaired BCAA breakdown in fat tissue, not high protein intake.
Keypoints: BCAA and Visceral Fat
- Valine is the standout marker, not just “BCAAs” as a group.
Of leucine, isoleucine, and valine, valine showed the strongest independent links to waist circumference and HOMA-IR in 2026 clinical data. If you only track one BCAA for metabolic risk, make it valine.
- Elevated BCAAs signal impaired breakdown, not excess protein intake.
Twin and dietary intake studies show circulating BCAA levels and protein consumption are largely decoupled. The rise comes from slowed catabolism in fat and muscle tissue, which leads to buildup of BCAAs and toxic intermediates like BCKAs and 3-HIB.
- The BCAA-insulin resistance link is a self-reinforcing loop.
Impaired BCAA breakdown raises blood BCAAs. Those BCAAs and their byproducts chronically activate mTORC1 and JNK pathways, which interfere with insulin signaling. Insulin resistance then further impairs BCAA breakdown.
- Obesity plus type 2 diabetes amplifies the signal.
In the 2026 Gul et al. study, valine averaged 30.48 µg/mL in healthy controls, 36.48 µg/mL in obesity without diabetes, and 43.46 µg/mL in obesity with diabetes. That 43% jump from healthy to T2DM suggests valine tracks metabolic severity, not just body size.
- Sex and fat distribution change the picture.
2025 data from Lausanne found BMI correlated most with BCAAs in men, while waist circumference correlated most in women. Central fat distribution matters more than total mass for BCAA elevation, especially for women.
- BCAA testing is promising but not diagnostic.
No major medical body endorses BCAAs as a standalone screen for insulin resistance or diabetes. It adds context alongside HOMA-IR, fasting insulin, HbA1c, and waist circumference. Treat it as a research-stage biomarker, not a verdict.
- Don't cut protein to “fix” BCAA levels.
Circulating BCAA elevation is driven by metabolism, not diet. Restricting healthy protein risks muscle loss without addressing visceral fat or insulin resistance. Whole-diet patterns, sustained fat loss, and exercise move the needle. Supplements may worsen insulin resistance in a high-fat context per animal models.
- Weight loss helps, but BCAAs are a lagging indicator.
One trial saw major HOMA-IR improvement after 6 weeks of very-low-calorie dieting with no significant BCAA drop. Expect BCAA normalization to trail behind insulin sensitivity gains. Track trends over months, not weeks.
Branched-chain amino acids (BCAAs) — leucine, isoleucine, and valine — are reliably elevated in people with visceral obesity, and among the three, valine appears to track most closely with central fat and insulin resistance. That's not a guess. It's the headline finding of a 2026 clinical study published in BMC Endocrine Disorders, and it lines up with a decade of metabolomics research before it.
This matters because visceral fat — the fat packed around your organs, not the fat you can pinch — is the kind most strongly linked to type 2 diabetes, fatty liver disease, and cardiovascular risk. A simple blood test that helps flag who's accumulating it before the damage shows up elsewhere would be genuinely useful. BCAA testing is starting to look like one candidate for that role.
1. What Are BCAAs, Exactly?
Branched-chain amino acids are three of the nine essential amino acids your body can't make on its own — leucine, isoleucine, and valine. You get them entirely from food: meat, dairy, eggs, legumes, and to a lesser extent, grains.
They're called "branched-chain" because of their molecular shape — a side chain that branches off rather than running in a straight line. That's just chemistry trivia, though. What matters clinically is what they do:
They make up roughly 20% of the protein in your diet and a similar share of muscle tissue.
Unlike most amino acids, which get processed in the liver first, BCAAs go straight to muscle, fat, and other peripheral tissues for metabolism.
Leucine in particular acts as a direct signal to a cellular growth pathway called mTOR (mammalian target of rapamycin) — this is the same mechanism that makes leucine valuable for muscle protein synthesis after a workout.
That last point — bypassing the liver — is part of why BCAA levels in the blood respond so directly to what's happening in muscle and fat tissue. They're a closer mirror of peripheral metabolic health than most lab values.
For decades, BCAAs were mostly known as a sports nutrition supplement, marketed for muscle recovery. The metabolic research community has been telling a very different, less marketable story for about 15 years: higher circulating BCAAs are one of the most consistent biomarkers of obesity, insulin resistance, and type 2 diabetes risk in the literature.
This isn't a contradiction — it's two different contexts. Short-term BCAA supplementation around exercise is a different physiological scenario than chronically elevated baseline BCAA levels from impaired metabolism. We'll separate these clearly throughout this article, because conflating them is where a lot of online confusion comes from.
2. The Core Finding: BCAAs and Visceral Fat
The 2026 Study That Anchors This Article
A study published in BMC Endocrine Disorders in June 2026 by Gul, Ullah, Li, and colleagues at Northern Jiangsu People's Hospital in China gives us the most directly relevant clinical data on this topic. Here's what they actually did and found — no rounding up, no inflation.
Study design: 105 participants split into three groups:
52 people with obesity, no type 2 diabetes
32 people with obesity and type 2 diabetes
21 healthy, normal-weight controls
Everyone underwent anthropometric measurements (waist circumference, visceral fat area), blood work (HOMA-IR, fasting insulin, HbA1c, lipids), and serum amino acid profiling.
What they found:
Serum BCAA levels were significantly higher in both groups with obesity compared to the healthy, normal-weight control group. Among the three BCAAs, valine showed the greatest increase: average concentrations were 36.48 µg/mL in the obesity-without-diabetes group, climbing to 43.46 µg/mL in the obesity-with-diabetes group, compared to just 30.48 µg/mL in healthy controls.
That's roughly a 20% increase in valine for obesity alone, and a 43% increase when type 2 diabetes is layered on top. The progression itself is clinically informative — it suggests valine doesn't just mark obesity, it tracks with how metabolically unwell that obesity has become.
On the correlation side: BCAAs were positively associated with visceral fat area, BMI, waist circumference, body fat ratio, and markers of insulin resistance including HOMA-IR, fasting insulin, and HbA1c — all statistically significant.
Valine stood out specifically. It demonstrated the strongest correlations with HOMA-IR (r = 0.481) and waist circumference (r = 0.507), both highly significant. When the researchers ran multivariable models — meaning they controlled for other confounding factors — valine remained independently and positively associated with central adiposity as measured by waist circumference, and with insulin resistance as measured by HOMA-IR. Leucine and isoleucine were also independently associated with waist circumference and fasting insulin, though less strongly than valine. Notably, two other amino acids studied — phenylalanine and tyrosine — showed no independent associations once the models adjusted for confounders.
Why that last detail matters clinically: it tells us this isn't just "all amino acids go up with obesity." The BCAA signal — and valine specifically — is doing something distinct from general amino acid elevation. That specificity is what makes it potentially useful as a targeted biomarker rather than a generic marker of "metabolic stress."
How This Fits the Broader Literature
This 2026 finding isn't an outlier — it's a confirmation, with finer detail, of a pattern researchers have been documenting since at least 2009.
A 2025 cross-sectional study from Lausanne, Switzerland (Liu et al., published in Nutrition, Metabolism and Cardiovascular Diseases) looked at this from a slightly different angle, asking which anthropometric measure tracks BCAAs most closely — and found an interesting sex difference. BMI showed the strongest positive association with BCAA levels in men, while waist circumference showed the strongest positive association with BCAA levels in women.
That sex-specific pattern is a detail worth sitting with: it suggests fat distribution, not just fat amount, interacts with BCAA metabolism differently depending on biological sex — which has real implications for how this biomarker might eventually be used in clinical risk stratification.
A 2026 review in the International Journal of Obesity (Wang, Wang, and Yang) ties the mechanistic threads together at a higher level. The review frames BCAA metabolic disorders as a core feature of obesity and its associated metabolic syndrome, while noting that the specific mechanisms and clinical significance remain genuinely debated in the field — an important caveat we'll come back to. The review specifically highlights branched-chain α-keto acids (BCKAs) and a related metabolite called 3-hydroxyisobutyric acid (3-HIB) as key intermediates that disrupt insulin signaling, lipid balance, and drive chronic inflammation in the progression of obesity-related disease.
Other recent research — including bidirectional Mendelian randomization studies looking at causal relationships between BCAA levels and conditions like nonalcoholic fatty liver disease, and population studies like the FiLWHEL cohort examining circulating BCAAs and obesity risk in Filipino women in Korea — is actively expanding this picture for 2026. We're watching this literature closely; as those specific findings become more fully accessible, this section will be the first to get updated.
3. The Mechanism: Why BCAAs Rise With Obesity
Here's the part most articles skip, and it's the part that actually explains why the clinical numbers above look the way they do.
It's Not Just "Eating More Protein"
The first instinct is to assume people with obesity simply eat more protein, so their BCAA levels go up. The research doesn't support this as the primary driver. A 2016 twin study examining BCAA intake versus circulating BCAA levels found these two things were essentially unrelated to each other once genetics were accounted for — dietary intake explained very little of the variation in blood levels. Something else is going on, and it's metabolic, not just nutritional.
The Real Driver: Impaired BCAA Breakdown
The leading explanation is that obesity disrupts the body's ability to break down BCAAs, not just how much it takes in. Here's the chain of events research has mapped out:
Catabolism slows down. In obese and insulin-resistant tissue — particularly adipose (fat) tissue — the enzymes responsible for breaking down BCAAs become less active. BCAAs build up in the blood not because more is coming in, but because less is being cleared out.
Toxic intermediates accumulate. When BCAA breakdown stalls partway through, it generates byproducts called branched-chain α-keto acids (BCKAs) and related metabolites like 3-hydroxyisobutyric acid (3-HIB). These aren't inert — they actively interfere with normal insulin signaling.
mTOR gets persistently activated. Leucine, in particular, is a direct activator of the mTORC1 pathway. In short bursts (like after a workout), that's beneficial — it drives muscle repair. But chronic, persistent activation from sustained high BCAA levels has the opposite effect: it triggers a cascade (involving the IRS-1 and JNK pathways) that interferes with how cells respond to insulin.
Insulin resistance compounds the problem. Once insulin resistance sets in, it further impairs BCAA catabolism, especially in adipose tissue — creating a self-reinforcing loop where elevated BCAAs contribute to insulin resistance, and insulin resistance keeps BCAAs elevated.
This loop is exactly why valine showed up so strongly correlated with HOMA-IR in the Gul et al. data above — the biomarker and the underlying dysfunction are mechanistically intertwined, not coincidentally associated.
A Landmark Study You Should Know About
This entire research direction traces back to a pivotal 2009 study by Newgard and colleagues in Cell Metabolism. They fed rats a high-fat diet with added BCAA supplementation and found something counter to what you'd expect: despite reduced food intake and equivalent weight gain to a high-fat-only group, the BCAA-supplemented rats were just as insulin resistant — driven by chronic activation of mTOR, JNK, and a related insulin-signaling protein, plus a buildup of fatty acid byproducts called acylcarnitines in muscle tissue.
That finding has been replicated and extended in dozens of studies since, including more recent work showing BCAA supplementation can also trigger pro-inflammatory immune cell activity in fat tissue through a separate signaling pathway (IFNGR1/JAK1/STAT1).
Gut Microbiota's Emerging Role
One more piece worth knowing: there's growing evidence that gut bacteria composition influences how much BCAA your body absorbs and how it's processed downstream. Imbalances in gut microbial populations have been linked to altered BCAA uptake, which then indirectly affects insulin signaling. This is a newer thread in the research (most actively explored from 2023 onward) and isn't fully mapped out yet, but it may eventually explain some of the individual variation in BCAA levels that body composition alone doesn't account for.
4. Valine, Leucine, and Isoleucine: Are They All the Same?
No — and this is one of the more clinically useful nuances in the recent research. Lumping all three BCAAs into a single number loses real information.
Valine: The Standout Signal
Across the 2026 Gul et al. data, valine consistently outperformed the other two BCAAs as a marker of metabolic dysfunction — strongest correlation with HOMA-IR, strongest correlation with waist circumference, and the only BCAA that remained robustly significant in fully adjusted models for both central adiposity and insulin resistance.
Leucine and Isoleucine: Real, But Secondary Signals
Leucine and isoleucine were still independently associated with waist circumference and fasting insulin in the same study — they're not irrelevant. They're just less specific than valine. Leucine's outsized role in mTOR activation makes it mechanistically central to the insulin resistance side of the story, even if it's not the strongest statistical marker of fat distribution specifically.
Why This Matters If You Ever See a Lab Report
If you have access to individual BCAA values (rather than just a "total BCAA" number), valine deserves the closest attention as a marker of central adiposity and insulin resistance risk — based on current evidence. A single elevated valine reading isn't a diagnosis of anything on its own, but in combination with other risk markers, it adds meaningful information.
5. How to Interpret a BCAA Test — Clinically
This is the section we want to get right, because it's where most consumer health content either oversimplifies or overpromises.
What "Elevated" Actually Means in Reference Ranges
Typical adult reference ranges for plasma BCAAs are roughly:
Amino Acid Normal Adult Range Isoleucine 42–100 µmol/L Leucine 66–170 µmol/L Valine 150–310 µmol/L
These ranges vary somewhat by lab and assay method (NMR spectroscopy vs. LC-MS/MS vs. GC-MS all calibrate slightly differently), which is the first thing to flag with your physician if you're comparing results across different tests or time points.
What a Result Above Range Does — and Doesn't — Tell You
What it can reasonably suggest, in context:
A pattern consistent with insulin resistance, particularly if paired with elevated fasting insulin or HOMA-IR
A signal worth investigating further if you have other metabolic risk factors (elevated waist circumference, family history of type 2 diabetes, fatty liver markers)
In research settings, BCAA panels have shown moderate diagnostic value for distinguishing children with obesity from healthy-weight peers, with combined BCAA levels reaching an AUC of 0.78 in one pediatric study — "moderate," not "definitive."
What it does not tell you on its own:
It is not a stand-alone diagnostic test for diabetes, obesity, or any specific disease. No major medical body currently recommends BCAA testing as a primary screening tool.
It cannot tell you why your levels are elevated — genetics, gut microbiome composition, degree of insulin resistance, and visceral fat mass all contribute, and current testing can't cleanly separate these.
A single measurement is a snapshot, not a trend. The clinically interesting signal is often the trajectory over time, paired with other markers.
The Honest Limitation Nobody Markets
Here's the caveat the Wang et al. 2026 review itself raises, and it's important: the specific mechanisms and clinical significance of BCAA metabolism in obesity remain genuinely debated, even among researchers actively publishing in this space. The Gul et al. authors are explicit about this too — their own conclusion states that BCAA profiling "may help identify individuals with increased metabolic risk," but that "further prospective studies are required to validate its clinical and predictive value."
In plain terms: this is a promising, active area of research — not a settled clinical tool. If a BCAA panel comes back elevated, the right next step is a conversation with your doctor about your overall metabolic picture, not a panic response to one number.
A Quick Self-Check Framework
If you're trying to make sense of a result, ask these questions (ideally with your physician):
Is this paired with other insulin resistance markers (fasting insulin, HOMA-IR, HbA1c)?
Is my waist circumference elevated relative to standard cutoffs for my sex and ethnicity?
Do I have a family history of type 2 diabetes or fatty liver disease?
Was this measured via a validated method (NMR or LC-MS/MS). consistently across time points if I'm tracking change?
Is valine specifically elevated, or just total BCAA, and by how much relative to my lab's reference range?
6. Evidence Summary Table
Gul, Ullah, Li et al. (2026) — BMC Endocrine Disorders
Study Design: Cross-sectional clinical study.
Population: $n=105$ participants in China (comparing individuals with obesity $\pm$ Type 2 Diabetes to healthy controls).
Key Findings:
Valine showed the strongest correlation with metabolic markers among all amino acids tested.
It was independently associated with increased waist circumference ($\beta=0.357$) and insulin resistance via HOMA-IR ($\beta=0.306$).
Liu, Borreggine, Gallart-Ayala et al. (2025) — Nutrition, Metabolism & Cardiovascular Diseases
Study Design: Cross-sectional cohort study using data from the CoLaus|PsyCoLaus and OsteoLaus cohorts.
Population: Adults living in Lausanne, Switzerland.
Key Findings: Revealed distinct sex-specific differences in how BCAA levels correlate with body composition:
In men, BCAA levels associate most strongly with overall body mass index (BMI).
In women, BCAA levels associate most strongly with central adiposity (waist circumference).
Wang, Wang & Yang (2026) — International Journal of Obesity
Study Design: Narrative review of mechanistic literature.
Population: N/A.
Key Findings:
Identified downstream branched-chain ketoacids (BCKAs) and 3-hydroxyisobutyrate (3-HIB) as the critical molecular mediators that disrupt insulin signaling.
Notes that the exact precise pathways and causal mechanisms remain actively debated.
Newgard et al. (2009) — Cell Metabolism
Study Design: Combined animal model and human metabolomics study.
Population: Rats fed a High-Fat Diet (HFD) $\pm$ BCAA supplementation, alongside a comparative cohort of obese vs. lean humans.
Key Findings:
A seminal foundational paper establishing a specific BCAA-related metabolic signature that clearly distinguishes obese from lean individuals.
Demonstrated that BCAA accumulation drives insulin resistance by overactivating the mTOR/JNK signaling pathways.
Mansoori et al. (2025) — Obesity Reviews
Study Design: Narrative review.
Population: N/A.
Key Findings:
Provides a comprehensive, up-to-date synthesis of BCAA pathophysiology.
Maps how BCAA dysregulation spans across multiple aspects of metabolic syndrome, specifically focusing on non-alcoholic fatty liver disease (NAFLD) and Type 2 Diabetes
7. Practical Steps: What Actually Moves the Needle
This is where we have to be careful and honest. The strongest available evidence supports addressing the underlying drivers of elevated BCAAs — visceral fat and insulin resistance — rather than trying to manipulate BCAA levels directly through diet or supplements.
What the Evidence Supports
1. Reducing visceral fat through sustained weight loss. This is the most evidence-backed lever, though it comes with a caveat worth knowing: in one trial of overweight men following a 6-week very-low-calorie diet, significant weight loss and a major improvement in HOMA-IR did not produce a measurable drop in BCAA levels over that short window. This suggests BCAA normalization may lag behind other metabolic improvements, or may require more sustained fat loss (particularly visceral fat) than a 6-week intervention can achieve. Don't expect BCAA levels to be a fast-feedback metric for weight loss progress.
2. Resistance and aerobic exercise. Exercise interventions — independent of major weight change — have been linked to improvements in metabolic markers associated with the BCAA-insulin resistance pathway. A study following central obesity and NAFLD patients through a 12-month exercise program tracked changes in BCAA levels alongside liver fat improvements, reinforcing exercise as a meaningful lever even when weight loss alone is incomplete.
3. Addressing insulin resistance directly. Since the relationship between BCAAs and insulin resistance appears bidirectional (each feeds the other), interventions that directly target insulin sensitivity — sustainable calorie deficit, strength training, adequate sleep, stress management — indirectly address the BCAA side of the equation too.
4. Whole-dietary-pattern approaches over single-nutrient tweaks. Some research (e.g., on dietary BCAA intake, as opposed to circulating levels) has actually found higher dietary BCAA intake associated with lower insulin resistance and adiposity markers in certain populations — the opposite direction of the circulating level findings. This is a genuinely confusing point for readers, so let's be direct about it:
Dietary BCAA intake and circulating BCAA levels are not the same thing, and they don't move in the same direction. The clinical research connecting BCAAs to obesity risk is almost entirely about circulating (blood) levels, which are driven mainly by metabolism, not intake. Cutting dietary protein or BCAA-rich foods specifically is not supported by this research as a way to lower blood BCAA levels or improve metabolic risk.
What the Evidence Does Not Support
Restricting dietary protein or BCAA-rich foods (meat, dairy, eggs) to "lower your BCAA levels." As above, intake and circulating levels are largely decoupled. Restricting healthy protein sources to chase a lab number isn't supported by current evidence and could compromise muscle mass, especially during a weight-loss phase when preserving lean mass matters most.
Taking BCAA supplements to "improve" levels related to obesity risk. This conflates two very different contexts. Short-term BCAA supplementation around training has a separate evidence base related to muscle recovery — it has nothing to do with the chronic elevation patterns discussed in this article, and animal research (the Newgard 2009 study, for instance) actually showed added BCAA supplementation worsened insulin resistance independent of weight gain in a high-fat-diet context.
Treating a single BCAA test result as a diagnosis. As covered in Section 5, this is a research-stage biomarker, not a validated stand-alone diagnostic.
A Reasonable Action Checklist
[ ] Discuss any BCAA or amino acid panel results with your physician in the context of your full metabolic profile (HOMA-IR, lipids, waist circumference, HbA1c)
[ ] Focus on sustainable fat loss strategies if visceral fat is a concern, rather than chasing a specific lab marker
[ ] Incorporate both resistance and aerobic exercise — both have separate, evidence-backed mechanisms relevant here
[ ] Don't restrict dietary protein based on BCAA-related health content you've read online without medical guidance
[ ] If considering BCAA supplements for athletic performance, treat that as a separate decision from any metabolic health concern — talk to a doctor or registered dietitian if you have insulin resistance or are at risk for type 2 diabetes
[ ] Re-test relevant markers over a meaningful timeframe (months, not weeks) if you're tracking metabolic improvement
8. Common Myths and Mistakes
Myth: "High BCAA levels mean you eat too much protein." Reality: Research on dietary intake versus circulating levels generally shows these are weakly correlated at best. Metabolic dysfunction — specifically, impaired BCAA breakdown in fat and muscle tissue — is the primary driver, not how much protein is on your plate.
Myth: "BCAA supplements cause obesity." Reality: This overstates the evidence. The strongest data here comes from animal studies using BCAA supplementation layered onto an already high-fat diet, which isn't the same as moderate supplementation in an otherwise balanced human diet. The honest takeaway is narrower: chronic, food-derived elevation of circulating BCAAs (the kind seen in obesity) is associated with insulin resistance — that's a different claim than "supplements cause obesity."
Myth: "A BCAA blood test can diagnose insulin resistance or diabetes." Reality: As covered above, this is a research-stage biomarker with moderate, not definitive, diagnostic accuracy. It's a piece of the picture, not the picture.
Myth: "All three BCAAs matter equally." Reality: Current evidence, especially the 2026 Gul et al. data, points to valine as the most clinically informative individual marker for central adiposity and insulin resistance — leucine and isoleucine are relevant but secondary.
Myth: "If I lose weight fast, my BCAA levels will normalize quickly." Reality: At least one controlled trial found no significant BCAA change after six weeks of aggressive calorie restriction, despite real improvements in insulin sensitivity. BCAA normalization may be a slower-moving marker than other metabolic improvements.
Myth: "This is settled science — BCAAs definitely cause insulin resistance." Reality: Even the most recent reviews (Wang et al. 2026) are explicit that the specific mechanisms and clinical significance remain actively debated. Association is well-established; the full causal picture is still being worked out, including ongoing Mendelian randomization research designed specifically to test causality rather than just correlation.
9. Frequently Asked Questions
Are BCAAs bad for you? No. BCAAs are essential nutrients your body needs for muscle maintenance, protein synthesis, and normal metabolic function. The concern in this article is specifically about chronically elevated circulating BCAA levels associated with obesity and insulin resistance — not BCAAs themselves as nutrients.
What is a normal BCAA level in blood? Typical adult reference ranges are roughly 42–100 µmol/L for isoleucine, 66–170 µmol/L for leucine, and 150–310 µmol/L for valine, though exact ranges vary by lab and testing method. Always interpret results against your specific lab's reference range.
Does losing weight lower BCAA levels? It can, but not always quickly or predictably. One study found no significant BCAA reduction after six weeks of very-low-calorie dieting despite meaningful HOMA-IR improvement, suggesting BCAA normalization may lag behind other metabolic markers or require more sustained fat loss.
Should I stop eating high-protein foods if my BCAA levels are high? Current evidence doesn't support this. Circulating BCAA levels appear to be driven primarily by how your body metabolizes BCAAs (linked to insulin resistance and fat tissue function), not by how much protein you eat. Restricting protein could risk muscle loss without addressing the underlying issue.
Can BCAA supplements cause insulin resistance? Animal research has shown that adding BCAA supplementation to an already high-fat diet can worsen insulin resistance independent of weight gain, via mTOR and JNK pathway activation. This doesn't necessarily generalize directly to moderate supplementation in humans with an otherwise balanced diet, but it's a legitimate reason for anyone with existing insulin resistance or metabolic syndrome risk to discuss BCAA supplementation with a doctor before using it regularly.
Which BCAA matters most for visceral fat? Based on the most detailed 2026 clinical data available, valine shows the strongest and most consistent independent associations with both waist circumference and insulin resistance (HOMA-IR) compared to leucine and isoleucine.
Is a BCAA test the same as a glucose or HbA1c test? No. BCAA testing measures specific amino acid concentrations and is currently a research-stage biomarker for metabolic risk. HbA1c and fasting glucose are established, validated diagnostic tools for diabetes. BCAA results should be interpreted alongside these standard markers, not as a replacement for them.
Why do BCAA levels differ between men and women with obesity? Research suggests fat distribution patterns interact with BCAA metabolism differently by sex — one 2025 study found BMI was the strongest BCAA predictor in men, while waist circumference (a marker more specific to central/visceral fat) was the strongest predictor in women. The exact biological reason for this sex difference isn't fully understood yet.
Can children have elevated BCAA levels linked to obesity risk? Yes. Pediatric research has found BCAA panels show moderate diagnostic value for identifying metabolic risk in children with obesity, with combined BCAA levels achieving meaningful (though not perfect) accuracy in distinguishing affected children from healthy-weight peers.
Is visceral fat the same as belly fat? Not exactly. "Belly fat" is a general term that includes both subcutaneous fat (just under the skin, the kind you can pinch) and visceral fat (deeper, surrounding internal organs). Visceral fat is the metabolically active, higher-risk type most closely linked to the BCAA findings discussed in this article — and it's not always visually obvious from body shape alone.
Does exercise lower BCAA levels even without major weight loss? There's evidence supporting exercise as a meaningful lever independent of weight change, particularly through its effects on insulin sensitivity and liver fat in NAFLD patients. Exercise programs lasting 12 months have been used specifically to study this relationship, suggesting sustained, longer-term activity matters more than short-term intervention.
10. Conclusion and Action Steps
The connection between branched-chain amino acids and visceral obesity isn't a fringe theory or a supplement-marketing narrative — it's a well-documented, mechanistically grounded pattern with real clinical data behind it, most recently reinforced by a detailed 2026 study showing valine's strong, independent link to both central adiposity and insulin resistance.
But the honest, complete picture also includes real limitations: this remains a research-stage biomarker, not a diagnostic tool, and the field itself acknowledges that mechanisms and clinical applications are still being worked out.
Here's what to actually do with this information:
If you've had BCAA testing done, bring the results to your physician alongside your other metabolic markers (HOMA-IR, fasting insulin, HbA1c, lipid panel) — don't interpret it in isolation.
If you're concerned about visceral fat, focus on the well-established levers: sustainable weight management, regular resistance and aerobic exercise, and addressing insulin resistance directly — not on manipulating BCAA intake.
Don't restrict dietary protein based on BCAA-related health content without professional guidance — the evidence doesn't support this approach, and it carries real downside risk to muscle health.
If you're considering BCAA supplements for athletic performance and you have any metabolic risk factors, talk to your doctor first — the contexts are different enough that a blanket assumption either way isn't warranted.
Stay appropriately skeptical of absolute claims in either direction — both "BCAAs are dangerous" and "BCAA levels don't matter" oversimplify genuinely nuanced, still-developing science.
If anything in this article raised questions specific to your own health — particularly your weight, blood sugar, or a lab result you've received — that's a conversation for your doctor or an endocrinologist, not a Google search. This article is designed to help you have that conversation more informed, not to replace it.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Gul, F., Ullah, A., Li, Y., Qian, Z., Cao, L., She, D., & Li, Y. (2026). Association between body fat composition and serum branched-chain amino acids in patients with visceral obesity. BMC Endocrine Disorders. https://doi.org/10.1186/s12902-026-02368-x
Wang, D., Wang, X., & Yang, M. (2026). The emerging role of branched-chain amino acid metabolism in obesity. International Journal of Obesity. https://doi.org/10.1038/s41366-026-02103-5
Liu, K., Borreggine, R., Gallart-Ayala, H., Ivanisevic, J., & Marques-Vidal, P. (2025). Serum branched-chain amino acids are mainly associated with body mass index and waist circumference. Nutrition, Metabolism and Cardiovascular Diseases, 35(7), 103880. https://doi.org/10.1016/j.numecd.2025.103880
Zhou, M., Zheng, X., Cao, M., & Zhang, L. (2026). Causal relationship between plasma branched-chain amino acids levels and nonalcoholic fatty liver disease: A bidirectional Mendelian randomization study. Experimental Gerontology. https://doi.org/10.1016/j.exger.2026.113210
Okekunle, A. P., Lee, H., Provido, S. M. P., Chung, G. H., Hong, S., Yu, S. H., Lee, C. B., & Lee, J. E. (2026). Circulating branched-chain amino acids are associated with higher odds of obesity: Findings from the FiLWHEL Study. Nutrition and Metabolic Insights, 19. https://doi.org/10.1177/11786388251395146
Newgard, C. B., An, J., Bain, J. R., et al. (2009). A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metabolism, 9(4), 311–326.
Mansoori, S., et al. (2025). Branched-chain amino acid metabolism: Pathophysiological mechanism and therapeutic intervention in metabolic diseases. Obesity Reviews. https://doi.org/10.1111/obr.13856
Abdualkader, A. M., Karwi, Q. G., Lopaschuk, G. D., & Al Batran, R. (2024). The role of branched-chain amino acids and their downstream metabolites in mediating insulin resistance. Journal of Pharmacy & Pharmaceutical Sciences, 27, 13040.
Mei, J., Yang, F., & Gong, Q. (2026). Branched-chain amino acids and insulin resistance in type 2 diabetes: From metabolic dysregulation to therapeutic targets. Frontiers in Endocrinology.
Huang, H., Chen, H., Yao, Y., et al. (2024). Branched-chain amino acids supplementation induces insulin resistance and pro-inflammatory macrophage polarization via INFGR1/JAK1/STAT1 signal pathway. Molecular Medicine, 30, 149.
Frontiers in Pediatrics (2025). Plasma amino acid profiles in pediatric obesity: Potential biomarkers for the early assessment of metabolic risk.
Tobias, D. K., et al. Caloric restriction improves glycaemic control without reducing plasma branched-chain amino acids or keto-acids in obese men. (Open-access study on VLCD and BCAA response).
Jennings, A., et al. Associations between branched chain amino acid intake and biomarkers of adiposity and cardiometabolic health independent of genetic factors: A twin study.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Insulin Resistance & Prediabetes. (General reference on HOMA-IR and insulin resistance markers.)
American Diabetes Association. Standards of Care in Diabetes. (General reference for HbA1c and diagnostic criteria context.)