Heart Rate Variability (HRV): Why Doctors, Athletes, and Researchers Are Paying Attention
Discover what heart rate variability (HRV) is, why it matters, normal HRV ranges by age, and science-backed ways to improve stress resilience, recovery, and heart health
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/30/202622 min read
Your heart doesn’t beat like a steady drum. The tiny pauses between beats—sometimes a little longer, sometimes shorter—are called heart rate variability, or HRV. And those milliseconds matter.
Think of HRV as your body’s stress report card. When you’re rested, calm, and recovering well, the gaps between heartbeats vary more. That’s high HRV. It means your “rest and digest” nervous system is in charge, keeping you resilient (Shaffer & Ginsberg, 2017). When you’re stressed, sick, sleep-deprived, or pushing too hard, those gaps shrink. Low HRV is your body waving a yellow flag.
Why should you care? Research from 2025–2026 shows HRV connects your brain and heart in powerful ways (Liu et al., 2025). Lower HRV is linked to higher risk of high blood pressure (American Heart Association, 2025), heart problems, anxiety, and poor sleep. The good news: HRV isn’t set in stone. You can improve it.
Start simple. Get consistent, quality sleep because your HRV responds within days. Breathe slowly, around 5–6 breaths per minute, for 5 minutes a day. This “resonance breathing” is the core of HRV biofeedback, which has been shown to increase vagal tone in cardiovascular patients (Kaneko et al., 2026). Move your body, but don’t overtrain, because recovery matters for HRV (Dong, 2016). Limit alcohol, especially before bed, because it reduces HRV overnight.
Wearables can help you track trends, but don’t panic over one low day. Measurement conditions matter, and supine morning readings are most reliable (Besson et al., 2025). Look at your 7-day average. And remember, your number is yours. A healthy 55-year-old might have higher HRV than a stressed 25-year-old.
HRV won’t diagnose disease, and it’s not a replacement for medical care. But it is a window into how well your body is balancing stress and recovery. Listen to it. Small daily choices add up. Over weeks, your heart’s hidden language gets stronger. And so do you.
Key Takeaways About Heart Rate Variability (HRV)
HRV measures the variation in time between heartbeats, reflecting how well your autonomic nervous system adapts to stress, recovery, and daily demands.
Higher HRV is generally associated with better health, improved stress resilience, stronger cardiovascular function, and enhanced recovery from exercise.
Lower HRV may indicate physiological strain, including poor sleep, chronic stress, illness, overtraining, inflammation, or increased cardiovascular risk.
Sleep quality is one of the strongest drivers of HRV, making consistent, restorative sleep essential for autonomic nervous system health.
Evidence-based strategies such as aerobic exercise, slow breathing, stress management, and a Mediterranean-style diet can improve HRV over time.
Track HRV trends rather than single readings, as day-to-day fluctuations are normal and long-term patterns provide the most meaningful insights into health and recovery.
Bottom Line: Heart rate variability is a powerful, non-invasive biomarker that provides valuable insights into stress, recovery, cardiovascular health, and overall physiological resilience.
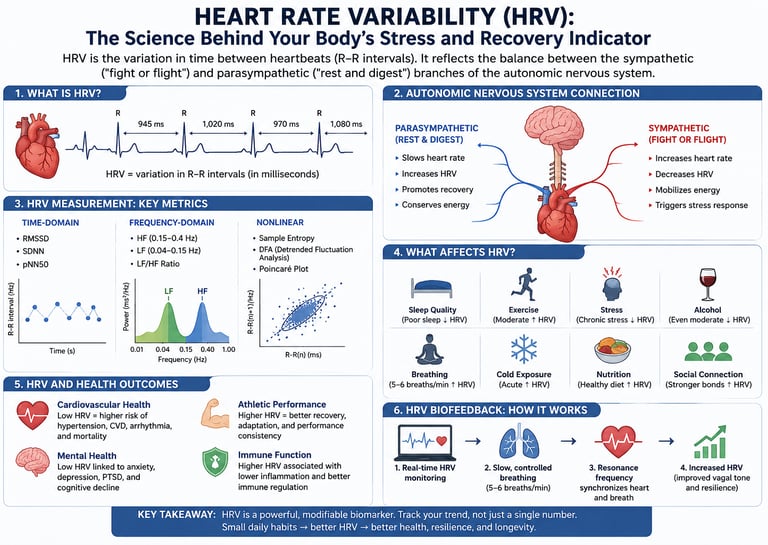
1. What Is Heart Rate Variability (HRV)?
Heart rate variability refers to the variation in time intervals between consecutive heartbeats — technically called R-R intervals (or inter-beat intervals, IBI), named after the "R" peaks on an electrocardiogram (ECG).
Your heart does not beat like a metronome. Even if your average heart rate is 60 beats per minute, the gap between each beat might be 900ms, then 1,050ms, then 950ms. That variation is HRV.
Higher HRV generally = healthier, more adaptable nervous system.
Lower HRV generally = more physiological stress, fatigue, or disease risk.
The Autonomic Nervous System Connection
HRV is a direct window into your autonomic nervous system (ANS) — the part of your nervous system that runs automatically without conscious thought, controlling heart rate, digestion, breathing, and more.
The ANS has two branches:
Sympathetic nervous system ("fight or flight"): Speeds up the heart, reduces variability
Parasympathetic nervous system ("rest and digest"): Slows the heart, increases variability
When you're stressed, sleep-deprived, overtrained, or sick, your sympathetic system dominates — and HRV drops. When you're rested, recovered, and calm, parasympathetic activity rises — and HRV increases.
Key insight: HRV is essentially a real-time report card on how well your nervous system is balancing these two branches.
2. How HRV Is Measured
HRV can be measured in several ways, each capturing different aspects of autonomic function.
Time-Domain Metrics
These are the simplest and most commonly reported:
RMSSD (Root Mean Square of Successive Differences): The most widely used metric in consumer wearables. It reflects short-term HRV and parasympathetic activity.
SDNN (Standard Deviation of all NN intervals): Reflects overall HRV across both ANS branches. More common in clinical ECG readings.
pNN50: The percentage of successive R-R interval differences greater than 50ms.
Frequency-Domain Metrics
These analyze HRV using spectral analysis — breaking the signal into frequency bands:
HF (High Frequency, 0.15–0.4 Hz): Strongly tied to parasympathetic (vagal) activity and respiratory patterns
LF (Low Frequency, 0.04–0.15 Hz): Reflects a mix of sympathetic and parasympathetic modulation
LF/HF Ratio: Once thought to be a pure sympathetic/parasympathetic balance indicator — now considered more nuanced (more on this in the myths section)
Nonlinear Metrics
Newer research increasingly uses nonlinear measures like DFA alpha1, sample entropy, and approximate entropy to capture the complexity of heart rhythm patterns beyond simple averages.
Short-Term vs. Long-Term HRV Measurements
A 2025 study published in Scientific Reports by Besson et al. examined the clinical reliability of short-term HRV measurements across dual environments (lab vs. field) and dual positions (supine vs. standing). The researchers found that measurement conditions significantly affect HRV values — a critical point for anyone using wearable data.
Short-term recordings (1–5 minutes) are most common in consumer devices. Clinical gold-standard measurements typically use 24-hour ambulatory ECG recordings (Holter monitors).
3. Why HRV Matters: The Science
HRV isn't just a curiosity — it's one of the most robust biomarkers ever studied. Decades of research link it to:
Cardiovascular disease risk and mortality
Mental health and anxiety disorders
Athletic performance and recovery
Cognitive function and brain health
Sleep quality
Inflammation and immune function
A 2025 review in Frontiers in Cardiovascular Medicine by Liu, Cui, and Chen described HRV as a "multidimensional physiological marker" with strong predictive value across a spectrum of conditions — from heart failure to psychiatric disorders. They specifically highlight HRV's role in what researchers now call the brain-heart axis.
HRV as a Predictor of Mortality
Reduced HRV is one of the strongest independent predictors of all-cause mortality in both healthy adults and those with heart disease. In post-myocardial infarction patients, low HRV was shown to predict sudden cardiac death independently of other risk factors.
HRV and Inflammation
Chronic low-grade inflammation — a driver of nearly every major chronic disease — is closely connected to HRV. The vagal anti-inflammatory reflex means that higher parasympathetic (vagal) tone, reflected by higher HRV, actively suppresses inflammatory pathways.
This is why athletes with high HRV often show lower CRP (C-reactive protein) and other inflammatory markers.
4. HRV and the Brain-Heart Axis
One of the most exciting frontiers in HRV research is the brain-heart axis — the bidirectional communication network between the brain and the cardiovascular system.
The 2025 review by Liu et al. lays out how HRV fluctuations can predict disorders across this axis, including:
Depression and anxiety: Lower HRV is consistently found in anxiety disorders, reflecting reduced prefrontal control over limbic responses.
PTSD: Trauma significantly blunts parasympathetic activity, reducing HRV — and HRV biofeedback is emerging as a therapeutic tool.
Cognitive decline: Higher HRV in older adults is linked to better executive function, attention, and memory.
Schizophrenia and bipolar disorder: Both are associated with markedly reduced HRV, suggesting disrupted autonomic-brain regulation.
The practical implication: Your HRV score isn't just a fitness metric. It reflects how well your brain and body are communicating — and how resilient your entire physiology is to stress.
5. What Is a Good HRV? Norms by Age and Fitness {#hrv-norms}
This is one of the most common questions about HRV — and the honest answer is: it depends.
HRV is highly individual. Comparing your number to someone else's is rarely useful. What matters far more is:
Your personal baseline trend over time
How your HRV changes in response to stress, sleep, and lifestyle
That said, general population norms exist.
HRV Reference Ranges (RMSSD, ms)
20–29 years:
Lower HRV: < 40 ms
Typical HRV: 55–70 ms
Higher HRV: > 80 ms
30–39 years:
Lower HRV: < 35 ms
Typical HRV: 45–60 ms
Higher HRV: > 70 ms
40–49 years:
Lower HRV: < 28 ms
Typical HRV: 38–50 ms
Higher HRV: > 60 ms
50–59 years:
Lower HRV: < 22 ms
Typical HRV: 30–42 ms
Higher HRV: > 52 ms
60–69 years:
Lower HRV: < 18 ms
Typical HRV: 24–35 ms
Higher HRV: > 45 ms
70 years and older:
Lower HRV: < 15 ms
Typical HRV: 18–28 ms
Higher HRV: > 38 ms
Important: HRV naturally declines with age. However, regular physical activity, good sleep, stress management, and overall cardiovascular fitness can help maintain higher HRV levels. Tracking your personal HRV trend over time is far more valuable than comparing your numbers with population averages.
Ranges are approximations based on population studies; individual variation is substantial.
Factors That Affect "Normal" HRV
Fitness level: Elite endurance athletes routinely have HRV scores 2–3× higher than sedentary peers
Sex: Women tend to have slightly lower RMSSD than men of the same age, though differences narrow with fitness
Measurement time: Morning resting HRV (upon waking) is most reliable for tracking trends
Body position: Supine HRV is higher than standing HRV — always measure in the same position
The golden rule of HRV: Track your own trend. A consistent upward trend over weeks and months matters far more than any single number.
6. HRV and Cardiovascular Disease
A landmark 2025 study published in Hypertension (AHA Journals) examined HRV's relationship to hypertension risk. The researchers found that reduced HRV preceded the development of hypertension in previously normotensive adults — suggesting HRV may serve as an early warning biomarker for high blood pressure.
HRV in Heart Failure and Arrhythmia
In patients with established heart failure, HRV analysis helps stratify risk and guide treatment intensity. Severely reduced HRV in this population is associated with higher risk of ventricular arrhythmia and sudden death.
HRV After Myocardial Infarction
Post-MI patients with low HRV have a significantly elevated risk of re-infarction and sudden cardiac death. Monitoring HRV in this group helps guide decisions about implantable cardioverter-defibrillators (ICDs) and pharmacotherapy.
A 2026 paper in the European Journal of Clinical Investigation (ScienceDirect) explored real-time HRV frameworks for clinical monitoring, demonstrating that continuous HRV tracking in cardiac patients enables earlier detection of deterioration than standard vital signs alone.
⚠️ Medical note: If you have heart disease, arrhythmia, or are at high cardiovascular risk, HRV monitoring should be discussed with your cardiologist. Do not make clinical decisions based on consumer wearable HRV data alone.
7. HRV Biofeedback: A Powerful Tool for Recovery
HRV biofeedback is a technique in which you receive real-time feedback about your heart rate patterns and learn to consciously regulate them — typically through controlled breathing at a specific rate (usually 5–6 breaths per minute, known as resonance frequency breathing).
The Evidence Is Strong
A 2026 systematic review and meta-analysis by Kaneko et al., published in Applied Psychophysiology and Biofeedback, examined HRV biofeedback specifically in patients with cardiovascular disease. Key findings:
HRV biofeedback significantly increased vagal tone (parasympathetic activity)
Improvements were seen in RMSSD, SDNN, and HF power
Benefits were observed after as little as 4–8 weeks of regular practice
The technique was safe and well-tolerated even in high-risk cardiac populations
How HRV Biofeedback Works in Practice
Find your resonance frequency breathing rate (typically 5–6 breaths/min, or about 4.5–6 seconds per inhale and exhale)
Use a biofeedback device or app to watch your HRV in real time
Practice 20 minutes per day, ideally in two 10-minute sessions
Consistency matters — improvements compound over 4–12 weeks
Who Benefits Most from HRV Biofeedback?
People with anxiety or chronic stress
Athletes seeking faster recovery
Individuals with hypertension or pre-hypertension
Post-cardiac event patients (under medical supervision)
People with PTSD or trauma histories
8. How to Improve Your HRV: Proven Strategies
HRV isn't fixed. It responds — sometimes dramatically — to lifestyle changes. Here are the interventions with the strongest evidence base.
1. Prioritize Sleep Quality
Sleep is the single biggest modulator of next-day HRV. Poor sleep quality, sleep deprivation, and irregular sleep schedules all crush HRV. Aim for:
7–9 hours per night
Consistent wake time (even on weekends)
Cool, dark sleep environment
Limiting alcohol within 3 hours of bedtime (alcohol devastates HRV even in small amounts)
2. Exercise — But Don't Overdo It
Regular aerobic exercise is one of the most reliable HRV improvers. However, the relationship is dose-dependent:
Moderate aerobic exercise (3–5 sessions/week at 60–75% max heart rate): Consistently raises resting HRV over weeks
Overtraining / insufficient recovery: Acutely reduces HRV — a key signal to back off
Pro tip: Use morning HRV readings to guide training intensity. If your HRV is significantly below your baseline, reduce training load that day.
3. Practice Slow, Controlled Breathing
Even outside formal biofeedback sessions, slow diaphragmatic breathing (5–6 breaths per minute) for 5–10 minutes acutely raises HRV and lowers perceived stress. This is one of the few tools that works immediately.
4. Cold Exposure (Selectively)
Cold water immersion and cold showers have shown acute increases in HRV in several studies, likely via activation of the diving reflex (which triggers vagal activation). Start with 30–60 seconds of cold water at the end of your shower.
5. Manage Chronic Stress
Chronic psychological stress is one of the most powerful HRV suppressors. Evidence-based approaches include:
Mindfulness meditation (even 10 minutes/day improves HRV over 8 weeks in multiple RCTs)
Cognitive behavioral therapy (CBT) for anxiety
Social connection — strong social bonds consistently predict higher HRV
Nature exposure — spending time in green spaces measurably raises HRV
6. Optimize Nutrition
Anti-inflammatory diet (Mediterranean pattern): Associated with higher HRV in population studies
Omega-3 fatty acids: Multiple trials show modest HRV improvements with fish oil supplementation (2–4g EPA+DHA/day)
Limit ultra-processed foods: High ultra-processed food consumption is linked to lower HRV
Hydration: Even mild dehydration reduces HRV
7. Limit Alcohol
Even moderate alcohol consumption significantly depresses HRV during sleep — a finding so consistent that researchers now use overnight HRV as a biomarker for alcohol intake. If you drink, try to keep it to 1–2 drinks and allow at least 3 hours before sleep.
HRV Improvement Timeline
Breathing exercises and HRV biofeedback: Improvements may be noticeable within 1–4 weeks of regular practice.
Sleep optimization: Better sleep quality and consistency can enhance HRV in as little as 1–2 weeks.
Aerobic exercise training: Sustained cardiovascular training typically produces measurable HRV improvements within 4–8 weeks.
Stress reduction practices (meditation, mindfulness, relaxation techniques): Benefits are often observed after 4–8 weeks of consistent practice.
Omega-3 fatty acid supplementation: Changes in HRV generally become apparent after 8–12 weeks of regular supplementation.
Comprehensive lifestyle improvement: Combining exercise, nutrition, sleep, stress management, and recovery habits may lead to substantial HRV improvements over 3–6 months.
Key Point: HRV responds gradually to positive lifestyle changes. Consistency matters more than intensity, and long-term trends are far more meaningful than day-to-day fluctuations.
9. HRV Wearables: What the Research Says
Consumer HRV wearables have exploded in popularity. But how accurate are they?
The Short Answer
Good wrist-based devices are reasonably accurate for tracking trends, but not for absolute clinical values.
The 2025 study by Besson et al. in Scientific Reports rigorously tested short-term HRV measurement reliability across environments and positions. Key takeaways:
Supine measurements are significantly more reliable than standing or seated measurements
Environmental conditions matter — temperature, movement, and lighting affect optical sensors
RMSSD is the most reliable metric for short-term recordings
Clinical-grade HRV still requires a chest-strap ECG or Holter monitor
Wearable Comparison at a Glance
Here is the device comparison breakdown rewritten for quick, clean scanning:
Holter ECG (Clinical): Uses clinical-grade electrical sensors (gold standard), providing very high accuracy. It is best utilized for formal medical and clinical diagnosis.
Chest Strap (e.g., Polar H10): Uses electrical sensors to deliver high accuracy. It is best suited for athletes, trainers, and field researchers.
Apple Watch (ECG Mode): Uses on-demand electrical sensors to achieve high accuracy. It is best for reliable daily monitoring and periodic spot checks.
Wrist Wearables (e.g., Garmin, WHOOP, Fitbit): Rely on optical sensors (PPG) that offer moderate accuracy. They are best optimized for longitudinal lifestyle and recovery trend tracking.
Smartphone Camera Apps: Utilize basic optical sensing through the phone lens, resulting in low-to-moderate accuracy. They are best restricted to occasional, casual spot checks
Best Practices for Wearable HRV Tracking
Always measure at the same time and position (supine, upon waking before getting up)
Use a 5-minute measurement window minimum; 1-minute readings are less reliable
Look at 7-day rolling averages, not single-day values
Establish your personal baseline over 2–3 weeks before making decisions
10. Common HRV Myths and Mistakes
Myth 1: "Higher HRV is always better"
Not necessarily. Extremely high HRV in the presence of symptoms — especially in older adults — can sometimes indicate pathological states like sick sinus syndrome or atrial fibrillation. Context always matters.
Myth 2: "The LF/HF ratio tells you your sympathetic/parasympathetic balance"
This was a popular interpretation for decades, but it's been substantially revised. A 2026 review in Frontiers in Physiology by Banerjee explicitly identifies this as a major shortcoming of HRV analysis. LF power reflects both ANS branches, and the ratio is heavily influenced by breathing rate and other non-autonomic factors. Modern HRV researchers rely less on this metric.
Myth 3: "One low HRV reading means something is wrong"
HRV fluctuates naturally day to day. A single low reading is almost always meaningless. What matters is your trend over 1–4 weeks.
Myth 4: "HRV only matters for athletes"
HRV is equally — arguably more — valuable for non-athletes managing stress, sleep, chronic disease, or mental health. Athletes just popularized the metric.
Myth 5: "HRV apps on your phone are accurate enough for health decisions"
For casual trend awareness, perhaps. For any clinical or health decision, you need higher-quality hardware (chest strap ECG at a minimum).
Mistake: Measuring HRV at different times of day
HRV follows a circadian rhythm. Afternoon HRV is not comparable to morning HRV. Always measure at the same time (morning resting is the standard).
Mistake: Ignoring confounders
Illness, alcohol, dehydration, travel across time zones, menstrual cycle phase, and medications (especially beta-blockers) all substantially alter HRV. Account for these when interpreting your data.
11. HRV Measurement Checklist
Use this checklist for the most reliable HRV readings:
Before Measurement:
Just woken up — before getting out of bed
No alcohol in the past 12 hours
Bladder not uncomfortably full
Room temperature comfortable
No intense emotional stress in past 30 minutes
During Measurement:
Lying supine (on your back)
Breathing naturally — don't try to control it
Minimum 5-minute recording
Using a validated device (chest strap preferred)
For Tracking:
Consistent measurement time daily
Recording sleep quality and duration alongside HRV
Noting training load, stress events, alcohol, illness
Looking at 7-day rolling averages, not single data points
12. Evidence Summary Table
Besson et al. (Scientific Reports, 2025)
Demonstrated that body position and measurement environment significantly influence HRV values and reliability.
Evidence Strength: High
Liu, Cui & Chen (Frontiers in Cardiovascular Medicine, 2025)
Identified HRV as a multidimensional physiological marker linking cardiovascular, neurological, and psychiatric disorders through the brain-heart axis.
Evidence Strength: High (Review)
Kaneko et al. (Applied Psychophysiology and Biofeedback, 2026)
Found that HRV biofeedback significantly improves vagal activity and autonomic function in patients with cardiovascular disease.
Evidence Strength: High (Meta-analysis)
Banerjee (Frontiers in Physiology, 2026)
Highlighted important methodological limitations of traditional HRV metrics, particularly the LF/HF ratio as a marker of autonomic balance.
Evidence Strength: High (Review)
Nakano et al. (Journal of Medical Systems, 2026)
Developed a real-time, personalized HRV monitoring framework with potential clinical applications for continuous patient assessment.
Evidence Strength: Moderate
Hypertension (American Heart Association), 2025
Reported that lower HRV predicts future hypertension development in adults with previously normal blood pressure.
Evidence Strength: High
Overall Conclusion: Current evidence supports HRV as a valuable biomarker for autonomic function, cardiovascular health, stress resilience, disease prediction, and personalized health monitoring.
13. FAQs
What is a good HRV for my age?
HRV declines with age. For reference: adults in their 20s typically average 55–70 ms (RMSSD), while those in their 50s average around 30–42 ms. However, these are population averages. A fit 55-year-old may have a higher HRV than a sedentary 25-year-old. Focus on your personal trend, not population comparisons.
How quickly can I improve my HRV?
Some interventions — like slow breathing exercises and HRV biofeedback — can produce measurable improvements in 1–4 weeks. Aerobic training effects on HRV typically take 4–8 weeks of consistent effort to show. Sleep quality improvements often show effects within 1–2 weeks.
Does HRV predict heart attacks?
Reduced HRV is an established risk marker for major cardiovascular events, particularly in people with existing heart disease. However, HRV alone cannot predict heart attacks. It is most useful as one factor among many in cardiovascular risk assessment.
Can stress permanently lower HRV?
Chronic, unmanaged psychological stress can chronically suppress HRV — but this is largely reversible with appropriate intervention. HRV is dynamic, not fixed. Even years of low HRV can improve significantly with lifestyle change and stress management.
Is HRV the same as heart rate?
No. Heart rate (HR) measures average beats per minute. HRV measures the variation between those beats. You can have the same resting heart rate as another person but very different HRV scores.
Should I measure HRV every day?
Daily measurement is ideal for tracking trends, but only if you're consistent about conditions (time, position, device). For most people, measuring 5–7 days per week and viewing rolling averages gives the most actionable data.
Does caffeine affect HRV?
Yes. Caffeine is a stimulant that temporarily reduces HRV by increasing sympathetic nervous system activity. For the most accurate baseline measurements, measure HRV before caffeine consumption in the morning.
Can HRV biofeedback replace medication for hypertension?
No — HRV biofeedback is a complementary approach, not a replacement for medication. However, research (including Kaneko et al.'s 2026 meta-analysis) shows it meaningfully improves autonomic function in cardiovascular patients and may reduce medication needs in some cases. Always discuss with your physician.
What's the best wearable for HRV monitoring?
For research-grade accuracy, the Polar H10 chest strap is widely considered the consumer gold standard. Among wrist devices, the Apple Watch (in ECG mode) and WHOOP are among the most validated. Accuracy varies; always pair any wearable with contextual data (sleep, stress, training).
Is HRV affected by breathing?
Profoundly. Breathing is the dominant driver of short-term HRV through a phenomenon called respiratory sinus arrhythmia (RSA). This is why breathing slowly (5–6 breaths/min) acutely increases HRV — and why your HRV reading can change significantly depending on whether you breathe fast or slow during measurement. Standardising breathing rate during measurements is important for comparability.
Can children and teenagers use HRV monitoring?
Yes. HRV monitoring is safe for children and is used in pediatric research and clinical settings. Children and adolescents generally have higher HRV than adults, and HRV naturally declines through early adulthood.
What medications affect HRV?
Several common medications significantly alter HRV:; anticholinergics reduce parasympathetic tone; SSRIs may modestly increase HRV over time; stimulant medications (Adderall, etc.) typically reduce HRV acutely. If you're on regular medications, consult your physician before using HRV to guide health decisions.
14. How do beta blockers affect HRV?
The answer depends on which aspect of HRV you're looking at.
Short Answer
Beta-blockers are generally associated with higher HRV and improved autonomic balance, which is usually considered beneficial. However, they can also alter HRV measurements, making interpretation more complicated.
Why Beta-Blockers Often Increase HRV
Beta-blockers (such as Metoprolol, Bisoprolol, and Atenolol) block sympathetic ("fight-or-flight") stimulation of the heart.
As a result, they:
Reduce heart rate
Decrease sympathetic activity
Allow greater parasympathetic (vagal) influence
Often increase RMSSD and other HRV measures
In patients with:
Hypertension
Heart failure
Coronary artery disease
Post-heart attack states
an increase in HRV after beta-blocker therapy is generally viewed as a favorable sign.
Why Interpretation Gets Tricky
A higher HRV caused by medication is not necessarily the same as a higher HRV resulting from:
Better fitness
Better sleep
Lower stress
Improved cardiovascular health
The drug is directly modifying autonomic input to the heart.
Therefore:
HRV values measured while taking beta-blockers cannot be directly compared with HRV values from people who are not taking beta-blockers.
What Researchers Usually Do
Most HRV studies either:
Exclude people taking beta-blockers, or
Adjust statistical analyses for medication use
because beta-blockers can substantially influence HRV metrics.
Practical Takeaway
For cardiovascular patients: Beta-blockers are often beneficial and may improve HRV.
For HRV tracking: Beta-blockers can artificially alter HRV readings, so trends should be interpreted cautiously.
For athletes: Starting or stopping a beta-blocker can dramatically change HRV values independent of fitness changes.
One Important Myth
Many articles incorrectly state:
"Beta-blockers reduce HRV."
What beta-blockers reliably reduce is heart rate. In contrast, many studies show they increase vagally mediated HRV measures, particularly RMSSD and HF power, although effects vary by drug, dose, and patient population.
Bottom line: From an HRV perspective, beta-blockers are usually associated with higher HRV and reduced sympathetic stress, which is generally favorable clinically. However, they also make HRV a less "pure" reflection of your natural autonomic state, so HRV data should always be interpreted in the context of medication use.
15. HRV in Exercise Physiology: What Athletes Should Know
Sports scientists increasingly use HRV to monitor training adaptation, recovery, and fatigue. One emerging metric is DFA alpha1 (Detrended Fluctuation Analysis alpha1), a nonlinear HRV measure that reflects the complexity of autonomic regulation during exercise. Research suggests that a DFA alpha1 value around 0.75 may correspond closely to the first ventilatory or aerobic threshold, making it a promising tool for exercise intensity prescription.
HRV-guided training uses daily HRV measurements to adjust workout intensity. Studies have shown that athletes who modify training based on HRV trends often achieve similar or greater fitness improvements while reducing the risk of excessive fatigue compared with fixed training programs.
As aerobic fitness improves, resting HRV generally increases, reflecting enhanced parasympathetic (vagal) activity and improved autonomic flexibility. This adaptation is commonly observed in endurance-trained individuals.
Importantly, HRV can help distinguish functional overreaching from overtraining syndrome. A temporary reduction in HRV may occur during periods of intensified training and can be part of a normal adaptation process. However, persistently suppressed HRV accompanied by declining performance, poor recovery, sleep disturbances, and mood changes may indicate non-functional overreaching or overtraining, warranting a reduction in training load and greater recovery emphasis.
16. Clinical pearls
Pearl 1: The Trap of "Universal Standards" (Individual Baselines vs. Population Averages)
Scientific Perspective: HRV displays immense inter-individual variability heavily driven by unmodifiable factors like age, biological sex, genetics, and baseline fitness levels (Banerjee, 2026). Attempting to evaluate a patient's health by comparing their absolute time-domain metrics (such as RMSSD) against a broad population average is clinically flawed.
Never compare your HRV score to your spouse's, your training partner's, or an online chart. Your HRV is as unique to you as a fingerprint. What matters is your personal trend over time—if your 7-day rolling average is improving, your health and recovery are moving in the right direction, regardless of what the absolute number is.
Pearl 2: Posture and Environment Destabilize Short-Term Metrics
Scientific Perspective: Short-term HRV recordings (typically 1–5 minutes) are highly sensitive to external variables. Rigorous dual-environment testing demonstrates that changing measurement positions (e.g., switching from supine to standing) or altering ambient surroundings significantly shifts autonomic regulation and introduces measurement variance (Besson et al., 2025).
To get a clean, reliable reading from a wearable device, you must standardize your routine. The gold standard is to check it every single morning, immediately upon waking, while lying flat on your back (supine). If you check it sitting up one day and standing the next, or after walking around, the data becomes useless noise.
Pearl 3: The Obsolescence of the LF/HF Ratio for "Sympathetic Tone"
Scientific Perspective: Historically, the low-frequency to high-frequency (LF/HF) spectral ratio was viewed as a clean metric for "sympathetic-parasympathetic balance." Contemporary autonomic research has overturned this, noting that LF power is highly complex, heavily modulated by parasympathetic activity and breathing rates, and prone to severe methodological shortcomings (Banerjee, 2026).
If your health app or smart ring gives you a breakdown of "stress vs. rest" based on an LF/HF ratio, ignore it. For a reliable snapshot of your nervous system's recovery, focus almost exclusively on RMSSD—the standard time-domain metric that cleanly tracks parasympathetic ("rest and digest") activity.
Pearl 4: The Vulnerability of Optical (PPG) Sensors to Rhythm Distortions
Scientific Perspective: Consumer wearables rely primarily on photoplethysmography (PPG)—using light sensors to detect blood volume changes at the wrist or finger. PPG is highly susceptible to motion artifacts, changes in skin perfusion, and ectopic beats (such as PVCs or PACs); these artifacts can destabilize algorithmic filtering and completely distort HRV readings (Banerjee, 2026).
If you have an underlying heart rhythm issue like Atrial Fibrillation (AFib) or frequent skipped beats, your consumer wearable's HRV data will likely be inaccurate or erratic. If you need precise data for athletic or health reasons, opt for an electrical chest-strap monitor (like a Polar H10), which tracks the heart's raw electrical signals like a clinical ECG.
Pearl 5: The Therapeutic Efficacy of Cardiorespiratory Resonance
Scientific Perspective: Heart rate variability biofeedback (HRV-BF) explicitly utilizes paced diaphragmatic breathing to stimulate the baroreflex and optimize vagal tone. Systematic meta-analysis confirms that training at a patient's "resonance frequency" (typically 5 to 6 breaths per minute) successfully increases RMSSD, SDNN, and high-frequency power, even in high-risk cardiovascular disease populations (Kaneko et al., 2026).
You can actively train your nervous system to be more resilient. Practicing slow, controlled belly breathing at about 5.5 breaths per minute—roughly a 5-second inhale and a 5-second exhale—for 10 to 20 minutes a day acts like a workout for your vagus nerve, lowering physiological stress and physically boosting your baseline HRV over 4 to 8 weeks.
Pearl 6: Confounding Organ Specificity (HRV is Cardiac-Specific)
Scientific Perspective: While sympathetic output can manifest as generalized systemic activation, parasympathetic (vagal) regulation is highly organ-specific. Clinicians must recognize that cardiac vagal tone, as indexed by HRV metrics, cannot be used to infer parasympathetic functioning or autonomic health in non-cardiac organ systems (Banerjee, 2026).
While a high HRV is a fantastic indicator that your cardiovascular system and brain-heart connection are rested and healthy, it isn't an all-powerful shield. It doesn't tell you how well your digestive tract, liver, or kidneys are functioning. Use HRV as a tool for tracking stress and heart health, not as a master dashboard for your entire body's internal medicine.
16. Conclusion and Action Steps
Heart rate variability is one of the most scientifically validated and practically useful health metrics available to you today — and it's increasingly accessible through consumer wearables. But HRV is only as valuable as the context you bring to it.
Here's what the current science makes clear:
Higher HRV reflects healthier autonomic balance and is linked to better cardiovascular, mental, and cognitive health
HRV is modifiable — sleep, exercise, breathing, stress management, and nutrition all have measurable effects
HRV biofeedback is a legitimate therapeutic tool, supported by 2026 meta-analysis data, even for cardiovascular patients
Wearable accuracy is improving but still imperfect — use consumer devices for trend tracking, not clinical decisions
The LF/HF ratio is not the reliable autonomic balance marker it was once thought to be
Your Action Plan
Start tracking your morning HRV today — use a validated device, measure supine, same time daily
Establish your baseline over 2–3 weeks before drawing conclusions
Prioritize sleep above all else — it's the most powerful single lever for HRV
Add 5 minutes of slow breathing (5–6 breaths/min) to your morning routine
Begin or maintain a consistent aerobic exercise program — aim for 150+ minutes/week
Limit alcohol, especially within 3 hours of sleep
If you have cardiovascular disease, ask your cardiologist about formal HRV monitoring and biofeedback
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your medication, diet, or treatment plan. The clinical thresholds discussed represent general evidence-based guidance; individual targets should be determined with your physician.
Related Articles
GLP-1 Receptor Agonists and Cardiovascular Protection: Evidence from CVOT Trials Explained
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Atherogenic Dyslipidemia Explained: The Role of ApoB in Hidden Cardiovascular Risk
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
References
American Heart Association Journals. (2025). Hypertension and HRV. Hypertension. https://www.ahajournals.org/doi/10.1161/HYPERTENSIONAHA.125.26014
Banerjee, A. (2026). Understanding the shortcomings of heart rate variability as a tool for autonomic analysis. Frontiers in Physiology, 17, Article 1760160. https://doi.org/10.3389/fphys.2026.1760160
Besson, C., Baggish, A. L., Monteventi, P., Schmitt, L., Stucky, F., & Gremeaux, V. (2025). Assessing the clinical reliability of short-term heart rate variability: Insights from controlled dual-environment and dual-position measurements. Scientific Reports, 15, Article 5611. https://doi.org/10.1038/s41598-025-89892-3
Dong, J. G. (2016). The role of heart rate variability in sports physiology. Experimental and Therapeutic Medicine, 11(5), 1531–1536. https://doi.org/10.3892/etm.2016.3104
Kaneko, K., Aikawa, G., Sakuramoto, H., Ota, Y., Oyama, Y., Tomooka, M., Naya, K., Fukunaga, T., Sugishima, K., & Yamada, T. (2026). Effects of heart rate variability biofeedback on cardiac autonomic function in patients with cardiovascular disease: A systematic review and meta-analysis. Applied Psychophysiology and Biofeedback. https://doi.org/10.1007/s10484-025-09765-3
Kiviniemi, A. M., Hautala, A. J., Kinnunen, H., & Tulppo, M. P. (2007). Endurance training guided individually by daily heart rate variability measurements. European Journal of Applied Physiology, 101(6), 743–751. https://doi.org/10.1007/s00421-007-0552-2
Kleiger, R. E., Miller, J. P., Bigger, J. T., & Moss, A. J. (1987). Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. The American Journal of Cardiology, 59(4), 256–262. https://doi.org/10.1016/0002-9149(87)90795-8
Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research — Recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, Article 213. https://doi.org/10.3389/fpsyg.2017.00213
Lehrer, P. M., & Gevirtz, R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 5, Article 756. https://doi.org/10.3389/fpsyg.2014.00756
Liu, S., Cui, Y., & Chen, M. (2025). Heart rate variability: A multidimensional perspective from physiological marker to brain-heart axis disorders prediction. Frontiers in Cardiovascular Medicine, 12, Article 1630668. https://doi.org/10.3389/fcvm.2025.1630668
Malik, M. (1996). Heart rate variability. Annals of Noninvasive Electrocardiology, 1(2), 151–181. https://doi.org/10.1111/j.1542-474X.1996.tb00275X
Nakano, T., Fujino, M., Miyata, M., & Nakasuka, S. (2026). A clinically oriented framework for real-time heart rate variability analysis: A novel approach to personalized and robust monitoring. Journal of Medical Systems, 50, Article 13. https://doi.org/10.1007/s10916-026-02342-z
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, Article 258. https://doi.org/10.3389/fpubh.2017.00258
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996). Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation, 93(5), 1043–1065. https://doi.org/10.1161/01.CIR.93.5.1043
Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J., & Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neuroscience & Biobehavioral Reviews, 36(2), 747–756. https://doi.org/10.1016/j.neubiorev.2011.11.009This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your health management, especially if you have a diagnosed cardiovascular condition.
Last updated: May 2026 | Reviewed against literature through 2026