Fatty Liver, Insulin Resistance, and Hidden Organ Fat: What Actually Works
Cut liver fat, improve cholesterol, and boost insulin sensitivity. Discover the most effective strategy: combining diet and exercise.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/30/202613 min read
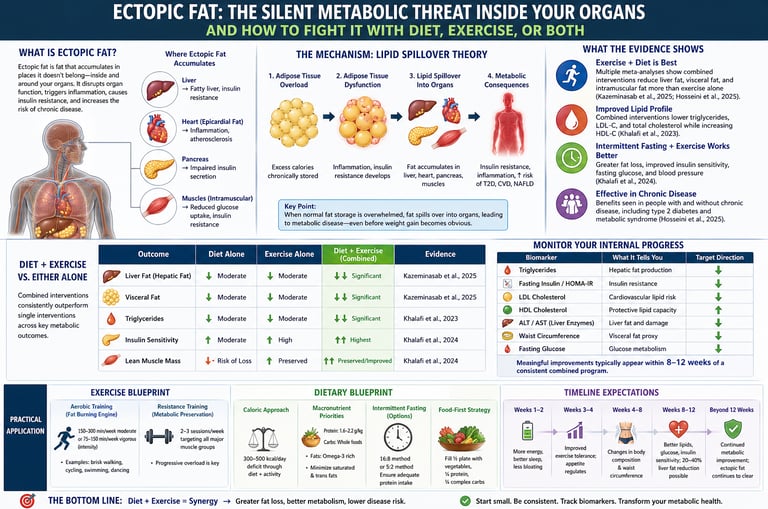
What is ectopic fat, and how do you reduce it?
Ectopic fat is fat stored in organs like the liver, heart, pancreas, and muscles, where it disrupts metabolism and increases the risk of Type 2 Diabetes, Non-Alcoholic Fatty Liver Disease, and cardiovascular disease.
How Ectopic Fat Develops
Caloric excess → adipose tissue overload
Adipose dysfunction → lipid spillover
Fat deposition in organs:
Liver → triglyceride overproduction
Muscle → impaired glucose uptake
Pancreas → beta-cell dysfunction
Result → Insulin Resistance + metabolic disease
The most effective strategy to reduce ectopic fat is a combination of diet and exercise, which works by:
Lowering liver fat production
Increasing fat oxidation
Improving insulin sensitivity
Best evidence-based approach:
150–300 min/week aerobic exercise
2–3 resistance sessions/week
Moderate calorie deficit (300–500 kcal/day)
Optional intermittent fasting
Combined interventions reduce liver fat by up to 20–40% in 8–12 weeks
Results depend on the starting point, consistency, age, other health conditions, sleep, and stress
Clinician’s Perspective:
From a clinical standpoint, ectopic fat is not merely a radiologic or biochemical observation—it is a central driver of cardiometabolic disease progression. Increasingly, we encounter patients with relatively normal body weight but clear metabolic dysfunction, underscoring that fat distribution and organ infiltration are more clinically relevant than BMI alone (Han et al., 2026). This paradigm shift has practical implications: risk stratification must extend beyond anthropometry to include triglycerides, liver enzymes, fasting insulin, and waist circumference as surrogate markers of ectopic fat burden.
The therapeutic cornerstone is no longer debated. High-quality evidence demonstrates that combined dietary and exercise interventions produce superior reductions in hepatic, visceral, and intramuscular fat compared with either modality alone (Kazeminasab et al., 2025; Hosseini et al., 2025). In practice, this translates into structured programs integrating moderate caloric restriction with both aerobic and resistance training, sustained for at least 12 weeks to achieve clinically meaningful improvements. Importantly, patients should be counseled that metabolic benefits often precede visible weight loss, a concept that improves adherence and reduces early dropout.
Intermittent fasting may be considered as an adjunct in selected patients, particularly those with insulin resistance, as it enhances fat oxidation and improves glycemic control when combined with exercise (Khalafi et al., 2024). However, individualized assessment is essential, especially in patients with diabetes on pharmacotherapy, where hypoglycemia risk must be addressed.
A key mechanistic insight guiding treatment is the lipid spillover model, wherein adipose tissue dysfunction leads to ectopic lipid deposition in non-adipose organs, driving insulin resistance and systemic inflammation (Khanna et al., 2026). This reinforces the need for early, aggressive lifestyle intervention rather than delayed pharmacologic escalation.
In routine care, setting measurable targets—such as reductions in triglycerides and alanine aminotransferase—provides tangible feedback and aligns patient expectations with physiological progress. Ultimately, managing ectopic fat is less about weight loss per se and more about restoring metabolic flexibility and organ health through sustained lifestyle therapy.
The New Science: Four Studies That Reframe Everything
Over the past two years, a wave of high-quality meta-analyses has delivered some of the clearest guidance we've ever had on how to reduce ectopic fat. Let's break each one down in plain language — and then look at what they all say together.
Study 1: The Landmark Comparison — Exercise Alone vs. Diet + Exercise
Kazeminasab et al. (2025) | Journal of the International Society of Sports Nutrition
This systematic review and meta-analysis is the most direct answer science has produced to the question: does combining diet and exercise work better than exercise alone for reducing organ fat?
The answer is an unambiguous yes.
Researchers pooled data from multiple randomized controlled trials in adults with overweight and obesity. They found that combined exercise training and dietary interventions produced significantly greater reductions in hepatic fat (fatty liver), visceral adipose tissue, and intramuscular fat compared to exercise training alone (Kazeminasab et al., 2025). Critically, meta-regression analysis revealed that programs lasting 12 weeks or longer delivered progressively greater benefits — underlining that consistency and duration are not just helpful, they are the active therapeutic ingredient.
The mechanism behind this synergy is elegant: dietary restriction reduces the influx of calories and shifts the hormonal environment toward fat mobilization (by lowering insulin and suppressing hepatic fat production), while exercise increases energy expenditure, builds mitochondria — the cellular "furnaces" that burn fat — and improves the muscle's sensitivity to insulin. Together, they don't simply add up; they amplify each other.
Study 2: Lipid Profiles as a Window Into Organ Fat
Khalafi et al. (2023) | Nutrition, Metabolism and Cardiovascular Diseases
Ectopic fat is invisible, but its footprints are visible in your bloodwork. This comprehensive meta-analysis examined how exercise alone, diet alone, and their combination affect lipid profiles — total cholesterol, LDL ("bad") cholesterol, HDL ("good") cholesterol, and triglycerides — in adults with overweight and obesity.
The combined intervention won on virtually every measure. It produced the greatest reductions in total cholesterol and LDL-C, the most substantial decrease in triglycerides, and — importantly — maintained or increased protective HDL-C (Khalafi et al., 2023). Why does this matter for ectopic fat? Elevated triglycerides are a direct biomarker of excess hepatic fat production. When the liver is overwhelmed with fat, it releases triglyceride-rich VLDL particles into the bloodstream. When triglycerides fall significantly, it's a reliable signal that the liver is clearing its fat burden.
In other words, your next blood panel isn't just a snapshot of cardiovascular risk — it's a window into your organ fat stores. And the research is detailed that the combined lifestyle approach cleans that window most effectively.
Study 3: Intermittent Fasting + Exercise — A Powerful Pairing
Khalafi et al. (2024) | Nutrition Journal
Intermittent fasting (IF) has attracted enormous popular interest over the past decade, but does the science back up the hype when combined with exercise? This systematic review and meta-analysis found a compelling answer.
The combination of IF and exercise produced greater reductions in total body fat and fat mass than either approach alone, while crucially preserving lean muscle mass — a critical outcome that separates this combination from basic caloric restriction (Khalafi et al., 2024). Beyond body composition, the pairing also substantially improved insulin sensitivity, fasting glucose, and blood pressure — a full cardiometabolic benefit package.
The biological logic is sound: intermittent fasting shifts the body's metabolic state toward fat oxidation during the fasting window, enhances autophagy (cellular cleanup), and sensitizes tissues to insulin. Exercise then amplifies energy expenditure and channels that metabolic momentum toward ectopic fat stores. The result is a one-two punch that targets organ fat from two complementary directions.
Study 4: Ectopic Fat in Chronic Disease — The Lipid Spillover Theory
Khanna, Nerlekar & Bhat (2026) | Journal of the American College of Cardiology: Basic to Translational Science | Hosseini et al. (2025) | Current Developments in Nutrition
The most recent research introduces the concept of lipid spillover as the unifying mechanism behind ectopic fat pathology (Khanna et al., 2026). When adipose tissue — our normal fat storage system — becomes overwhelmed and dysfunctional (a condition called adipose tissue failure), excess lipids "spill over" into organs that are not equipped to handle them. This lipid overflow into the liver, heart, pancreas, and muscle is the biological root cause of the metabolic syndrome cluster: fatty liver, insulin resistance, dyslipidemia, and cardiovascular disease.
Hosseini et al. (2025) extended this understanding further with a meta-analysis examining populations both with and without chronic disease, confirming that the combined diet-plus-exercise approach reduces ectopic fat across diverse clinical contexts, including in individuals already managing conditions like type 2 diabetes and metabolic syndrome. This finding is important because it means the evidence-based strategy doesn't just work for healthy adults trying to prevent disease — it works for those already living with chronic illness.
Why the Combination Is More Than the Sum of Its Parts
The concept of synergy is central to understanding why diet plus exercise outperforms either alone. Each intervention targets different — but complementary — biochemical pathways:
Dietary intervention (whether caloric restriction, Mediterranean-style eating, or intermittent fasting):
Reduces caloric surplus and liver fat production
Lowers circulating insulin, unlocking fat stores
Shifts metabolic hormones toward fat mobilization
Slows lipid spillover into organs
Exercise training (aerobic and resistance combined):
Builds mitochondrial capacity to burn mobilized fat
Increases skeletal muscle's glucose uptake independently of insulin
Elevates basal metabolic rate through muscle preservation
Directly reduces intramuscular and visceral fat
Improves cardiac function and reduces epicardial fat
When both are active simultaneously, the body experiences what researchers describe as dual metabolic pressure: demand for fat as fuel is high (exercise) and supply of new dietary fat is controlled (diet). The ectopic fat stored in organs becomes a prime energy source because it is metabolically active and readily mobilized. The result is faster, deeper, and more durable organ fat reduction than either strategy could achieve alone.
Diet vs Exercise vs Combination: Key Outcomes
1. Diet Alone
Liver fat reduction: Moderate
Insulin sensitivity: Moderate improvement
Muscle preservation: ❌ Risk of muscle loss (especially with aggressive caloric restriction)
2. Exercise Alone
Liver fat reduction: Moderate
Insulin sensitivity: High improvement
Muscle preservation: ✅ Preserved (particularly with resistance training)
3. Combined (Diet + Exercise) — Best Strategy
Liver fat reduction: High (most effective approach)
Insulin sensitivity: Highest improvement
Muscle preservation: ✅ Optimal (fat loss with lean mass retention/improvement)
Clinical Takeaway
Diet reduces fat input and hepatic fat production
Exercise increases fat oxidation and insulin sensitivity
Combination creates metabolic synergy → superior ectopic fat reduction
Practical Application: What This Means for Your Daily Life
The science is compelling — but the real question is how to translate it into a sustainable, liveable routine. Here is a practical, evidence-based framework built on the four studies reviewed above.
Exercise Blueprint
Aerobic Training (Fat Burning Engine)
Target: 150–300 minutes per week of moderate intensity (brisk walking, cycling, swimming, dancing)
OR 75–150 minutes per week of vigorous intensity (jogging, HIIT, aerobic classes)
Start where you are: even 20–30 minute daily walks have shown measurable reductions in hepatic fat
Resistance Training (Metabolic Preservation)
2–3 sessions per week targeting all major muscle groups (legs, back, chest, shoulders, core)
Progressive overload: gradually increase weight, reps, or resistance over weeks
This is non-negotiable — muscle is your body's primary metabolic engine, and protecting it protects your insulin sensitivity
Practical tip: You don't need a gym. Bodyweight squats, lunges, push-ups, and resistance bands at home deliver the resistance training signal your muscles need.
Dietary Blueprint
Caloric Approach
Create a modest deficit of 300–500 calories per day through a combination of reduced intake and increased activity
Avoid extreme restriction — it accelerates muscle loss and slows metabolism
Macronutrient Priorities
Protein: 1.6–2.2 g per kg of body weight daily (preserves muscle, increases satiety)
Carbohydrates: favour whole grains, legumes, and vegetables over refined sugars and ultra-processed foods
Fats: emphasize omega-3-rich sources (oily fish, walnuts, flaxseed) and minimise saturated and trans fats
Intermittent Fasting (Optional but Powerful)
The 16:8 method (eating within an 8-hour window, fasting for 16 hours) integrates naturally with exercise
The 5:2 method (normal eating 5 days, 500–600 calories on 2 non-consecutive days) suits those who prefer flexibility
Key: ensure protein intake remains adequate on fasting days to protect muscle mass
Food-first strategy: Focus on adding nutrient-dense foods before you restrict. Fill half your plate with vegetables, a quarter with quality protein, a quarter with complex carbohydrates. This crowding-out approach is sustainable and reduces dietary fat without deprivation.
Monitoring Your Internal Progress
Because ectopic fat is not visible, clinical progress must be assessed using metabolic and biochemical markers—not just body weight. These indicators provide a reliable window into changes in organ fat, insulin sensitivity, and overall cardiometabolic health.
Key Biomarkers to Track
Triglycerides
Reflect hepatic fat production and lipid overflow
Target: ↓ Decrease
Fasting Insulin / HOMA-IR
Indicates degree of Insulin Resistance
Target: ↓ Decrease
LDL Cholesterol
Marker of atherogenic lipid burden and Cardiovascular Disease risk
Target: ↓ Decrease
HDL Cholesterol
Reflects protective lipid transport and vascular health
Target: ↑ Increase
ALT / AST (Liver Enzymes)
Surrogate markers of liver fat accumulation and hepatocellular injury (relevant to Non-Alcoholic Fatty Liver Disease)
Target: ↓ Decrease
Waist Circumference
Practical proxy for visceral adiposity
Target: ↓ Decrease
Fasting Glucose
Indicator of glycemic control and metabolic function
Target: ↓ Decrease
Clinical Timeline
Patients should be advised to request these markers during routine evaluation. With a consistent combined diet and exercise program, clinically meaningful improvements are typically observed within 8–12 weeks (Khalafi et al., 2023).
Timeline Expectations
Weeks 1–2: Improved energy, better sleep, reduced bloating
Weeks 3–4: Exercise tolerance improves; appetite begins to regulate
Weeks 4–8: Measurable changes in body composition and waist circumference
Weeks 8–12: Significant improvements in blood lipids, fasting glucose, and insulin sensitivity; hepatic fat reductions of 20–40% possible (Kazeminasab et al., 2025)
Beyond 12 weeks: Progressive, compounding metabolic benefit; ectopic fat continues to clear
Frequently Asked Questions
Q1. Can ectopic fat reduction happen even if I don't lose much weight on the scale?
Yes — and this is one of the most important findings in this field. Exercise training can reduce hepatic fat and visceral fat even with minimal overall weight loss, because exercise improves how the body partitions nutrients and enhances fat oxidation at the cellular level. However, adding dietary intervention produces significantly greater ectopic fat reduction alongside greater weight loss than exercise alone (Kazeminasab et al., 2025). The internal metabolic improvements often outpace what is visible externally.
Q2. Is intermittent fasting safe to combine with exercise?
For most healthy adults, yes. Khalafi et al. (2024) found that the combination of IF and exercise was both effective and well-tolerated, producing superior body composition outcomes compared to either alone. However, individuals with diabetes, a history of disordered eating, or chronic illness should consult their physician before starting IF, as fasting may require medication adjustments and close monitoring.
Q3. How much of my ectopic fat is driven by genetics versus lifestyle?
Both contribute, but lifestyle plays a dominant and modifiable role. The lipid spillover model (Khanna et al., 2026) demonstrates that even genetically predisposed individuals who develop adipose tissue dysfunction can reverse or mitigate ectopic fat accumulation through sustained dietary and exercise interventions. Genetics set the stage; lifestyle writes the script.
Q4. I'm not obese — do I still need to worry about ectopic fat?
Absolutely. The study by Han et al. (2026) found significant ectopic fat accumulation and insulin resistance in non-obese individuals with type 2 diabetes. Ectopic fat is a quality-of-fat-storage problem, not exclusively a quantity-of-weight problem. Lean individuals with sedentary lifestyles, high refined carbohydrate intake, or a family history of metabolic disease may carry dangerous ectopic fat despite a normal BMI — sometimes referred to as "metabolically obese, normal weight" (MONW) or TOFI (Thin Outside, Fat Inside).
Q5. What if I can only do diet OR exercise right now — which should I prioritize?
Both are beneficial — doing one is far better than doing neither. If forced to choose: dietary modification typically produces more rapid fat loss and hepatic fat reduction, while exercise provides unique benefits that diet alone cannot replicate, including improved cardiovascular fitness, muscle preservation, and direct effects on intramuscular fat. The evidence consistently shows, however, that adding the second component within 4–8 weeks delivers synergistic benefits that far exceed either alone (Kazeminasab et al., 2025; Hosseini et al., 2025).
Q6. How do I know my liver fat is reducing if I can't see it?
Blood triglycerides and liver enzymes (ALT and AST) are your most accessible indirect markers. Triglyceride reductions strongly correlate with hepatic fat clearance. For direct measurement, a liver ultrasound (widely available and affordable) can detect and grade hepatic steatosis. MRI-based liver fat quantification (MR-PDFF) is the gold standard but typically reserved for clinical research or specialist settings.
Q7. Once I reduce ectopic fat, will it stay reduced?
Only with sustained lifestyle behaviors. Ectopic fat can return if habitual patterns revert. The transition from an aggressive fat-loss phase to a sustainable maintenance phase is critical: continue regular exercise (even at reduced volume), maintain improved dietary patterns, and monitor key biomarkers periodically. Building these behaviors into your identity — not viewing them as temporary "interventions" — is the most reliable predictor of durable success. Even modest ongoing physical activity appears to meaningfully prevent ectopic fat reaccumulation.
Clinical Pearls: The Scientific Strategy for Ectopic Fat Reduction
1. Weight Is Not the Whole Story
Clinician perspective:
Ectopic fat deposition—particularly in the liver and muscle—can drive Insulin Resistance even in individuals with normal BMI. Reliance on weight alone risks underdiagnosis of metabolically unhealthy patients.
You can look “fit” but still have harmful fat inside your organs. Focus on waist size, blood tests, and fitness, not just the scale.
2. Triglycerides Reflect Liver Fat
Clinician perspective:
Elevated triglycerides are a surrogate marker of hepatic fat overproduction and are closely linked to Non-Alcoholic Fatty Liver Disease.
If your triglycerides are high, your liver may be storing excess fat—even if you feel fine. Lowering them improves internal health.
3. Exercise Has Independent Metabolic Effects
Clinician perspective:
Exercise improves insulin sensitivity via insulin-independent glucose uptake, even without significant weight loss.
You don’t need to lose weight to benefit—exercise improves your metabolism from day one.
4. Diet + Exercise Creates Synergy
Clinician perspective:
Combined interventions reduce ectopic fat more effectively than either alone by targeting both fat input and fat oxidation pathways.
Diet helps reduce the amount of fat coming in, and exercise helps burn it. Doing both together yields faster, better results.
5. Early Biomarker Changes Precede Visible Results
Clinician perspective:
Reductions in fasting insulin, triglycerides, and ALT often occur within weeks, preceding anthropometric changes.
Your body starts improving on the inside before you see it outside—stay consistent even if the scale doesn’t move initially.
6. Muscle Preservation Is Metabolic Protection
Clinician perspective:
Loss of lean mass during caloric restriction worsens metabolic outcomes and reduces long-term insulin sensitivity.
Don’t just “lose weight”—protect your muscle with protein and strength training to keep your metabolism strong.
Author’s Note
Ectopic fat represents one of the most under-recognized yet clinically significant drivers of modern metabolic disease. In daily practice, I frequently encounter patients whose standard metrics—body weight or BMI—fail to reflect the severity of their underlying metabolic dysfunction. This disconnect reinforces an important truth: metabolic health cannot be assessed by appearance alone. The silent accumulation of fat within vital organs such as the liver, heart, and pancreas often precedes overt disease by years, if not decades. In clinical practice, patients often show significant reductions in triglycerides and liver enzymes within 8–12 weeks of combined lifestyle intervention—even before major weight loss occurs. This highlights that metabolic health improves earlier than body weight changes.
This article was written with a dual purpose. First, to translate complex, evolving scientific evidence into a form that is both clinically meaningful and practically actionable. Second, to emphasize that the most powerful interventions we currently possess—targeted nutrition and structured exercise—remain underutilized despite overwhelming evidence supporting their efficacy. The convergence of recent meta-analyses provides a level of clarity rarely seen in lifestyle medicine: combined dietary and exercise strategies are not optional enhancements, but foundational therapies for reversing ectopic fat and restoring metabolic health.
It is equally important to acknowledge that sustainable change is rarely immediate. Patients and readers should understand that improvements in biomarkers, energy levels, and metabolic flexibility often precede visible physical transformation. Recognizing and valuing these early internal changes is critical for long-term adherence and success.
Bottom Line
Ectopic fat drives metabolic disease—even in non-obese individuals
It accumulates in liver, muscle, heart, and pancreas
Diet + exercise is the most effective intervention
Improvements occur within 8–12 weeks
Blood markers reflect internal fat reduction
Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making significant changes to your diet, exercise routine, or health regimen, particularly if you have a pre-existing medical condition.
Related Articles
Movement Snacks: How VILPA Delivers Max Health Benefits in Minutes | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
How Insulin Resistance Accelerates Cardiovascular Aging | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
Lowering Cholesterol with Food: 4 Phases of Dietary Dyslipidemia Treatment | DR T S DIDWAL
Breakthrough Research: Leptin Reduction is Required for Sustained Weight Loss | DR T S DIDWAL
References
Han, Q., Xue, M., Li, F., et al. (2026). Ectopic fat distribution and its correlation with insulin resistance indices in non-obese individuals with type 2 diabetes. Acta Diabetologica, 63, 589–599. https://doi.org/10.1007/s00592-025-02632-x
Hosseini, S., Gholami, F., Rahimi, M., et al. (2025). The impact of exercise training plus dietary interventions on ectopic fat in overweight/obese population with and without chronic disease: A systematic review, meta-analysis, and meta-regression of randomized clinical trials. Current Developments in Nutrition, 9(4), 104574. https://doi.org/10.1016/j.cdnut.2025.104574
Kazeminasab, F., Mohebinejad, M., Mahboobi, M. H., Nojoumi, M., Belyani, S., Bagheri, R., & Dutheil, F. (2025). Combined exercise training and dietary interventions versus independent effect of exercise on ectopic fat in individuals with overweight and obesity: A systematic review, meta-analysis, and meta-regression. Journal of the International Society of Sports Nutrition, 22(1), 2528534. https://doi.org/10.1080/15502783.2025.2528534
Khalafi, M., Sakhaei, M. H., Kazeminasab, F., Rosenkranz, S. K., & Symonds, M. E. (2023). Exercise training, dietary intervention, or combined interventions and their effects on lipid profiles in adults with overweight and obesity: A systematic review and meta-analysis of randomized clinical trials. Nutrition, Metabolism and Cardiovascular Diseases, 33(9), 1662–1683. https://doi.org/10.1016/j.numecd.2023.05.024
Khalafi, M., Symonds, M. E., Maleki, A. H., Sakhaei, M. H., Ehsanifar, M., & Rosenkranz, S. K. (2024). Combined versus independent effects of exercise training and intermittent fasting on body composition and cardiometabolic health in adults: A systematic review and meta-analysis. Nutrition Journal, 23(1), 7. https://doi.org/10.1186/s12937-023-00909-x
Khanna, S., Nerlekar, N., & Bhat, A. (2026). Rethinking obesity through the lens of lipid spillover. Journal of the American College of Cardiology: Basic to Translational Science, 11(4). https://doi.org/10.1016/j.jacbts.2026.101532