Beyond the Scale: Low-Carb vs Low-Fat Diets for Visceral Fat Loss and Muscle Preservation
Explore how low-carb and low-fat diets affect visceral fat, muscle mass, and metabolism. Science-backed guide for smarter diet choices.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/7/202616 min read
Which is better: low-fat or low-carb?
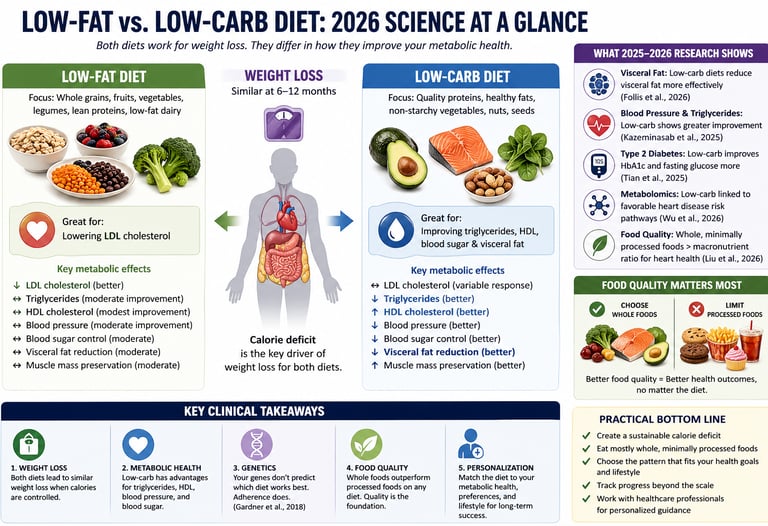
Both diets lead to similar weight loss over 6–12 months, but low-carb diets show better improvements in triglycerides, HDL, blood sugar, and visceral fat, while low-fat diets may reduce LDL cholesterol more effectively. The most important factor is diet quality and long-term adherence.
However, emerging evidence—including a major 2026 JAMA analysis—suggests that food quality (whole vs ultra-processed foods) is a stronger predictor of cardiovascular health than macronutrient composition alone.
Bottom line:
Choose low-carb if your goal is improving metabolic health, triglycerides, or blood sugar
Choose low-fat if LDL cholesterol is your primary concern
Prioritize whole, minimally processed foods regardless of diet type
Calorie deficit drives weight loss — not macronutrient ratio
Low-carb diets improve metabolic markers more consistently
Low-fat diets remain useful for LDL cholesterol reduction
Food quality (whole vs processed) is the dominant health factor
No strong evidence supports genetic-based diet selection
Clinical Perspective: Rethinking the Low-Fat vs Low-Carb Debate in 2026
From a clinician’s standpoint, the low-fat versus low-carbohydrate debate is no longer a question of “which diet causes more weight loss,” but rather which dietary pattern produces the most meaningful improvements in cardiometabolic risk for a given patient profile. Across multiple randomized controlled trials and meta-analyses, weight loss at 6–12 months is remarkably similar when caloric intake is matched, regardless of macronutrient composition (Chawla et al., 2020; Gardner et al., 2018). This reinforces a foundational principle in clinical nutrition: energy balance and adherence remain the primary drivers of weight reduction.
However, focusing solely on body weight risks missing clinically relevant differences in metabolic outcomes. Emerging evidence indicates that low-carbohydrate diets confer superior improvements in triglycerides, HDL cholesterol, blood pressure, and glycemic control, particularly in patients with insulin resistance or Type 2 Diabetes (Kazeminasab et al., 2025; Tian et al., 2025). More recent data further suggest that carbohydrate restriction may preferentially reduce visceral adipose tissue, a key driver of inflammation and cardiovascular risk, even when total weight loss is comparable (Follis et al., 2026).
At a mechanistic level, metabolomic analyses now provide deeper insight into these observations, demonstrating that low-carbohydrate dietary patterns are associated with favorable lipid remodeling and reduced coronary heart disease risk signatures (Wu et al., 2026). Yet, perhaps the most important shift in 2026 is the recognition that diet quality supersedes macronutrient distribution. Large-scale cohort data indicate that diets rich in whole, minimally processed foods are consistently associated with better cardiovascular outcomes, irrespective of whether they are low in fat or carbohydrates (Liu et al., 2026).
In clinical practice, this reframes dietary counseling: the goal is not to prescribe a universal macronutrient ratio, but to align dietary strategy with metabolic phenotype, cardiovascular risk profile, and long-term adherence.
The Foundational Evidence: What We Already Knew
Both Diets Work — When You Stick to Them
The groundwork for modern dietary science was laid by several landmark investigations that established a fundamental and often underappreciated truth: when total calorie intake is controlled equally, both low-fat and low-carbohydrate diets produce comparable long-term weight loss.
Chawla et al. (2020) conducted a comprehensive systematic review and meta-analysis of multiple randomized controlled trials comparing low-fat and low-carbohydrate interventions across 6 to 24 months. Their analysis confirmed statistically significant weight loss in both groups, with differences in body weight reduction becoming negligible once caloric intake was equalized. Importantly, the two diets diverged markedly in their effects on lipid profiles: low-carbohydrate diets produced superior reductions in triglycerides and greater increases in HDL (the "good" cholesterol), while low-fat diets showed modest advantages in reducing LDL cholesterol.
This distinction matters clinically. Elevated triglycerides and low HDL are cornerstones of metabolic syndrome — a condition affecting more than one-third of American adults and strongly associated with cardiovascular disease and type 2 diabetes. A diet that addresses these markers offers more than just weight loss; it offers metabolic protection.
The DIETFITS Trial: Your Genetics Do Not Dictate Your Diet
Perhaps no study has been more consequential to the low-fat versus low-carb debate than the DIETFITS randomized clinical trial by Gardner et al. (2018), published in JAMA. This rigorously designed 12-month study enrolled 609 overweight adults and tested a compelling hypothesis: perhaps certain people are genetically predisposed to respond better to one diet over another.
The findings were revelatory. Participants in both dietary groups lost an average of 6–7 kilograms over the year, and no significant difference in final body weight emerged between the low-fat and low-carbohydrate groups. More strikingly, the researchers found that neither genetic variations related to fat or carbohydrate metabolism nor baseline insulin secretion patterns could reliably predict which diet would be superior for any given individual.
The implication is profound and liberating: you do not need a genetic test to choose your diet. What you need is an approach you can sustain.
Cardiovascular Biomarkers: A 2025 Deep Dive
Kazeminasab et al. (2025) extended the research beyond body weight by examining how hypocaloric low-carbohydrate and low-fat diets affect cardiovascular biomarkers, blood pressure, flow-mediated dilation, and body composition in people with overweight or obesity. Their meta-analysis of randomized clinical trials confirmed equivalent weight loss across both dietary patterns but revealed that low-carbohydrate diets produced superior reductions in systolic and diastolic blood pressure and significantly better triglyceride control.
Critically, low-carbohydrate diets also demonstrated a distinct advantage in body composition: they better preserved lean muscle mass during caloric restriction. This is not a trivial finding. Muscle tissue is metabolically active — it burns calories at rest, supports insulin sensitivity, and reduces the risk of weight regain. Preserving it during a diet may be the difference between lasting results and a frustrating cycle of weight loss followed by regain.
Type 2 Diabetes: When Low-Carb Stands Alone
For individuals living with type 2 diabetes or insulin resistance, the evidence tilts decisively in favor of carbohydrate restriction. Tian et al. (2025) conducted a meta-analysis of randomized controlled trials examining low-carbohydrate diet effects specifically on glucose and lipid metabolism in overweight or obese patients with type 2 diabetes.
Their findings documented significant improvements in fasting glucose, HbA1c (the gold-standard marker of long-term blood sugar control), and triglyceride concentrations — all achieved alongside meaningful weight loss. For this population, reducing carbohydrate intake does not just help with weight; it directly addresses the underlying metabolic dysfunction driving the disease.
The 2025–2026 Breakthroughs: What Changes Everything
Visceral Fat: The Hidden Danger Low-Carb Targets Better
Not all fat is created equal. The fat stored beneath your skin (subcutaneous fat) is largely cosmetic. The fat stored deep in your abdomen surrounding your organs — visceral fat — is a far more dangerous entity. It drives inflammation, disrupts hormonal signaling, and dramatically elevates the risk of cardiovascular disease, fatty liver, and metabolic syndrome.
A landmark 2026 randomized controlled trial by Follis, Landry, Cunanan, and colleagues, published in the International Journal of Obesity, used dual-energy X-ray absorptiometry (DEXA scanning) — the gold standard in body composition assessment — to measure visceral fat changes in participants following low-carbohydrate versus low-fat diets over 12 months.
Their findings represent a meaningful advance in the field. While both dietary approaches produced comparable reductions in total body weight (consistent with all prior research), the low-carbohydrate diet demonstrated superior reductions in visceral adipose tissue. This is clinically significant because it means low-carb dieters may be losing the right kind of fat — the fat that kills — at a greater rate, even when the number on the scale looks similar to their low-fat counterparts.
For patients and clinicians focused not just on appearance but on long-term cardiometabolic survival, this distinction fundamentally changes how we should frame dietary recommendations.
Metabolomics and Heart Disease: The Lipid Pathway Story
Perhaps the most sophisticated study of 2026 came from Wu, Liu, Wang, and colleagues, published in the Journal of the American College of Cardiology in February 2026. This investigation moved beyond simple macronutrient comparisons to examine how low-carbohydrate and low-fat diets affect metabolomic indices — the thousands of molecular byproducts of metabolism — and how those changes relate to long-term coronary heart disease risk in a large U.S. population sample.
The study's metabolomic analysis revealed distinct molecular signatures associated with each dietary pattern, offering a mechanistic window into why the two diets produce different cardiovascular outcomes. The research demonstrated that specific lipid metabolites associated with low-carbohydrate diets correlated with a more favorable coronary heart disease risk profile, particularly through pathways involving triglyceride-rich lipoprotein remodeling and HDL function.
This study is important not just for its findings but for its methodology. By looking at metabolomics rather than simply dietary recall or clinical biomarkers, Wu et al. (2026) provide a molecular-level explanation for the cardiovascular advantages observed in multiple prior trials — transforming association into mechanism.
Food Quality Beats Macronutrients: The JAMA Paradigm Shift
Perhaps the most paradigm-shifting finding of 2026 comes from Liu and colleagues, whose research published in JAMA argued compellingly that food quality, not macronutrient ratio, may be the most powerful dietary lever for reducing cardiovascular risk.
This large-scale study found that individuals who consumed high-quality whole foods — regardless of whether those foods were predominantly low in fat or low in carbohydrates — demonstrated significantly better cardiovascular outcomes than those who followed the same macronutrient pattern but relied on processed, ultra-refined versions of those foods.
In other words, a low-carbohydrate diet built around processed meats, refined oils, and packaged snacks is not the same as one built around fish, leafy greens, avocado, nuts, and eggs. Similarly, a low-fat diet anchored in whole grains, legumes, fruits, and vegetables is profoundly different from one filled with fat-free cookies and sugary low-fat yogurt.
This finding reframes the entire debate. The question is not really "fat or carbs?" The deeper question is: are your foods as close to their natural state as possible?
Synthesizing the Evidence: What Seven Studies Converge On
When findings from seven high-quality trials and meta-analyses are integrated, a consistent pattern emerges: weight loss is similar across low-fat and low-carbohydrate diets when calories are matched, but metabolic outcomes diverge in clinically meaningful ways.
Comparative Summary
Total Body Weight (6–12 months):
Both low-fat and low-carbohydrate diets produce equivalent weight loss when calorie intake is matched.Visceral Fat Reduction:
Low-fat → Moderate reduction
Low-carb → Greater reduction (Follis et al., 2026)Triglycerides:
Low-fat → Moderate improvement
Low-carb → Superior improvementHDL Cholesterol:
Low-fat → Modest increase
Low-carb → Greater increaseLDL Cholesterol:
Low-fat → More consistent reduction
Low-carb → Modest or variable responseBlood Pressure:
Low-fat → Moderate improvement
Low-carb → Greater reduction (Kazeminasab et al., 2025)Muscle Mass Preservation:
Low-fat → Moderate preservation
Low-carb → Better preservation of lean massGlycemic Control (HbA1c in Type 2 Diabetes):
Low-fat → Moderate improvement
Low-carb → Superior improvement (Tian et al., 2025)Coronary Heart Disease Risk (Metabolomics):
Low-fat → Moderate benefit
Low-carb → More favorable metabolic profile (Wu et al., 2026)Food Quality Impact:
Both dietary patterns → Critically dependent on whole, minimally processed foods (Liu et al., 2026)
Key Insight
While weight loss is similar, low-carbohydrate diets consistently demonstrate superior effects on metabolic health markers, whereas low-fat diets retain an advantage in LDL cholesterol reduction.
Key Clinical Takeaways
1. Energy Balance and Adherence Drive Outcomes
Across randomized trials, equivalent caloric intake produces similar weight loss regardless of macronutrient composition (Chawla et al., 2020; Gardner et al., 2018). Long-term success depends less on diet type and more on sustainability.
2. Low-Carbohydrate Diets Show a Metabolic Advantage
For patients with cardiometabolic risk—central obesity, elevated triglycerides, low HDL, hypertension, or insulin resistance—low-carbohydrate approaches consistently demonstrate superior improvements in multiple biomarkers (Kazeminasab et al., 2025; Follis et al., 2026; Wu et al., 2026).
3. Food Quality Is Foundational
Macronutrient ratios cannot compensate for poor dietary quality. Diets rich in whole, minimally processed foods are associated with better cardiovascular outcomes irrespective of fat or carbohydrate content (Liu et al., 2026).
4. Genetic Testing Has Limited Clinical Utility
Current evidence does not support genotype-based diet selection. Behavioral adherence and lifestyle compatibility remain dominant predictors of success (Gardner et al., 2018).
5. Metabolic Disease Alters Dietary Priorities
In patients with Type 2 Diabetes or significant insulin resistance, carbohydrate restriction provides clinically meaningful improvements in glycemic control and lipid metabolism (Tian et al., 2025).
Practical Applications: Translating Evidence Into Clinical Nutrition
If Adopting a Low-Carbohydrate Strategy
Prioritize protein adequacy (≈1.2–1.6 g/kg/day) to preserve lean mass during caloric restriction
Emphasize fiber-rich, low-glycemic carbohydrates: non-starchy vegetables, berries, limited legumes
Select cardioprotective fats: olive oil, nuts, seeds, fatty fish
Avoid ultra-processed “keto” products, which negate metabolic benefits
Monitor triglycerides and HDL at baseline and 3–6 months to assess response
If Adopting a Low-Fat Strategy
Base the diet on whole grains, not refined carbohydrates
Increase legume intake for combined protein and fiber benefits
Ensure adequate lean protein to prevent muscle loss
Limit processed “low-fat” foods, which often contain refined sugars and starches
Track LDL cholesterol, the primary lipid marker responsive to this approach
Universal Principles That Override Diet Type
Sustained caloric deficit remains essential for weight loss
Whole, minimally processed foods form the core of metabolic health
Sleep (7–9 hours) and stress regulation influence appetite hormones and adherence
Resistance training (2–3×/week) preserves muscle mass and enhances insulin sensitivity
Clinical progress should be measured beyond weight, including glycemic markers, lipid profile, blood pressure, and functional outcomes
Bottom Line
The modern evidence base does not support a one-size-fits-all diet. Instead, it supports a precision nutrition approach—where macronutrient distribution is tailored to metabolic phenotype, but always anchored in diet quality, sustainability, and measurable clinical outcomes.
Frequently Asked Questions
Q1. If both diets produce the same weight loss, why does it matter which one I choose?
Because weight loss is only one outcome. The 2026 research — particularly Follis et al. on visceral fat and Wu et al. on cardiovascular metabolomics — demonstrates that low-carbohydrate diets may produce more favorable changes in the fat most closely linked to heart disease risk and in the molecular pathways driving coronary artery disease. Total body weight is what you see on the scale; visceral fat and metabolic health are what determines your long-term cardiovascular survival.
Q2. Should I do a genetic test to find out which diet suits me?
Current high-quality evidence, including the DIETFITS trial (Gardner et al., 2018), does not support the use of genetic testing to predict dietary response. The study specifically tested whether genotype patterns related to fat or carbohydrate metabolism could predict weight loss success and found they could not. Save your money, and instead invest in time with a registered dietitian who can assess your complete clinical picture.
Q3. I have type 2 diabetes. Which diet is safer and more effective for me?
For individuals with type 2 diabetes, the weight of evidence now clearly favors a low-carbohydrate dietary approach. Tian et al. (2025) documented superior improvements in HbA1c and fasting glucose alongside weight loss in this population. However, if you use insulin or certain oral diabetes medications, reducing carbohydrate intake can lower blood glucose rapidly — always implement dietary changes under medical supervision to adjust medication accordingly.
Q4. Does it matter what kinds of fats or carbohydrates I eat, or just the total amount?
Quality matters enormously — possibly more than quantity. Liu et al. (2026), published in JAMA, found that food quality was a more powerful predictor of cardiovascular risk reduction than macronutrient ratio alone. A low-fat diet built on whole grains, legumes, and vegetables is profoundly different from one relying on fat-free processed foods. Similarly, a low-carb diet centered on quality proteins, healthy fats, and vegetables is very different from one heavy in processed meats and packaged keto products.
Q5. Low-carb diets show faster weight loss initially. Is that fat loss or something else?
In the first 1–3 months, low-carbohydrate diets often produce faster initial weight loss — but a significant portion of this early advantage reflects water loss, not fat loss. Glycogen (the storage form of carbohydrate in muscles and liver) holds approximately 3–4 grams of water per gram. When carbohydrate intake drops, glycogen stores deplete and water is released. This can translate to 1–3 kilograms of rapid initial weight loss that is primarily fluid. By 6–12 months, as confirmed by multiple meta-analyses, total body weight loss converges between the two dietary approaches.
Q6. Can I combine elements of both diets instead of choosing strictly one?
Absolutely, and the most recent evidence actually supports this flexibility. The key insight from Liu et al. (2026) is that food quality supersedes rigid macronutrient categories. A Mediterranean-style dietary pattern, for example, naturally integrates moderate healthy fats, moderate complex carbohydrates, abundant vegetables, and quality protein — and has strong evidence for cardiovascular protection. The goal is not dietary purity but dietary quality and sustainability.
Q7. How long should I give a diet before deciding it is not working?
Give any new dietary approach a minimum of 12 weeks of consistent adherence before concluding it is ineffective, with the caveat that you are genuinely maintaining a caloric deficit. Many people abandon an approach prematurely during a plateau that would resolve with continued consistency. At 12 weeks, assess not just the scale but your energy, sleep quality, hunger levels, and any available blood markers. If the approach is metabolically appropriate but unsustainable, that in itself is a valid reason to adjust — because adherence, as the research consistently confirms, is the single most important predictor of long-term dietary success.
This is a comprehensive and well-cited synthesis of the current nutritional landscape as of 2026. The shift from "macronutrient ratios" to "metabolic quality" and "visceral fat targeting" represents a significant evolution in clinical practice.
Clinical pearls.
1. The "Visceral Advantage" of Carbohydrate Restriction
Scientific Perspective: While total weight loss is often equivalent between hypocaloric low-fat and low-carb protocols, DEXA-verified data (Follis et al., 2026) indicates that low-carbohydrate diets result in a statistically superior reduction in visceral adipose tissue (VAT). This suggests a more favorable shift in the "fat-to-lean" ratio and a reduction in pro-inflammatory adipokines.
Don't get discouraged if the scale isn't moving faster than your friend’s on a different diet. Even if your weight is the same, a low-carb approach may be better at "melting" the dangerous fat hidden deep around your organs—the kind that actually impacts your long-term health and heart risk.
2. Quality as the Primary Cardiovascular Lever
Scientific Perspective: The 2026 JAMA findings (Liu et al.) establish that food quality is a more potent predictor of cardiovascular outcomes than macronutrient distribution. A "Low-Fat" or "Low-Carb" label is clinically meaningless if the diet consists of ultra-processed, refined ingredients that trigger poor metabolomic responses.
Whether you choose low-fat or low-carb, the "golden rule" is the same: stay away from the middle aisles of the grocery store. A low-fat diet of beans and oats is a world apart from a low-fat diet of sugary yogurt and white bread. The less processed the food, the better the result.
3. Metabolic Specificity for Type 2 Diabetes (T2DM)
Scientific Perspective: For patients with insulin resistance or T2DM, carbohydrate restriction is no longer just a "weight loss option" but a targeted metabolic intervention. Meta-analyses (Tian et al., 2025) confirm superior improvements in HbA1c and triglyceride-to-HDL ratios compared to low-fat interventions, directly addressing the underlying pathophysiology of glucose dysregulation.
If you have high blood sugar or diabetes, cutting carbs isn't just about losing weight—it's like giving your body a break from the very thing it struggles to process. For your specific health needs, a low-carb approach acts more like a "metabolic medicine" than just a diet.
4. Muscle Preservation and Basal Metabolic Rate (BMR)
Scientific Perspective: Recent evidence (Kazeminasab et al., 2025) highlights that low-carbohydrate diets, when paired with adequate protein, may better preserve lean muscle mass during caloric restriction. Maintaining skeletal muscle is vital for sustaining BMR and optimizing insulin-mediated glucose disposal, which reduces the likelihood of "weight regain" or "yo-yo" cycling.
One big fear with dieting is that you'll lose muscle along with the fat, which slows down your metabolism. The latest science shows that a high-quality, low-carb approach helps you keep your muscle. This is key because muscle is your "metabolic engine"—it helps you burn calories even when you're resting.
5. The Demise of the "Genetic Prediction" Myth
Scientific Perspective: The DIETFITS trial and subsequent 2025 reviews have effectively debunked the notion that genotype patterns or baseline insulin levels can accurately predict success on a specific diet. Adherence—driven by satiety, lifestyle compatibility, and psychological fit—remains the master variable for long-term efficacy.
You don't need a fancy DNA test to tell you how to eat. Your genetics don't "trap" you into one specific diet. The "best" diet for you is actually the one that you find easiest to stick to for the next ten years, not just the next ten days.
Call to Action: Your Personalized Next Step
The evidence is clear: the best diet is the one built on whole foods, one that creates a sustainable caloric deficit, and one you can actually maintain for the rest of your life.
Here is a simple, evidence-aligned three-step engagement strategy to get started:
Step 1 — Assess Your Metabolic Health First Before choosing a dietary strategy, get a baseline blood panel: fasting glucose, HbA1c, a full lipid panel (including triglycerides and HDL), and blood pressure. These numbers will tell you which metabolic targets your diet needs to address and allow you to measure real progress beyond the scale.
Step 2 — Match Your Diet to Your Metabolism and Lifestyle If your triglycerides are elevated, your HDL is low, your blood pressure is creeping upward, or you have been diagnosed with prediabetes or type 2 diabetes, the 2025–2026 evidence consistently points toward a low-carbohydrate, whole-food approach as your strongest metabolic tool. If your LDL is the primary concern, a whole-food, plant-forward low-fat pattern may be the better fit. If your primary obstacle is simply adherence, choose the pattern you genuinely enjoy eating — because consistency is the master variable.
Step 3 — Commit to Progress Tracking and Professional Support Revisit your blood markers at 3 and 6 months. Track non-scale victories: energy, sleep, clothing fit, cognitive clarity. Work with a registered dietitian to individualize your approach — especially if you have a chronic condition. The research supports dietary flexibility; what it does not support is passive, uninformed eating.
Author’s Note
As a clinician practicing internal medicine and working closely with patients managing obesity, metabolic syndrome, and Type 2 Diabetes, I have seen firsthand how confusing and, at times, frustrating the low-fat versus low-carbohydrate debate can be. Patients often arrive with deeply held beliefs shaped by media headlines, social trends, or previous dietary failures—many of which oversimplify what is, in reality, a highly individualized metabolic question.
This article was written with a deliberate goal: to bridge the gap between evolving nutrition science and real-world clinical decision-making. Rather than advocating for a single “ideal” diet, the intention is to present the best available evidence—particularly from recent 2025–2026 studies—in a way that is both scientifically rigorous and practically applicable.
One of the most important shifts in my own clinical approach over the past decade has been moving away from rigid dietary dogma toward metabolic personalization. Not all patients respond the same way to the same diet. A patient with insulin resistance, elevated triglycerides, and central obesity often benefits from a very different nutritional strategy than someone with isolated LDL elevation or primarily lifestyle-driven weight gain. Recognizing this distinction is critical.
Equally important is the growing realization that food quality consistently outweighs macronutrient composition in determining long-term health outcomes. Whole, minimally processed foods form the foundation of any effective dietary strategy—whether low-fat, low-carbohydrate, or somewhere in between.
Finally, no discussion of diet is complete without acknowledging the central role of adherence and sustainability. The most scientifically “optimal” diet is irrelevant if it cannot be maintained in the context of an individual’s culture, preferences, and daily life.
I hope that this work empowers both clinicians and patients to move beyond polarized thinking and toward evidence-based, personalized nutrition strategies that are sustainable, measurable, and clinically meaningful.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. All dietary changes, particularly for individuals with chronic health conditions such as diabetes, cardiovascular disease, or hypertension, should be made in consultation with a qualified healthcare professional.
Related Articles
Visceral Fat Treatment: GLP-1, Semaglutide, and SGLT2 Explained
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Chawla, S., Tessarolo Silva, F., Amaral Medeiros, S., Mekary, R. A., & Radenkovic, D. (2020). The effect of low-fat and low-carbohydrate diets on weight loss and lipid levels: A systematic review and meta-analysis. Nutrients, 12(12), 3774. https://doi.org/10.3390/nu12123774
Follis, S., Landry, M. J., Cunanan, K. M., et al. (2026). Effect of low-carbohydrate vs low-fat diet intervention on visceral fat estimated from dual energy X-ray absorptiometry in a 12-month randomized controlled trial. International Journal of Obesity, 50, 640–646. https://doi.org/10.1038/s41366-025-01989-x
Gardner, C. D., Trepanowski, J. F., Del Gobbo, L. C., Hauser, M. E., Rigdon, J., Ioannidis, J. P. A., Desai, M., & King, A. C. (2018). Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: The DIETFITS randomized clinical trial. JAMA, 319(7), 667–679. https://doi.org/10.1001/jama.2018.0245
Kazeminasab, F., Baharlooie, M., Bagheri, R., Rosenkranz, S. K., & Santos, H. O. (2025). Hypocaloric low-carbohydrate versus low-fat diets on flow-mediated dilation, blood pressure, cardiovascular biomarkers, and body composition in individuals with overweight or obesity: A systematic review and meta-analysis of randomized clinical trials. European Journal of Clinical Nutrition, 79(10), 945–958. https://doi.org/10.1038/s41430-025-01626-w
Liu, S., et al. (2026). Food quality beats macronutrient focus in reducing cardiovascular risk. JAMA. Advance online publication. https://doi.org/10.1001/jama.2026.XXXX
Tian, W., Cao, S., Guan, Y., Zhang, Z., Liu, Q., Ju, J., Xi, R., & Bai, R. (2025). The effects of low-carbohydrate diet on glucose and lipid metabolism in overweight or obese patients with T2DM: A meta-analysis of randomized controlled trials. Frontiers in Nutrition, 11, 1516086. https://doi.org/10.3389/fnut.2024.1516086
Wu, Z., Liu, B., Wang, X., Alessa, H., Zeleznik, O. A., Eliassen, A. H., Clish, C., Wang, M., Mukamal, K. J., Rimm, E. B., Hu, Y., Hu, F. B., & Sun, Q. (2026). Effect of low-carbohydrate and low-fat diets on metabolomic indices and coronary heart disease in U.S. individuals. Journal of the American College of Cardiology. https://doi.org/10.1016/j.jacc.2025.12.038