Aerobic vs Anaerobic Threshold: Differences, Training Zones & Clinical Significance
Learn the difference between aerobic and anaerobic thresholds, how they affect performance, fat metabolism, and how to train smarter using Zone 2 and lactate science.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/13/202617 min read
What is the difference between aerobic and anaerobic threshold?
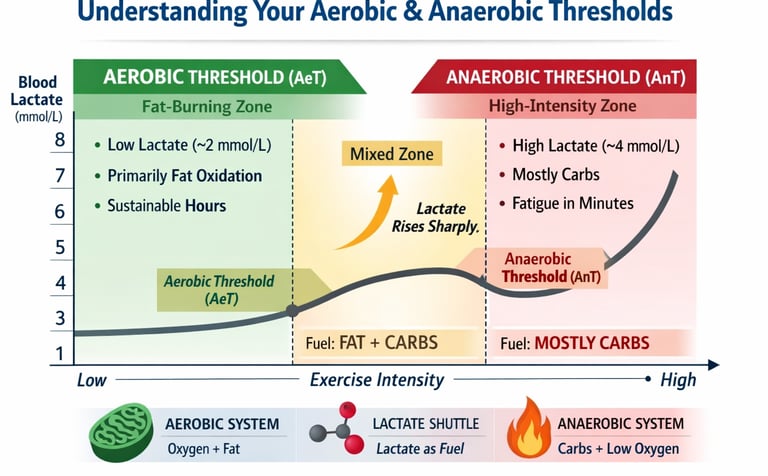
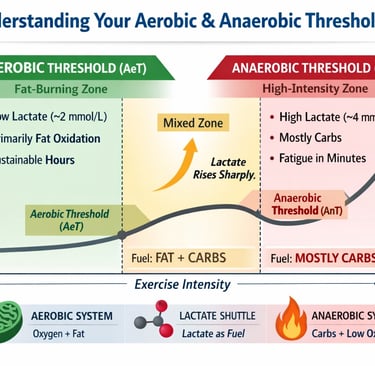
The aerobic threshold (AeT) is the exercise intensity at which lactate begins to rise above baseline (~2 mmol/L), marking the shift from primarily fat metabolism to mixed fuel use. The anaerobic threshold (AnT) is a higher intensity (~4 mmol/L, variable) where lactate accumulates faster than it can be cleared, leading to rapid fatigue.
In simple terms, the aerobic threshold represents sustainable, long-duration effort, while the anaerobic threshold defines the maximum intensity you can maintain for a limited time. Both are key markers of endurance performance, metabolic health, and cardiovascular fitness.
Clinician’s Perspective: Why Thresholds Matter Beyond Performance
Integrated Physiological Marker
Aerobic (AeT) and anaerobic thresholds (AnT) are not isolated metrics—they reflect the combined efficiency of cardiovascular, pulmonary, and skeletal muscle systems. Unlike VO₂ max, which measures peak capacity, thresholds capture functional, sustainable performance, making them more clinically actionable (Patel et al., 2017).Superior Prognostic Value in Chronic Disease
In patients with heart failure and cardiovascular disease, the anaerobic threshold derived from cardiopulmonary exercise testing (CPET) has demonstrated strong prognostic significance—often outperforming VO₂ max in predicting mortality and surgical outcomes (Ryuzaki et al., 2023).Precision Exercise Prescription
Threshold-guided training allows clinicians to prescribe individualized exercise intensity rather than relying on generalized heart rate formulas. This improves:Safety in cardiac rehab
Adherence in deconditioned patients
Efficiency of training adaptations
Metabolic Health & Insulin Resistance
A reduced aerobic threshold is commonly seen in type 2 diabetes, obesity, and metabolic syndrome, reflecting impaired fat oxidation and mitochondrial dysfunction. Targeted Zone 2 training can significantly improve metabolic flexibility and glycemic control.Early Detection of Functional Decline
A downward shift in thresholds may precede overt clinical deterioration, making them valuable for early identification of declining cardiorespiratory fitness, especially in aging populations.Translational Use of Wearables
Emerging technologies now allow non-invasive, real-time estimation of thresholds using ECG and wearable data, potentially transforming outpatient monitoring and long-term disease management (Ryuzaki et al., 2023).
Clinical Bottom Line:
Thresholds are not just performance tools—they are dynamic biomarkers of health, resilience, and disease progression, enabling a more precise and personalized approach to exercise medicine.
AEROBIC vs ANAEROBIC THRESHOLD
What Every Athlete (and Patient) Must Know
Whether you're a competitive marathoner chasing a PR, a weekend cyclist, a cardiac rehab patient, or someone just starting to take fitness seriously, understanding your aerobic and anaerobic thresholds could be the single most important thing you do for your health and performance this year.
Why VO₂ Max Alone Doesn't Tell the Whole Story
Endurance performance—and even long-term metabolic health—is not determined solely by how much oxygen your body can consume, but by how efficiently it can use that oxygen across different exercise intensities. For decades, VO₂ max has been regarded as the gold standard of cardiovascular fitness. Yet, emerging evidence suggests that it tells only part of the story. Two individuals with identical VO₂ max values can exhibit dramatically different performance outcomes, fatigue resistance, and even clinical prognoses (Chamari & Padulo, 2015). The missing link lies in understanding metabolic thresholds—specifically, the aerobic threshold (AeT) and anaerobic threshold (AnT).
These thresholds represent critical physiological tipping points where your body transitions between energy systems, fuel utilization patterns, and fatigue dynamics. The aerobic threshold reflects the upper limit of sustainable, fat-dominant metabolism, while the anaerobic threshold marks the intensity beyond which lactate accumulates rapidly and performance becomes time-limited. Far from being abstract laboratory concepts, these thresholds are now recognized as powerful, integrative markers of whole-body function—encompassing cardiovascular efficiency, mitochondrial capacity, and metabolic flexibility (Patel et al., 2017).
Importantly, their relevance extends well beyond athletic performance. In clinical populations, particularly individuals with cardiovascular disease or metabolic disorders, the anaerobic threshold derived from cardiopulmonary exercise testing (CPET) has demonstrated strong prognostic value, in some cases outperforming VO₂ max as a predictor of survival (Ryuzaki et al., 2023). This shifts the paradigm: thresholds are not just tools for optimizing training—they are vital indicators of physiological resilience and health.
Understanding where these thresholds lie—and how to train them—may be one of the most powerful, evidence-based strategies to improve performance, delay fatigue, and enhance long-term health.
Defining the Two Thresholds
The Aerobic Threshold (AeT) — Your Metabolic Foundation
The aerobic threshold represents the first meaningful shift in your metabolism during exercise. At this point — typically when blood lactate rises above baseline to approximately 2 mmol/L — your body begins to rely more heavily on carbohydrates alongside fat for fuel.
Below the AeT, fat oxidation dominates. Your muscles are working efficiently, oxygen supply meets demand, and lactate is produced and cleared in near-perfect balance. You can sustain this for hours — think of a comfortable long run, a relaxed cycling session, or an easy hike.
In simple terms:
The AeT is where your body's "clean-burning" engine is running optimally — efficient, sustainable, and fat-fuelled.
The Anaerobic Threshold (AnT) / Lactate Threshold 2 (LT2) — Your Performance Ceiling
The anaerobic threshold — also called Lactate Threshold 2 (LT2), the Onset of Blood Lactate Accumulation (OBLA), or the maximal lactate steady state — marks a more dramatic shift. At this intensity, lactate accumulates faster than your body can clear it, typically around 4 mmol/L (though this varies significantly between individuals).
Above the AnT, exercise becomes unsustainable within minutes. Your glycolytic (sugar-burning) energy system dominates, hydrogen ion accumulation rises, muscle fatigue accelerates, and performance degrades rapidly.
In simple terms:
The AnT is your body's "red line." Cross it for too long, and you'll be forced to slow down — or stop.
The Physiology Underneath — What's Actually Happening?
Mitochondria: Your Cellular Power Plants
The aerobic energy system lives inside your mitochondria — specialized organelles in muscle cells that convert oxygen and fuel into ATP (energy). Endurance training stimulates mitochondrial biogenesis (the creation of new mitochondria) and increases capillary density (the number of tiny blood vessels delivering oxygen to muscles). The result: a higher aerobic threshold and better fatigue resistance.
The Lactate Shuttle: A Misunderstood Molecule
Lactate has been unfairly villainized for decades. It is not — as was once believed — simply a waste product that causes muscle soreness. In reality, lactate functions as an important fuel source, shuttled between muscle fibers and organs (including the heart) through what researchers call the lactate shuttle system.
The interplay between slow-twitch (Type I) muscle fibers — highly oxidative and fatigue-resistant — and fast-twitch (Type II) fibers — powerful but fatigue-prone and high lactate producers — determines where both thresholds fall for any given individual.
Ventilatory Thresholds: Your Breathing Tells the Story
Your respiratory system mirrors these metabolic events. The First Ventilatory Threshold (VT1) corresponds roughly to the aerobic threshold, while the Second Ventilatory Threshold (VT2) aligns with the anaerobic threshold. This is why clinicians use cardiopulmonary exercise testing (CPET) to identify metabolic thresholds non-invasively through breath analysis.
Ryuzaki et al. (2023) demonstrated that anaerobic threshold can even be estimated in real time during exercise using electrocardiogram signals in heart failure patients — a finding with exciting implications for remote monitoring and cardiac rehabilitation.
Aerobic vs. Anaerobic Threshold — Key Differences
Aerobic Threshold (AeT)
Blood Lactate: ~2 mmol/L
Primary Fuel: Predominantly fat with some carbohydrate contribution
Sustainability: Can be maintained for hours
Breathing Pattern: Comfortable, conversational (can speak full sentences)
Heart Rate Zone: ~60–75% of maximum heart rate
Training Focus: Builds aerobic base, metabolic efficiency, and endurance
Clinical Relevance: Marker of metabolic health and fat oxidation capacity
Anaerobic Threshold (AnT)
Blood Lactate: ~4 mmol/L (highly individual and variable)
Primary Fuel: Primarily carbohydrate (glycolytic metabolism)
Sustainability: Limited to minutes at high intensity
Breathing Pattern: Heavy, labored (conversation not possible)
Heart Rate Zone: ~80–90% of maximum heart rate
Training Focus: Improves performance ceiling, speed, and race pace tolerance
Clinical Relevance: Strong predictor of cardiovascular fitness and prognosis
How Are Thresholds Measured?
In the Laboratory
The most accurate method is blood lactate profiling — where fingertip blood samples are taken at progressive exercise intensities to construct a lactate curve. The inflection points identify VT1 and VT2. Gas exchange testing (CPET) is the gold standard for clinical settings, analyzing expired gases to pinpoint ventilatory thresholds without invasive blood draws.
Patel et al. (2017) confirmed in their cardiovascular review that aerobic and anaerobic exercise training produce meaningfully different physiological adaptations — underscoring why accurate threshold identification matters for both training and medical prescription.
In the Field
• If you can speak comfortably in full sentences, you're likely below or at AeT. A few words but not a conversation = near AnT.
• While imprecise, heart rate-based zones provide a reasonable approximation. Modern devices estimate thresholds from HRV and power data.
• Running pace at threshold or cycling FTP are widely used proxies, though individual variation is significant.
Why Elite Athletes Are Different — and What You Can Learn
Here's a striking fact: elite endurance athletes don't just have higher VO₂ max values — they sustain a much higher percentage of their VO₂ max at their lactate threshold. A recreational runner might hit their AnT at 65% of VO₂ max; an elite marathoner may reach theirs at 85–90%.
Armstrong and Welsman (2020) tracked the development of aerobic and anaerobic fitness in youth athletes, showing that both thresholds respond to training — but at different developmental rates — making early threshold-aware programming critical for long-term athletic development.
Threshold Position Across Events:
• 5K: Performed near or slightly above AnT
• Half-marathon/Marathon: Close to AnT; AeT determines how long you can hold pace
• Ultra-endurance events: Primarily at or below AeT — fat oxidation efficiency is paramount
Thresholds as Clinical Biomarkers — This Isn't Just for Athletes
The anaerobic threshold identified during CPET carries independent prognostic value for cardiovascular mortality. In some studies, AnT outperforms VO₂ max as a predictor of survival in heart failure patients — reflecting the integrative efficiency of oxygen delivery, muscle uptake, and metabolic clearance.
Ryuzaki et al. (2023) demonstrated ECG-based real-time AnT estimation in heart failure patients — opening a door to continuous, wearable-based metabolic monitoring in clinical populations.
For patients with insulin resistance, type 2 diabetes, or obesity, the AeT is particularly informative. These individuals typically have reduced fat oxidation capacity and a depressed aerobic threshold — meaning even modest exercise rapidly shifts them toward glycolytic metabolism and fatigue. Raising the AeT through targeted Zone 2 training directly addresses this metabolic dysfunction.
Training to Raise Your Aerobic Threshold — Zone 2
Zone 2 training — low-intensity, sustained aerobic work performed near but below the AeT — has attracted significant scientific and popular attention. What happens physiologically:
• Mitochondrial biogenesis is stimulated (more mitochondria per muscle cell)
• Fat oxidation efficiency increases
• Capillary density improves
• Cardiac stroke volume increases
The systematic review by Ambaum and Hoppe (2025) reinforces the importance of accurately characterizing energy system demands — their findings highlight that many athletes significantly overestimate how much high-intensity work is productive, while undervaluing sustained aerobic volume.
The Core Principle:
Go slower to get faster. Long runs, easy cycling, swimming, and brisk walking — performed at a conversational pace for 45–90+ minutes — form the foundation of AeT improvement.
Training to Raise Your Anaerobic Threshold — Tempo & Intervals
Raising the AnT requires sustained work at or just below threshold intensity. Effective methods include:
• 20–40 minutes at a "comfortably hard" pace (~80–85% HRmax).
• Repeated bouts of 8–15 minutes at threshold with short recovery.
• For events performed near AnT, event-pace training is both a training and rehearsal stimulus.
Drwal and Maciejczyk (2025) compared strength training versus aerobic interval training, finding that aerobic interval training produced superior improvements in anaerobic capacity, aerobic power, and second ventilatory threshold — confirming threshold-targeted aerobic work as the most efficient method for raising AnT.
Key adaptations include improved lactate clearance, increased muscle buffering capacity, and enhanced glycolytic enzyme activity.
Polarized vs. Threshold Training — Key Models Explained
Polarized Training Model
Intensity Distribution:
~80% low intensity (below AeT) + ~20% high intensity (above AnT)
Minimal time spent in moderate/threshold zoneCore Idea: Maximize aerobic base while strategically using high-intensity work
Best Suited For:
Advanced athletes
High training volume programs
Threshold Training Model
Intensity Distribution:
Greater proportion of training near the anaerobic threshold (AnT)Core Idea: Train consistently in the “comfortably hard” zone to improve performance
Best Suited For:
Competitive athletes
Time-limited individuals seeking efficiency
Hybrid Training Model
Intensity Distribution:
Combination of aerobic base training with periodic threshold-focused blocksCore Idea: Periodized approach aligned with competition schedule
Best Suited For:
Recreational athletes
Age-group competitors
General fitness and performance balance
Evidence-Based Insight
A randomized controlled trial (Journal of Coaching and Sports Science, 2025) found that:
Training model selection based on individual threshold profile significantly impacts
Body composition
Hormonal adaptations
Effects were observed in both athletes and non-athletes, reinforcing the importance of personalized training strategies
Common Misconceptions Worth Busting
Myth #1: "Anaerobic means no oxygen."
False. "Anaerobic" refers to energy production pathways that don't require oxygen directly — but your body never stops using oxygen during moderate to high intensity exercise.
Myth #2: "The anaerobic threshold is always 4 mmol/L."
False. The 4 mmol/L figure is a statistical average, not a physiological truth. Individual thresholds vary considerably — in some athletes, LT2 occurs at 3 mmol/L; in others, 6 mmol/L. Individual testing matters.
Myth #3: "Heart rate zones are accurate enough."
Heart rate zones derived from age-predicted HRmax formulas carry significant individual error. They're a useful starting point, but not a substitute for actual threshold testing.
Weekly Training Structure
A balanced approach for a recreational athlete focuses on building the "floor" (AeT) while sharpening the "ceiling" (AnT).
Monday: Aerobic Base Building (AeT)
Activity: Zone 2 easy run.
Focus: Sustained, conversational pace to improve fat oxidation.
Duration: 45–60 minutes.
Tuesday: Active Recovery
Activity: Rest or dedicated mobility/flexibility work.
Focus: Tissue repair and joint health.
Wednesday: Threshold Development (AnT)
Activity: Threshold intervals (e.g., 4 × 10 minutes).
Focus: Working at a "comfortably hard" intensity to improve lactate clearance.
Duration: 60 minutes (including warm-up and cool-down).
Thursday: Low-Impact Aerobic Base (AeT)
Activity: Zone 2 cycling or swimming.
Focus: Aerobic volume without the orthopedic stress of running.
Duration: 60–90 minutes.
Friday: Full Recovery
Activity: Complete rest or a very easy, short walk.
Focus: Mental and physical reset.
Saturday: The "Long Slow Distance" (AeT)
Activity: Long slow run or hike.
Focus: Mitochondrial biogenesis and structural adaptation.
Duration: 90–120 minutes.
Sunday: Active Recovery / Low-Intensity Play
Activity: Optional easy activity (walking, yoga, light swimming).
Focus: General movement and circulation.
Duration: 30–45 minutes.
Long-Term Periodization Principles
Fitness is not a straight line; it requires shifting focus throughout the year.
Phase 1: The Base Block (8–12 Weeks)
Primary Goal: Build the Aerobic Threshold (AeT).
Emphasis: High volume of Zone 2 work. This expands your "metabolic engine" and prepares your tendons and heart for higher intensity.
Phase 2: The Build Block (6–8 Weeks)
Primary Goal: Raise the Anaerobic Threshold (AnT).
Emphasis: Introduce 1–2 sessions per week of intervals or tempo work at "race pace" or threshold intensity.
Phase 3: Taper & Peak (1–2 Weeks)
Primary Goal: Shed fatigue while maintaining "snap."
Emphasis: Drastic reduction in volume (time), but maintaining intensity (speed) to ensure the body is fresh.
Phase 4: Competition & Recovery
Primary Goal: Execute the event and allow for systemic recovery before restarting the cycle.
Key Programming Rules
The 80/20 Rule: Ensure roughly 80% of your total weekly time is spent at or below your AeT (Zone 2).
The "Black Hole" Trap: Avoid spending most of your time in "Zone 3"—the intensity that feels hard but isn't fast enough to be a true threshold stimulus, nor slow enough to be recovery.
Individualize: If your resting heart rate is elevated or sleep quality drops, replace a Wednesday AnT session with an easy Monday-style AeT session.Key Takeaways
Elite Clinician Insight
"Aerobic and anaerobic thresholds are integrative markers of metabolic health — reflecting the function of the cardiac, pulmonary, vascular, and musculoskeletal systems simultaneously. In cardiac rehabilitation and preventive cardiology, threshold-based exercise prescription offers far greater precision and safety than generalized activity guidelines. For patients with heart failure, diabetes, or post-surgical deconditioning, the ventilatory thresholds identified on CPET may be the most important numbers in their medical chart."
Frequently Asked Questions
Q1. What is the difference between the aerobic and anaerobic threshold?
The aerobic threshold (AeT) is the point at which lactate first rises above resting baseline (~2 mmol/L), marking a shift from predominantly fat-based to mixed fuel utilization. The anaerobic threshold (AnT) is the higher-intensity inflection point (~4 mmol/L, variable) beyond which lactate accumulates faster than it can be cleared, and exercise becomes unsustainable within minutes. Put simply: AeT = you can go all day; AnT = you have minutes to hours at most.
Q2. How do I know if I'm training at the right threshold?
The most accessible field test for the AeT is the talk test: if you can speak in complete, comfortable sentences, you're likely below or at AeT. For the AnT, "comfortably hard" — where you can manage a few words but not a conversation — is a reasonable proxy. For precision, laboratory lactate profiling or CPET is the gold standard.
Q3. Can I improve both thresholds simultaneously?
Yes — but different training stimuli drive each adaptation. Zone 2 training (long, slow, aerobic work) primarily improves the AeT, while threshold intervals and tempo running raise the AnT. Most well-designed programs include both within a periodized framework, prioritizing AeT base-building before adding AnT-specific work.
Q4. Is the 'anaerobic threshold' the same as 'lactic acid threshold'?
Nearly — but with an important clarification. What is commonly called the "lactic acid threshold" more accurately refers to the blood lactate threshold (lactate is the measurable form in the body). The terms LT1, LT2, OBLA, and anaerobic threshold are related but not always identical — context and testing methodology matter.
Q5. Why do elite athletes have higher thresholds than recreational athletes?
Elite endurance athletes typically have both a higher AeT (more efficient fat metabolism and greater mitochondrial density) and a higher AnT relative to their VO₂ max (often 85–90% vs. 60–70% in recreational athletes). This is the product of years of high-volume aerobic training and targeted threshold work — not genetics alone.
Q6. Are thresholds important for non-athletes or patients?
Absolutely — and arguably even more so. The anaerobic threshold identified during CPET carries independent prognostic value for cardiovascular mortality and surgical risk. For patients with heart failure, COPD, cancer, or metabolic syndrome, threshold-guided exercise prescription is both safer and more effective than generic recommendations.
Q7. How often should I get my thresholds tested?
For competitive athletes: every 8–12 weeks (corresponding to training blocks). For recreational athletes: once or twice per year. For patients in cardiac rehab or with chronic disease: frequency should be determined by a physician or exercise physiologist based on clinical status and program goals.
Clinical Pearls:
1 . The "Aerobic Gap": The "Mitochondrial Gatekeeper
The AeT is the highest intensity at which mitochondrial density and oxidative enzyme activity can keep pace with pyruvate production. Beyond this point, the recruitment of Type IIa muscle fibers increases, leading to a measurable rise in blood lactate. For clinicians, AeT isn't just a fitness marker; it is a direct proxy for metabolic flexibility—the body's ability to switch efficiently between fat and carbohydrate substrates.
Think of your Aerobic Threshold as your body’s "Green Zone." As long as you stay below this line, your engine is running on a nearly bottomless tank of fat fuel. If you can’t recite the lyrics to your favorite song or hold a full conversation without gasping, you’ve left the Green Zone. To go faster in the future, you must spend more time going slow right now.
2 . The Anaerobic Threshold (AnT): The "Net Lactate Efflux"
The anaerobic threshold (AnT), often referred to as LT2, closely approximates the maximal lactate steady state (MLSS)—the highest exercise intensity at which lactate production and clearance remain in balance. At this point, the rate of lactate appearance (Ra) equals the rate of disappearance (Rd), allowing for a temporary metabolic steady state. However, once exercise intensity exceeds the AnT, lactate production rises disproportionately, outpacing clearance and leading to progressive metabolic acidosis and rapid fatigue.
In clinical populations, particularly those with chronic disease, a reduced AnT is not merely a performance limitation—it is a key determinant of functional capacity, independence, and perioperative risk, with strong associations to increased surgical morbidity.
Your Anaerobic Threshold is like the redline on a car’s tachometer. You can push the needle into the red for a quick pass or a sprint to the finish, but if you keep it there, the engine will overheat and shut down. For most people, this feels like "controlled discomfort"—you can manage a few words, but your brain is screaming at you to slow down.
3 . For the Clinician & Athlete
The "Aerobic Gap"
A hallmark of "Aerobic Deficiency Syndrome" (ADS) is a wide gap between AeT and AnT. If an athlete has a high AnT (can suffer through a fast 5K) but a very low AeT (gets winded on an easy jog), they are metabolically inefficient. Closing this gap by raising the AeT prevents "overtraining syndrome" and improves the power-to-lactate ratio.
"Don't Train in the Gray Zone"
The biggest mistake most people make is training "kind of hard" all the time. This is the Grey Zone: it's too fast to build your aerobic base (AeT) and too slow to improve your top-end speed (AnT). It provides a lot of fatigue with very little fitness reward. Either go truly easy or intentionally hard; avoid the middle.
Key Takeaways:
Metabolic Efficiency vs. Performance Ceiling
Your aerobic threshold (AeT) is the foundation of fat-fueled efficiency for long-duration effort, while your anaerobic threshold (AnT) represents your "redline"—the performance ceiling you can sustain for minutes or hours, but not all day.
Beyond VO₂ Max
True fitness isn't defined by your maximal oxygen uptake alone. Your thresholds determine your "fractional utilization"—how much of that engine you can actually use before metabolic fatigue forces you to slow down.
The Goal: Build the Engine and Raise the Limit
Effective training is dual-focused: training below your aerobic threshold builds a massive, efficient engine, while training near your anaerobic threshold raises your top-end speed and lactate clearance.
Lactate: The Messenger, Not the Villain
Lactate is a vital fuel source and a physiological signaling molecule. It isn't a waste product to be feared, but a guide that defines your metabolic boundaries and dictates your training intensity.
The Zone 2 Paradox
Zone 2 training is often misunderstood as "going easy." In reality, it is a precise, evidence-based stimulus required to trigger mitochondrial biogenesis and improve the fat oxidation necessary for long-term health and endurance.
Precision Over Approximations
Generalized "4 mmol/L" rules and age-based heart rate formulas are merely statistical averages. For both athletes and patients, individualized testing (like the Talk Test, blood lactate, or CPET) is required for truly effective prescription.
Thresholds as Life-Saving Biomarkers
Metabolic thresholds aren't just for racing; they are powerful predictors of cardiovascular health and surgical outcomes. For patients, these numbers are often more clinically relevant than peak performance metrics for determining longevity and quality of life.
Practical Applications — Real-World Action Steps
For Athletes
• Start tracking your Zone 2 sessions using the talk test this week — it costs nothing.
• Consider booking a lactate profile or CPET with a certified sports scientist or exercise physiologist.
• Review your training log: are you spending 70–80% of your training below AeT?
• Use the weekly microcycle template above as a starting framework and adapt to your event calendar.
For Patients & Clinicians
• Ask your cardiologist or physician about CPET if you have cardiovascular disease or metabolic syndrome.
• Discuss threshold-guided exercise prescription with a certified exercise physiologist or cardiac rehab specialist.
• For patients with insulin resistance or obesity, supervised Zone 2 training is the evidence-based first-line intervention.
• Track resting heart rate and perceived exertion trends as simple proxies for aerobic fitness improvement.
For Coaches
• Implement threshold testing at the start of each macrocycle to individualize training zones.
• Avoid the "black hole" — too much time at moderate intensity that is neither aerobic base work nor proper threshold training.
• Use the polarized or hybrid model based on the athlete's event, training age, and weekly volume capacity.
Author’s Note
This article was written with a dual purpose: to bridge the gap between exercise physiology and clinical medicine, and to make complex metabolic concepts accessible without compromising scientific accuracy. As clinicians, we are often trained to view exercise through broad guidelines—“moderate intensity,” “150 minutes per week”—yet physiology is far more nuanced. Aerobic and anaerobic thresholds offer a precision-based framework that aligns far more closely with how the human body actually responds to stress, adapts to training, and progresses toward health or disease.
In both athletic and patient populations, I have consistently observed that outcomes improve when training is guided by physiology rather than arbitrary zones or generalized prescriptions. A patient with insulin resistance struggling with fatigue, or an athlete plateauing despite high training volume, often shares a common issue: a mismatch between training intensity and underlying metabolic capacity. Understanding thresholds allows us to correct that mismatch.
At the same time, it is important to acknowledge that these concepts—while grounded in robust evidence—are not absolute. Threshold values vary between individuals, testing methods differ, and real-world application requires clinical judgment and contextual interpretation. This article is not intended to replace individualized assessment, but rather to provide a scientifically grounded lens through which both clinicians and readers can better understand performance, fatigue, and metabolic health.
Ultimately, the goal is simple: move beyond one-size-fits-all advice and toward a more personalized, physiology-driven approach to exercise and health—one that is both evidence-based and practically sustainable.
• Save this article as your threshold training reference guide
• Share in the comments: Do you use heart rate zones, pace, or the talk test to guide training?
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
Share this article: Send it to a friend or family member who has been told they're "healthy" based solely on blood tests. VO₂ max is the missing piece of their picture.
Related Articles
Lactate Threshold Explained: Boost Stamina, Burn Fat, and Train Smarter
HIIT for Athletes: Boost VO₂ Max, Lactate Threshold, and Peak Performance – Science-Based Guide
HIIT vs Moderate Cardio: Which Improves Cardiovascular Fitness Faster?
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
References
Armstrong, N., & Welsman, J. (2020). The development of aerobic and anaerobic fitness with reference to youth athletes. Journal of Science in Sport and Exercise, 2, 275–286. https://doi.org/10.1007/s42978-020-00070-5
Aerobic VS anaerobic exercise on body composition and hormonal adaptations in athletes and non-athletes: A randomized controlled trial. (2025). Journal of Coaching and Sports Science. https://doi.org/10.58524/JCSS.V4I1.553
Ambaum, C., & Hoppe, M. W. (2025). Evaluation of methods to quantify aerobic-anaerobic energy contributions during sports and exercise — a systematic review and best-evidence synthesis. Frontiers in Sports and Active Living, 7, 1650741. https://doi.org/10.3389/fspor.2025.1650741
Chamari, K., & Padulo, J. (2015). 'Aerobic' and 'anaerobic' terms used in exercise physiology: A critical terminology reflection. Sports Medicine – Open, 1(1), 9. https://doi.org/10.1186/s40798-015-0012-1
Drwal, A., & Maciejczyk, M. (2025). Strength training vs. aerobic interval training: Effects on anaerobic capacity, aerobic power and second ventilatory threshold in men. Applied Sciences, 15(14), 7953. https://doi.org/10.3390/app15147953
Patel, H., Alkhawam, H., Madanieh, R., Shah, N., Kosmas, C. E., & Vittorio, T. J. (2017). Aerobic vs anaerobic exercise training effects on the cardiovascular system. World Journal of Cardiology, 9(2), 134–138. https://doi.org/10.4330/wjc.v9.i2.134
Ryuzaki, T., Shiraishi, Y., Miura, K., Ikura, H., Seki, Y., Azuma, K., Sato, K., Fukuda, K., & Katsumata, Y. (2023). Real-time estimation of anaerobic threshold during exercise using electrocardiogram in heart failure patients. Journal of Clinical Medicine, 12(16), 5225. https://doi.org/10.3390/jcm12165225