Why Skeletal Muscle Is the Body’s Most Powerful Metabolic Organ
Discover how skeletal muscle controls blood sugar, burns fat, and protects your brain. Science-backed guide with practical steps to boost metabolic health
METABOLISMEXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/10/202622 min read
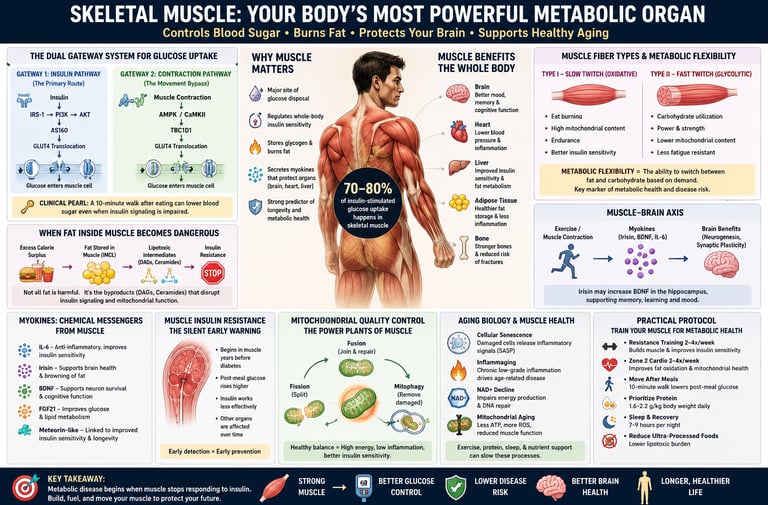
Skeletal muscle is far more than a movement organ—it is the body's metabolic powerhouse. By controlling most glucose uptake, burning fat, producing beneficial myokines, and supporting brain function, healthy muscle plays a key role in preventing insulin resistance, diabetes, cardiovascular disease, and unhealthy aging.
Key Takeaways: Skeletal Muscle & Metabolic Health
1. Your muscle is your main blood sugar sink
Skeletal muscle handles 70–80% of insulin-stimulated glucose disposal after meals. When it stops responding to insulin, blood sugar rises downstream. Metabolic disease starts in the muscle, often years before your A1c moves.
2. You have two ways to clear blood sugar, not one
Insulin activates the PI3K/AKT pathway to move GLUT4 transporters to the cell surface. But muscle contraction activates AMPK/TBC1D1 — a completely separate, insulin-independent route. A 10-minute post-meal walk lowers glucose levels even when insulin signalling is impaired.
3. Strength doesn’t equal metabolic health
Muscle fibers can lose their fat-burning capacity while keeping the same contractile strength. This “metabolic fiber switch” means you can be strong in the gym but still have poor mitochondrial function and rising lactate on a single flight of stairs.
4. Fat in muscle isn’t always bad — but toxic leftovers are
Athletes store more intramyocellular lipid yet remain insulin-sensitive. The danger is when that fat breaks down into DAGs and ceramides. These lipids jam insulin signaling and spill into the blood, damaging your liver, pancreas, and heart in a process called pan-lipotoxicity.
5. Your muscles are an endocrine organ
Contracting muscle releases myokines like IL-6 and irisin. IL-6 reduces inflammation and boosts fat oxidation. Irisin browns white fat and crosses the blood-brain barrier to increase BDNF — essentially fertilizing your hippocampus for memory and mood.
6. The muscle-brain axis is real
Irisin secreted during exercise directly stimulates BDNF in the brain. Declining irisin with inactivity may link muscle disuse to both insulin resistance and cognitive decline. Movement protects your brain as much as your metabolism.
7. Normal labs don’t mean normal metabolism
Skeletal muscle insulin resistance precedes type 2 diabetes by up to a decade. Fasting glucose and HbA1c can look perfect while GLUT4 trafficking, mitochondrial oxidation, and ceramide burden are already impaired. This is the diagnostic gap.
8. Muscle adapts at any age — if you give it the right signals
Zone 2 training rebuilds mitochondria and burns intramuscular fat. Resistance training increases GLUT4 protein. Post-meal walks activate the contraction gateway. Adequate protein enables repair. You don’t need elite athletics; you need consistent, specific stimulus.
Why Skeletal Muscle Is Central to Metabolic Health
Most people think of skeletal muscle as the tissue that moves their body — something to tone at the gym or lose during aging. But research over the past decade tells a very different story: skeletal muscle is the body's most powerful metabolic organ, and its health determines whether you develop insulin resistance, type 2 diabetes, metabolic syndrome, and even cognitive decline, often years before any blood test reveals a problem.
Here is the number that reframes everything: skeletal muscle accounts for 70–80% of insulin-stimulated glucose uptake in healthy individuals (Richter, Bilan & Klip, 2025). That means after every meal, the fate of most of the sugar entering your bloodstream is decided almost entirely by your muscles. When muscle metabolism falters — silently, gradually, without raising your fasting glucose or HbA1c — the metabolic consequences ripple outward to your liver, heart, brain, and fat tissue.
A 2026 report from the Harvard Nutrition Obesity Symposium reinforced this view: skeletal muscle is now recognized as a central mediator of systemic metabolic health, not just a passive consumer of calories (Carollo et al., 2026). A parallel review in iScience described skeletal muscle metabolism as a linchpin of both health and disease, with implications extending well beyond exercise physiology (Lin et al., 2026).
What you will learn in this article:
How muscle controls blood sugar through two distinct biological pathways
Why fat stored inside muscle cells is not always harmless
How your muscles secrete hormones that protect your brain
Why insulin resistance begins in muscle — silently, often a decade before diagnosis
A science-backed protocol to maintain and restore muscle metabolic health at any age
📌 Key Takeaway: Metabolic disease does not begin with high blood sugar. It begins when skeletal muscle stops responding efficiently to insulin. The earlier you understand this, the more powerful your prevention strategy becomes.
How Muscle Controls Blood Sugar: The Dual-Gateway System
When you eat a carbohydrate-rich meal, blood glucose rises and insulin is released from the pancreas. In a healthy individual, that insulin drives most of the incoming glucose into skeletal muscle for storage or energy. But there are actually two completely separate pathways through which glucose enters a muscle cell — and understanding both is critical for anyone managing blood sugar, insulin resistance, or energy levels.
Gateway 1: The Insulin Pathway
Insulin binds to receptors on the muscle cell surface and activates a cascade:
Insulin → IRS-1 → PI3K → AKT → AS160 → GLUT4 translocation
GLUT4 is the glucose transporter protein that moves to the cell membrane and physically shuttles glucose from the bloodstream into the cell. When this pathway is impaired — a condition called insulin resistance — glucose accumulates in the blood instead.
According to a comprehensive 2025 review in Physiological Reviews, defects in IRS-1 phosphorylation, AKT activation, and GLUT4 vesicle trafficking are among the earliest measurable signs of metabolic dysfunction in muscle (Richter et al., 2025).
Gateway 2: The Contraction Pathway (The "Movement Bypass")
Here is what makes exercise genuinely irreplaceable: muscle contraction activates AMPK (AMP-activated protein kinase) and CaMKII, which trigger GLUT4 translocation independently of insulin. Contraction also activates TBC1D1, a separate regulatory node that bypasses the broken insulin pathway entirely.
This means that even when insulin signaling is damaged, physical movement can still lower blood sugar. A 10-minute post-meal walk, a set of resistance exercises, or a cycling session activates this backup gateway.
🔑 Clinical Pearl: Postprandial blood glucose that drops sharply with a 10-minute walk — but remains elevated after rest — is a sign that the insulin gateway is failing while the contraction gateway remains intact. This is an early, actionable warning sign.
Muscle Fiber Types and Metabolic Flexibility
For decades, muscle physiology divided fibers into two categories: Type I (slow-twitch, oxidative) and Type II (fast-twitch, glycolytic). Type I fibers were thought to burn fat; Type II fibers were thought to burn sugar. Simple and clean — but incomplete.
Emerging research reveals a more flexible and clinically important reality: a muscle fiber can lose its metabolic characteristics without changing its contractile identity.
A landmark 2022 study published in Molecular Metabolism by Pereyra and colleagues demonstrated this directly: when fatty acid oxidation was experimentally impaired in mouse muscle, Type I fibers underwent a glycolytic metabolic shift — burning predominantly glucose and producing more lactate — without any change in myosin heavy chain (MHC) isoform composition. The fibers still "looked" like Type I fibers. They still contracted at the same speed. But metabolically, they had switched.
What This Means in Clinical Practice
Muscle strength does not always reflect metabolic health.
A person can have good grip strength and perform well in the gym while still having impaired muscle metabolism.
Type I (slow-twitch) muscle fibers can undergo a metabolic shift.
They may retain their normal contraction speed and appearance.
However, they become less efficient at burning fat and increasingly dependent on glucose for energy.
Mitochondrial function declines during this metabolic switch.
Mitochondrial density decreases.
Fat oxidation becomes impaired.
Energy production becomes less efficient.
Lactate production increases.
Individuals may experience earlier fatigue during low-intensity activities.
Everyday tasks can feel more demanding despite preserved strength.
Insulin sensitivity worsens.
Muscle cells become less responsive to insulin.
Glucose uptake declines, increasing the risk of insulin resistance.
Standard strength tests cannot detect this problem.
Grip strength and muscle size may appear normal.
Metabolic dysfunction can remain hidden for years.
Loss of metabolic flexibility is a key warning sign.
The body becomes less capable of switching between fat and carbohydrate oxidation based on energy demands.
Reduced metabolic flexibility is associated with:
Obesity
Type 2 diabetes
Metabolic syndrome
Cardiovascular disease
Accelerated metabolic aging
Key Takeaway: Metabolically unhealthy muscle can exist even when strength is preserved. Maintaining mitochondrial health and metabolic flexibility may be just as important as maintaining muscle mass and strength for long-term metabolic health
Red Flag Signs of Reduced Metabolic Flexibility:
Post-meal energy crashes ("sugar crash") despite normal fasting glucose
Inability to sustain low-intensity fasted exercise without fatigue
Rapid lactate buildup climbing a single flight of stairs
Getting winded at low heart rates despite good gym strength ("Zone 2 weakness")
Lipotoxicity: When Fat Stored in Muscle Becomes Dangerous
It seems intuitive that fat stored inside muscle cells (intramyocellular lipid, or IMCL) would be harmful. But the reality is more nuanced — and this distinction has major implications for how we interpret body composition.
The Athlete's Paradox
Endurance-trained athletes store significantly more IMCL than sedentary individuals, yet have exceptional insulin sensitivity. This apparent contradiction — known as the Athlete's Paradox — reveals that IMCL accumulation alone is not the problem.
The difference lies in what happens to the stored fat. In athletes, high mitochondrial density and oxidative enzyme activity ensure that IMCL is rapidly oxidized (burned) during activity, and the metabolic intermediates that arise are efficiently cleared.
The Real Problem: Toxic Lipid Intermediates
In sedentary or metabolically impaired individuals, IMCL is not efficiently burned. Instead, it accumulates and is metabolized into two particularly damaging molecules:
Diacylglycerols (DAGs): These activate PKC (protein kinase C), which phosphorylates IRS-1 at serine residues rather than tyrosine. This is like putting the wrong key in a lock — it jams the insulin signaling cascade.
Ceramides: These inhibit AKT directly, shutting down the downstream glucose uptake machinery.
A 2025 review in Cell Discovery introduced the concept of pan-lipotoxicity — the idea that ceramides and DAGs generated in one tissue do not stay there. They enter systemic circulation and inflict parallel damage on the liver (hepatic insulin resistance), pancreatic beta cells (impaired insulin secretion), kidneys, and cardiovascular tissue (Cheng et al., 2025). Lipotoxicity is not a local problem; it is a whole-body, self-amplifying crisis.
Who Is at Risk?
Sedentary individuals regardless of body weight (the "TOFI" phenotype — Thin Outside, Fat Inside)
Those with high waist-to-height ratios or elevated Body Roundness Index (BRI), even with normal BMI
People with poor mitochondrial oxidative capacity (sedentary aging, chronic inactivity)
⚠️ Safety Note: Decreased muscle "tone" or firmness despite adequate protein intake — without weight gain — may suggest intramyocellular lipid infiltration. This warrants clinical evaluation.
Myokines: How Your Muscles Communicate with the Rest of Your Body
Skeletal muscle does far more than contract. When activated — especially during sustained exercise — it releases a family of signaling proteins called myokines into the bloodstream. These molecules act as hormones, coordinating metabolic activity across multiple organ systems.
This discovery, consolidated in research over the past decade, has fundamentally reframed muscle as an endocrine organ — on par with the pancreas, liver, and adipose tissue in its influence over systemic metabolism (Horváth et al., 2025).
Key Myokines and Their Effects
IL-6 (Interleukin-6)
Released During: Prolonged aerobic exercise
Primary Effects: * Exerts anti-inflammatory effects
Stimulates fat oxidation (burning)
Improves hepatic (liver) glucose output
Irisin
Released During: Resistance and aerobic training
Primary Effects: * Promotes "browning" of white fat cells (making them easier to burn)
Crosses the blood-brain barrier
Upregulates BDNF (Brain-Derived Neurotrophic Factor)
BDNF (Brain-Derived Neurotrophic Factor)
Released During: Exercise (specifically within the muscle)
Primary Effects: * Enhances neuroplasticity (brain adaptability)
Improves mood
Boosts memory
Myostatin
Released During: Inactivity
Primary Effects: * Inhibits muscle growth (acts as a counterproductive brake on muscle development)
FGF21 (Fibroblast Growth Factor 21)
Released During: Endurance training
Primary Effects: * Stimulates fat oxidation
Improves metabolic flexibility (the body's ability to switch between burning carbs and fat)
Meteorin-like (METRNL)
Released During: Exercise
Primary Effects: * Promotes adipose (fat) browning
Reduces overall inflammation
IL-6: The Anti-Inflammatory Exercise Signal
Although IL-6 is well known as a pro-inflammatory cytokine in the context of illness or injury, exercise-derived IL-6 operates differently. Released from contracting muscle fibers, it acts to suppress TNF-α, boost fat oxidation, and stimulate glucagon-like peptide-1 (GLP-1) secretion from the gut. This context-dependent signaling is one reason why regular physical activity reduces systemic inflammation.
Irisin: The Fat-Browning, Brain-Boosting Myokine
Irisin is cleaved from the membrane protein FNDC5 during muscle contraction. Its effects are remarkable:
Adipose tissue browning: Irisin converts metabolically sluggish white adipose tissue into calorie-burning beige/brown fat, increasing resting energy expenditure.
Neurological protection: Irisin crosses the blood-brain barrier (discussed in detail in the next section).
Bone health: Emerging evidence links irisin to osteoblast activity and bone mineral density.
📌 Key Takeaway: The myokine secretome — what your muscles "say" to the rest of your body — is determined largely by how much and how hard you exercise. A sedentary lifestyle is not just a calorie imbalance; it is a communication failure between your most powerful metabolic organ and every other tissue in your body.
The Muscle–Brain Axis: Exercise, Irisin, and Cognitive Health
One of the most striking developments in recent metabolic science is the discovery of a direct biological link between skeletal muscle activity and brain health — a pathway now called the muscle–brain axis.
Irisin and the Hippocampus
A 2026 study by Arosio and Picca, published in Experimental Gerontology, described the molecular mechanism in detail: irisin secreted by contracting skeletal muscle crosses the blood-brain barrier and binds to receptors in the hippocampus — the brain region critical for memory formation and learning. There, it stimulates the expression of Brain-Derived Neurotrophic Factor (BDNF), a protein often described as "fertilizer" for neurons (Arosio & Picca, 2026).
BDNF promotes:
Synaptic plasticity (the ability of neurons to form new connections)
Neurogenesis in the adult hippocampus
Protection against age-related neurodegeneration
Improvements in mood and resistance to depression
Clinical Implications: Exercise as Neuroprotection
Declining irisin levels — which occur with physical inactivity and aging — may contribute to both metabolic dysfunction and cognitive decline through a shared upstream cause: muscle disuse.
This means that the same prescription that protects against type 2 diabetes also protects the aging brain. Aerobic exercise, particularly moderate-intensity sustained activity, produces the largest irisin response.
Signs that the muscle–brain axis may be underperforming:
Brain fog that clears noticeably after vigorous exercise
Mood improvements associated specifically with physical activity
Cognitive decline that correlates with periods of inactivity
Muscle Insulin Resistance: The Silent Early Warning
Perhaps the most important public health message in modern metabolic science is this: the disease process of type 2 diabetes begins in skeletal muscle — often a decade before blood tests become abnormal.
The 10-Year Window
Skeletal muscle insulin resistance — characterised by impaired GLUT4 translocation, serine phosphorylation of IRS-1, reduced mitochondrial oxidative capacity, and ceramide accumulation — is measurable years before fasting glucose or HbA1c drifts into the prediabetic range.
A 2025 landmark review in Circulation Research by Whytock and Goodpaster argued that skeletal muscle insulin resistance should be understood as the primary pathological event in type 2 diabetes development, with hepatic and pancreatic dysfunction occurring downstream as compensatory mechanisms eventually fail (Whytock & Goodpaster, 2025).
The Diagnostic Gap
Current standard metabolic screening — fasting glucose, HbA1c, fasting insulin, lipid panel — is largely blind to the earliest stage of this disease. A patient can have:
Normal fasting glucose (< 5.6 mmol/L)
Normal HbA1c (< 5.7%)
Normal fasting insulin
And yet: measurable skeletal muscle insulin resistance
Emerging biomarkers that may eventually close this gap include circulating acylcarnitines, ceramide profiles, and irisin levels — but these are not yet in routine clinical use.
The Good News
Skeletal muscle is one of the most responsive and adaptable tissues in the human body. Even in advanced insulin resistance, the contraction-mediated GLUT4 pathway remains at least partially intact, meaning that structured exercise can meaningfully restore glucose uptake even before full insulin sensitivity is recovered.
Skeletal Muscle Assessment: A Clinical Checklist
The following five domains can help identify early metabolic muscle dysfunction before blood sugar rises on standard tests. These are clinical observations, not diagnostic tests — use them to guide conversations with your healthcare provider.
✅ 1. Metabolic Flexibility
What to observe: Can you transition between fat and carbohydrate burning without crashing?
Warning signs: Post-meal energy crashes, reactive hypoglycemia, inability to exercise fasted without immediate fatigue
Science: Impaired substrate switching reflects a "stuck" Randle Cycle secondary to intramyocellular lipid accumulation
✅ 2. Myokine Function (Muscle–Brain Proxy)
What to observe: Does exercise reliably sharpen your thinking?
Warning sign: Persistent brain fog that improves after aerobic exercise — suggesting baseline neuro-inflammation and reliance on acute BDNF pulses
Science: Chronic inflammation suppresses basal irisin, leaving the brain dependent on exercise-induced spikes
✅ 3. Body Composition Quality (Lipotoxicity Risk)
What to observe: Waist-to-height ratio, Body Roundness Index (BRI), muscle firmness
Warning sign: High BRI or waist-to-height > 0.5 in someone with normal BMI (the TOFI phenotype)
Science: Visceral fat correlates strongly with ceramide spillover into skeletal muscle
✅ 4. Post-Meal Glucose Response (GLUT4 Efficiency)
What to observe: Blood glucose at 1 and 2 hours post-meal, and response to light movement
Warning sign: Glucose remains elevated at 2 hours but drops quickly with a 10-minute walk
Science: Indicates insulin gateway impairment (AS160 dysfunction) with intact contraction gateway (AMPK/TBC1D1)
✅ 5. Zone 2 Endurance (Mitochondrial Capacity)
What to observe: Heart rate at low exercise intensities; lactate accumulation during everyday activity
Warning sign: Breathing heavily while climbing one flight of stairs; high heart rate during a gentle walk; poor sustainable aerobic output despite gym strength
Science: Reflects a metabolic fiber type switch — oxidative capacity lost while contractile strength remains
When to get labs
Standard fasting glucose and HbA1c miss the earliest phase of muscle insulin resistance, which can start 5–10 years before blood sugar rises. Consider advanced testing if you have normal labs but show red flags: post-meal crashes, high waist-to-height ratio >0.5, poor Zone 2 endurance, or a strong family history of type 2 diabetes. The most sensitive clinical test is a 2-hour oral glucose tolerance test (OGTT) with insulin levels drawn at 0, 30, 60, 90, and 120 minutes. From those values, your clinician can calculate the Matsuda Index — a validated measure of whole-body insulin sensitivity that heavily reflects skeletal muscle function. A Matsuda Index <4.3 suggests insulin resistance even with normal fasting glucose. Other emerging markers include fasting ceramide panels and acylcarnitines, but OGTT with insulin remains the gold standard for detecting the “muscle phase” of disease before A1c changes.
Mitochondrial Quality Control: The Hidden Guardian of Muscle Metabolism
Healthy skeletal muscle depends not only on the number of mitochondria it contains but also on their quality. To maintain an efficient energy-producing network, muscle cells continuously perform mitochondrial quality control, a process involving mitophagy, fusion, and fission. Mitophagy selectively removes damaged mitochondria before they generate excessive reactive oxygen species (ROS) or impair cellular metabolism. Meanwhile, mitochondrial fusion allows healthy mitochondria to share proteins, enzymes, and genetic material, enhancing energy production and resilience. In contrast, fission separates damaged mitochondrial segments so they can be repaired or eliminated.
With aging, physical inactivity, obesity, and insulin resistance, these quality-control systems become less efficient. Dysfunctional mitochondria accumulate, contributing to reduced fat oxidation, impaired glucose uptake, chronic inflammation, and metabolic inflexibility. Regular aerobic exercise, resistance training, and metabolic stressors such as intermittent fasting stimulate mitophagy and improve mitochondrial dynamics. Emerging evidence suggests that preserving mitochondrial quality may be just as important as increasing mitochondrial quantity for maintaining long-term metabolic health and preventing age-related disease.
Skeletal Muscle, Aging, and Longevity: More Than Strength Preservation
Skeletal muscle plays a central role in healthy aging, influencing processes far beyond movement. As we age, muscle tissue accumulates senescent cells—damaged cells that stop dividing but continue releasing inflammatory molecules known as the senescence-associated secretory phenotype (SASP). This contributes to inflammaging, the chronic low-grade inflammation that accelerates insulin resistance, cardiovascular disease, frailty, and cognitive decline. Aging is also associated with a gradual decline in NAD+, a critical cellular molecule required for energy production, DNA repair, and activation of longevity-related proteins called sirtuins. Reduced NAD+ impairs mitochondrial function and metabolic resilience. At the same time, mitochondrial aging leads to decreased ATP production, increased oxidative stress, and reduced fat oxidation, contributing to metabolic inflexibility and sarcopenia. Regular exercise—particularly resistance and aerobic training—helps counter these changes by reducing inflammation, stimulating mitochondrial renewal, improving NAD+ metabolism, and preserving muscle function, making skeletal muscle one of the most powerful regulators of healthy aging and longevity.
Evidence Summary: Key Studies at a Glance
Muscle as a Systemic & Endocrine Organ
Carollo et al. (2026) | American Journal of Clinical Nutrition
Key Finding: Harvard Symposium report establishing skeletal muscle as a vital systemic metabolic mediator.
Lin et al. (2026) | iScience
Key Finding: A comprehensive review of skeletal muscle metabolism in both healthy states and disease.
Horváth et al. (2025) | Physiological Research
Key Finding: Overview of myokine biology, detailing how muscle functions as an endocrine, paracrine, and autocrine organ (signaling systemically, locally, and to itself).
The Muscle-Brain Axis
Arosio & Picca (2026) | Experimental Gerontology
Key Finding: Irisin successfully crosses the blood-brain barrier (BBB) to upregulate hippocampal BDNF, proving a direct muscle-to-brain communication axis.
Insulin Resistance, Lipotoxicity, & Exercise Recovery
Richter, Bilan & Klip (2025) | Physiological Reviews
Key Finding: Comprehensive review of the dual GLUT4 gateway highlights AMPK activation during exercise as an insulin-independent rescue mechanism for glucose uptake.
Whytock & Goodpaster (2025) | Circulation Research
Key Finding: Skeletal muscle insulin resistance (IR) precedes Type 2 Diabetes (T2D) diagnoses by years; exercise successfully restores these damaged signaling pathways.
Cheng et al. (2025) | Cell Discovery
Key Finding: Introduces the "pan-lipotoxicity" concept, mapping the systemic damage loop caused by lipotoxic compounds like ceramides and diacylglycerol (DAG).
Fiber Types & Exercise Adaptation
Smith, Murach, Dyar et al. (2023) | Nature Reviews Molecular Cell Biology
Key Finding: A thorough, mechanistic overview of exercise metabolism and how skeletal muscle adapts to stress.
Pereyra et al. (2022) | Molecular Metabolism
Key Finding: Demonstrates that metabolic fiber type switching can occur without changing myosin heavy chain (MHC) expression, revealing completely dissociable regulatory programs
Common Myths and Mistakes About Muscle and Metabolism
❌ Myth 1: "If My Blood Sugar Is Normal, My Metabolism Is Fine"
The truth: Standard glucose testing cannot detect skeletal muscle insulin resistance. Years of impaired GLUT4 signaling, mitochondrial decline, and ceramide accumulation can occur while fasting glucose and HbA1c remain in normal ranges. Treating a normal A1c as a clean bill of metabolic health is one of the most consequential errors in preventive medicine.
❌ Myth 2: "Fat in Muscle Is Always Bad"
The truth: Elite endurance athletes store more intramyocellular fat than sedentary people. What matters is not the quantity of stored fat, but the oxidative capacity to clear it and prevent toxic intermediate accumulation. This is the Athlete's Paradox — and it means fitness quality matters more than body fat percentage alone.
❌ Myth 3: "Strong Muscles Are Metabolically Healthy Muscles"
The truth: Contractile strength and metabolic function are independently regulated. The 2022 Pereyra study demonstrated that muscle can undergo a complete glycolytic metabolic switch without any change in myosin heavy chain composition or strength output. A person can have high gym numbers and seriously impaired fat oxidation capacity simultaneously.
❌ Myth 4: "Only Obese People Have Metabolic Muscle Problems"
The truth: The TOFI phenotype (Thin Outside, Fat Inside) demonstrates that intramyocellular lipid infiltration, visceral fat accumulation, and pan-lipotoxicity can occur in individuals with normal or even low BMI. Sedentary behavior is a more reliable predictor of skeletal muscle metabolic dysfunction than body weight.
❌ Myth 5: "Exercise Only Helps Because It Burns Calories"
The truth: The caloric accounting of exercise is its least important metabolic effect. Regular exercise independently: increases GLUT4 protein expression, expands mitochondrial density, reduces ceramide and DAG accumulation, restores IRS-1 signaling, secretes myokines that protect the liver and brain, and activates AMPK — a bypass route around broken insulin signaling. These effects persist long after the post-exercise calorie burn is over.
Practical Protocol: How to Train Your Muscle for Metabolic Health
The following evidence-based framework targets the specific mechanisms described in this article. Always consult your physician before beginning a new exercise or nutrition program, especially if you have metabolic disease, cardiovascular risk, or musculoskeletal conditions.
🏃 Component 1: Zone 2 Aerobic Training (Mitochondrial Density + IMCL Oxidation)
What it is: Sustained aerobic exercise at ~60–70% of maximum heart rate — a pace where you can hold a broken conversation but cannot sing.
Why it works: Zone 2 is the primary stimulus for mitochondrial biogenesis (via PGC-1α), fatty acid oxidation enzyme upregulation, and IMCL clearance. It is the most direct intervention for restoring metabolic fiber type function.
Protocol:
Frequency: 3–5 sessions per week
Duration: 30–60 minutes per session
Modes: Brisk walking, cycling, swimming, light jogging, rowing
🏋️ Component 2: Resistance Training (GLUT4 Upregulation + Muscle Mass Preservation)
What it works: Resistance training increases GLUT4 transporter protein expression in muscle cells, increases insulin-independent glucose uptake capacity, and preserves or builds metabolically active muscle tissue.
Protocol:
Frequency: 2–3 sessions per week
Structure: 2–4 sets, 8–15 repetitions, major compound movements (squat, deadlift, press, row)
Progressive overload: Gradually increase weight or volume over weeks
🚶 Component 3: Post-Meal Walks (Contraction Gateway Activation)
What it does: Even a 10-minute walk after a carbohydrate-containing meal activates AMPK and TBC1D1, driving GLUT4 to the membrane and lowering postprandial glucose by 15–30% in studies of individuals with and without insulin resistance.
Protocol:
Timing: Within 30 minutes of finishing a meal
Duration: 10–20 minutes minimum
Intensity: Light — no special effort required
🥩 Component 4: Protein Timing and Adequacy (Muscle Protein Synthesis)
Adequate dietary protein is the substrate for muscle maintenance and repair. Without it, exercise stimulus cannot translate into structural or functional improvements.
Evidence-based targets:
General metabolic health: 1.2–1.6 g protein per kg body weight per day
Older adults (> 60): 1.6–2.0 g/kg/day due to anabolic resistance
Distribution: 30–40 g per meal maximizes muscle protein synthesis per session
Sources: Lean meats, fish, eggs, dairy, legumes, soy
🧘 Component 5: Reducing Sedentary Time (GLUT4 Baseline Maintenance)
Even in the absence of formal exercise, extended uninterrupted sitting suppresses GLUT4 activity and AMPK signaling. Breaking sitting time every 30–60 minutes with light movement preserves baseline glucose transporter function.
Simple strategies:
Stand and walk for 2–3 minutes every hour
Take all phone calls standing or walking
Use a standing desk for part of the workday
Walk to a colleague's desk rather than messaging
Frequently Asked Questions
1. What makes skeletal muscle a metabolic organ?
Skeletal muscle is classified as a metabolic organ because it is responsible for 70–80% of insulin-stimulated glucose disposal in healthy individuals and actively secretes hormones called myokines — including IL-6, irisin, and BDNF — that regulate metabolism, inflammation, and neurological function in distant tissues. This qualifies it as an endocrine, paracrine, and autocrine organ with effects far beyond locomotion (Horváth et al., 2025).
2. Can you have insulin resistance with a normal HbA1c and fasting glucose?
Yes. Skeletal muscle insulin resistance — characterized by impaired IRS-1 phosphorylation, reduced GLUT4 translocation, and increased ceramide burden — can be measurably present years before blood glucose or HbA1c rise into the prediabetic range. This is why standard glucose screening misses the earliest and most treatable stage of metabolic disease (Whytock & Goodpaster, 2025).
3. How does exercise improve insulin sensitivity?
Exercise activates AMPK independently of insulin, driving GLUT4 to the muscle cell membrane through the TBC1D1 pathway. With consistent training, the muscle adapts by increasing GLUT4 protein expression, expanding mitochondrial density, reducing ceramide and DAG accumulation, and normalizing IRS-1 signaling. These changes collectively restore insulin sensitivity through mechanisms that rival or exceed the effects of many pharmacological agents (Richter et al., 2025).
4. What is the Athlete's Paradox?
The Athlete's Paradox refers to the observation that endurance athletes store more intramyocellular lipid (IMCL) than sedentary individuals, yet have superior insulin sensitivity. The resolution is that trained muscle burns IMCL rapidly and efficiently, preventing accumulation of the toxic ceramide and DAG intermediates that drive insulin resistance. Total IMCL volume is not harmful; it is the inability to oxidize it that causes metabolic dysfunction.
5. What is pan-lipotoxicity?
Pan-lipotoxicity, described by Cheng et al. (2025) in Cell Discovery, refers to the systemic, multi-organ injury caused by circulating bioactive lipid species — primarily ceramides and diacylglycerols — generated when fatty acid oxidation is overwhelmed. These molecules do not stay in the muscle where they are generated; they damage the liver, pancreatic beta cells, kidneys, and heart in a self-amplifying cycle. This concept reframes lipotoxicity from a tissue-local problem to a systemic disease mechanism.
6. What is the muscle–brain axis?
The muscle–brain axis describes the bidirectional hormonal communication between contracting skeletal muscle and the central nervous system. During exercise, muscle secretes irisin (cleaved from FNDC5), which crosses the blood-brain barrier and stimulates hippocampal BDNF expression. This promotes neuroplasticity, synaptic connectivity, and protection against age-related neurodegeneration. Declining irisin with inactivity and aging may contribute to both metabolic dysfunction and cognitive decline simultaneously (Arosio & Picca, 2026).
7. Can older adults improve skeletal muscle metabolic function?
Yes. Skeletal muscle retains its capacity for metabolic adaptation across the lifespan, though older adults may require higher protein intake (1.6–2.0 g/kg/day) and progressive resistance training to overcome age-related anabolic resistance. Both Zone 2 aerobic training and resistance training are effective in adults over 60 for improving insulin sensitivity, increasing GLUT4 expression, reducing ceramide burden, and enhancing mitochondrial density. The biology of adaptation does not retire.
8. Is a metabolic fiber type switch reversible?
Based on current evidence, yes. The metabolic glycolytic shift observed in Type I fibers under conditions of defective fatty acid oxidation is driven primarily by regulatory signals that are modifiable with exercise training and metabolic interventions, not permanent structural changes. Regular Zone 2 training in particular stimulates PGC-1α, which drives mitochondrial biogenesis and restores oxidative fiber characteristics without requiring full MHC isoform switching (Pereyra et al., 2022).
9. How do I know if my Zone 2 capacity is poor?
Practical signs of reduced Zone 2 (mitochondrial) capacity include: becoming significantly breathless when walking uphill at a moderate pace; heart rate rising rapidly and staying elevated during low-intensity activity; feeling of muscular burning or fatigue during what should be easy exercise; and pronounced post-exercise fatigue from activity that should feel manageable. If you have access to lactate testing, a lactate level above 2 mmol/L during what should be Zone 2 effort confirms the impairment.
10. What biomarkers might identify early skeletal muscle insulin resistance?
While not yet in routine clinical practice, emerging biomarkers under investigation include circulating acylcarnitines (markers of incomplete fatty acid oxidation), ceramide species in plasma, irisin levels (which decline with inactivity and insulin resistance), and the Matsuda insulin sensitivity index derived from oral glucose tolerance tests. Future metabolic screening may incorporate these to detect the "muscle phase" of disease before blood glucose rises.
11. How quickly does exercise improve muscle insulin sensitivity?
A single bout of moderate to vigorous exercise can improve insulin sensitivity for 24–72 hours through AMPK-mediated GLUT4 translocation and post-exercise glycogen replenishment signaling. Structural improvements — increased GLUT4 protein content, mitochondrial density, and reduced ceramide burden — develop over 6–12 weeks of consistent training. This is why consistency, not intensity spikes, is the key variable.
12. Does diet alone improve skeletal muscle metabolism?
Diet modifies the substrate environment but cannot replicate the mechanistic benefits of exercise on muscle metabolism. Reducing refined carbohydrates and saturated fat lowers the ceramide and DAG burden, and adequate protein supports muscle protein synthesis. However, only exercise activates AMPK, stimulates GLUT4 upregulation, triggers myokine secretion, and expands mitochondrial capacity. Diet and exercise are synergistic, not interchangeable.
13. How does skeletal muscle affect metabolism?
Skeletal muscle controls metabolism by removing glucose from the bloodstream, oxidizing fats for energy, and releasing signaling molecules that influence the brain, liver, heart, and adipose tissue. Healthy muscle improves insulin sensitivity, metabolic flexibility, and long-term cardiometabolic health
Conclusion and Action Steps
The central insight of modern metabolic science is straightforward and transformational: type 2 diabetes, metabolic syndrome, and much of the cognitive decline associated with aging do not begin in the pancreas or the brain. They begin in skeletal muscle — quietly, slowly, and years before standard tests reveal anything.
Skeletal muscle is not background tissue. It is the body's primary glucose regulator, its most responsive endocrine organ, and the source of biological signals that determine the health of your liver, brain, cardiovascular system, and adipose tissue. It accounts for 70–80% of insulin-stimulated glucose uptake, secretes hormones that protect your neurons, and retains its capacity for adaptation at virtually any age.
Your Evidence-Based Action Plan
This week:
Add a 10–15 minute walk after your two largest meals
Break sitting time every 60 minutes with 2–3 minutes of light activity
Ensure at least 25–30 grams of protein at each main meal
This month:
Establish 3 Zone 2 aerobic sessions per week (30–45 minutes each)
Add 2 resistance training sessions targeting major compound movements
Track your postprandial energy: note if a short walk meaningfully reduces energy crashes
This year:
Build progressive aerobic capacity (measured by sustainable heart rate and recovery speed)
Work with your healthcare provider to consider advanced metabolic markers if you have risk factors
Review your diet for sources of excess saturated fat and refined carbohydrate that contribute to the ceramide burden
⚠️ Consult Your Doctor: If you have existing cardiovascular disease, type 2 diabetes, musculoskeletal conditions, or take medications that affect blood glucose, please speak with your healthcare provider before beginning a new exercise protocol. The recommendations above are general health information and require individualization.
📌 The Most Important Takeaway: Muscle adapts. It is not destiny. At nearly any age, and across a wide spectrum of metabolic states, skeletal muscle retains a remarkable capacity for recovery and remodeling. Understanding that biology changes how we approach prevention — and how we live.
Author's Note
As a clinician, one of the most common misconceptions I encounter is the belief that normal blood sugar levels automatically mean good metabolic health. In reality, many of the earliest changes that lead to insulin resistance and type 2 diabetes occur silently within skeletal muscle years before routine laboratory tests become abnormal.
I recall a middle-aged patient who maintained a normal body weight, had a normal HbA1c, and appeared healthy by conventional standards. However, he frequently complained of post-meal fatigue, declining exercise tolerance, and increasing abdominal fat despite no major changes in diet. Further evaluation revealed several markers of metabolic dysfunction despite "normal" routine testing. After implementing a structured program of resistance training, aerobic exercise, increased daily movement, and improved protein intake, his energy levels, body composition, and metabolic markers improved substantially over the following months.
Cases like this reinforce an important lesson: metabolic health is not determined solely by the pancreas, the scale, or a laboratory report. Skeletal muscle is a dynamic metabolic organ that influences glucose regulation, fat metabolism, inflammation, cognitive health, and healthy aging. Protecting muscle health may be one of the most powerful investments we can make for long-term disease prevention and longevity.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health | DR T S DIDWAL
References
Arosio, B., & Picca, A. (2026). Irisin and the muscle–brain axis: Mechanisms and translational potential. Experimental Gerontology, 214, 113028. https://doi.org/10.1016/j.exger.2026.113028
Carollo, L., et al. (2026). Muscle movement and metabolism: Exercise and skeletal muscle as mediators of health — A report from the 26th Annual Harvard Nutrition Obesity Symposium, 2025. The American Journal of Clinical Nutrition, 123(5), Article 101262. https://doi.org/10.1016/j.ajcnut.2026.101262
Cheng, Y., Shao, S., Wang, Z., et al. (2025). From lipotoxicity to pan-lipotoxicity. Cell Discovery, 11, 27. https://doi.org/10.1038/s41421-025-00787-z
Horváth, L., Pekař, M., Švagera, Z., Horká, V., Mráz, M., & Bužga, M. (2025). Skeletal muscle as an auto-, para- and endocrine organ: The role of myokines in muscle metabolism and other metabolic organs. Physiological Research, 74(Suppl 1), S37–S56. https://doi.org/10.33549/physiolres.935751
Lin, D., et al. (2026). Skeletal muscle metabolism in health and disease: Mechanisms, interventions, and clinical perspectives. iScience, Article 115024. https://doi.org/10.1016/j.isci.2026.115024
Pereyra, A. S., Lin, C.-T., Mesa Sanchez, D., Laskin, J., Spangenburg, E. E., Neufer, P. D., Fisher-Wellman, K., & Ellis, J. M. (2022). Skeletal muscle undergoes fiber type metabolic switch without myosin heavy chain switch in response to defective fatty acid oxidation. Molecular Metabolism, 59, 101456. https://doi.org/10.1016/j.molmet.2022.101456
Richter, E. A., Bilan, P. J., & Klip, A. (2025). A comprehensive view of muscle glucose uptake: regulation by insulin, contractile activity, and exercise. Physiological Reviews, 105(3), 1867–1945. https://doi.org/10.1152/physrev.00033.2024
Smith, J. A. B., Murach, K. A., Dyar, K. A., et al. (2023). Exercise metabolism and adaptation in skeletal muscle. Nature Reviews Molecular Cell Biology, 24, 607–632. https://doi.org/10.1038/s41580-023-00606-x
Whytock, K. L., & Goodpaster, B. H. (2025). Unraveling skeletal muscle insulin resistance: Molecular mechanisms and the restorative role of exercise. Circulation Research, 137(2), 184–204. https://doi.org/10.1161/CIRCRESAHA.125.325532
Last reviewed: June 2026 | Next review scheduled: December 2026