Want Faster Fat Loss? Here's What Science Says About HIIT vs. MICT
Does HIIT really outperform steady-state cardio? Explore the latest evidence on fat burning, fitness, metabolic health, and who should choose HIIT or MICT.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/2/202617 min read
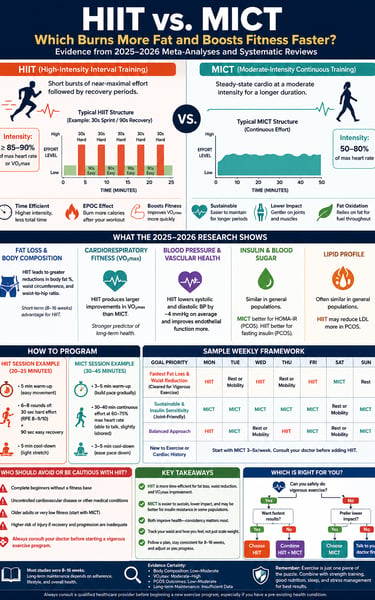
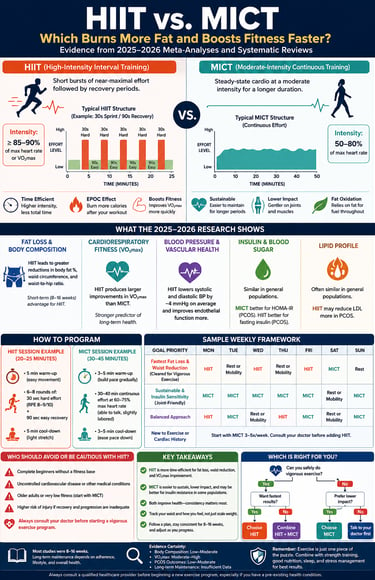
HIIT vs. MICT: Key Research Findings
HIIT burns body fat and reduces waist circumference more efficiently per minute.
HIIT produces larger improvements in VO₂max (cardiorespiratory fitness).
MICT is easier to sustain and carries a lower injury risk.
Both improve blood pressure, insulin sensitivity, and overall cardiovascular health.
A combination of HIIT and MICT provides the most balanced long-term fitness strategy.
1. The "Time-Efficiency" Rule is Quantified
The World Health Organization (WHO) baseline guidelines formally establish a 2:1 time-efficiency ratio for high-intensity training. You can achieve comparable or superior cardiometabolic adaptations in just 75 minutes of weekly vigorous-intensity HIIT, compared to the 150 minutes required for moderate-intensity continuous training (MICT).
2. HIIT Claims the Short-Term Fat Loss Edge
According to 2026 Bayesian network meta-analyses tracking adults with overweight or obesity, HIIT at the recommended dose (75+ min/week) ranks first for reducing body fat percentage, waist circumference, and waist-to-hip ratio. In direct, 8-to-16-week clinical windows, it consistently outperforms MICT for shedding visceral adiposity.
3. The Scale is Deceptive; Track the Tape Measure
An important nuance from the latest clinical trials is that overall body weight and BMI often show no statistical difference between the two methods. HIIT’s physiological magic shifts body composition by targeting fat stores and sparing lean mass, meaning your progress will show up in how your clothes fit long before it registers on a standard bathroom scale.
4. HIIT Decisively Wins the VO2max Race
When it comes to boosting cardiorespiratory fitness—one of the single strongest predictors of all-cause mortality—HIIT is the superior modality. By forcing your heart rate to near-maximal thresholds (85–90%+), it rapidly drives adaptations in cardiac stroke volume and mitochondrial capacity that steady-state jog loops simply cannot match in the same timeframe.
5. Metabolic Responses are Population-Specific
While the 2025 global umbrella reviews confirm that HIIT produces powerful vascular benefits—including a clinically meaningful 4 mmHg drop in average blood pressure—its superiority isn't universal. In trials involving younger, healthier college student cohorts, the metabolic differences (such as lipid profiles and fasting glucose) between HIIT and MICT completely leveled out.
6. The PCOS Paradox: Different Paths for Different Markers
In women managing Polycystic Ovary Syndrome (PCOS), the research splits the crown. MICT proves statistically superior for improving overall insulin resistance (HOMA-IR), likely due to the higher volume of total muscle contraction. Meanwhile, HIIT yields significantly better outcomes for lowering fasting insulin levels and reducing LDL ("bad") cholesterol.
7. The Overtraining and Injury Asterisk
High intensity carries a high tax rate. Systematic reviews explicitly warn that complete beginners, older adults, and individuals with unmanaged cardiovascular profiles face exponentially higher risks of muscle strains, joint overload, and cardiac stress with HIIT. For these populations, MICT serves as a much safer, lower-impact foundational gateway.
8. Consistency Trumps Intensity Over the Long Haul
The most crucial takeaway from the 2026 literature is that current data primarily maps short-term (8–16 week) physiological adaptations. For permanent weight maintenance and metabolic health, the "best" routine is entirely dependent on behavioral adherence. If the grueling nature of HIIT leads to burnout, MICT remains an exceptionally powerful, highly sustainable alternative.
Introduction
If you only have 25 minutes a day to exercise, does it matter whether you spend it sprinting or jogging?
This question sits at the center of one of the most researched debates in exercise science: high-intensity interval training (HIIT) versus moderate-intensity continuous training (MICT). Both are backed by decades of research, both are endorsed by major health bodies, and both can genuinely change your body composition, cardiorespiratory fitness, and metabolic health. But they don't do it the same way, at the same speed, or with the same risk profile.
This guide pulls from several 2025–2026 systematic reviews and network meta-analyses — including a Bayesian network meta-analysis of 18 randomized controlled trials in adults with overweight or obesity, a 133-study umbrella review of HIIT across cardiometabolic, neurologic, and oncologic outcomes, a network meta-analysis in women with polycystic ovary syndrome (PCOS), and a fresh 2026 trial synthesis in college students — to give you a clear, evidence-based answer.
What Is HIIT?
High-intensity interval training alternates short bursts of near-maximal effort with brief recovery periods. Clinically, HIIT is generally defined as work performed at or above roughly 85–90% of maximal heart rate, VO2max, or heart rate reserve, delivered in repeated intervals rather than one continuous effort.
The World Health Organization's baseline recommendation is at least 75 minutes of vigorous-intensity activity (the HIIT category) per week, compared with 150 minutes of moderate-intensity activity for MICT — a built-in "time efficiency" that makes HIIT attractive to busy people.
What Is MICT?
Moderate-intensity continuous training is steady-state cardio performed without intervals — think brisk walking, cycling, swimming, or jogging at roughly 50–80% of maximum heart rate for a sustained period, usually 30–60 minutes.
MICT relies primarily on aerobic, fat-based energy metabolism throughout the session, whereas HIIT recruits both aerobic and anaerobic pathways in rapid succession.
HIIT vs. MICT for Fat Loss and Body Composition
This is where most people start — and where the newest evidence gives a fairly consistent answer, with important caveats.
What the 2026 network meta-analysis found
A 2026 Bayesian network meta-analysis in BMC Sports Science, Medicine and Rehabilitation pooled 18 randomized trials (952 participants) comparing HIIT and MICT at WHO-recommended volumes in adults with overweight or obesity. Compared with a non-exercising control group, HIIT performed at 75 or more minutes per week produced meaningfully larger reductions in body fat percentage, waist-to-hip ratio, and waist circumference than any other intervention tested, and it ranked first on the statistical ranking system (SUCRA) for nearly every body-composition outcome measured.
In direct head-to-head comparisons, this HIIT dose outperformed MICT (150+ minutes/week) for both body fat percentage and waist circumference. MICT still produced statistically meaningful improvements versus doing nothing — it just didn't match HIIT's effect size on these specific markers over the 8–16 week intervention windows studied.
Confirmed by an independent 2026 trial pool
A separate 2026 synthesis of 20 randomized trials in college students (745 participants) reached a similar conclusion in direct HIIT-vs-MICT comparisons: HIIT produced significantly greater reductions in body weight, body fat percentage, waist-to-hip ratio, waist circumference, and fat mass than MICT. Neither method reliably outperformed the other on BMI, hip circumference, lean muscle mass, or routine blood lipid and glucose markers.
The important asterisk
Two things temper the "HIIT wins" headline:
Body weight and BMI themselves often show no difference between HIIT and MICT. The advantage shows up in body composition markers (fat percentage, waist circumference) more consistently than on the bathroom scale.
This is short-term evidence. Almost all included trials ran 8–16 weeks. Researchers explicitly caution that these findings describe short-term physiological adaptation, not long-term weight maintenance or relapse prevention — an area where adherence, not exercise mode, may matter more.
Clinical takeaway: if your primary goal is losing body fat and shrinking your waistline in a defined 8–16 week window, and you're medically cleared for vigorous exercise, HIIT has a time-efficient edge. If you have more time, prefer steady efforts, or need a lower-impact entry point, MICT still delivers real, statistically significant fat-loss benefits — just somewhat more slowly per minute invested.
Cardiorespiratory Fitness: VO2max Head-to-Head
VO2max — your body's maximum capacity to use oxygen during exercise — is one of the strongest predictors of long-term cardiovascular health and all-cause mortality risk in the research literature.
Here, HIIT's advantage is more decisive. In the 2026 obesity network meta-analysis, HIIT at 75+ minutes/week produced the largest improvement in VO2max among all interventions tested, and it significantly outperformed lower-volume HIIT as well as combined HIIT-plus-recovery protocols. The 2025 umbrella review of 133 systematic reviews similarly concluded that even low-dose HIIT was more effective than MICT for improving cardiorespiratory fitness, although the evidence did not clearly show HIIT beating MICT or no exercise for reducing body fat or building muscle mass in isolation — reinforcing that "better VO2max" and "better fat loss" are not the same claim.
Why VO2max responds so strongly to HIIT
Repeated near-maximal efforts recruit fast-twitch muscle fibers and stress both the cardiac pump and the oxidative machinery inside muscle cells simultaneously. This combined stimulus appears to drive faster gains in stroke volume, capillary density, and mitochondrial biogenesis than continuous, sub-maximal effort — though MICT still improves all of these over longer training periods.
Insulin, Blood Sugar, and Metabolic Health
Fitness and fat loss aren't the whole story — insulin sensitivity and lipid markers matter just as much for long-term cardiometabolic risk.
The umbrella review of 133 systematic reviews found HIIT conferred benefits comparable to or better than MICT across diabetes, blood pressure, and vascular function outcomes, including a roughly 4 mmHg average reduction in systolic and diastolic blood pressure — a change large enough to be clinically meaningful at a population level, since even 2 mmHg reductions are associated with lower cardiovascular event rates.
HIIT was also found to improve vascular endothelial function (a marker of artery health) more than MICT in several of the reviews synthesized, potentially through greater nitric oxide bioavailability.
However, the 2026 college-student trial pool found no significant HIIT-vs-MICT difference in total cholesterol, triglycerides, HDL, LDL, fasting glucose, or fasting insulin — suggesting that HIIT's metabolic edge over MICT is not universal and may depend heavily on population, baseline health status, and program duration.
Bottom line: for blood pressure and vascular function, HIIT has an edge supported by a large evidence base. For routine lipid and glucose panels in relatively healthy populations, the two methods often perform similarly.
Special Case: HIIT and MICT in PCOS
Polycystic ovary syndrome (PCOS) affects up to 13% of reproductive-age women and carries elevated cardiometabolic risk through insulin resistance, dyslipidemia, and often obesity. A 2026 network meta-analysis of 23 randomized trials (1,192 participants) specifically compared HIIT, MICT, low-intensity training, and no exercise in women with PCOS — and the results split by outcome in a genuinely interesting way:
Insulin resistance (HOMA-IR): MICT produced a statistically significant improvement; HIIT did not reach significance for this specific marker, possibly because the MICT protocols studied often exceeded 160 minutes per week.
Cardiorespiratory fitness (VO2max): Both methods improved fitness substantially, with HIIT showing a slightly larger average gain.
Fasting insulin and LDL cholesterol: Both HIIT and MICT produced significant reductions, with HIIT showing a larger effect size for both markers.
BMI, glucose, triglycerides, HDL, and blood pressure: Neither method produced statistically significant changes in this population.
Practical implication for PCOS: this isn't a case of "one method wins." MICT appears especially valuable for insulin resistance specifically, while HIIT may offer a stronger fitness and lipid response — supporting a genuinely individualized approach rather than a blanket recommendation, which mirrors current PCOS management guidelines that don't endorse one exercise intensity over another.
The Physiology: Why the Two Methods Diverge
Interpreting why these results happen matters more than memorizing the numbers, because it tells you what to expect from your own training.
HIIT's proposed mechanisms (drawn from mechanistic research summarized in the 2026 obesity meta-analysis):
Repeated high-intensity efforts stimulate epinephrine and norepinephrine release, activating hormone-sensitive lipase and mobilizing stored fat into free fatty acids for use as fuel.
Post-exercise oxygen consumption stays elevated for longer after HIIT than after steady-state work, meaning calorie burn continues after the session ends.
Short, explosive efforts recruit fast-twitch fibers not heavily used during steady jogging or cycling, which may explain the added benefit to waist circumference and fat percentage even when total exercise time is lower.
Important caveat: the underlying randomized trials generally did not measure these molecular pathways directly — the mechanistic explanation is drawn from separate physiology research and should be read as a plausible model, not proven causation in every study population.
MICT's proposed mechanisms:
Sustained, moderate effort relies predominantly on fat oxidation as a fuel source throughout the session.
Continuous aerobic stress is associated with gradual, well-established improvements in mitochondrial density and oxidative enzyme activity, built up over a longer time horizon than HIIT typically requires for comparable adaptation.
Because MICT is lower-impact and easier to sustain by feel, it may support better long-term inflammation control and vascular remodeling in populations who can commit to higher weekly volumes.
Who Should Avoid HIIT
HIIT is not risk-free, and the same umbrella review that documented its benefits was explicit about who needs caution:
Complete beginners without a base level of fitness face a higher injury risk from HIIT's speed and complexity — proper warm-up, technique coaching, and a gradual progression matter more than for MICT.
People with uncontrolled cardiovascular disease or other conditions worsened by vigorous exertion should not begin HIIT without medical clearance and, ideally, supervised programming.
Older adults or those with very low baseline fitness may get comparable cardiorespiratory benefit from MICT with substantially lower injury risk, according to the same review.
HIIT's rapid pace and higher joint loading also raise the risk of overuse injuries and muscle strains if recovery between sessions is inadequate.
Always consult your doctor before starting a new vigorous exercise program, especially if you have a heart condition, are pregnant, have uncontrolled hypertension, or are returning to exercise after a long period of inactivity.
How to Program HIIT and MICT (Practical Protocols)
Sample beginner HIIT session (20–25 minutes, 2–3x/week)
Warm-up: 5 minutes easy cycling, walking, or rowing
6–8 rounds of: 30 seconds hard effort (RPE 8–9/10) + 90 seconds easy recovery
Cool-down: 5 minutes easy movement + light stretching
Sample intermediate/advanced HIIT session
Warm-up: 5–8 minutes
8–10 rounds of: 45–60 seconds at 85–90%+ max heart rate + 60–75 seconds active recovery
Cool-down: 5 minutes
Sample MICT session (30–45 minutes, 3–5x/week)
Warm-up: 3–5 minutes gradually building pace
30–40 minutes continuous effort at a pace where conversation is possible but slightly labored (roughly 60–75% max heart rate)
Cool-down: 3–5 minutes easing pace down
Here is the weekly framework :
For Fastest Fat Loss & Waistline Reduction (If cleared for vigorous exercise)
Suggested Split: 2–3 HIIT sessions per week.
Target Volume: At least 75 total minutes of weekly vigorous-intensity training.
For Better Insulin Sensitivity & Long-Term Sustainability (Joint-friendly approach)
Suggested Split: 4–5 MICT sessions per week.
Target Volume: At least 150 total minutes of weekly moderate-intensity, steady-state cardio.
For a Balanced Approach (If you want the benefits of both or are unsure where to start)
Suggested Split: 2 HIIT sessions + 2 MICT sessions per week.
Target Volume: Blends time-efficient high-intensity training with lower-impact cardiovascular volume.
For Beginners, Older Adults, or Those with a Cardiac History (Safety-first approach)
Suggested Split: Start with MICT only.
Next Steps: Build a baseline of continuous, moderate cardio and thoroughly reassess your fitness with a physician before introducing any high-intensity intervals.
Evidence Summary Tables
Body Composition & Anthropometric Outcomes (HIIT vs. MICT)
Body Fat Percentage: Favors HIIT. Clinical data shows a significantly greater reduction in body fat with HIIT compared to MICT.
Waist Circumference & Waist-to-Hip Ratio: Favors HIIT. HIIT leads to a significantly greater reduction in midsection measurements, indicating superior efficiency at targeting visceral fat.
Body Weight: Mixed Results. HIIT showed a significantly greater reduction in weight among healthy college student cohorts, but this weight-loss edge was inconsistent in adults with overweight or obesity.
BMI (Body Mass Index): No Consistent Difference. Neither training modality reliably outperformed the other across multiple studies.
Lean Muscle Mass: No Significant Difference. Neither cardio method serves as a primary driver for muscle hypertrophy, showing equivalent (minimal) impacts on lean mass.
Cardiorespiratory & Metabolic Outcomes
VO2max (Cardiorespiratory Fitness): Favors HIIT. HIIT consistently drives larger average gains in maximal oxygen uptake compared to MICT.
Blood Pressure: Favors HIIT. High-intensity training reduces systolic and diastolic blood pressure (SBP/DBP) by an average of roughly 4 mmHg, which is a clinically meaningful reduction.
Fasting Insulin (General Population): Comparable Results. Both training methods perform similarly when evaluated in a broad, relatively healthy population.
HOMA-IR (Insulin Resistance in PCOS): Favors MICT. For women with Polycystic Ovary Syndrome, steady-state MICT protocols demonstrated statistical superiority over HIIT.
Fasting Insulin & LDL Cholesterol (PCOS Specific): Favors HIIT. Despite the HOMA-IR results, HIIT produced larger overall reductions in both baseline fasting insulin and "bad" LDL cholesterol within the PCOS study groups.
Scientific Certainty of the Evidence
VO2max Improvements: Moderate to High Certainty. The scientific community has strong confidence in HIIT's superior ability to boost cardiorespiratory fitness.
Body Fat & Waist Circumference Reductions: Low to Moderate Certainty. While data points to a HIIT advantage, confounding real-world variables keep the certainty level modest.
PCOS Metabolic Adaptations: Low to Moderate Certainty. Findings are promising but limited by smaller specialized trial pools.
Long-Term Weight Maintenance: Insufficient Data. There is currently a lack of long-term tracking data to crown either method a definitive winner for preventing weight relapse over extended periods
Common Myths and Mistakes
Myth: "HIIT burns more total calories than MICT." Not necessarily per session — MICT sessions are longer and can match or exceed total calorie expenditure. HIIT's advantage is efficiency per minute and elevated post-exercise oxygen consumption, not a guaranteed higher total burn.
Myth: "If HIIT works better for fat loss, more HIIT is always better." The 2026 obesity meta-analysis found diminishing or inconsistent returns beyond the studied volumes, and higher HIIT frequency raises injury and overtraining risk. More is not automatically better.
Myth: "MICT is a waste of time compared to HIIT." MICT produced statistically significant improvements over no exercise in nearly every outcome studied — including body fat, waist circumference, and VO2max — just with somewhat smaller effect sizes than HIIT in some populations. It also carries lower injury risk and works well for people who cannot tolerate vigorous exercise.
Myth: "These results apply to everyone equally." Almost all trials ran 8–16 weeks in adults with overweight/obesity, college students, or women with PCOS. Results in older adults, adolescents, or people with cardiac disease come from separate, often smaller, evidence bases.
Mistake: Skipping the warm-up before HIIT. Given HIIT's higher injury risk profile, a proper 5–8 minute warm-up is not optional.
Mistake: Judging progress by body weight alone. Since HIIT's clearest advantage shows up in body fat percentage and waist circumference rather than scale weight, tracking a tape measure or body composition scan will show progress that the scale misses.
FAQs
1. Is HIIT or MICT better for losing belly fat? Recent network meta-analyses show HIIT performed at 75+ minutes per week produces significantly greater reductions in waist circumference and waist-to-hip ratio than MICT in adults with overweight or obesity, though MICT still produces meaningful improvements over no exercise.
2. How many days a week should I do HIIT? Most of the trials reviewed used 2–3 HIIT sessions per week totaling at least 75 minutes of vigorous activity, aligning with WHO physical activity guidelines. More frequent HIIT has not been shown to produce proportionally greater benefit and may raise injury risk.
3. Can I do HIIT every day? This isn't well supported by the evidence reviewed here and is generally discouraged; HIIT's intensity requires recovery time between sessions to avoid overuse injury and excessive cardiovascular stress.
4. Does HIIT improve insulin sensitivity as well as MICT? It depends on the population. In women with PCOS, MICT showed a clearer benefit for HOMA-IR (a marker of insulin resistance), while HIIT showed a larger reduction in fasting insulin specifically. In general adult populations, differences between the two methods on insulin markers were often not statistically significant.
5. Is MICT a waste of time if HIIT gets faster results? No. MICT produced statistically significant improvements in body composition and fitness compared with no exercise across the studies reviewed, and it carries a lower injury risk profile, making it a sound long-term option, especially for people who cannot tolerate vigorous training.
6. What heart rate counts as "high intensity" for HIIT? Most clinical definitions used in these studies set HIIT at or above roughly 85–90% of maximum heart rate or VO2max, delivered in short bursts, compared with roughly 50–80% of maximum heart rate for continuous MICT effort.
7. Can beginners do HIIT safely? Yes, with modification — shorter work intervals, longer recovery periods, and a proper warm-up. However, systematic reviews note that complete beginners face a higher relative injury risk with HIIT than with MICT, so building a base fitness level first is often advisable.
8. Does HIIT or MICT build more muscle? Neither method is primarily a muscle-building tool, and the evidence reviewed found no significant difference between HIIT and MICT for lean muscle mass. Resistance training remains the most effective tool for building muscle regardless of which cardio method you choose.
9. Is HIIT safe during or after cancer treatment? Short-term HIIT has shown effectiveness for reducing cancer-related fatigue and pain according to systematic review evidence, and appears comparably safe to usual care in feasibility studies, but any exercise program during or after cancer treatment should be designed with your oncology care team.
10. How long until I see results from HIIT or MICT? Most of the randomized trials reviewed here measured outcomes over 8–16 weeks. Meaningful body composition and fitness changes are generally detectable within that window, but researchers caution these are short-term physiological adaptations, not evidence about long-term weight maintenance.
11. Can I combine HIIT and MICT in the same training week? Yes — many real-world exercise programs mix both, using HIIT for time-efficient fitness and fat-loss stimulus and MICT for lower-impact volume and recovery-friendly cardio. None of the studies reviewed here found combined approaches to be harmful; individualized programming based on your goals and tolerance is reasonable.
12. Does age affect which method is better? Direct age-stratified comparisons were limited in the studies reviewed, but reviews note that older adults and those with lower baseline fitness may achieve comparable cardiorespiratory benefit from MICT with lower injury risk, making it a common starting recommendation before progressing to HIIT under guidance.
Conclusion and Action Steps
The 2025–2026 research doesn't crown one universal winner — it clarifies what each method is genuinely good at:
Choose HIIT if your top priority is time-efficient fat loss, waistline reduction, and rapid VO2max gains, and you're medically cleared for vigorous exercise.
Choose MICT if you want a lower-injury-risk, highly sustainable option — particularly strong for insulin resistance markers in specific populations like PCOS, and just as effective for general health when performed consistently at recommended volumes.
Combine both if you want the fitness edge of HIIT alongside the joint-friendly volume of MICT.
Your next three steps:
Get medical clearance if you have any cardiovascular risk factors, are new to exercise, or are managing a chronic condition.
Pick a starting protocol from the sample sessions above and commit to it for at least 8 weeks — the timeframe used in most of the trials cited here.
Track waist circumference and how your clothes fit, not just the number on the scale, since that's where HIIT's advantage most consistently shows up.
If you're unsure which approach fits your specific health profile, a conversation with your doctor or an exercise physiologist can help translate this research into a plan tailored to you.
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
Related Articles
HIIT for Athletes: Boost VO₂ Max, Lactate Threshold, and Peak Performance – Science-Based Guide
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Sources and References
Deng, Z., Li, Q., Ma, M., Shi, T., Wang, Y., Li, C., Liu, Y., & Wang, Y. (2026). Efficacy of different high-intensity interval training versus moderate-intensity continuous training for body composition and cardiorespiratory fitness in obese/overweight patients: a systematic review and network meta-analysis. BMC Sports Science, Medicine & Rehabilitation, 18(1), 255. https://doi.org/10.1186/s13102-026-01686-w
Viderman, D., Rakhmanov, Y., Aubakirova, M., Kalikanov, S., & Fredericson, M. (2025). The Impact of High-Intensity Interval Training on Cardiometabolic, Neurologic, Oncologic, and Pain-Related Outcomes: A Comprehensive Review of Systematic Reviews. Journal of Clinical Medicine, 14(23), 8328. https://doi.org/10.3390/jcm14238328
Sun, H., Khramov, V. V., Li, J., & Wang, M. (2026). Effects of High-Intensity Interval Training and Moderate-Intensity Continuous Training on Body Composition and Glucose and Lipid Metabolism in College Students: A Systematic Review and Meta-Analysis. Frontiers in Endocrinology, 17, 1894767. https://doi.org/10.3389/fendo.2026.1894767
Sámano Sánchez, M., Floridia Rietmann, L. M., Magallanes Bajana, A., et al. (2026). Comparative cardiometabolic effects of high, moderate, and low intensity exercise in polycystic ovary syndrome: a systematic review and network meta-analysis of randomized controlled trials. BMC Women's Health, 26, 89. https://doi.org/10.1186/s12905-025-04201-4
Zhong, J., Wang, Y., Wu, H., Chen, H., & Li, M. (2026). The independent effects of isolated high-intensity interval training modalities on body composition and adiposity indices in overweight or obese adults: a systematic review and meta-analysis. Frontiers in Physiology, 17, 1791740. https://doi.org/10.3389/fphys.2026.1791740
World Health Organization. (2020). WHO Guidelines on Physical Activity and Sedentary Behaviour.
Coates, A. M., Joyner, M. J., Little, J. P., Jones, A. M., & Gibala, M. J. (2023). A perspective on high-intensity interval training for performance and health. Sports Medicine, 53(Suppl 1), 85–96.
Gibala, M. J., & MacInnis, M. J. (2022). Physiological basis of brief, intense interval training to enhance maximal oxygen uptake: a mini-review. American Journal of Physiology-Cell Physiology, 323(5), C1410–C1416.
Sultana, R. N., Sabag, A., Keating, S. E., & Johnson, N. A. (2019). The Effect of Low-Volume High-Intensity Interval Training on Body Composition and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Sports Medicine, 49, 1687–1721.
Ramos, J. S., Dalleck, L. C., Tjonna, A. E., Beetham, K. S., & Coombes, J. S. (2015). The Impact of High-Intensity Interval Training versus Moderate-Intensity Continuous Training on Vascular Function: A Systematic Review and Meta-Analysis. Sports Medicine, 45, 679–692.
Oppert, J. M., Bellicha, A., van Baak, M. A., et al. (2021). Exercise training in the management of overweight and obesity in adults: synthesis of the evidence and recommendations from the European Association for the Study of Obesity Physical Activity Working Group. Obesity Reviews, 22(4), e13273.
Teede, H. J., Tay, C. T., Laven, J. J. E., et al. (2023). Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. European Journal of Endocrinology, 189, G43–64.
Mueller, S., Winzer, E. B., Duvinage, A., et al. (2021). Effect of high-intensity interval training, moderate continuous training, or guideline-based physical activity advice on peak oxygen consumption in patients with heart failure with preserved ejection fraction: a randomized clinical trial. JAMA, 325(6), 542–551.
Powell-Wiley, T. M., Poirier, P., Burke, L. E., et al. (2021). Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation, 143(21), e984–1010.
Mahase, E. (2023). Global cost of overweight and obesity will hit $4.32tn a year by 2035, report warns. BMJ, 380, 523.