Sarcopenia and Metabolic Disorders: Understanding the Hidden Connection Between Muscle Loss and Metabolism
Explore how sarcopenia links to metabolic dysfunction, and learn evidence-based strategies to prevent muscle loss, boost metabolism, and age healthier
SARCOPENIA
DR T S DIDWAL MD
5/29/202627 min read
Why Your Muscles Are More Than Strength — They’re Your Metabolic Engine
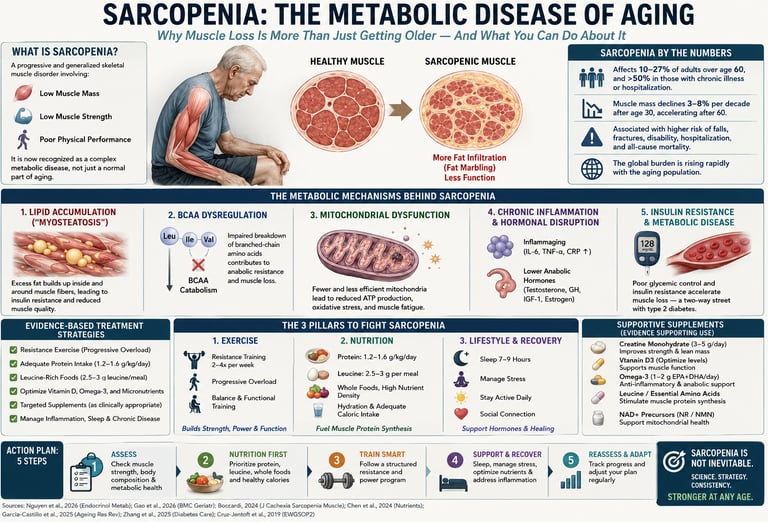
Think muscle loss only means feeling weaker with age? The newest research says otherwise. Sarcopenia — age-related muscle loss — is now understood as a metabolic disease that silently rewires how your body handles energy, sugar, and fat, often years before you notice trouble with a staircase (Boccardi, 2024).
Here’s what’s happening inside you: Your muscles aren’t just shrinking. They’re filling with fat, like a marbled steak (Lal et al., 2025), and their cellular power plants — mitochondria — are failing (Nguyen et al., 2026). Even more surprising, your muscles may lose the ability to properly break down branched-chain amino acids, the building blocks you eat every day. When that process jams up, it doesn’t just hurt muscle — it can actually cause insulin resistance and diabetes (Zuo et al., 2025).
This creates a two-way street: muscle loss drives blood sugar problems, and diabetes accelerates muscle loss (Gao et al., 2026). It’s also why popular weight-loss medications like GLP-1 drugs need caution. They melt pounds, but up to 40% can come from muscle unless you actively protect it (Yang et al., 2026).
But here’s the good news: this isn’t fate. Muscle is remarkably responsive at any age. Progressive resistance training is medicine — it reboots your mitochondria, restores amino acid processing, and melts fat out of muscle tissue (Chen & Wu, 2024). Pair it with 25–40g of high-quality protein per meal, plus vitamin D and creatine, and you’re targeting the root causes, not just symptoms (Dent et al., 2018).
The bottom line: Your muscles are metabolic organs. Protect them like you would your heart. Start lifting weights 2–3 times weekly, prioritize protein at every meal, and talk to your doctor about screening. Because staying strong isn’t vanity — it’s how you stay metabolically alive.
Key Takeaways:
🔹 Sarcopenia is fundamentally a metabolic disease, not simply a loss of muscle tissue. Understanding its metabolic origins opens new avenues for prevention and treatment.
🔹 Lipid metabolism dysfunction plays a central role in sarcopenia, with abnormal fat accumulation in muscle tissue and impaired fatty acid utilization contributing significantly to muscle deterioration.
🔹 Disrupted BCAA catabolism has been identified as a causal mechanism in sarcopenia development, representing a specific metabolic target for future interventions.
🔹 Mitochondrial dysfunction underlies many of the energy metabolism problems in sarcopenic muscle, affecting the cellular powerhouses that generate ATP.
🔹 Chronic low-grade inflammation (inflammaging) creates a hostile metabolic environment that accelerates muscle protein breakdown while inhibiting synthesis.
🔹 Multimodal interventions are most effective—combining nutritional optimization, progressive resistance exercise, and addressing underlying metabolic dysfunction provides the best outcomes.
🔹 Bioactive peptides from dietary proteins may offer benefits beyond their amino acid content, influencing muscle metabolism through signaling mechanisms.
🔹 Early intervention matters—the metabolic changes preceding visible muscle loss may be more easily reversed than established sarcopenia, emphasizing the importance of proactive muscle health maintenance.
🔹 Prevention is possible—sarcopenia is not an inevitable consequence of aging. Evidence-based strategies can maintain muscle health and metabolic function well into advanced age.
1. What Is Sarcopenia? A Modern Definition
The word "sarcopenia" comes from the Greek sarx (flesh) and penia (poverty or loss). But the clinical reality in 2025 is far richer than etymology suggests.
The European Working Group on Sarcopenia in Older People (EWGSOP2) defines sarcopenia as a progressive and generalized skeletal muscle disorder involving accelerated loss of muscle mass and function, associated with adverse outcomes including falls, functional decline, frailty, and premature mortality.
What has fundamentally changed in recent research is the why behind muscle loss. According to a landmark 2026 review by Nguyen et al. published in Endocrinology and Metabolism, sarcopenia involves coordinated failures across multiple molecular systems — not simply a slow erosion of tissue.
Sarcopenia is characterized by three overlapping deficits:
Low muscle mass — typically quantified by appendicular skeletal muscle index (ASMI) via DEXA scan or bioimpedance
Low muscle strength — most commonly assessed by handgrip dynamometry
Poor physical performance — measured by gait speed, 5-times sit-to-stand, or Short Physical Performance Battery (SPPB)
Critically, muscle mass alone is no longer considered sufficient for diagnosis. Strength and performance are now recognized as the more clinically meaningful outcomes — and they reflect the underlying metabolic health of muscle tissue more faithfully than mass alone.
Featured Snippet Answer: Sarcopenia is a progressive muscle disease characterized by low muscle mass, strength, and physical performance. It is driven by metabolic dysfunction including mitochondrial failure, disrupted amino acid metabolism, and chronic inflammation — and is now classified as a complex metabolic disorder, not merely an aging side effect.
2. How Common Is It? The Epidemiology
The global burden of sarcopenia is enormous — and rising.
Sarcopenia affects 10–27% of adults over age 60, with rates increasing sharply after 70
Muscle mass declines at approximately 3–8% per decade after age 30, accelerating after age 60
In hospitalized older adults and those with chronic disease, prevalence can exceed 50%
Sarcopenia is independently associated with increased risk of falls, fractures, hospitalization, and all-cause mortality
A 2026 prospective analysis published in BMC Geriatrics (Gao et al.) using the CHARLS cohort demonstrated that sarcopenia changes — even modest declines in muscle function — significantly predicted new-onset type 2 diabetes mellitus in older adults, underscoring the bidirectional relationship between muscle health and metabolic disease.
As global populations age, the economic and healthcare burden of untreated sarcopenia is projected to climb dramatically. Early identification and intervention are both medically justified and economically imperative.
3. Sarcopenia as a Metabolic Disease
The most important conceptual shift in the field is this: sarcopenia is not just a musculoskeletal disorder — it is a systemic metabolic disease.
Boccardi's (2024) influential paper in Mechanisms of Ageing and Development makes this case compellingly. Rather than viewing muscle wasting as the primary problem, Boccardi frames sarcopenia as the clinical manifestation of deep metabolic failures that impair how muscle cells produce energy, process nutrients, and renew themselves.
The 2026 comprehensive review by Mao et al. in Bone Research expands this framework to the full musculoskeletal system, identifying sarcopenia as part of a broader metabolic syndrome affecting muscle, bone, and connective tissue simultaneously.
The Metabolic Web of Sarcopenia
The major metabolic disruptions involved include:
Energy Metabolism
Mitochondrial dysfunction → reduced ATP production
Impaired substrate switching (metabolic inflexibility)
Reduced resting energy expenditure due to lower muscle mass
Nutrient Processing
Anabolic resistance to dietary protein
Disrupted branched-chain amino acid (BCAA) catabolism
Impaired lipid oxidation and intramuscular fat accumulation
Cellular Signaling
Dysregulated mTOR, AMPK, and insulin signaling
Elevated myostatin (a muscle growth inhibitor)
Blunted IGF-1 and growth hormone sensitivity
Inflammatory Environment
Chronic low-grade inflammation ("inflammaging")
Elevated IL-6, TNF-α, and C-reactive protein
NF-κB pathway activation promoting protein catabolism
Each disruption feeds the others. A decline in mitochondrial function, for instance, raises reactive oxygen species (ROS), which amplify inflammation, which suppresses anabolic signaling, which further impairs mitochondria — a self-reinforcing metabolic spiral.
4. The Lipid Connection: Fat Inside Your Muscle
One of the most striking findings in recent sarcopenia research involves fat — specifically, fat inside muscle tissue.
A 2025 study by Lal et al. published in BMC Biology investigated lipid metabolism in age-related musculoskeletal disorders. Their key discoveries:
Intramuscular Fat Infiltration ("Muscle Marbling")
As we age, lipid deposits accumulate within muscle fibers and between muscle cells — a phenomenon sometimes called myosteatosis or "muscle marbling." This is not the same as subcutaneous or visceral fat. It is fat that physically infiltrates the contractile machinery of muscle.
This intramuscular fat:
Directly impairs contractile force production
Contributes to local insulin resistance in muscle tissue
Replaces functional muscle fiber volume
Is associated with a higher risk of falls and mobility disability independent of total muscle mass
Impaired Fatty Acid Oxidation
Sarcopenic muscle also loses the ability to burn fat efficiently for fuel. Healthy muscle tissue is metabolically flexible — it can switch between carbohydrates, fats, and amino acids as fuel sources depending on the situation. Sarcopenic muscle becomes metabolically rigid: it cannot oxidize fatty acids effectively, creating a dual problem of energy deficit (can't use fat for fuel) and lipotoxicity (fat accumulates to harmful levels).
The Bone Connection
Lal et al. (2025) also demonstrated shared metabolic pathways between muscle lipid dysfunction and osteoporosis. The same lipid metabolic disruptions driving sarcopenia also impair bone mineral density maintenance — explaining why the two conditions so commonly coexist in the same patients.
Clinical Implication: Targeting lipid metabolism — through exercise, dietary fat quality, and potentially pharmacological agents — may simultaneously improve both muscle function and bone health.
5. The BCAA Breakthrough: Amino Acid Metabolism
Perhaps the most scientifically exciting development in sarcopenia research is the identification of disrupted branched-chain amino acid (BCAA) catabolism as a causal mechanism — not merely a symptom — of muscle loss.
The Landmark Zuo et al. 2025 Study
Using multi-omic profiling (genomics, transcriptomics, proteomics, and metabolomics combined), Zuo and colleagues published findings in Nature Aging (2025) that fundamentally reframe how we understand BCAA nutrition in sarcopenia.
What they found:
Sarcopenic muscle shows a profound impairment in BCAA catabolism — the biological pathways that break down and utilize the amino acids leucine, isoleucine, and valine. This is not caused by inadequate BCAA intake. Rather, the enzymatic machinery inside muscle cells (particularly BCAT2 and BCKDH complex enzymes) becomes dysfunctional with aging.
The consequences of impaired BCAA catabolism:
BCAA accumulation — Paradoxically, BCAAs build up to toxic levels inside muscle cells even as intake may be adequate
mTOR dysregulation — Chronic BCAA accumulation without proper catabolism disrupts mTOR signaling, the key anabolic switch
Insulin resistance — Accumulated BCAAs and their metabolic byproducts interfere with insulin receptor signaling
Energy deficits — BCAAs cannot serve as alternative fuel sources when catabolism is impaired, contributing to cellular energy crisis
What This Means for BCAA Supplementation
This discovery carries a nuanced and important message for practice:
Simply supplementing more BCAAs may not be the answer — and may even be counterproductive in individuals whose BCAA catabolism is already impaired. The priority should be restoring the metabolic capacity to process BCAAs, which is best achieved through progressive resistance training (which upregulates BCAA-catabolizing enzymes) and potentially through targeted nutritional strategies.
Using Mendelian Randomization for Causality
What distinguishes the Zuo study is the use of Mendelian randomization — a genetic analysis technique that establishes causal direction rather than mere correlation. Their analysis confirmed that BCAA catabolism impairment is not just associated with sarcopenia; it causes it. This is a crucial distinction that elevates BCAA metabolism from a biomarker to a therapeutic target.
6. Mitochondrial Dysfunction: The Energy Crisis
Mitochondria — the organelles that produce ATP (cellular energy) — are central actors in sarcopenia's metabolic story.
The 2026 review by Nguyen et al. in Endocrinology and Metabolism provides an updated molecular map of mitochondrial changes in aging muscle:
What Goes Wrong
Reduced mitochondrial biogenesis: The PGC-1α pathway, which drives new mitochondria formation, becomes blunted with age and inactivity
Impaired mitophagy: The quality-control process that removes damaged mitochondria (mitophagy) becomes dysfunctional, allowing accumulation of defective organelles
Increased ROS production: Aging mitochondria leak electrons, generating excessive reactive oxygen species that damage DNA, proteins, and membranes
Reduced NAD⁺ availability: NAD⁺, a critical coenzyme for mitochondrial function and the sirtuin longevity pathway, declines with age. This impairs SIRT1 and SIRT3 activity, further compromising mitochondrial quality
Reduced ATP output: The net result is chronic energy deficit in muscle cells, impairing both protein synthesis and contractile function
The NAD⁺ Connection
Recent translational research has highlighted NAD⁺ decline as a particularly important driver of sarcopenia-associated mitochondrial dysfunction. Preclinical studies suggest that NAD⁺ precursor supplementation (NMN or NR) can restore mitochondrial function and improve muscle performance in aged animals. Human trials are ongoing, with early results showing promise particularly for muscle endurance and metabolic flexibility.
Exercise as Mitochondrial Medicine
Progressive resistance training and high-intensity interval training (HIIT) are the most potent known stimulators of mitochondrial biogenesis in human muscle. Both exercise modalities activate PGC-1α and AMPK, driving production of new, functional mitochondria and improving NAD⁺ metabolism — effectively reversing age-related mitochondrial decline.
7. Inflammation and Hormonal Disruption
Inflammaging: The Slow Burn
Chronic low-grade inflammation — termed "inflammaging" — is a hallmark of aging and a key driver of sarcopenia. This isn't the acute inflammation of injury or infection, but a persistent, low-level inflammatory state that creates a catabolic muscle environment.
Key inflammatory mediators elevated in sarcopenia include:
IL-6 (Interleukin-6) — directly inhibits muscle protein synthesis and activates the ubiquitin-proteasome degradation system
TNF-α (Tumor Necrosis Factor-alpha) — promotes muscle cell apoptosis and insulin resistance
CRP (C-reactive protein) — a biomarker of systemic inflammation, elevated in sarcopenic individuals
IL-1β — activates NF-κB signaling, which upregulates muscle protein breakdown pathways
Adipose tissue — particularly visceral fat — is a major source of pro-inflammatory cytokines. This creates a vicious cycle: sarcopenia leads to fat gain (due to lower metabolic rate), fat gain increases inflammation, and inflammation accelerates sarcopenia.
Hormonal Decline
Muscle is an endocrine-responsive tissue. Multiple hormonal changes with aging conspire against muscle maintenance:
Here is the rewritten hormone section structured into clear, scannable points for both professional and patient-facing use.
Age-Related Hormonal Shifts and Muscle Decay
Testosterone (Declines ~1–2% per year after age 30)
The Damage: Directly reduces muscle protein synthesis and blunts the activation of satellite cells (the stem cells responsible for muscle repair and growth).
The Result: A steadily shrinking capacity to recover from minor tissue breakdown, leading to progressive muscle thinning.
IGF-1 & Growth Hormone (Significant decline after age 50)
The Damage: Impairs systemic anabolic signaling, severely limiting cellular regeneration and muscle hypertrophy (growth).
The Result: Muscles lose their ability to adapt to training stimuli, making it significantly harder to maintain or build new tissue even with dedicated effort.
DHEA (Declines ~2% per year after age 25)
The Damage: Weakens the foundational hormonal precursors required for local anabolic signaling within musculoskeletal tissues.
The Result: An early, silent shift toward a catabolic (breakdown-dominant) cellular environment long before physical weakness manifests.
Estrogen (Sharp decline at menopause)
The Damage: Removes a critical regulator of muscle quality, antioxidant protection, and stem cell function in women.
The Result: A sudden, accelerated loss of both muscle mass and structural strength immediately following menopause, independent of baseline activity levels.
Cortisol (Relatively elevated with aging)
The Damage: Shifts the overall metabolic balance toward protein catabolism (the active breakdown of muscle tissue into free amino acids).
The Result: A persistent, low-level hormonal "tax" that continuously erodes existing muscle fibers to fuel systemic stress responses.
Insulin Sensitivity (Decreases with age)
The Damage: Impairs the muscle's ability to pull glucose from the bloodstream and blunts the normal muscle-building response that occurs after eating.
The Result: Muscle tissue becomes starved of its primary fuel source, forcing the body to store excess energy as fat instead of utilizing it to sustain healthy muscle.These hormonal shifts are not irreversible. Exercise — particularly resistance training — can partially restore anabolic hormone sensitivity and reduce catabolic signaling even in older adults.
8. Sarcopenia and Type 2 Diabetes: A Two-Way Street
The relationship between sarcopenia and type 2 diabetes mellitus (T2DM) is one of the most clinically important connections in metabolic medicine.
How Sarcopenia Causes Diabetes
Skeletal muscle is the primary site of insulin-stimulated glucose disposal — responsible for approximately 80% of postprandial glucose uptake. When muscle mass declines and insulin resistance within muscle increases:
Glucose cannot be adequately cleared from the bloodstream
The pancreas compensates with higher insulin secretion
Eventually, β-cell capacity is exhausted and hyperglycemia develops
A landmark 2026 prospective cohort study by Gao et al. in BMC Geriatrics (CHARLS cohort) confirmed this pathway: individuals with sarcopenia at baseline had significantly higher rates of incident T2DM at follow-up, independent of body weight, age, and lifestyle factors.
How Diabetes Causes Sarcopenia
The relationship runs in reverse as well. T2DM promotes muscle loss through:
Hyperglycemia-induced oxidative stress damaging muscle fibers
Advanced glycation end products (AGEs) stiffen connective tissue and impair muscle function
Peripheral neuropathy reduces motor neuron stimulation of the muscle
Mitochondrial dysfunction caused by chronic metabolic stress
Chronic inflammation linked to metabolic dysregulation
This bidirectionality means that treating one condition without addressing the other is likely insufficient. An integrated metabolic approach targeting both conditions simultaneously is now considered best practice.
9. GLP-1 Receptor Agonists: New Hope for Muscle?
GLP-1 receptor agonists (GLP-1 RAs) — medications like semaglutide and liraglutide — have transformed the treatment of T2DM and obesity. But their effects on skeletal muscle are more complex, and a 2026 review in Diabetology & Metabolic Syndrome (Yang et al.) provides a critical analysis.
Potential Benefits for Sarcopenia
Emerging evidence suggests GLP-1 RAs may benefit muscle health through several mechanisms:
Improved insulin sensitivity — enhancing muscle glucose uptake and reducing glucotoxicity
Anti-inflammatory effects — reducing the systemic inflammation that drives muscle catabolism
Potential direct muscle signaling — GLP-1 receptors are expressed in skeletal muscle, suggesting direct anabolic or protective effects
Improved physical function — by reducing body weight and visceral fat, GLP-1 RAs may improve the fat-to-muscle ratio and functional capacity
A Critical Caution: Muscle Mass Loss
Here is the important nuance that clinicians and patients must understand: GLP-1 RA-induced weight loss includes lean mass loss, not just fat loss. Studies suggest that 25–40% of weight lost with semaglutide comes from lean (muscle) tissue, not fat.
This means:
GLP-1 RAs without concurrent resistance training may worsen sarcopenia in vulnerable older adults
The combination of GLP-1 RA therapy + structured resistance exercise is likely necessary to preserve muscle during pharmacological weight loss
Protein intake must be optimized (≥1.2 g/kg/day) during GLP-1 RA treatment
Clinical Bottom Line: GLP-1 RAs are not a muscle-sparing therapy on their own. Their use in patients at risk for sarcopenia should always be accompanied by a comprehensive muscle-preservation strategy.
10. Sarcopenia and Diabetic Foot: An Overlooked Risk
A 2026 narrative review in Frontiers in Endocrinology (Sui et al.) highlights a clinically underappreciated connection: sarcopenia significantly increases the risk of diabetic foot complications.
The mechanisms include:
Reduced lower limb muscle mass impairs plantar pressure distribution, increasing ulceration risk
Loss of intrinsic foot and lower leg muscle leads to foot deformity (Charcot-like changes)
Sarcopenia-associated poor balance and gait abnormalities increase fall and trauma risk
Impaired wound healing due to reduced muscle-derived growth factor signaling
Sarcopenic individuals have poorer outcomes after diabetic foot interventions
This finding reinforces the need for routine sarcopenia screening in all patients with diabetes, particularly those with peripheral neuropathy or a history of foot complications.
11. Diagnosis: How Sarcopenia Is Detected
Standard Diagnostic Approach (EWGSOP2 Algorithm)
Step 1 – Find (Screening)
SARC-F questionnaire (5-item, validated self-report tool)
Any score ≥4/10 warrants further evaluation
Step 2 – Assess (Confirm)
Handgrip strength: <27 kg (men), <16 kg (women) = low muscle strength
Chair stand test: >15 seconds for 5 stands = low muscle performance
Step 3 – Confirm
DXA scan or bioelectrical impedance (BIA) to quantify muscle mass
ASMI cutoffs: <7.0 kg/m² (men), <5.5 kg/m² (women)
Step 4 – Severity
Severe sarcopenia = low muscle mass + low strength + low physical performance
Emerging Diagnostic Tools
Ali et al. (2024) in the Canadian Journal of Physiology and Pharmacology highlight next-generation diagnostic approaches:
Metabolomic biomarker panels — measuring circulating BCAA metabolites, acylcarnitines, and inflammatory markers to detect pre-sarcopenic metabolic changes before muscle loss occurs
Muscle ultrasound — assessing muscle thickness, cross-sectional area, and echogenicity (a measure of intramuscular fat infiltration)
Muscle quality MRI — quantifying intramuscular fat content with high precision
Phase angle (BIA) — a direct measure of cellular membrane integrity and hydration; a lower phase angle is associated with sarcopenia and poor outcomes
12. Evidence-Based Treatment Strategies
Sarcopenia requires a multimodal intervention strategy — no single treatment is sufficient because no single mechanism explains the full pathology.
The evidence supports five major therapeutic pillars:
Pillar 1: Progressive Resistance Training (PRT)
Pillar 2: Protein Optimization
Pillar 3: Targeted Supplementation
Pillar 4: Aerobic and Combined Exercise
Pillar 5: Management of Underlying Metabolic Conditions
Each is detailed in the sections below.
13. The Optimal Sarcopenia Nutrition Protocol
Total Protein: How Much?
Current evidence strongly supports higher protein intake in older adults:
Minimum: 1.2 g/kg body weight/day (vs. the 0.8 g/kg RDA for general adults)
Optimal for sarcopenia prevention/treatment: 1.2–1.5 g/kg/day
During active resistance training: Up to 1.6–2.0 g/kg/day may be beneficial
For a 70 kg person: This equals 84–105 g of protein daily (optimal range)
Protein Distribution: Timing Matters
Older muscle exhibits anabolic resistance — it requires a larger protein stimulus to trigger muscle protein synthesis (MPS) than younger muscle. Key principles:
Distribute protein across 3–4 meals rather than consuming most at dinner
Each main meal should provide 25–40 g of high-quality protein to maximally stimulate MPS
Leucine threshold: Each meal should deliver ≥2.5–3 g of leucine, as leucine is the primary amino acid trigger for mTOR activation and MPS
Protein Quality: Not All Proteins Are Equal
Protein Source Leucine Content Digestibility MPS Stimulation Whey protein High (11%) Very high Excellent Egg white High (8.8%) High Excellent Meat/poultry High (8–9%) High Very good Fish High (8–9%) High Very good Soy protein Moderate (7.8%) High Good Casein Moderate (9%) Slow Good (sustained) Legumes Lower (6–8%) Moderate Moderate Plant blends Variable Variable Good (when combined)
Beyond Protein: Key Nutrients for Sarcopenia
Omega-3 Fatty Acids (EPA/DHA)
Reduce intramuscular inflammation
Improve muscle membrane fluidity and receptor sensitivity
Dose: 2–4 g/day of EPA+DHA from fish oil
Evidence: Multiple RCTs show improvement in MPS response and physical function
Vitamin D
Vitamin D deficiency is extremely common (>50% of older adults) and independently associated with muscle weakness and falls
Vitamin D receptors are present in muscle cells; deficiency impairs calcium handling and contractile function
Target serum 25(OH)D: >75 nmol/L (30 ng/mL)
Dose: 1,000–2,000 IU/day; higher doses (up to 4,000 IU/day) may be needed to correct deficiency
Creatine Monohydrate
Increases intramuscular phosphocreatine stores, improving high-intensity exercise capacity
Combined with resistance training, consistently improves muscle mass and strength gains
Dose: 3–5 g/day (no loading phase required for older adults)
Well tolerated, including in older adults with normal renal function
HMB (Beta-hydroxy beta-methylbutyrate)
A leucine metabolite that reduces muscle protein breakdown (anticatabolic)
Particularly useful during periods of inactivity, illness, or caloric restriction
Dose: 3 g/day (1 g with each meal)
A Sample One-Day Meal Plan for Sarcopenia
Breakfast (30g protein)
3 whole eggs scrambled + 1 cup Greek yogurt (plain, full-fat) + berries + 1 tbsp ground flaxseed
Mid-Morning (optional)
Whey protein smoothie (25g protein) with frozen berries and almond butter
Lunch (35g protein)
150g grilled salmon + large salad with olive oil + ½ cup lentils + whole grain bread
Dinner (35g protein)
150g chicken breast or lean beef + roasted vegetables in olive oil + 1 cup quinoa
Evening (optional)
1 cup cottage cheese (slow-digesting casein protein — excellent pre-sleep option)
Total: ~125–140g protein, ~1.8 g/kg for a 70 kg person
14. The Best Exercise Program for Sarcopenia
Progressive Resistance Training (PRT): The Gold Standard
PRT is the most evidence-supported intervention for sarcopenia — not simply because it builds muscle mass, but because it repairs the underlying metabolic dysfunction:
Stimulates mitochondrial biogenesis via PGC-1α and AMPK
Upregulates BCAA catabolic enzymes (BCAT2, BCKDH), restoring proper amino acid metabolism
Reduces intramuscular fat infiltration
Improves insulin sensitivity and glucose uptake
Reduces systemic inflammation (exercise has potent anti-inflammatory effects)
Restores anabolic hormone sensitivity
Sample Resistance Training Protocol
Frequency: 3 sessions/week (e.g., Monday, Wednesday, Friday)
Intensity: Progressive overload — start at 60–70% of 1-rep max, increase by 5% when current load becomes easy
Volume: 2–4 sets × 8–12 repetitions per exercise
Recommended Exercises:
Here is the exercise guide organized by muscle group and options:
Legs / Glutes
Options: Leg press, goblet squat, step-ups, hip thrust
Back
Options: Seated row, lat pulldown, dumbbell row
Chest
Options: Dumbbell press (floor or bench), push-up variations
Shoulders
Options: Overhead press, lateral raises
Core
Options: Dead bug, plank, bird dog
Functional
Options: Farmer's carry, suitcase carry, balance exercisesKey Principles:
Always warm up for 5–10 minutes
Focus on proper form over heavy weight, particularly initially
Work with a certified trainer if new to resistance training
Progress load, not just repetitions
Include functional movements that mimic daily activities
Aerobic Training: The Mitochondrial Booster
Aerobic exercise complements resistance training by:
Improving cardiovascular function and endurance
Enhancing mitochondrial function and oxidative capacity
Reducing visceral adiposity and systemic inflammation
Improving insulin sensitivity
Recommendation: 150 minutes/week of moderate-intensity aerobic exercise (brisk walking, cycling, swimming, dancing), or 75 minutes of vigorous-intensity exercise, in addition to resistance training.
High-Intensity Interval Training (HIIT):
2×/week, 20–30 minute sessions
Particularly effective for mitochondrial biogenesis in older adults
Should be progressed carefully — consult a healthcare provider if you have cardiovascular risk factors
The Combined Training Protocol (Most Effective)
Based on current evidence, a combined resistance + aerobic training program produces superior outcomes compared to either alone:
Maximizes muscle mass gains AND metabolic improvements
Improves both strength and cardiovascular fitness
Provides greater reduction in inflammatory biomarkers
Produces the best functional outcomes (walking speed, chair-stand time, balance)
15. Supplements: What the Evidence Says
Creatine monohydrate
Evidence Level: Strong (A)
Key Effect: Increases muscle mass and strength when paired with progressive resistance training (PRT)
Recommended Dose: 3–5 g/day
Vitamin D
Evidence Level: Strong (A)
Key Effect: Supports overall muscle function and aids in fall prevention
Recommended Dose: 1,000–4,000 IU/day
Omega-3 (EPA+DHA)
Evidence Level: Moderate (B)
Key Effect: Reduces inflammation and improves muscle protein synthesis (MPS)
Recommended Dose: 2–4 g/day
HMB
Evidence Level: Moderate (B)
Key Effect: Acts as an anticatabolic agent, reducing muscle breakdown
Recommended Dose: 3 g/day
Leucine/EAAs
Evidence Level: Moderate (B)
Key Effect: Stimulates muscle protein synthesis (especially helpful if overall protein intake is low)
Recommended Dose: 3 g of leucine per meal
Whey protein
Evidence Level: Strong (A)
Key Effect: Provides convenient, high-quality protein delivery to muscles
Recommended Dose: 25–40 g post-exercise
Collagen peptides
Evidence Level: Emerging (C)
Key Effect: May support and repair muscle connective tissue
Recommended Dose: 15 g post-exercise
NMN/NR (NAD+ precursors)
Evidence Level: Emerging (C)
Key Effect: Supports mitochondrial function and cellular energy
Recommended Dose: 250–500 mg/day
Magnesium
Evidence Level: Moderate (B)
Key Effect: Supports muscle function (highly beneficial as it is a common dietary deficiency)
Recommended Dose: 300–400 mg/day
Zinc
Evidence Level: Moderate (B)
Key Effect: Supports protein synthesis and healthy hormone production
Recommended Dose: 10–15 mg/day
Evidence levels: A = multiple RCTs/meta-analyses; B = some RCTs or consistent observational data; C = preclinical or early human data only
⚠️ Important: Always consult your healthcare provider before starting any supplement regimen, especially if you take medications or have underlying health conditions.
16. Common Myths and Mistakes About Sarcopenia
Myth 1: "Sarcopenia is inevitable — you can't stop it."
Reality: While some muscle decline with age is normal, sarcopenia is a disease state that is largely preventable and partially reversible. Multiple RCTs demonstrate meaningful improvements in muscle mass, strength, and function with appropriate intervention at virtually any age.
Myth 2: "Just eat more protein — that's all you need."
Reality: Protein quality, distribution, and timing matter as much as total quantity. And in individuals with impaired BCAA catabolism (common in sarcopenia), simply adding more protein may not translate to anabolic benefit. The cellular machinery to process protein must be functional — which is where exercise becomes critical.
Myth 3: "BCAA supplements will fix my muscle loss."
Reality: The Zuo et al. (2025) discovery of impaired BCAA catabolism means that in sarcopenic individuals, BCAAs may actually accumulate to toxic levels. Supplementation without addressing the metabolic machinery is potentially counterproductive. Resistance training is the most powerful tool to restore BCAA-processing enzymes.
Myth 4: "Cardio is the best exercise for aging."
Reality: While cardiovascular exercise has important benefits, progressive resistance training is the most evidence-supported intervention for sarcopenia. A combined approach is optimal, but if forced to prioritize, resistance training takes precedence.
Myth 5: "Sarcopenia only affects very old or frail people."
Reality: The metabolic changes predisposing to sarcopenia begin as early as the third decade of life. Proactive muscle preservation starting in your 30s and 40s dramatically reduces risk of clinically significant sarcopenia in later life.
Myth 6: "GLP-1 medications will improve my muscle health while I lose weight."
Reality: GLP-1 receptor agonists cause significant lean mass loss alongside fat loss. Without concurrent resistance training and adequate protein intake, GLP-1 therapy can worsen sarcopenia in vulnerable individuals.
Myth 7: "Supplements can replace exercise."
Reality: No supplement produces the metabolic benefits of exercise. Creatine, whey protein, and vitamin D all show their strongest effects in combination with resistance training. Supplements are adjuncts, not substitutes.
17. Study Evidence Summary
1. BCAA & Protein Quality
Zuo et al. (2025) | Nature Aging
Finding: Disrupted BCAA (branched-chain amino acid) catabolism (breakdown) is a causal mechanism in sarcopenia.
Implication: BCAA metabolism is a clear therapeutic target; progressive resistance training (PRT) helps restore this metabolic pathway.
Naumovski et al. (2025) | J Cachexia Sarcopenia
Finding: Bioactive peptides derived from dietary proteins actively modulate muscle metabolism.
Implication: The quality and specific source of dietary protein matter, not just the raw amino acid content.
2. Muscle-Bone Crosstalk & Lipid Metabolism
Lal et al. (2025) | BMC Biology
Finding: Dysfunctional lipid (fat) metabolism is a primary driver of both sarcopenia and osteoporosis.
Implication: Interventions that target lipid metabolism have the potential to preserve both muscle and bone health simultaneously.
Mao et al. (2025) | Bone Research
Finding: Sarcopenia is not isolated; it actively impacts the entire musculoskeletal system.
Implication: Clinical management requires an integrated muscle-bone treatment approach.
3. Diabetes & Metabolic Complications
Gao et al. (2026) | BMC Geriatrics
Finding: Sarcopenic changes are strong predictors of developing Type 2 Diabetes (T2DM), as observed in the CHARLS cohort.
Implication: Routine screening for sarcopenia should be implemented for pre-diabetic and metabolic syndrome patients.
Yang et al. (2026) | Diabetol Metab Syndr
Finding: GLP-1 receptor agonists (RAs) offer mixed results—providing metabolic benefits but posing a significant risk for lean mass loss.
Implication: GLP-1 therapy should always be paired with progressive resistance training and optimized protein intake to protect muscle mass.
Sui et al. (2026) | Front. Endocrinol.
Finding: Sarcopenia stands out as a significant risk factor for developing diabetic foot complications.
Implication: Sarcopenia screening should be mandatory for all patients presenting with diabetic foot issues.
4. Evidence-Based Interventions & Multimodal Care
Boccardi (2024) | Mech. Ageing Dev.
Finding: Sarcopenia is a complex, multi-system metabolic disease.
Implication: No single therapy works in isolation; patients require combined, multimodal interventions involving exercise, nutrition, and pharmacology.
Chen & Wu (2024) | Aging and Disease
Finding: Mapping the metabolic fingerprint of sarcopenia points toward specific, evidence-based management strategies.
Implication: Clinical protocols should aim for 1.2–1.5 g/kg/day of protein, progressive resistance training 2–3× per week, alongside evidence-backed supplementation with creatine and vitamin D.
5. Cellular Mechanisms & Biomarkers
Nguyen et al. (2026) | Endocrinol Metab
Finding: Updated molecular frameworks highlight the roles of NAD⁺ depletion and impaired mitophagy (the clearing of damaged mitochondria).
Implication: NAD⁺ precursors are emerging as viable therapeutic targets, alongside therapies designed to enhance mitophagy.
Ali et al. (2024) | Can J Physiol Pharmacol
Finding: Sarcopenia presents with distinct, updated metabolic alterations and emerging biomarkers.
Implication: Utilizing targeted metabolomic panels in clinical settings may allow for much earlier detection of the disease.
18. Frequently Asked Questions
Q1: What are the first signs of sarcopenia I should watch for?
Early signs include difficulty with tasks that were previously easy — carrying groceries, rising from a chair, and climbing stairs without holding the rail. Declining grip strength, noticeably slower walking pace, and increased fatigue with physical activity are also early indicators. The SARC-F questionnaire (available online) is a validated 5-question screening tool. Any score ≥4 warrants evaluation by a healthcare provider.
Q2: At what age does sarcopenia typically begin?
Muscle mass begins declining around age 30, at a rate of approximately 3–8% per decade. This accelerates significantly after age 60. However, the metabolic changes predisposing to sarcopenia (mitochondrial decline, increasing insulin resistance, reduced anabolic hormone sensitivity) can begin in the 30s and 40s. This makes proactive muscle health strategies relevant at any adult age, not just in older adults.
Q3: Can sarcopenia be reversed?
Yes — partially and meaningfully. Studies consistently show that resistance training and protein optimization can increase muscle mass, strength, and function in sarcopenic individuals, including those in their 80s and beyond. Full reversal to youthful muscle biology is not achievable, but the trajectory of decline can be substantially altered, and functional capacity can be meaningfully improved at any stage.
Q4: Is sarcopenia the same as frailty?
They are related but distinct. Sarcopenia refers specifically to loss of muscle mass, strength, and performance. Frailty is a broader clinical syndrome encompassing sarcopenia plus exhaustion, unintentional weight loss, slow gait speed, and low physical activity. Sarcopenia is a major contributor to frailty, and the two conditions commonly coexist — but frailty involves additional physiological systems beyond skeletal muscle.
Q5: How does menopause affect sarcopenia risk in women?
Menopause significantly accelerates sarcopenia risk. Estrogen has direct anabolic effects on skeletal muscle, promotes satellite cell activity, and reduces systemic inflammation. The sharp decline in estrogen at menopause removes these protective effects, and women can lose up to 3% of muscle mass per year in the first 3–5 years post-menopause. This makes the perimenopausal period a critical window for intervention. Resistance training and protein optimization are particularly important for women during and after this transition.
Q6: What blood tests can detect sarcopenia or its metabolic drivers?
No single blood test diagnoses sarcopenia. However, useful biomarkers to assess the metabolic context include: 25-hydroxyvitamin D (muscle function), testosterone and IGF-1 (anabolic hormones), C-reactive protein and IL-6 (inflammaging), HbA1c and fasting glucose (insulin resistance), creatinine/cystatin C (muscle mass proxy), and albumin (protein status and inflammation). Research-grade metabolomic panels measuring BCAA metabolites and acylcarnitines are emerging but not yet standard clinical tools.
Q7: Is sarcopenia linked to dementia or cognitive decline?
Yes. Growing evidence suggests skeletal muscle loss is associated with accelerated cognitive decline and dementia risk. Proposed mechanisms include: reduced production of muscle-derived neuroprotective factors (irisin, BDNF), shared inflammatory pathways, and the cardiovascular consequences of physical deconditioning. This bidirectional brain-muscle connection is an active area of research and reinforces the systemic importance of muscle health.
Q8: Can plant-based diets support muscle health for people concerned about sarcopenia?
Yes, with careful planning. The key challenge on a plant-based diet is achieving adequate leucine per meal (≥2.5g) from lower-leucine plant protein sources. Strategies include: consuming larger portions of protein-rich plants (legumes, tofu, tempeh, seitan), combining complementary proteins, and using plant-based protein powders (soy, pea+rice blend) to supplement intake. Monitoring B12, zinc, omega-3s, and vitamin D is also essential. Plant-based eaters may benefit from slightly higher total protein intakes (1.4–1.6 g/kg/day) to compensate for lower digestibility.
Q9: Does poor sleep affect sarcopenia?
Significantly. Poor sleep quality and short sleep duration are independently associated with reduced muscle mass and strength. Sleep is when the majority of growth hormone secretion occurs — a key anabolic driver of muscle protein synthesis. Sleep disruption also elevates cortisol (catabolic) and systemic inflammation. Targeting 7–9 hours of quality sleep per night should be considered part of any sarcopenia management strategy.
Q10: How long before I see results from exercise and nutrition interventions?
Functional improvements (strength, balance, walking speed) typically begin within 4–8 weeks of consistent resistance training. Meaningful increases in muscle mass as measured by DEXA usually become apparent at 8–12 weeks. The most important thing is consistency — the benefits compound over months and years. Studies in octogenarians show that even individuals in their 80s and 90s achieve significant strength gains within 8–12 weeks of structured PRT.
Q11: Should I be concerned about protein intake if I have kidney disease?
Yes — this is an important clinical nuance. In individuals with chronic kidney disease (CKD), higher protein intakes must be approached cautiously, as excess protein metabolism generates nitrogenous waste that compromised kidneys cannot adequately excrete. For people with CKD, sarcopenia management should be guided by a nephrologist and registered dietitian, and protein recommendations are individualized based on kidney function stage. This represents a genuine therapeutic tension between muscle preservation and kidney protection.
Q12: What role does gut health play in sarcopenia?
The gut-muscle axis is an emerging area of significant scientific interest. The gut microbiome influences sarcopenia through multiple mechanisms: modulating systemic inflammation, affecting amino acid absorption and bioavailability, producing short-chain fatty acids (SCFAs) with anabolic signaling properties, and regulating nutrient sensing pathways. Dysbiosis (disrupted gut microbiome composition) is associated with increased sarcopenia risk. Dietary strategies supporting gut health — high fiber intake, fermented foods, diverse plant consumption — may offer an additional layer of protection against muscle loss.
19. Clinical Pearls
The Leucine Threshold vs. Total Protein Volume: Due to age-related anabolic resistance, older adults require a higher peak plasma concentration of essential amino acids to activate the mTORC1 pathway. Simply meeting a daily macro target is insufficient. Clinicians should prescribe protein distributed into explicit boluses of 25–40 g per meal, ensuring each exposure hits the 2.5–3.0 g leucine threshold required to trigger muscle protein synthesis (MPS).
The BCAA Paradox (De-prescribing Isolated Supplements): Multi-omic data (Zuo et al., 2025) demonstrates that the enzymatic machinery for branched-chain amino acid degradation (specifically BCAT2 and the BCKDH complex) is down-regulated in sarcopenic muscle. Because isolated BCAA supplements can cause an accumulation of toxic intermediates and worsen insulin resistance when catabolism is blocked, clinicians should prioritize progressive resistance training to upregulate these enzymes rather than prescribing free-form amino acid concentrates.
Mandatory Co-Prescription with GLP-1 Receptor Agonists: When utilizing GLP-1 receptor agonists (e.g., semaglutide) in older adults or those with metabolic syndrome, weight loss should not be monitored in isolation. Because up to 40% of the mass lost can originate from lean skeletal tissue, a concurrent prescription of progressive resistance training (2 days/week) and elevated protein (1.2 g/kg/day) is medically necessary to prevent inducing or worsening sarcopenic obesity.
Muscle is Your Body’s "Sugar Sink": Think of your skeletal muscle as the main reservoir that clears sugar from your bloodstream after you eat. When you lose muscle mass to sarcopenia, you lose your primary storage space for glucose. This directly forces your pancreas to work harder, pushing you toward type 2 diabetes. Protecting your muscles isn't just about looking fit; it's about maintaining your body's built-in defense system against blood sugar spikes.
The Danger of "Muscle Marbling": Just like a premium cut of steak, an aging muscle that isn't regularly challenged can become marbled with microscopic fat deposits (a process called myosteatosis). This fat doesn't just sit there; it actively crowds out healthy muscle fibers, reduces your physical power, and causes local inflammation. The most effective way to "melt" this internal fat and restore muscle density is through targeted weight training.
Exercise Unlocks the Power of Your Food: Eating high-quality protein is only half the battle. If your muscle cells have become inactive, they lose the tools needed to properly absorb and utilize those nutrients. Lifting weights acts as the cellular key that turns these processing tools back on. Protein cannot effectively rebuild your body until exercise signals the muscle cells to open their doors.
20. Conclusion and Action Plan
The New Paradigm
Sarcopenia is no longer just "getting old and losing muscle." It is a complex metabolic disease with identified molecular mechanisms — disrupted BCAA catabolism, lipid infiltration, mitochondrial failure, inflammatory excess, and hormonal decline — that can be targeted with evidence-based precision.
The research of 2024–2026 has given us a more complete map of why muscles fail with aging, and a clearer roadmap for what to do about it. The answers are not simple, but they are actionable.
Your 5-Step Action Plan
Step 1: Screen and assess. Use the SARC-F questionnaire. Discuss muscle mass testing (BIA or DEXA) with your doctor, especially if you're over 50, have T2DM, or have experienced unexplained weight loss or weakness.
Step 2: Start resistance training. This is non-negotiable. Three sessions per week of progressive resistance training, targeting all major muscle groups, is the single most powerful intervention available for sarcopenia. Start today, at whatever level you're at.
Step 3: Optimize your protein. Aim for 1.2–1.5 g/kg/day of high-quality protein, distributed across 3–4 meals with at least 25–30g per meal. Prioritize leucine-rich sources. If you're on a GLP-1 medication, this is especially critical.
Step 4: Address your deficiencies. Have your vitamin D, magnesium, and zinc levels checked. Add omega-3 fatty acids (2–4 g EPA+DHA/day) and consider creatine monohydrate (3–5 g/day) in consultation with your healthcare provider.
Step 5: Manage metabolic co-conditions. If you have diabetes, obesity, chronic inflammation, or hormonal imbalances, work with your healthcare team to optimize these — they all directly accelerate sarcopenia.
Sarcopenia is not inevitable. Your muscles are metabolic organs, and like all organs, they respond to how you treat them. The evidence is clear: move progressively, eat purposefully, supplement smartly, and manage your metabolic health holistically. The results can be transformative at any age
Disclaimer: This article is intended for educational and informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional before making changes to your exercise, nutrition, or supplementation regimen, particularly if you have existing health conditions or take medications
Related Articles
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
Sarcopenia in Diabetes: Managing Muscle Loss with Chronic Disease | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
Best Exercises for Sarcopenia: Strength Training Guide for Older Adults | DR T S DIDWAL
Best Supplements for Sarcopenia: Vitamin D, Creatine, and HMB Explained | DR T S DIDWAL
References
Ali, S. R., Nkembo, A. T., Tipparaju, S. M., Ashraf, M., & Xuan, W. (2024). Sarcopenia: Recent advances for detection, progression, and metabolic alterations along with therapeutic targets. Canadian Journal of Physiology and Pharmacology, 102(12), 697–708. https://doi.org/10.1139/cjpp-2024-0201
Bauer, J. M., Verlaan, S., Bautmans, I., Brandt, K., Donini, L. M., Maggio, M., & Sieber, C. C. (2015). Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults. Journal of the American Medical Directors Association, 16(9), 740–747. https://doi.org/10.1016/j.jamda.2015.03.013
Boccardi, V. (2024). Sarcopenia: A dive into metabolism to promote a multimodal, preventive, and regenerative approach. Mechanisms of Ageing and Development, 219, Article 111941. https://doi.org/10.1016/j.mad.2024.111941
Chen, Y., & Wu, J. (2024). Aging-related sarcopenia: Metabolic characteristics and therapeutic strategies. Aging and Disease, 16(2), 1003–1022. https://doi.org/10.14336/AD.2024.0407
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., & Zamboni, M. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Dent, E., Morley, J. E., Cruz-Jentoft, A. J., Arai, H., Kritchevsky, S. B., Guralnik, J., & Cederholm, T. (2018). International clinical practice guidelines for sarcopenia (ICFSR): Screening, diagnosis and management. Journal of Nutrition, Health & Aging, 22(10), 1148–1161. https://doi.org/10.1007/s12603-018-1139-9
Gao, L., Chen, Y., Su, S., et al. (2026). Sarcopenia changes and incident type 2 diabetes mellitus: A prospective analysis of the CHARLS cohort. BMC Geriatrics, 26, Article 556. https://doi.org/10.1186/s12877-026-07169-4
Lal, S., Gunji, S., Ahluwalia, P., Patil, R., Singh, S., Akbare, S., Limaye, S., Vishwanatha, J. K., & Banerji, D. (2025). Lipid metabolism in age-related musculoskeletal disorders: Insights into sarcopenia and osteoporosis. BMC Biology, 23, Article 265. https://doi.org/10.1186/s12915-025-02383-9
Mao, X., Lv, K., Qi, W., et al. (2025). Research progress on sarcopenia in the musculoskeletal system. Bone Research, 13, Article 78. https://doi.org/10.1038/s41413-025-00455-8
Naumovski, P., De Spiegeleer, B., Wakjira, A., Van De Wiele, C., Mouly, V., Goljanek-Whysall, K., Da Costa, K. S., De Oliveira, E. C. L., Wynendaele, E., & De Spiegeleer, A. (2025). Role of peptides in skeletal muscle wasting: A scoping review. Journal of Cachexia, Sarcopenia and Muscle, 16(6), Article e70109. https://doi.org/10.1002/jcsm.70109
Nguyen, T. T., Dao, T., Nguyen, H. T., Park, J. H., Jeong, S. J., Kim, S., Jo, Y., Thieu, N. T. H., Zhao, J., Ding, F., Yu, Y., Dung, V. C., Gariani, K., Kim, B. J., & Ryu, D. (2026). Sarcopenia and muscle aging: Updated insights into molecular mechanisms and translational therapeutics. Endocrinology and Metabolism, 41(1), 57–85. https://doi.org/10.3803/EnM.2025.2656
Smith, G. I., Atherton, P., Reeds, D. N., Mohammed, B. S., Rankin, D., Rennie, M. J., & Mittendorfer, B. (2011). Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults. The American Journal of Clinical Nutrition, 93(2), 402–412. https://doi.org/10.3945/ajcn.110.005611
Stout, J. R., Antonio, J., & Castalaneta, D. (2023). Creatine supplementation in healthy aging adults: A systematic review. Journal of the International Society of Sports Nutrition, 20(1). https://doi.org/10.1186/s12970-023-00602-4
Sui, Y., Ma, Y., Zhou, K., Liang, R., & Liu, X. (2026). A narrative review on the correlation between diabetic foot and sarcopenia. Frontiers in Endocrinology, 17, Article 1711060. https://doi.org/10.3389/fendo.2026.1711060
Yang, Q., Wang, Y., Gao, G., et al. (2026). Research progress on the molecular mechanism and clinical evidence of glucagon-like peptide-1 receptor agonists in improving sarcopenia. Diabetology & Metabolic Syndrome, 18, Article 118. https://doi.org/10.1186/s13098-026-02133-z
Zuo, X., Zhao, R., Wu, M., Wang, M., Zhao, Z., Jia, S., Sun, L., Qi, Y., Fan, W., Ruan, Q., Zhang, X., Deng, L., Song, W., Zou, L., Yan, M., Tian, Q., Jin, Y., Yu, Z., & Shen, B. (2025). Multi-omic profiling of sarcopenia identifies disrupted branched-chain amino acid catabolism as a causal mechanism and therapeutic target. Nature Aging, 5, 419–436. https://doi.org/10.1038/s43587-024-00797-8
This article was last reviewed and updated in June 2026 to incorporate the most recent peer-reviewed evidence.