Is Resistance Training Safe and Effective for Cardiovascular Patients? A Clinical Guide
Resistance training is essential for heart patients. Learn how strength training improves blood pressure, metabolism, and cardiovascular outcomes safely.
EXERCISEHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/5/202615 min read
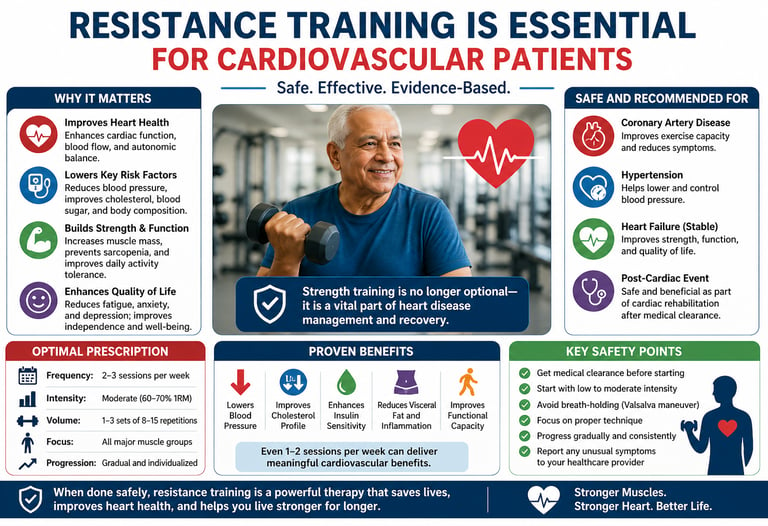
Resistance training is now a core, evidence-based therapy for patients with cardiovascular disease—not just a fitness option. It improves functional capacity, reduces cardiovascular risk factors, enhances quality of life, and is considered safe when properly prescribed and supervised.
Major guidelines, including those from the American Heart Association, recommend incorporating resistance exercise into cardiac rehabilitation and long-term cardiovascular care.
Why Resistance Training Matters in Heart Disease
For patients with cardiovascular conditions, resistance exercise provides multisystem benefits:
Improves functional capacity → better ability to perform daily activities
Lowers blood pressure → supports hypertension control
Enhances glucose metabolism → critical in diabetes and insulin resistance
Reduces visceral fat and inflammation → key drivers of atherosclerosis
Improves muscle strength and prevents sarcopenia → linked to lower mortality
Enhances quality of life and mental health
In many patients, improved muscle strength translates directly into better survival and independence.
Is Resistance Training Safe for Cardiac Patients?
Yes—in most stable patients, resistance training is safe and beneficial when appropriately prescribed.
It is now routinely recommended for:
Coronary artery disease (CAD)
Controlled hypertension
Stable heart failure
Post-myocardial infarction (after medical clearance)
Cardiac rehabilitation programs
Key requirement: Individualized assessment, gradual progression, and avoidance of improper techniques (e.g., breath-holding).
Optimal Prescription for Cardiovascular Patients
Frequency: 2–3 sessions per week
Intensity: Moderate (≈60–70% of one-repetition maximum)
Volume: 1–3 sets of 8–15 repetitions
Focus: All major muscle groups
Progression: Gradual, supervised in early phases
Even low volumes (1–2 sessions/week) provide meaningful cardiovascular benefits.
Beyond Fitness: A Therapeutic Intervention
Resistance training is not just supportive—it acts as a biological therapy by:
Improving endothelial function
Reducing sympathetic overactivity
Lowering systemic inflammation
Potentially modifying gene expression linked to cardiac health
This positions resistance exercise alongside lifestyle medicine and pharmacotherapy in modern cardiovascular care.
While strong evidence supports benefits across risk factors and functional outcomes, much of the long-term outcome data is derived from observational and interventional studies. Exercise prescriptions should always be individualized based on clinical status.
Bottom Line
For cardiovascular patients, resistance training is essential—not optional.
When performed safely, even two sessions per week can improve strength, reduce risk factors, and enhance long-term heart health and quality of life.
Resistance training is not only safe but highly beneficial for most patients with cardiovascular disease.
Once viewed with caution, strength training is now strongly recommended by major guidelines, including the American Heart Association. When properly prescribed, it improves blood pressure, insulin sensitivity, lipid profile, muscle mass, functional capacity, and quality of life — while reducing cardiovascular risk.
Key Evidence-Based Benefits:
Lowers resting blood pressure and systemic inflammation
Improves glucose control and reduces visceral fat
Prevents sarcopenia and enhances cardiac rehabilitation outcomes
Provides benefits even with low volume (2 sessions per week)
Safety Profile: Resistance training is safe for stable patients with coronary artery disease, controlled hypertension, and heart failure when introduced gradually with proper breathing technique and medical clearance.
Bottom Line: Resistance training should be considered an essential — not optional — component of modern cardiovascular care. Combined with aerobic exercise, it offers powerful, complementary protection for the heart and overall metabolic health.
This post brings together the most current peer-reviewed research on resistance exercise and cardiovascular health. Whether you are a healthy adult wanting to protect your heart, someone managing cardiovascular risk factors, or a patient recovering from a cardiac event, this comprehensive guide is for you. Let's look at what the science says, how much exercise you actually need, and how to get started safely.
What Is Resistance Exercise? A Quick Primer
Resistance exercise (RE) refers to any physical activity that causes your muscles to contract against an external force — such as free weights, resistance bands, weight machines, or even your own body weight. Unlike aerobic exercise, which primarily trains your cardiovascular and respiratory systems through sustained rhythmic movement, resistance training focuses on muscular strength, endurance, and power.
Common forms include:
Free weights (dumbbells, barbells, kettlebells)
Weight machines (gym equipment with guided resistance)
Bodyweight exercises (push-ups, squats, lunges, planks)
Resistance bands (elastic bands providing variable tension)
Functional training (movements mimicking daily life activities)
For years, the concern was that resistance training might harm the heart — that the sharp spikes in blood pressure during heavy lifting could be dangerous. Modern research has thoroughly dismantled that concern, replacing it with a far more optimistic picture.
The Cardiovascular Benefits of Resistance Exercise
1. Blood Pressure Reduction
Hypertension — high blood pressure — is one of the most dangerous and pervasive cardiovascular risk factors in the world. It silently damages arteries over years, setting the stage for heart attack, stroke, and heart failure. Resistance training has been shown to lower both resting systolic and diastolic blood pressure, particularly in individuals with elevated readings (Dores et al., 2024; Nazir et al., 2024).
The mechanism involves several pathways: improved arterial elasticity, reduced sympathetic nervous system activity at rest, and enhanced endothelial function (the health of the inner lining of blood vessels). Over time, regular resistance training makes your blood vessels more responsive, flexible, and efficient.
2. Improved Cholesterol and Lipid Profiles
Dyslipidaemia — abnormal levels of cholesterol and triglycerides in the blood — is another major cardiovascular risk factor. Resistance training has been found to reduce LDL ("bad") cholesterol and triglyceride levels while modestly raising HDL ("good") cholesterol (Oude et al., 2025). These changes collectively reduce the risk of atherosclerosis, the buildup of fatty plaques in arteries that underlie most heart attacks and strokes.
3. Blood Sugar Control and Insulin Sensitivity
Diabetes and pre-diabetes dramatically increase the risk of cardiovascular disease. Resistance training improves insulin sensitivity and glucose metabolism by building skeletal muscle — the body's primary tissue for glucose uptake. More muscle mass means better blood sugar regulation, reducing the long-term cardiovascular damage associated with high blood glucose (Dores et al., 2024; Johnson, 2026).
A systematic review and meta-analysis published in the European Heart Journal Open confirmed that resistance training produces clinically meaningful improvements in glycaemic control across diverse populations, with effects comparable to first-line pharmacological interventions in some cases (de Oude et al., 2025).
4. Weight Management and Reduced Visceral Fat
Obesity — particularly visceral (abdominal) fat — is strongly linked to inflammation, high blood pressure, dyslipidaemia, and type 2 diabetes. While aerobic exercise is often emphasised for weight loss, resistance training offers a powerful complementary approach. It increases resting metabolic rate by building muscle tissue, which burns more calories at rest than fat tissue. Over months of consistent training, this metabolic advantage contributes significantly to weight management (Nazir et al., 2024; Johnson, 2026).
5. Reduced Inflammation
Chronic low-grade inflammation underlies many cardiovascular diseases. Resistance training has been shown to reduce inflammatory biomarkers such as C-reactive protein (CRP) and interleukin-6 (IL-6), suggesting it has genuine anti-inflammatory effects beyond simply improving physical fitness (Dores et al., 2024).
6. Heart Structure and Function
Beyond risk factors, resistance training appears to make beneficial adaptations within the heart itself. It promotes moderate left ventricular remodelling, improves cardiac output, and may enhance heart rate variability — a marker of autonomic nervous system health closely linked to reduced cardiovascular mortality (Dores et al., 2024).
How Much Is Enough? The Optimal Dose of Resistance Exercise
One of the most important practical questions for patients and clinicians alike is: how much resistance exercise do you actually need to protect your heart?
The answer, according to a landmark analysis by Lee and Lee (2023) published in Current Cardiology Reports, is that even small amounts produce substantial cardiovascular benefits — and the relationship between dose and benefit is not strictly linear. Specifically:
As little as 1–2 sessions per week of resistance training produced significant reductions in cardiovascular mortality and all-cause mortality risk.
Benefits appeared to plateau at approximately 60 minutes of resistance training per week in terms of cardiovascular mortality risk reduction.
More is not always better: extremely high volumes of resistance training (>140 minutes/week) showed diminishing returns and, in some analyses, a slight attenuation of the protective effect.
This "sweet spot" finding is critically important for patients who feel overwhelmed by the prospect of committing to a demanding exercise regimen. Two sessions per week of 30 minutes each — achievable even for busy adults — appear sufficient to meaningfully lower heart disease risk.
The American Heart Association's 2023 Scientific Statement on resistance training (Paluch et al., 2024), published in Circulation, recommends that adults perform muscle-strengthening activities involving all major muscle groups at least two days per week, alongside moderate aerobic exercise, as part of a comprehensive cardiovascular health strategy. The statement notes the strong evidence base for resistance training in both primary prevention (protecting healthy individuals) and secondary prevention (supporting patients who already have cardiovascular disease).
A systematic review and meta-analysis in the European Heart Journal Open further clarified that moderate intensity resistance training (approximately 60–79% of one-repetition maximum) consistently produced the best cardiovascular risk factor outcomes, outperforming both low-intensity and very high-intensity regimens in most measured parameters (de Oude et al., 2025).
Resistance Training for People Already Living With Heart Disease
Here is perhaps the most transformative finding of recent cardiovascular research: resistance training is not only safe for most people with established heart disease — it is actively beneficial.
For decades, patients recovering from cardiac events were advised to avoid strenuous exertion. That advice has been substantially revised. The AHA's 2023 Scientific Statement (Paluch et al., 2024) states explicitly that resistance exercise training is safe and effective for individuals with a wide range of cardiovascular conditions, including:
Coronary artery disease (CAD): A comprehensive review by Nazir et al. (2025) in the Journal of Multidisciplinary Healthcare found that resistance exercise is a safe and effective modality for improving quality of life in CAD patients. It improved functional capacity, reduced anxiety and depression, enhanced musculoskeletal health, and — crucially — did not significantly increase adverse cardiac events when appropriate precautions were taken.
Heart failure: Supervised resistance training improves exercise tolerance, muscle strength, and quality of life in stable heart failure patients.
Hypertension: As noted above, resistance training is now considered a lifestyle intervention that can contribute meaningfully to blood pressure management alongside or in place of some medications.
Post-cardiac surgery: Cardiac rehabilitation programmes increasingly incorporate resistance training components, recognising its role in restoring strength, confidence, and cardiovascular function.
The key qualifier throughout the literature is appropriate supervision and progression, especially in the early stages. Patients with known heart disease should consult their cardiologist or cardiac rehabilitation specialist before starting a resistance training programme, and ideally begin under supervised conditions.
Absolute Contraindications for Resistance Training
Resistance training should not be initiated if a patient presents with any of the following:
Unstable Cardiovascular Conditions: Unstable angina, uncontrolled symptomatic heart failure, or uncontrolled high-grade arrhythmias.
Severe Valvular Disease: Severe symptomatic aortic stenosis.
Acute Inflammatory Conditions: Acute myocarditis, pericarditis, or endocarditis.
Uncontrolled Hypertension: Resting systolic BP >180 mmHg or diastolic BP >110 mmHg.
Aortic Complications: Known or suspected dissecting aneurysm or Marfan syndrome (due to the risk of aortic rupture during pressure spikes).
Recent Acute Events: Major cardiac events (e.g., MI or surgery) before receiving specific clearance from a cardiologist (typically 2–6 weeks depending on the procedure).
Clinical Rule of Thumb: If a patient is not yet stable enough for light aerobic activity (like slow walking), they are not yet a candidate for resistance training. Always prioritize hemodynamic stability before adding external load.
The Epigenetic Revolution: How Resistance Training Rewires Your Heart at the Molecular Level
Perhaps the most fascinating frontier in resistance exercise research is epigenetics — the study of how gene expression is modified without changes to the underlying DNA sequence. A landmark paper by Silva et al. (2026) in Frontiers in Physiology explored how resistance training regulates cardiovascular health through epigenetic mechanisms, including:
DNA methylation changes that silence pro-inflammatory and pro-fibrotic genes in cardiac tissue
Histone modifications that promote the expression of cardioprotective proteins
MicroRNA regulation that fine-tunes pathways involved in cardiac remodelling, angiogenesis (new blood vessel growth), and cellular survival
These findings indicate that when you lift weights consistently, you are not simply building muscles — you are fundamentally altering how your heart and blood vessels express their genetic blueprints. This may explain why the cardiovascular benefits of resistance training persist over time and seem to extend well beyond simple mechanical improvements in fitness.
This epigenetic lens opens exciting possibilities for precision medicine, where exercise "prescriptions" might one day be tailored based on an individual's epigenetic profile to maximise cardiovascular benefit.
Breaking the Sedentary Cycle: Why Resistance Training Is a Public Health Priority
Sedentary behaviour has been called "the new smoking" in public health circles, and with good reason. Prolonged sitting and physical inactivity are independently associated with elevated risks of cardiovascular disease, metabolic syndrome, and premature death.
Johnson (2026), writing in Current Epidemiological Reports, argues that resistance training deserves specific emphasis in public health strategies to combat sedentariness — not just aerobic exercise recommendations. The reasons are compelling:
Resistance training can be performed in short bouts (even 10–15 minutes), making it more accessible to those who struggle with sustained aerobic activity
It builds the muscular strength needed to remain physically active in daily life as people age
It addresses sarcopenia (age-related muscle loss), which independently predicts cardiovascular morbidity and mortality in older adults
It improves psychological wellbeing, motivation, and self-efficacy, potentially creating a positive feedback loop that sustains long-term physical activity
As Dores et al. (2024) emphasise in Revista Portuguesa de Cardiologia, the time has come for clinicians to move beyond vague recommendations to "exercise more" and toward specific, individualised resistance exercise prescriptions — just as they prescribe medications with specific doses, frequencies, and durations.
Practical Applications: How to Start Resistance Training for Heart Health
Getting Started Safely
Before beginning a resistance training programme — especially if you have known cardiovascular risk factors or established heart disease — speak with your doctor or a qualified exercise professional. A basic fitness assessment can identify any limitations and help create a safe, effective programme.
For beginners (weeks 1–4): Start with bodyweight exercises (squats, modified push-ups, glute bridges) or light resistance bands. Focus on learning correct form. Aim for 2 sessions per week, 20–30 minutes each.
Building up (weeks 5–12): Gradually introduce dumbbells or weight machines. Perform 2–3 sets of 8–15 repetitions per exercise. Include exercises for all major muscle groups (legs, hips, back, abdomen, chest, shoulders, arms). Allow at least 48 hours of recovery between sessions targeting the same muscle groups.
Ongoing maintenance: Aim for 2–3 sessions per week at moderate intensity (you should feel challenged but able to maintain proper form throughout). Progressively increase resistance by approximately 5–10% once you can comfortably complete the upper end of your target repetition range.
Sample Beginner Cardiovascular-Focused Workout (30 minutes)
Bodyweight Squats or Leg Press
Volume: 2–3 sets
Reps: 12–15
Rest: 60 seconds
Focus: Strengthens the lower body and improves circulation.
Dumbbell Chest Press or Push-ups
Volume: 2–3 sets
Reps: 10–12
Rest: 60 seconds
Focus: Targets chest and arms; modify push-ups on knees or a wall if needed.
Seated Row or Resistance Band Row
Volume: 2–3 sets
Reps: 12–15
Rest: 60 seconds
Focus: Improves posture and strengthens the upper back.
Dumbbell Shoulder Press
Volume: 2 sets
Reps: 10–12
Rest: 60 seconds
Focus: Builds functional overhead strength.
Plank (Core Stability)
Volume: 2 sets
Duration: 20–30 second hold
Rest: 45 seconds
Focus: Stabilizes the spine and strengthens the abdominal wall.
Glute Bridge
Volume: 2 sets
Reps: 15
Rest: 45 seconds
Focus: Activates the glutes and supports lower back health.
Quick Safety Tips
Keep Breathing: Exhale during the "work" part of the move and inhale as you return to the start.
Form First: Use a weight that allows you to complete all reps with control.
Warm Up: Always start with 5 minutes of light walking or dynamic stretching.
Warning Signs to Watch For
Stop exercising and seek medical attention if you experience: chest pain or pressure, unusual shortness of breath, dizziness or lightheadedness, palpitations or irregular heartbeat, or sudden severe fatigue during exercise.
Frequently Asked Questions (FAQs)
Q1: Is resistance training safe if I have high blood pressure? Yes — for most people with hypertension, resistance training is not only safe but actively recommended. It has been shown to reduce resting blood pressure over time (Nazir et al., 2024; de Oude et al., 2025). However, avoid breath-holding (the Valsalva manoeuvre) during exertion, as this can cause sharp temporary blood pressure spikes. If your blood pressure is very high (above 160/100 mmHg), consult your doctor before starting.
Q2: I had a heart attack six months ago. Can I do resistance training? Many post-heart attack patients benefit significantly from resistance training as part of a supervised cardiac rehabilitation programme (Nazir et al., 2025; Paluch et al., 2024). Always get clearance from your cardiologist first, begin under professional supervision, and start at a low intensity. The evidence strongly supports supervised resistance training for improving quality of life, functional capacity, and psychological wellbeing in this population.
Q3: How many days per week do I need to lift weights for heart health benefits? Even one to two sessions per week produces meaningful cardiovascular risk reduction, with the greatest benefits seen at approximately two sessions per week (Lee & Lee, 2023). More is not necessarily better — consistency matters far more than volume. Two 30-minute sessions weekly is an achievable and evidence-supported goal.
Q4: Should I do resistance training instead of — or in addition to — cardio? Both forms of exercise offer unique and complementary cardiovascular benefits. The AHA recommends combining resistance training with aerobic exercise for optimal cardiovascular health (Paluch et al., 2024). If time is limited, even replacing some sedentary time with resistance training confers significant benefits. The ideal programme includes both.
Q5: Does the type of resistance exercise matter for heart health? The specific mode (free weights, machines, bands, bodyweight) matters less than the principles of progressive overload, sufficient intensity, and training all major muscle groups. Moderate intensity (60–79% of maximum effort) appears to produce the best cardiovascular risk factor outcomes (de Oude et al., 2025). Choose whatever form you enjoy most and can sustain long-term.
Q6: Can resistance training actually change my genes? Research shows that resistance training modifies gene expression through epigenetic mechanisms — including DNA methylation, histone modification, and microRNA regulation — without altering the DNA itself (Silva et al., 2026). These changes promote cardioprotective pathways, reduce inflammation, and improve cardiac remodelling over time. You cannot change the genes you inherited, but you can significantly influence how they are expressed.
Q7: I am older and worried about injuring myself. Is resistance training still appropriate? Resistance training is especially important for older adults, for whom muscle loss (sarcopenia) is a major driver of cardiovascular risk and functional decline. Start slowly with light weights or bands, prioritise form over load, and consider working with a physiotherapist or certified fitness professional initially. The benefits — improved strength, balance, metabolic health, and cardiovascular protection — are well established in older populations.
Clinical Pearls
1. The "Sweet Spot" for Longevity
Scientific Perspective: The dose-response curve for RT and cardiovascular mortality is non-linear (U-shaped). Data suggests a "sweet spot" at approximately 60 minutes per week. Exceeding 140 minutes per week may lead to diminishing returns or attenuation of the protective benefit, likely due to excessive systemic stress or arterial stiffening in specific populations.
You don’t need to live in the gym to save your life. Just two 30-minute sessions a week provides nearly the maximum heart-protection benefit. More isn't always better; consistency beats intensity every time.
2. Myokines vs. Cytokines (The Anti-Inflammatory Shield)
Scientific Perspective: RT functions as a "biological therapy" by stimulating skeletal muscle to release myokines (e.g., IL-6 during acute exercise), which counteract pro-inflammatory cytokines like CRP. This shift reduces chronic low-grade inflammation, a primary driver of atherosclerosis and endothelial dysfunction.
Muscle is more than just "meat"—it’s a chemical factory. When you lift weights, your muscles release natural "medicine" into your bloodstream that fights inflammation and cleans up the "rust" inside your arteries.
3. Epigenetic "Rewiring" of Cardiac Fate
Scientific Perspective: RT induces specific DNA methylation and histone modifications that silence pro-fibrotic genes and upregulate cardioprotective pathways. This suggests that RT-induced adaptations are not merely mechanical (stronger pump) but molecular (better "software" instructions for the heart).
You aren't stuck with the hand you were dealt. Even if heart disease runs in your family, lifting weights can actually "flip the switches" on your genes, telling your body to stay healthy rather than following a blueprint for disease.
4. Sarcopenia as a Cardiovascular Risk Factor
Scientific Perspective: Skeletal muscle is the body's largest site for glucose disposal. The age-related loss of muscle (sarcopenia) creates a metabolic "sink-hole," leading to insulin resistance and increased visceral fat. Preserving muscle mass via RT is therefore a metabolic necessity for heart failure and diabetic patients.
Building muscle isn't about looking like a bodybuilder; it’s about giving your blood sugar a place to go. If you lose muscle as you age, your heart has to work twice as hard to manage your metabolism. Stronger legs mean a stronger heart.
5. Safety through the "Pressor Response" Management
Scientific Perspective: While RT causes a transient increase in blood pressure (the pressor response), it is generally safe for stable CAD/HF patients. The clinical priority is avoiding the Valsalva maneuver (breath-holding), which can cause dangerous spikes in intrathoracic pressure. Proper "exhale on exertion" technique keeps the hemodynamic load manageable.
The "grunt and hold your breath" style of lifting is dangerous for your heart. As long as you keep breathing (exhale while you lift, inhale while you lower), the temporary pressure on your heart is safe and actually helps your blood vessels become more flexible over time.
Author’s Note
As clinicians, we are trained to prioritise pharmacological precision in cardiovascular care—yet one of the most powerful interventions remains underprescribed: resistance training. The evolving body of evidence no longer supports viewing strength training as optional or secondary. Instead, it should be regarded as a foundational pillar of cardiovascular prevention and rehabilitation.
This article was written to bridge the persistent gap between exercise science and clinical cardiology. While aerobic exercise continues to receive deserved emphasis, resistance training uniquely addresses muscle loss, metabolic dysfunction, and functional decline—all of which are strongly linked to adverse cardiovascular outcomes but often overlooked in routine practice.
Importantly, the goal is not to replace existing therapies, but to integrate resistance exercise into standard care, much like we would prescribe antihypertensives or statins—appropriately dosed, individualised, and monitored.
For patients, the message is equally important: improving heart health does not always require extreme effort or complex routines. Small, consistent steps—such as two structured sessions per week—can produce meaningful, measurable benefits.
The future of cardiovascular care lies in combining molecular science, clinical medicine, and lifestyle intervention. Resistance training sits precisely at that intersection.
This content is intended for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Resistance training should be individualized based on clinical status, especially in patients with cardiovascular disease. Always consult a qualified healthcare professional before starting or modifying an exercise program, particularly if you have existing heart conditions, symptoms, or risk factors.
Related Articles
HIIT for Athletes: Boost VO₂ Max, Lactate Threshold, and Peak Performance – Science-Based Guide
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
References
de Oude, K. I., Elbers, R. G., Gerger, H., Maes-Festen, D. A. M., & Oppewal, A. (2025). The effect of different resistance exercise training intensities on cardiovascular risk factors: A systematic review and meta-analysis. European Heart Journal Open, 5(5), oeaf093. https://doi.org/10.1093/ehjopen/oeaf093
Dores, H., Antunes, M., Caldeira, D., & Pereira, H. V. (2024). Cardiovascular benefits of resistance exercise: It's time to prescribe. Revista Portuguesa de Cardiologia, 43(10), 573–582. https://doi.org/10.1016/j.repc.2024.02.009
Johnson, M. A. (2026). Breaking the sedentary cycle: The role of resistance training in cardiovascular health and disease prevention. Current Epidemiological Reports, 13, 10. https://doi.org/10.1007/s40471-026-00390-0
Lee, D. C., & Lee, I. M. (2023). Optimum dose of resistance exercise for cardiovascular health and longevity: Is more better? Current Cardiology Reports, 25, 1573–1580. https://doi.org/10.1007/s11886-023-01976-6
Nazir, A., Heryaman, H., Juli, C., Ugusman, A., Martha, J. W., Moeliono, M. A., & Atik, N. (2024). Resistance training in cardiovascular diseases: A review on its effectiveness in controlling risk factors. Integrated Blood Pressure Control, 17, 21–37. https://doi.org/10.2147/IBPC.S449086
Nazir, A., Heryaman, H., Juli, C., Ugusman, A., Martha, J. W., Moeliono, M. A., & Atik, N. (2025). Resistance exercise as a safe modality for quality of life improvement in patients with coronary artery diseases: A review. Journal of Multidisciplinary Healthcare, 18, 2813–2823. https://doi.org/10.2147/JMDH.S516441
Paluch, A. E., et al. (2024). Resistance exercise training in individuals with and without cardiovascular disease: 2023 update — A scientific statement from the American Heart Association. Circulation, 149(3), e217–e231. https://doi.org/10.1161/CIR.0000000000001189
Silva, J. G., Rodrigues, L. F., Torres, T., Improta-Caria, A. C., Oliveira, E. M., & Fernandes, T. (2026). Resistance training and cardiovascular health: Epigenetic regulation. Frontiers in Physiology, 16, 1701689. https://doi.org/10.3389/fphys.2025.1701689