Inflammation and Prediabetes: Can hs-CRP Predict Whether You'll Develop Diabetes?
Prediabetes involves more than elevated glucose. Learn how chronic inflammation measured by hs-CRP influences diabetes progression and heart health.
DIABETES
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/12/202620 min read
High-sensitivity C-reactive protein (hs-CRP) is a blood test that measures low-grade inflammation. Research shows that people with prediabetes and elevated hs-CRP are more likely to progress to type 2 diabetes, while those with lower hs-CRP have a greater chance of returning to normal blood sugar. Because chronic inflammation contributes to insulin resistance and cardiovascular disease, hs-CRP can help identify higher-risk individuals when interpreted alongside HbA1c, fasting glucose, HDL cholesterol, triglycerides, and other metabolic markers. Lifestyle measures such as weight loss, regular exercise, healthy sleep, and an anti-inflammatory diet can help lower inflammation and improve metabolic health.
Key takeaways
1. It’s Not Just a Heart Marker—It Forecasts Your Blood Sugar Path
While doctors traditionally look at high-sensitivity C-reactive protein (hs-CRP) to evaluate cardiovascular risk, recent studies show it acts like a compass for your metabolism. Your level of cellular inflammation helps predict whether your prediabetes is likely to reverse back to normal or progress toward type 2 diabetes.
2. Low Inflammation Gives You a Clear Green Light for Reversal
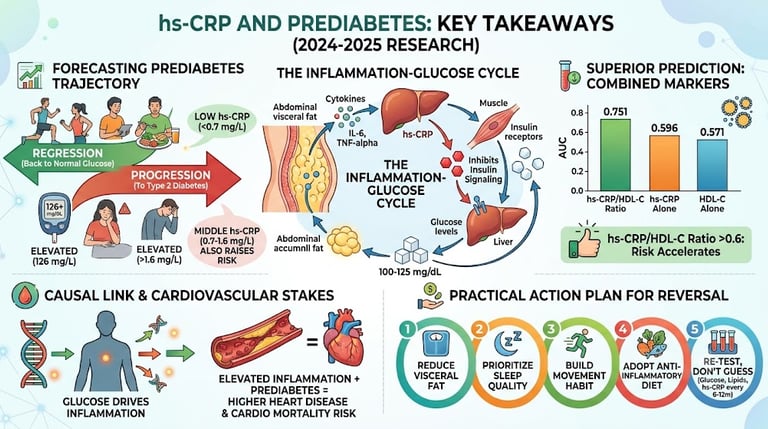
There is incredibly hopeful news in the data: prediabetes is highly fluid, not a permanent diagnosis. In major multi-year tracking studies, roughly two-thirds of people with prediabetes successfully reversed their blood sugar back to a completely healthy range. Having a low baseline hs-CRP (specifically below 0.7 mg/L was one of the strongest indicators that a person’s body was primed for full metabolic recovery.
3. Elevated hs-CRP Meaningfully Increases Progression Risk
If your chronic background inflammation is elevated, it acts like a headwind against your metabolic recovery. According to robust cohort data, individuals with prediabetes who had mid-to-high hs-CRP levels (ranging from 0.67 mg/L up to and exceeding 1.62 mg/Lfaced a 63% to 85% higher likelihood of developing type 2 diabetes over four years compared to those with low baseline inflammation.
4. Glucose and Inflammation Fuel a Two-Way Vicious Cycle
Genetic data (Mendelian randomization studies) reveal that this relationship isn't just a random coincidence. Elevated blood sugar levels actively cause your body's inflammatory response to spike. This creates a self-reinforcing loop: extra blood glucose triggers inflammation, and that inflammation blocks your insulin receptors, causing blood glucose to rise even higher.
5. Power-Pairing Markers Gives a Far More Accurate Picture
Looking at your hs-CRP value entirely by itself only tells a partial story. Combining your inflammation score with your lipid panel provides a much sharper diagnostic tool. Specifically, tracking the hs-CRP/HDL-C ratio outperforms either test alone in predicting metabolic health, with risk accelerating significantly once the ratio crosses a threshold of roughly 0.6 for prediabetes.
6. High Inflammation Plus Prediabetes Raises the Cardiac Stakes
When low-grade chronic inflammation and impaired fasting glucose occur together, they have a compounding, "supra-additive" effect on your cardiovascular system. This combination quietly accelerates plaque buildup in your arteries. Data shows individuals in the highest tiers of systemic inflammation experience a 50% higher risk of ischemic heart disease, meaning metabolic recovery is vital for your heart, not just your blood sugar.
7. Never Panic Over a Single "Bad" Reading
An isolated high hs-CRP score is never a definitive verdict. Because this protein is a highly sensitive responder to any acute stressor, your number can skyrocket temporarily due to a minor cold, a hard workout, a poor night's sleep, a minor injury, or a recent vaccination. Doctors always look for a sustained trend over multiple tests spaced months apart rather than reacting to one blood draw.
8. Your Action Plan Moves the Needle on Both Numbers Simultaneously
The exact same lifestyle modifications that calm your immune system's inflammatory response also happen to restore your insulin sensitivity. You don't need a separate strategy for each issue. Addressing visceral abdominal fat, protecting deep sleep quality, adopting a colorful Mediterranean-style dietary pattern rich in omega-3s and fiber, and building a consistent movement routine will drive down both your blood sugar and your hs-CRP at the exact same time.
If you've just seen the words "prediabetes" on a lab report, you probably have one urgent question: will this turn into type 2 diabetes, or can I still turn it around?
A blood marker most people have never heard of — high-sensitivity C-reactive protein (hs-CRP) — may hold part of the answer. hs-CRP is a simple, inexpensive marker of low-grade inflammation, and a growing body of 2024–2025 research shows it does more than flag heart disease risk. It appears to help determine which direction your blood sugar is heading.
1. What Is hs-CRP, and Why Does It Matter for Blood Sugar?
C-reactive protein is produced by your liver in response to inflammation anywhere in the body. The "high-sensitivity" (hs) version of the test can detect much lower concentrations than a standard CRP test, which makes it useful for picking up the low-grade, chronic inflammation associated with obesity, insulin resistance, and early metabolic disease — not just acute infection.
Typical hs-CRP risk categories used in cardiometabolic research:
Here is the breakdown of the hs-CRP risk categories and their general interpretations presented in a clear, scannable format:
Low Risk
hs-CRP Level: Less than 1.0 mg/L
General Interpretation: Indicates a low level of background inflammation in the body.
Average / Moderate Risk
hs-CRP Level: 1.0 to 3.0 mg/L
General Interpretation: Indicates a moderate level of background inflammation.
High Risk
hs-CRP Level: Greater than 3.0 mg/L
General Interpretation: Indicates elevated background inflammation.
Chronic low-grade inflammation is now considered a core driver — not just a bystander — of insulin resistance and pancreatic beta-cell dysfunction. Inflammatory signaling molecules interfere directly with the insulin receptor pathway, while HDL cholesterol (which normally has anti-inflammatory, antioxidant, and insulin-sensitizing properties) becomes less protective when inflammation is high, according to research summarized in a 2025 NHANES analysis.
This is why hs-CRP has moved from being "just a heart disease marker" to being studied as a genuine predictor of glucose trajectory — the direction someone's blood sugar is heading, not just where it stands today.
2. The Core Science: hs-CRP Predicts Whether Prediabetes Progresses or Regresses
This is the single most clinically important finding in this space, and it comes from a 2024 prospective cohort study published in the Journal of Diabetes Investigation.
The CHARLS Study: A 4-Year Look at Prediabetes Trajectories
Researchers followed 2,874 middle-aged and older adults with prediabetes from the China Health and Retirement Longitudinal Study (CHARLS) for four years, measuring hs-CRP at baseline and then reassessing glucose status. At follow-up:
1,894 people (66%) regressed back to normal blood sugar
834 people (29%) remained in the prediabetes range
146 people (5%) progressed to full type 2 diabetes
The critical discovery: hs-CRP level at baseline predicted which of these three paths a person was likely to take. Compared with people in the lowest hs-CRP tertile (under 0.67 mg/L):
People in the middle tertile (0.67–1.62 mg/L) had 85% higher odds of progressing to diabetes (odds ratio 1.85)
People in the high tertile (above 1.62 mg/L) had 63% higher odds of progression (odds ratio 1.63)
Both middle and high hs-CRP groups had 21–23% lower odds of regressing back to normal glucose
In plain language: low hs-CRP wasn't just "not harmful" — it was actively associated with a much greater chance of the prediabetes reversing on its own. These results held up even after the researchers controlled for age, sex, BMI, hypertension, heart disease, and cholesterol problems, and remained consistent across subgroups.
Confirmed in an Even Larger Cohort
A 2025 analysis from the Kailuan Study, a real-world cohort of over 82,000 Chinese adults followed for a median of 11 years, reinforced this pattern at scale. Diabetes incidence was clearly higher among people with elevated inflammation — roughly 90 new cases per 1,000 person-years among those with hs-CRP at or above 2 mg/L, compared to about 67 per 1,000 person-years in those with lower inflammation. Impaired fasting glucose and elevated hs-CRP each independently raised diabetes risk, and having both together raised it more than either alone — a "supra-additive" effect.
CRP as an Early Warning Sign, Even Before Formal Prediabetes Criteria Are Met
A 2024 case-control style study from Northern Clinics of Istanbul examined patients with impaired fasting glucose and found that elevated CRP (above roughly 0.8 mg/L) was significantly more common among people trending toward impaired fasting glucose than among those with completely normal glucose — about 1 in 5 people in the impaired-glucose group had high CRP, versus roughly 1 in 6 in the normal group. The authors concluded that clinicians should treat an elevated CRP as a signal to look more closely for early glucose dysregulation, describing it as a potential early warning sign worth acting on rather than dismissing.
Clinical takeaway: if your hs-CRP is elevated and you're prediabetic, that combination should be read as a meaningfully worse prognosis than prediabetes with a normal hs-CRP — not a coincidental extra number on your lab report.
3. Beyond hs-CRP Alone: Combination Markers That Sharpen the Picture
Because hs-CRP reflects only one piece of metabolic dysfunction (inflammation), researchers have started pairing it with lipid and insulin-resistance markers to build sharper predictive tools. Two combinations stand out.
hs-CRP/HDL-C Ratio
A 2025 cross-sectional study using NHANES data from 2015–2023 examined 18,472 U.S. adults, including 7,696 with prediabetes and 2,329 with diabetes. It found that:
Each one-unit rise in the hs-CRP/HDL-C ratio was linked to 13.3% higher odds of prediabetes and 26.9% higher odds of diabetes, after adjusting for a long list of confounders (age, sex, blood pressure, BMI, lipids, smoking, activity level, and more).
People in the top quartile of the ratio had roughly double the odds of prediabetes and nearly 3.7 times the odds of diabetes compared with the bottom quartile.
The relationship wasn't a straight line — it was a nonlinear, threshold-based relationship, with the association becoming much steeper once the ratio crossed roughly 0.6 (for prediabetes) or 1.2 (for diabetes) in the fully adjusted model.
Most notably, the combined ratio out-predicted either marker alone: the area under the curve (a measure of how well a test discriminates between people with and without a condition, where 1.0 is perfect and 0.5 is no better than chance) was 0.751 for prediabetes using the ratio, versus only 0.596 for hs-CRP alone and 0.571 for HDL-C alone. For diabetes, the ratio reached an AUC of 0.857.
A related 2025 study of nearly 11,000 adults with diabetes or prediabetes found that a higher CRP/HDL-C ratio was also independently associated with a substantially greater prevalence of hyperuricemia (high uric acid) — prevalence climbed from about 18% in the lowest ratio quartile to nearly 30% in the highest, pointing to shared inflammatory and metabolic roots between dysglycemia, dyslipidemia, and uric acid problems.
hs-CRP Combined With the TyG Index
The triglyceride-glucose (TyG) index is a simple, validated surrogate marker for insulin resistance, calculated from fasting triglycerides and glucose. A 2025 nine-year longitudinal study of 4,483 Chinese adults (also from CHARLS) examined hs-CRP and the TyG index together and found that people with both an elevated TyG index and elevated hs-CRP had a substantially higher risk of developing "cardiometabolic multimorbidity" — meaning two or more of diabetes, hypertension, high lipids, heart disease, or stroke — compared to people with only one marker elevated or neither. The authors concluded that assessing the two markers jointly gave a more complete risk picture than using either one in isolation, supporting combined inflammatory–metabolic screening as a more effective primary-prevention strategy.
Why this matters practically: if you only get a CRP test and it comes back "borderline," pairing it mentally (or with your doctor) against your HDL cholesterol and triglyceride/glucose numbers gives a far more accurate risk signal than the CRP value alone.
4. Why This Matters for Your Heart, Not Just Your Blood Sugar
Prediabetes and inflammation don't just raise future diabetes risk — together they raise cardiovascular risk right now, and there's genetic evidence suggesting this isn't just correlation.
A landmark 2024 study published in Cardiovascular Diabetology combined standard observational data with Mendelian randomization — a method that uses naturally occurring genetic variation to test whether a risk factor is likely to be a true cause of disease, rather than just associated with it — across more than 112,000 people from Danish cohorts, plus summary genetic data from hundreds of thousands more.
Key findings:
People in the top 20% of CRP levels had a 50% higher risk of ischemic heart disease and a more than doubled risk of cardiovascular death compared with those with lower CRP.
The Mendelian randomization analysis supported a causal link running from higher blood glucose toward higher CRP — in other words, hyperglycemia appears to drive inflammation, not simply accompany it.
Elevated CRP, hyperglycemia, and diagnosed type 2 diabetes each independently added to cardiovascular risk, meaning the combination of prediabetes-range glucose and high inflammation is not simply additive risk on paper — it reflects a genuinely reinforcing biological process.
This helps explain why prediabetes shouldn't be thought of as a purely glycemic issue. When hs-CRP is also elevated, it's a signal that the same inflammatory process quietly damaging insulin signaling may also be accelerating atherosclerosis.
5. How to Interpret Your Own hs-CRP Result
Here is the simplified framework for interpreting an hs-CRP reading alongside prediabetes
Below ~0.7 mg/L (Optimistic/Low Risk)
What Research Suggests: This level is associated with the highest rates of blood sugar reversing back to normal (regression) and the lowest odds of progressing to type 2 diabetes.
Suggested Next Step: Keep doing what is currently working for your health. Plan to recheck your glucose markers and hs-CRP annually.
0.7–1.6 mg/L (Moderate Risk)
What Research Suggests: This range is tied to meaningfully higher odds of your prediabetes progressing (roughly 60–85% higher according to cohort data) and a lower likelihood of blood sugar reversing on its own.
Suggested Next Step: Discuss the intensity of your lifestyle interventions with your doctor. It may be wise to look at your HDL-C, triglycerides, and fasting glucose levels together to get a clearer picture.
Above 1.6–2.0 mg/L (Elevated Risk)
What Research Suggests: This range carries the highest risk of progression and shows a significantly higher incidence of diabetes per 1,000 person-years in large tracking studies.
Suggested Next Step: This warrants a more thorough clinical workup. Talk to your doctor about screening for hidden sources of infection or inflammation, reviewing your weight, sleep, and physical activity, and potentially setting up more frequent glucose monitoring.
Important Clinical Context on Single Readings: A single hs-CRP test is just a snapshot. It can easily be temporarily spiked by a common cold, a minor injury, a recent vaccination, or even a bad night of sleep right before your blood draw. Because it is so sensitive to daily life, researchers and clinicians prefer to look at your hs-CRP as a trend over repeated measurements rather than treating a single blood draw as a final verdict. Always use this framework for educational context and discuss your specific numbers with your physician.
6. Clinical Importance: What Clinicians Should Take Away
For healthcare providers and highly engaged patients, here's why interpreting hs-CRP correctly in the context of prediabetes has real clinical weight:
1. It reclassifies risk within a single diagnostic category. "Prediabetes" is often treated as a single, homogeneous risk group. But the CHARLS data show that within that group, hs-CRP tertile alone shifts four-year outcomes by roughly 60–85% in either direction. Two patients with an identical fasting glucose of 108 mg/dL may have very different five-year trajectories depending on their inflammatory status.
2. Composite markers meaningfully outperform hs-CRP in isolation. The jump in discriminatory power from an AUC of 0.60 (hs-CRP alone) to 0.75–0.86 (hs-CRP combined with HDL-C) is not a marginal statistical improvement — it represents a real gain in the ability to correctly separate people who will develop dysglycemia from those who won't. Clinically, this argues for evaluating hs-CRP alongside the existing lipid panel rather than as a standalone test.
3. The relationship is nonlinear, so "a little elevated" may matter less than a specific threshold. The NHANES restricted cubic spline analysis identified inflection points (roughly 0.6 for prediabetes and 1.2 for diabetes on the hs-CRP/HDL-C ratio) beyond which risk accelerates sharply. This supports risk-stratifying patients at defined cut-points rather than treating hs-CRP as a smooth continuous variable in patient conversations.
4. Causality evidence changes how the marker should be discussed with patients. Because Mendelian randomization data support glucose causing higher CRP (rather than pure correlation), clinicians can accurately tell patients that improving glycemic control is likely to lower their inflammatory burden directly — not merely correlate with it. This is a stronger, more motivating clinical message.
5. hs-CRP adds cardiovascular context that glucose numbers alone miss. A patient with prediabetes and high hs-CRP is not just "at risk for diabetes" — the hazard ratio data from Danish cohorts suggest they may also be walking around with meaningfully elevated ischemic heart disease and cardiovascular mortality risk right now. This should inform how urgently lifestyle or pharmacologic intervention is pursued, and may justify earlier cardiovascular risk-factor screening (lipids, blood pressure, smoking cessation counseling) in prediabetic patients with elevated inflammation.
6. Interpret hs-CRP in a metabolic-multimorbidity frame, not a single-disease frame. The nine-year CHARLS analysis combining hs-CRP with the TyG index found the sharpest risk increases in people with both markers elevated, for a composite outcome spanning diabetes, hypertension, dyslipidemia, and cardiovascular disease. This supports using elevated hs-CRP as a trigger to screen more broadly across the whole cardiometabolic system, not just to re-check blood glucose.
7. Practical Action Plan: Lowering Inflammation and Reversing Prediabetes
None of the studies above tested a specific supplement or diet against hs-CRP in a prediabetes population directly, so the following is a general, evidence-informed lifestyle framework based on well-established inflammation and glucose-metabolism research — not a guaranteed protocol. Always check with your doctor before making major changes, especially if you take medication.
Step 1: Address Visceral Fat First
Visceral (abdominal) fat is one of the most consistent drivers of chronic low-grade inflammation because fat tissue itself releases inflammatory cytokines. Even modest waist circumference reduction is associated with meaningful drops in CRP in the broader literature.
Step 2: Prioritize Sleep Quality
Poor sleep quality and short sleep duration are independently linked to higher CRP levels and worse insulin sensitivity. Aim for consistent sleep and wake times and 7–9 hours nightly.
Step 3: Build a Consistent Movement Habit
Regular moderate-to-vigorous physical activity is one of the most reliable non-pharmacologic ways to lower systemic inflammation and improve insulin sensitivity simultaneously — addressing both sides of the inflammation-glucose loop at once.
Step 4: Shift Toward an Anti-Inflammatory Eating Pattern
Diets emphasizing vegetables, fiber, oily fish, nuts, and olive oil (loosely, a Mediterranean-style pattern) are consistently associated with lower CRP in the broader nutrition literature, while diets high in refined carbohydrates and processed meats tend to push it higher.
Step 5: Don't Ignore Your Lipids
Because the hs-CRP/HDL-C ratio outperformed either marker alone, raising HDL-C (through exercise, quitting smoking, and healthy fats) may meaningfully improve your combined risk profile even if your hs-CRP doesn't move much on its own.
Step 6: Re-test, Don't Guess
Because a minor illness can throw off a single hs-CRP reading, plan to recheck it — ideally alongside fasting glucose, HbA1c, and a lipid panel — every 6–12 months, or as your doctor recommends.
Sample Weekly Framework (Illustrative, Not Prescriptive)
Here is the sample weekly framework rewritten into clear, actionable points:
Monday / Wednesday / Friday
Focus: Moderate cardiovascular exercise.
Activities: Aim for 30–45 minutes of activities like brisk walking, cycling, or swimming.
Tuesday / Thursday
Focus: Strength and conditioning.
Activities: Perform resistance training targeting large muscle groups.
Daily Habits
Sleep: Prioritize getting 7+ hours of quality sleep while minimizing late-night screen time.
Nutrition: Include vegetables in at least 2 meals and place a strong emphasis on fiber and healthy fats.
Weekly & Ongoing Goals
Fish Consumption: Eat 2 or more servings of oily fish, such as salmon, sardines, or mackerel, each week.
Dietary Restrictions: Continuously limit your intake of ultra-processed foods and added sugars.⚠️ Safety note: If you are pregnant, have a heart condition, kidney disease, or are on glucose-lowering or blood-thinning medication, talk to your doctor before starting any new exercise or supplement regimen. hs-CRP can also rise temporarily due to infections, injuries, autoimmune flares, or recent vaccination — don't panic over a single elevated reading without clinical context.
8. Evidence Summary Table
Cheng et al., 2024 (Journal of Diabetes Investigation)
Population & Design: Evaluated 2,874 adults with prediabetes from the CHARLS cohort over a 4-year follow-up period.
Key Finding: A low hs-CRP tertile was linked to higher rates of regression to normal blood sugar (normoglycemia). Conversely, individuals in the middle and high tertiles faced 63% to 85% higher odds of progressing to type 2 diabetes.
Rolver et al., 2024 (Cardiovascular Diabetology)
Population & Design: Analyzed over 112,815 adults using Danish cohorts combined with Mendelian randomization.
Key Finding: Individuals in the top quintile of CRP had a 50% higher risk of ischemic heart disease and more than double the risk of cardiovascular death. Genetic data also suggested that elevated glucose levels causally drive up CRP.
Wan et al., 2025 (Frontiers in Endocrinology)
Population & Design: Tracked 4,483 adults from the CHARLS cohort across a 9-year longitudinal follow-up.
Key Finding: The combination of a high TyG index and high hs-CRP substantially increased the risk of developing cardiometabolic multimorbidity compared to having only one marker elevated.
Ileri & Oguz, 2024 (Northern Clinics of Istanbul)
Population & Design: Examined a retrospective clinical sample of patients.
Key Finding: Elevated CRP levels were significantly more common in individuals with impaired fasting glucose. The authors proposed using elevated CRP as an early clinical warning sign for prediabetes.
Sun et al., 2025 (BMC Endocrine Disorders)
Population & Design: Cross-sectional analysis of 18,472 adults utilizing U.S. NHANES data from 2015–2023.
Key Finding: Every one-unit increase in the hs-CRP/HDL-C ratio was associated with 13.3% higher odds of prediabetes and 26.9% higher odds of diabetes. This joint ratio vastly outperformed either marker evaluated on its own.
Huang et al., 2025 (Frontiers in Endocrinology)
Population & Design: Cross-sectional analysis of 10,915 adults already diagnosed with diabetes or prediabetes.
Key Finding: A higher CRP/HDL-C ratio directly correlated with a rising prevalence of hyperuricemia, with rates climbing from 18% to roughly 30% across the study quartiles.
9. Common Myths and Mistakes
Myth: "A single high hs-CRP reading means I definitely have inflammation-driven prediabetes risk." Reality: hs-CRP is sensitive to short-term illness, injury, and even poor sleep the night before testing. One elevated value should prompt a recheck, not panic.
Myth: "hs-CRP is only useful for heart disease risk." Reality: The 2024–2025 cohort data reviewed above show hs-CRP is independently predictive of whether prediabetes progresses or regresses, separate from its established cardiovascular role.
Myth: "If my glucose numbers are fine, my CRP doesn't matter." Reality: Elevated CRP in someone with normal-range glucose has been linked in clinical samples to a higher likelihood of impaired fasting glucose developing, suggesting it can be an early warning sign that precedes measurable glucose changes.
Myth: "Lowering CRP with supplements alone will reverse prediabetes." Reality: No study reviewed here tested a specific supplement's effect on hs-CRP-linked prediabetes outcomes. The evidence supports addressing the underlying drivers (visceral fat, sleep, activity, diet) rather than chasing the number in isolation.
Myth: "The hs-CRP/HDL-C ratio and TyG index are just research curiosities with no real-world use." Reality: Both consistently outperformed single markers for identifying at-risk individuals across several large 2025 studies, suggesting real potential for future clinical screening tools.
10. Frequently Asked Questions
1. What is considered a "high" hs-CRP for someone with prediabetes? Research cohorts on prediabetes progression have generally defined "high" as roughly above 1.6 mg/L, with a middle-risk band between about 0.7 and 1.6 mg/L, though clinical labs may use slightly different cutoffs (commonly >3.0 mg/L for general cardiovascular risk categorization).
2. Can prediabetes really reverse on its own? Yes. In the CHARLS cohort study, roughly two-thirds of people with prediabetes at baseline had returned to normal glucose four years later, and low hs-CRP was one factor associated with a higher likelihood of that happening.
3. Does losing weight lower hs-CRP? Weight loss, particularly loss of visceral abdominal fat, is broadly associated with reduced hs-CRP in the wider inflammation literature, since fat tissue is a direct source of inflammatory signaling molecules.
4. Is hs-CRP the same as regular CRP? They measure the same protein, but the "high-sensitivity" assay can detect much lower concentrations, making it suitable for assessing chronic low-grade inflammation rather than only acute infection or injury.
5. Should I ask my doctor for an hs-CRP test if I have prediabetes? It's reasonable to ask, since current research suggests it adds meaningful prognostic information beyond glucose numbers alone. Your doctor can help interpret it alongside your full metabolic panel.
6. What is the hs-CRP/HDL-C ratio, and is it a standard test? It's a calculated ratio (hs-CRP divided by HDL cholesterol) studied as a composite inflammation-lipid marker. It isn't yet a standard, universally ordered clinical test, but the 2025 NHANES data suggest it may be more informative than either component alone.
7. Can an infection or cold throw off my hs-CRP test? Yes. Because hs-CRP responds to any inflammatory trigger — including colds, minor injuries, and recent vaccinations — it's best tested when you're otherwise healthy and, ideally, confirmed with a repeat measurement.
8. Does high hs-CRP mean I will definitely develop diabetes? No single marker guarantees an outcome. Elevated hs-CRP is associated with meaningfully higher odds of progression in large cohort studies, but it's a risk factor, not a certainty, and it operates alongside diet, activity, weight, and genetics.
9. How does inflammation actually cause insulin resistance? Inflammatory signaling activates pathways such as NF-κB and JNK inside cells, which interfere with normal insulin receptor signaling, while also potentially impairing pancreatic beta-cell function over time — reducing the body's ability to both respond to and produce insulin effectively.
10. Is the TyG index better than hs-CRP for predicting diabetes risk? They measure different things — TyG reflects insulin resistance via triglycerides and glucose, while hs-CRP reflects inflammation. Combined-marker research suggests using both together provides a more complete risk picture than relying on either alone.
11. How often should hs-CRP be rechecked once prediabetes is diagnosed? There's no universal guideline specific to this use case, but many of the cohort studies reviewed here re-measured metabolic markers on a multi-year basis; discussing an annual or biannual recheck with your doctor alongside your glucose panel is a reasonable approach.
12. Are these findings only relevant to specific ethnic populations? Several of the largest cohort studies come from Chinese populations (CHARLS, Kailuan). In contrast, the hs-CRP/HDL-C ratio research comes from a nationally representative U.S. NHANES sample and Danish cohort data for the cardiovascular Mendelian randomization findings — together spanning multiple populations. However, further validation across additional ethnic and geographic groups is still warranted, as several study authors themselves note.
11. Conclusion and Action Steps
Prediabetes is not a fixed diagnosis — it's a fork in the road, and the latest research suggests hs-CRP may help show which direction you're more likely to travel. Across multiple large, prospective cohorts published in 2024 and 2025, low-grade inflammation consistently tracked with a higher chance of prediabetes progressing to diabetes, and a lower chance of it reversing back to normal glucose. Combining hs-CRP with HDL cholesterol or the TyG index sharpened that prediction considerably, and genetic evidence suggests glucose and inflammation may drive each other in a two-way, reinforcing cycle that also raises cardiovascular risk.
Your next steps:
Ask your doctor whether an hs-CRP test makes sense alongside your existing glucose and lipid panels.
If your hs-CRP is elevated, treat it as a prompt to intensify — not abandon — lifestyle efforts around weight, sleep, movement, and diet.
Recheck your numbers on a regular schedule rather than reacting to a single reading.
If you have both prediabetes and elevated inflammation, discuss with your doctor whether more proactive cardiovascular risk screening is warranted, given the compounding risk shown in the research above.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting, stopping, or adjusting any medication. Individual risk profiles and treatment decisions must be individualised.
Related Article
How Many Carbs Should Diabetics Eat? 2026 Evidence-Based Guidelines for Better Blood Sugar
Can You Reverse Type 2 Diabetes with Diet? Science-Based Guide 2026
Your Cholesterol Isn’t the Whole Story: The Hormone Imbalances Driving Heart Disease
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
References
Cheng ZJ, Wang YF, Jiang XY, et al. High sensitivity C-reactive protein and prediabetes progression and regression in middle-aged and older adults: A prospective cohort study. J Diabetes Investig. 2024;15(1):78-86.
Rolver MG, Emanuelsson F, Nordestgaard BG, Benn M. Contributions of elevated CRP, hyperglycaemia, and type 2 diabetes to cardiovascular risk in the general population: observational and Mendelian randomization studies. Cardiovasc Diabetol. 2024;23(1):165.
Wan B, Wang S, Hu S, et al. The comprehensive effects of high-sensitivity C-reactive protein and triglyceride glucose index on cardiometabolic multimorbidity. Front Endocrinol. 2025;16:1511319.
Ileri S, Oguz A. The relation of C-reactive protein and impaired fasting glucose: Could it be a predictor for prediabetic state? North Clin Istanb. 2024;11(1):81-87.
Sun H, Yang J, Ma L, Wu Y. Association between hs-CRP/HDL-C ratio and risk of prediabetes or diabetes: a cross-sectional study based on NHANES 2015–2023. BMC Endocr Disord. 2025;25:183.
Huang D, Ma J, Zhao Y, Pan Q, Xu G, Guo L. Higher C-reactive protein to high-density lipoprotein cholesterol ratio is associated with hyperuricemia in diabetes and prediabetes: a cross-sectional study. Front Endocrinol. 2025;16:1619370.
Lan Y, Wu D, Zheng H, et al. Elevated inflammation supra-additively promotes the progression from prediabetes to diabetes: a prospective cohort study. J Glob Health. 2025;15:04318.
Pradhan AD, Manson JE, Rifai N, Buring JE, Ridker PM. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA. 2001;286(3):327-334.
Wang X, Bao W, Liu J, et al. Inflammatory markers and risk of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2013;36(1):166-175.
Donath MY, Shoelson SE. Type 2 diabetes as an inflammatory disease. Nat Rev Immunol. 2011;11(2):98-107.
Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31-55.
Xepapadaki E, Nikdima I, Sagiadinou EC, Zvintzou E, Kypreos KE. HDL and type 2 diabetes: the chicken or the egg? Diabetologia. 2021;64:1917-1926.
Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279-2290.
Echouffo-Tcheugui JB, Selvin E. Prediabetes and what it means: the epidemiological evidence. Annu Rev Public Health. 2021;42(1):59-77.
ElSayed NA, Aleppo G, Aroda VR, et al. Classification and diagnosis of diabetes: Standards of Care in Diabetes—2023. Diabetes Care. 2023;46(Suppl 1):S19-S40.
Xue K, Sun M, Zong C, Xing S, Xue H. Non-linear association of a novel inflammation-lipid composite marker CRP/HDL with insulin resistance and type 2 diabetes. Diabetol Metab Syndr. 2025;17(1):125.
Gao Y, Wang M, Wang R, et al. The predictive value of the hs-CRP/HDL-C ratio for cardiovascular disease in middle-aged and elderly people: evidence from a large national cohort study. Lipids Health Dis. 2024;23(1):66.
Sarhan RS, Mohammed RR. Estimated levels of glycated albumin and C-reactive protein/total albumin ratio might distinguish prediabetics among apparently healthy people. Nutr Metab Insights. 2025.
Zhang X, Wu H, Fan B, et al. The role of age on the risk relationship between prediabetes and major morbidities and mortality. Lancet Reg Health West Pac. 2023;30.
Perreault L, Kahn SE, Christophi CA, et al. Regression from pre-diabetes to normal glucose regulation in the Diabetes Prevention Program. Diabetes Care. 2009;32:1583-1588.
Prediabetes transitions to normoglycaemia or type 2 diabetes and associated risk factors: an individual-level pooled analysis of 19 prospective cohort studies. Lancet Glob Health. 2025.
Han F, Guo H, Zhang H, Zheng Y. hs-CRP/HDL-C can predict the risk of all-cause mortality in cardiovascular-kidney-metabolic syndrome stage 1-4 patients. Front Endocrinol. 2025;16:1552219.
Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
Barter PJ, Nicholls S, Rye K, et al. Anti-inflammatory properties of HDL. Circ Res. 2004;95(8):764-772.
National Institutes of Health / MedlinePlus. C-reactive protein test. U.S. National Library of Medicine.
American Diabetes Association. Understanding Prediabetes. diabetes.org.
Centers for Disease Control and Prevention. Prediabetes — Your Chance to Prevent Type 2 Diabetes. cdc.gov.
Pickup JC. Inflammation and activated innate immunity in the pathogenesis of type 2 diabetes. Diabetes Care. 2004;27(3):813-823.