Improve Leptin & Adiponectin: Science-Based Guide to Metabolic Health
Learn how targeted diet and exercise, proven by recent meta-analyses, can reverse leptin resistance and boost adiponectin for optimal weight and metabolic health.
METABOLISM
Dr. T.S. Didwal, M.D.
5/27/202627 min read
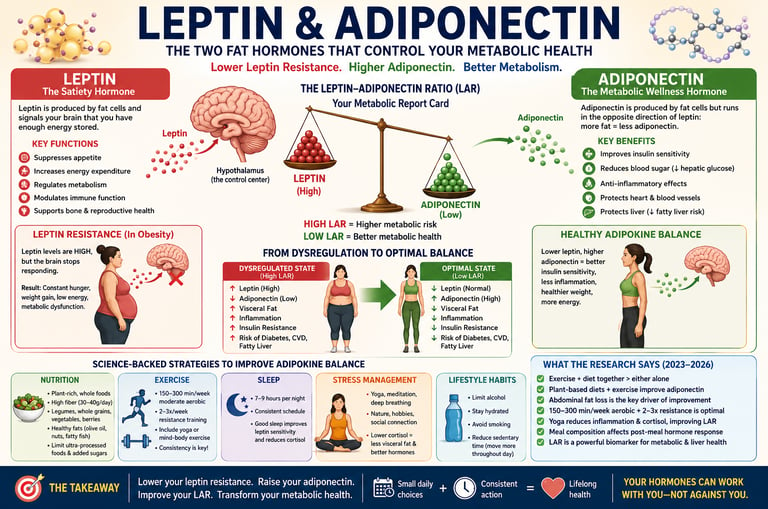
Leptin and adiponectin are essential adipokines secreted by fat tissue that regulate appetite control, insulin sensitivity, inflammation, and overall metabolic health. In individuals with obesity or metabolic syndrome, this hormonal balance becomes disrupted—circulating leptin levels rise but fail to signal satiety effectively (leptin resistance), while beneficial adiponectin levels decline, increasing the risk of insulin resistance, dyslipidemia, and cardiovascular disease .
High-quality evidence from randomized trials and meta-analyses demonstrates that combined lifestyle interventions are the most effective way to restore adipokine balance. Exercise paired with dietary modification produces significantly greater reductions in leptin and meaningful increases in adiponectin compared with either intervention alone (Khalafi et al., 2023; Wang et al., 2025) . Moderate-intensity aerobic exercise (150–300 minutes per week), resistance training, and yoga improve adipokine signaling by reducing visceral fat, systemic inflammation, and cortisol levels (Shimizu et al., 2025; Suder et al., 2024) .
Dietary quality further amplifies these effects. Plant-forward diets rich in fiber, whole grains, legumes, and vegetables enhance adiponectin secretion and improve insulin sensitivity, particularly when combined with regular physical activity (Kazeminasab et al., 2024) . Importantly, clinically meaningful improvements in leptin sensitivity and adiponectin levels can occur within 8–12 weeks, even without extreme weight loss, underscoring the power of sustainable lifestyle change.
Key Points
1. Synergistic Lifestyle Intervention is Superior
The combination of dietary improvement and regular exercise consistently produces greater reductions in leptin and increases in adiponectin than either approach alone. Moderate caloric restriction paired with 150–300 minutes of weekly moderate-intensity activity offers the most reliable metabolic benefits, often visible within 8–12 weeks.
2. Target Visceral Fat, Not Just Scale Weight
Abdominal (visceral) fat is the primary driver of leptin resistance and low adiponectin. Reducing waist circumference — even before major overall weight loss — is one of the most direct ways to restore healthy adipokine balance. Measure your waist regularly as a practical clinical marker.
3. Prioritize a Plant-Forward, High-Fiber Diet
Plant-rich eating patterns high in fiber (aim for 30–40 g/day from legumes, vegetables, whole grains, and seeds) reduce inflammation and support adiponectin production through improved gut microbiome function and short-chain fatty acid production. This approach outperforms standard diets even in people with existing metabolic conditions.
4. Exercise Modality Matters Less Than Consistency
All forms of movement help, but the optimal prescription is combined aerobic (150–300 min/week moderate intensity) plus resistance training (2–3 sessions/week). Add yoga or mind-body practices 1–2 times weekly for added benefits on stress hormones and the leptin-adiponectin ratio.
5. Sleep and Stress Management Are Non-Negotiable
Chronic sleep deprivation and elevated cortisol directly worsen leptin resistance and suppress adiponectin. Prioritizing 7–9 hours of consistent, high-quality sleep and daily stress-reduction practices (such as yoga, meditation, or nature time) addresses a critical pathway that diet and exercise alone may not fully correct.
6. Expect Meaningful Change in 12 Weeks
Clinically relevant improvements in leptin sensitivity and adiponectin levels typically begin within 4–8 weeks and become substantial by 12 weeks of consistent lifestyle changes. The leptin-to-adiponectin ratio serves as a valuable biomarker for tracking progress beyond weight alone. Small, sustainable habits compound powerfully over time.
What Are Leptin and Adiponectin?
Leptin: The Satiety Hormone
Leptin is a peptide hormone produced primarily by adipocytes (fat cells). Its core job is to travel to the hypothalamus in the brain and signal that you have sufficient energy stored — in other words, that you're full and don't need to eat.
In a healthy person, this feedback loop works beautifully:
Fat stores increase → more leptin is released
Brain detects leptin → appetite decreases, energy expenditure increases
Fat stores decrease → less leptin is released → hunger returns
In people with obesity, paradoxically, leptin levels are chronically elevated, yet the brain stops responding to the signal. This is called leptin resistance — a state functionally similar to insulin resistance, where the signal is loud but the receiver is broken.
Key functions of leptin:
Suppresses appetite via hypothalamic pathways
Regulates energy expenditure and thermogenesis
Modulates immune function and inflammation
Influences reproductive hormone signaling
Supports bone metabolism
Adiponectin: The Metabolic Wellness Hormone
Adiponectin is another adipokine secreted by fat tissue, but it works very differently from leptin. Here's the paradox that surprises most people: the more body fat you carry, the less adiponectin you produce. It runs in the opposite direction of leptin.
Adiponectin has earned its "wellness hormone" reputation through a remarkable range of protective effects:
Improves insulin sensitivity in muscle and liver
Reduces hepatic glucose production, lowering fasting blood sugar
Anti-inflammatory action: suppresses NF-κB and reduces pro-inflammatory cytokines
Cardioprotective: improves endothelial function, reduces atherosclerotic plaque formation
Anti-fibrotic: protective against non-alcoholic fatty liver disease (NAFLD)
Low adiponectin is independently associated with type 2 diabetes, cardiovascular disease, metabolic syndrome, and even certain cancers. It is one of the most clinically important biomarkers in metabolic medicine.
The Leptin-Adiponectin Ratio: Your Metabolic Report Card
Scientists increasingly use the leptin-to-adiponectin ratio (LAR) — or its inverse, the adiponectin-to-leptin ratio (ALR) — as a single, powerful biomarker of adipose tissue health and overall metabolic risk.
A high LAR (high leptin, low adiponectin) is associated with:
Insulin resistance and type 2 diabetes risk
Increased cardiovascular disease risk
Non-alcoholic fatty liver disease (NAFLD)
Chronic low-grade inflammation
Dyslipidemia (high triglycerides, low HDL)
A 2026 cross-sectional study by Aguirre-Cruz and colleagues, published in Adipocyte, examined the adiponectin/leptin ratio (ALR) specifically as a biomarker of adipose tissue dysfunction and visceral adipose tissue (VAT) accumulation in 54 adults aged 30–70. Their findings revealed important sex-specific differences: the ALR associated differently with visceral fat accumulation, macrophage infiltration of adipose tissue, and adipose tissue insulin resistance (ADIPO-IR) between males and postmenopausal females. This has major implications — it means that men and women may need modestly different strategies to optimise their adipokine balance, and that measuring the ALR may provide more nuanced clinical insight than measuring either hormone alone.
A 2026 pilot study by Balestra and colleagues, published in Frontiers in Nutrition, further validated the LAR as a multidimensional biomarker in obese patients with liver steatosis (fatty liver) undergoing a Very-Low Energy Ketogenic Therapy (VLEKT). Their results confirmed that the LAR reflects not just body fat levels but the deeper functional health of adipose tissue — making it a superior tool for tracking treatment response compared to body weight alone.
What this means for you: Even without laboratory tests, you can directionally improve your leptin/adiponectin ratio through the lifestyle strategies described in this article. If you do have access to metabolic blood work, ask your doctor about fasting leptin and adiponectin measurements — they provide uniquely actionable clinical information.
Why These Hormones Become Dysregulated
Understanding the root causes of adipokine dysregulation helps explain why certain interventions work and others don't.
1. Excess Visceral Fat
Visceral adipose tissue (VAT) — the fat stored deep in the abdomen around organs — is metabolically different from subcutaneous fat (the fat under your skin). VAT adipocytes are larger, more inflamed, more insulin-resistant, and produce far more leptin while secreting far less adiponectin. Reducing waist circumference, not just overall body weight, is the most direct lever for improving the LAR.
2. Chronic Inflammation
Elevated pro-inflammatory cytokines like TNF-α and IL-6 directly impair leptin receptor signaling in the brain (creating leptin resistance) and suppress adiponectin secretion from fat cells. The relationship is bidirectional: fat tissue inflammation causes adipokine dysregulation, and adipokine dysregulation amplifies fat tissue inflammation.
3. Insulin Resistance
Hyperinsulinemia suppresses adiponectin production and further promotes leptin resistance. This creates a self-reinforcing cycle: insulin resistance → worse adipokine balance → more insulin resistance.
4. Poor Diet Quality
Ultra-processed foods, refined carbohydrates, added sugars, and excessive saturated fat all promote visceral fat accumulation, systemic inflammation, and oxidative stress — the exact conditions that drive adipokine dysregulation. Conversely, dietary fiber and polyphenols (abundant in plant foods) support a gut microbiome that produces short-chain fatty acids (SCFAs) which directly enhance adiponectin signaling.
5. Sedentary Behavior
Physical inactivity reduces AMPK (AMP-activated protein kinase) activity — a key enzyme that stimulates adiponectin production in adipocytes. Regular exercise upregulates adiponectin receptors and reduces visceral fat, creating a favorable hormonal environment.
6. Sleep Disruption & Chronic Stress
Poor sleep acutely suppresses leptin and elevates ghrelin (the hunger hormone), while chronically elevating cortisol — which promotes central fat deposition and further disrupts adipokine balance. Chronic psychological stress operates through the same cortisol pathway.
What the Latest Research Says (2023–2026)
Here is a detailed synthesis of the most important recent research — the evidence base for every recommendation in this article.
Study 1 — Khalafi et al. (2023): The Combination Principle
This landmark systematic review and meta-analysis in Advances in Nutrition analyzed randomized controlled trials testing exercise and dietary interventions on circulating leptin and adiponectin in people with overweight or obesity.
Key finding: The combination of exercise plus dietary modification produced significantly greater reductions in leptin and increases in adiponectin than either intervention alone. Moderate-intensity aerobic exercise at 150 minutes per week, combined with dietary quality improvements and moderate caloric reduction, yielded the most consistent and clinically meaningful results.
Clinical takeaway: Neither diet nor exercise alone is sufficient. The synergy between them is where the magic happens.
Study 2 — Kazeminasab et al. (2024): The Plant-Based Advantage
This meta-analysis in Frontiers in Nutrition focused specifically on plant-based diets combined with exercise on leptin and adiponectin — in both healthy adults and those with chronic diseases, including type 2 diabetes.
Key finding: Plant-forward dietary patterns — emphasizing whole grains, legumes, vegetables, and fibre — significantly reduced inflammatory markers and improved adiponectin secretion. When these diets were paired with structured exercise, the improvements were amplified substantially. Importantly, these effects were seen even in people managing existing chronic conditions.
Clinical takeaway: You don't need to go fully vegan. But moving plants to the center of your plate creates an anti-inflammatory environment that fundamentally supports adipokine balance.
Study 3 — Suder et al. (2024): Abdominal Fat is the Primary Target
This randomized controlled trial in Scientific Reports studied males with abdominal obesity and found that combined aerobic and resistance training (3–5 aerobic sessions/week + 2 resistance sessions/week) with moderate caloric restriction produced significant improvements in leptin, adiponectin, and a newer adipokine called asprosin — which is involved in hepatic glucose release.
Key finding: Abdominal fat reduction was identified as the primary mechanistic driver of adipokine improvements — not just overall weight loss. Participants who reduced waist circumference most saw the greatest hormonal improvements, even if total weight loss was similar between groups.
Clinical takeaway: Monitor your waist circumference, not just the scale. Abdominal fat loss is the most direct path to better adipokine balance.
Study 4 — Shimizu et al. (2025): Yoga and the Mind-Body Connection
This narrative review in Cureus examined the evidence on yoga specifically and its effects on leptin and adiponectin in people with obesity.
Key finding: Yoga improves the leptin-to-adiponectin ratio through two primary pathways: (1) reducing systemic inflammation, and (2) improving cortisol regulation. The psychosomatic dimension of yoga — its impact on the hypothalamic-pituitary-adrenal (HPA) axis — adds a unique mechanism that conventional exercise does not fully replicate.
Clinical takeaway: Yoga is not just stretching. It is a scientifically supported tool for improving adipokine balance, particularly for those with high stress, elevated cortisol, or who find conventional exercise difficult.
Study 5 — Wang et al. (2025): The Optimal Exercise Prescription
This comprehensive systematic review with pairwise, network, and dose-response meta-analyses in Frontiers in Nutrition is the most granular exercise prescription study to date on adipokine dysregulation.
Key finding: All exercise modalities — aerobic, resistance, HIIT, yoga — improve leptin and adiponectin. Combined approaches produce the best results. The dose-response analysis found that 150–300 minutes of moderate-intensity aerobic activity per week is the sweet spot, with diminishing returns beyond 300–400 minutes/week. Resistance training 2–3 sessions/week provides additive benefits.
Clinical takeaway: More isn't always better. Consistent, well-structured, moderate exercise outperforms sporadic intense bursts. Adherence is the most important variable.
Study 6 — Moreira et al. (2025): Systemic Benefits Beyond Fat Loss
This emerging research in Antioxidants demonstrated that lifestyle interventions reduce oxidative stress and inflammation throughout the body — including in tissues beyond fat and muscle. The systemic reduction in inflammatory burden translates to improved adipocyte function and better adipokine signaling at the cellular level.
Clinical takeaway: The benefits of lifestyle change operate at a deeper level than fat loss alone. Reduced oxidative stress improves the intrinsic capacity of fat cells to secrete adiponectin and respond to leptin signaling.
Study 7 — Del Razo-Olvera et al. (2026): Does Meal Composition Matter Acutely?
This cross-sectional study in PloS One examined how standardized high-carbohydrate versus high-fat meals affect leptin and adiponectin in the postprandial (after-eating) period in adults.
Key finding: Women had significantly higher leptin and adiponectin levels than men, while individuals with obesity showed higher leptin and lower adiponectin levels regardless of meal type (p < 0.001). High-fat meals caused leptin levels to progressively decline, whereas high-carbohydrate meals produced little change. Adiponectin levels changed only minimally and were not significantly affected by meal composition..
Clinical takeaway: Obesity is associated with higher leptin and lower adiponectin levels, indicating worsening metabolic dysfunction. Meal composition also matters — high-fat meals may temporarily lower leptin levels, while adiponectin appears relatively stable after eating. These findings highlight the importance of body composition and dietary quality in metabolic health.
Study 8 — Balestra et al. (2026): The LAR as a Liver Health Biomarker
This pilot study in Frontiers in Nutrition found that the leptin/adiponectin ratio (LAR) tracks liver steatosis (fat accumulation in the liver) and responds meaningfully to intensive dietary intervention (VLEKT). The LAR improved significantly with treatment and correlated with histological improvement in liver fat.
Clinical takeaway: The LAR may become a routine, non-invasive biomarker for monitoring fatty liver disease in addition to its established role in cardiometabolic risk. This underscores the importance of adipokine balance far beyond weight management.
The Best Diet Strategies to Balance These Hormones
Diet is the single most powerful tool for reducing leptin (by reducing visceral fat) and increasing adiponectin (by reducing inflammation and improving insulin sensitivity). Here's how to structure your approach:
1. Go Plant-Forward (Not Necessarily Plant-Only)
The evidence from Kazeminasab et al. (2024) is clear: plant-rich diets consistently outperform standard Western diets for adipokine improvement. The specific mechanisms include:
Dietary fiber → feeds gut bacteria → produces short-chain fatty acids (butyrate, propionate) → reduces intestinal permeability and systemic inflammation → better adiponectin signaling
Polyphenols (found in berries, olive oil, green tea, legumes) → direct anti-inflammatory effects → improved adipocyte function
Phytosterols (found in whole grains, nuts) → reduce lipid absorption → better lipid profiles → improved adipokine environment
Practical tip: Aim to fill at least half your plate with non-starchy vegetables at every meal. Replace refined grains with whole grains (oats, barley, quinoa, brown rice). Eat legumes (lentils, chickpeas, black beans) at least 3–4 times per week.
2. Prioritize High-Fiber Foods
Soluble fibre — found in oats, legumes, apples, pears, flaxseed, and psyllium — has particularly strong evidence for improving metabolic markers. Aim for 30–40g of total dietary fiber per day (most people consume less than 15g).
Top fiber sources for metabolic health:
Lentils (1 cup cooked)
Fiber Content: 15.6g
Additional Benefits: Packed with plant-based protein and features a low glycemic index, making it exceptional for steady blood sugar control.
Black Beans (1 cup cooked)
Fiber Content: 15.0g
Additional Benefits: Highly rich in vital micronutrients, particularly magnesium and folate.
Chia Seeds (2 tbsp)
Fiber Content: 9.8g
Additional Benefits: Provides a powerful dose of heart-healthy omega-3 fatty acids and calcium.
Moderate-to-High Fiber Foods (5g to 8g per serving)
Oats (1 cup dry)
Fiber Content: 8.0g
Additional Benefits: Contains beta-glucan, a unique soluble fiber renowned for its anti-inflammatory properties and cholesterol-lowering effects.
Flaxseed (2 tbsp)
Fiber Content: 5.6g
Additional Benefits: Offers double-duty cellular protection with lignans (antioxidants) and plant-based omega-3 ALA.
Broccoli (1 cup cooked)
Fiber Content: 5.1g
Additional Benefits: Loaded with sulforaphane, a potent compound that triggers the body's natural anti-inflammatory and detox pathways.
Avocado (Half)
Fiber Content: 5.0g
Additional Benefits: Rich in oleic acid, a healthy monounsaturated fat that supports cardiovascular health and enhances nutrient absorption.
3. Moderate Your Caloric Intake Without Extreme Restriction
A moderate caloric deficit of 300–600 calories below your total daily energy expenditure (TDEE) is the most effective and sustainable approach to visceral fat reduction. Extreme restriction (below 800 cal/day) can paradoxically impair adiponectin secretion by triggering cortisol elevation and lean mass loss.
4. Reduce Ultra-Processed Foods and Added Sugars
Ultra-processed foods are the most reliable driver of adipokine dysregulation in the modern diet. They combine multiple mechanisms of harm: high glycemic load → hyperinsulinemia, refined vegetable oils (high omega-6) → pro-inflammatory arachidonic acid cascade, absence of fiber → dysbiosis, additives → gut permeability. These cascade into suppressed adiponectin and amplified leptin resistance.
Practical rule: If a food product contains more than 5 ingredients or contains ingredients you wouldn't cook with at home (emulsifiers, artificial colors, hydrogenated oils), minimize or eliminate it.
5. Include Anti-Inflammatory Fats
Not all fats are equal in their effects on adipokines:
Omega-3 fatty acids (fatty fish, walnuts, flaxseed, algae oil): directly reduce inflammatory cytokines that suppress adiponectin
Monounsaturated fats (olive oil, avocado): improve insulin sensitivity and adiponectin levels
Saturated fats (especially from processed meats and fried foods): promote inflammation and adipokine dysregulation — limit but do not necessarily eliminate
Trans fats (industrial partially-hydrogenated oils): avoid entirely — directly impair adiponectin secretion
6. Meal Timing and Composition Matter
Based on Del Razo-Olvera et al. (2026), the postprandial adipokine response differs based on meal macronutrient composition. While the research on optimal meal timing for adipokine control is still evolving, current evidence supports:
Avoiding very large meals in the evening (when insulin sensitivity is naturally lower)
Not skipping breakfast if you have obesity or metabolic syndrome (may worsen leptin signaling)
Pairing carbohydrates with protein, fat, and fiber to blunt glycemic response
Exercise Programming for Optimal Adipokine Response
Exercise is the most powerful tool for raising adiponectin — and it works even without significant weight loss. Based on Wang et al. (2025) and Suder et al. (2024), here is the evidence-based exercise prescription:
Aerobic Exercise: The Foundation
Target: 150–300 minutes per week of moderate-intensity aerobic activity
Moderate intensity = you can hold a conversation but couldn't sing (roughly 50–70% of maximum heart rate)
Best modalities: Walking, cycling, swimming, jogging, rowing, dancing, elliptical
Distribution: 5 days/week of 30–60 minutes is superior to 2 days of very long sessions
Why it works: Reduces visceral fat mass, stimulates AMPK in adipocytes (which upregulates adiponectin expression), reduces inflammatory cytokines, improves insulin sensitivity
Resistance Training: The Multiplier
Target: 2–3 sessions per week, targeting all major muscle groups
Structure: 3–4 sets of 8–12 reps per exercise, focusing on compound movements (squats, deadlifts, rows, presses, lunges)
Rest: 60–90 seconds between sets
Progression: Gradually increase load over weeks to maintain stimulus
Why it works: Increases muscle mass → improves insulin sensitivity → enhances adiponectin receptor expression; also directly reduces abdominal fat through metabolic rate elevation
Yoga and Mind-Body Exercise: The Stress Pathway
Based on Shimizu et al. (2025), yoga improves the LAR through mechanisms that are additive to conventional exercise, not redundant:
Reduces HPA-axis hyperactivity → lowers chronic cortisol → less visceral fat deposition
Improves parasympathetic tone → better insulin sensitivity
Reduces systemic inflammation independently of weight loss
Recommendation: 2–3 yoga sessions per week (60–75 minutes each) as a standalone intervention or 1–2 sessions weekly as an adjunct to aerobic and resistance training.
HIIT: For Time-Constrained Individuals
High-intensity interval training (HIIT) shows rapid improvements in adipokine profiles, particularly adiponectin, in a shorter total time investment. A practical format:
10-minute warm-up
20–30 seconds at near-maximum effort
40–90 seconds active recovery
Repeat 6–10 rounds
10-minute cool-down
Caution: HIIT is highly effective but raises cortisol acutely. For individuals with high baseline stress or HPA-axis dysfunction, prioritize moderate-intensity aerobic exercise and yoga first.
Complete Weekly Exercise Template
Daily Training Schedule
Monday: Resistance Training (Full Body)
Duration: 45–60 minutes
Intensity: Moderate-to-high
Tuesday: Moderate Aerobic Activity
Activity Types: Walking or cycling
Duration: 45 minutes
Intensity: Moderate
Wednesday: Yoga or Stretching
Duration: 60 minutes
Intensity: Low-to-moderate
Thursday: Resistance Training (Full Body)
Duration: 45–60 minutes
Intensity: Moderate-to-high
Friday: Moderate Aerobic Activity
Activity Types: Swimming or jogging
Duration: 45 minutes
Intensity: Moderate
Saturday: Extended Aerobic Activity
Activity Types: Hiking or outdoor cycling
Duration: 60–90 minutes
Intensity: Low-to-moderate
Sunday: Active Recovery
Activity Types: Casual walk or gentle yoga
Duration: 30 minutes
Intensity: Low
Weekly Volume Summary
Aerobic-Equivalent Activity: ~270–330 total minutes per week
Strength Training: 2 full-body resistance sessions per week
Beyond Diet and Exercise: Sleep, Stress & More
Sleep: The Overnight Metabolic Reset
Sleep is when your body rebalances hormonal systems, including leptin. Even a single night of poor sleep measurably reduces leptin levels and elevates ghrelin (the hunger hormone), driving the next day's appetite dysregulation. Chronically poor sleep:
Reduces leptin sensitivity in the hypothalamus
Elevates cortisol → promotes visceral fat deposition → suppresses adiponectin
Impairs glucose tolerance → worsens insulin resistance
Increases inflammatory cytokines → further disrupts adipokine signaling
Evidence-based sleep targets:
Duration: 7–9 hours per night for most adults
Consistency: Same bedtime and wake time 7 days/week — circadian rhythm consistency is as important as duration
Sleep hygiene: Cool room (65–68°F / 18–20°C), complete darkness, no screens 60 minutes before bed
Address sleep disorders: Obstructive sleep apnea is extremely common in people with obesity and severely worsens adipokine dysregulation — get evaluated if you snore loudly or feel unrefreshed after sleep
Stress Management: Cutting the Cortisol Connection
Chronic psychological stress elevates cortisol, which:
Promotes central fat deposition (visceral adipogenesis)
Directly suppresses adiponectin production
Induces leptin resistance via inflammatory pathways
Drives emotional eating behaviors that undermine dietary improvements
Evidence-supported stress reduction tools:
Yoga (Shimizu et al., 2025): proven direct effects on LAR via cortisol reduction
Meditation and mindfulness: 10–20 minutes daily reduces cortisol and inflammatory markers
Time in nature: regular exposure to natural environments (forests, parks, water) measurably reduces cortisol
Social connection: loneliness and social isolation elevate inflammatory cytokines — prioritize relationships
Diaphragmatic breathing: 5 minutes of slow deep breathing activates the parasympathetic nervous system within minutes
Alcohol: A Significant Disruptor
Excess alcohol consumption:
Promotes visceral fat deposition
Elevates triglycerides → worsens dyslipidemia
Directly suppresses adiponectin production in hepatocytes
Impairs sleep architecture
If you drink, moderate consumption means no more than 1 standard drink per day for women and 2 for men — and even this may impair adipokine balance in those with existing metabolic dysfunction. Consider a 4–8 week abstinence trial as part of your initial intervention.
Environmental Factors: The Emerging Evidence
Emerging research links endocrine-disrupting chemicals (EDCs) — including BPA (in plastics), phthalates, and certain pesticides — to adipokine dysregulation. While the clinical significance of typical human exposures is still being studied, reasonable precautions include:
Avoiding heating food in plastic containers
Choosing organic produce when possible for the "Dirty Dozen" high-pesticide crops
Using glass or stainless steel water bottles
Postprandial Response: Does Meal Type Matter?
The 2026 study by Del Razo-Olvera et al.,, published in PLoS One, adds an important layer of nuance: how your hormones respond in the hours after a meal depends significantly on what that meal contains.
Their cross-sectional study found that standardized high-carbohydrate and high-fat meals produced measurably different postprandial leptin and adiponectin responses in adults — meaning that fasting hormone levels alone may not capture the full picture of your metabolic hormonal environment.
What this means practically:
Mixed macronutrient meals — combining carbohydrates, protein, and fat — produce more favorable and stable postprandial hormonal responses than extreme macronutrient compositions
Meal quality matters independently of macronutrient ratios: a high-carbohydrate meal of lentils and vegetables behaves very differently from a high-carbohydrate meal of white bread and sugary drinks
For clinical testing: if your doctor is measuring fasting leptin or adiponectin levels, your recent dietary pattern in the 24–48 hours prior may influence results — a consideration for clinical interpretation
This research highlights that the goal isn't simply to eat "low carb" or "low fat" — it's to eat high-quality foods, with an emphasis on fibre, polyphenols, and minimally processed whole foods.
Evidence Summary Table
Here is the summary of recent clinical studies on leptin and adiponectin regulation, rewritten from the table into clear, point-by-point summaries categorized by study type and year.
Kazeminasab et al. (2024)
Study Design: Meta-analysis
Intervention: Plant-based diet combined with exercise
Leptin Finding: Successfully reduced circulating leptin levels compared to control groups.
Adiponectin Finding: Significantly raised adiponectin levels, an effect that was actively amplified by the inclusion of exercise.
Khalafi et al. (2023)
Study Design: Meta-analysis of Randomized Controlled Trials (RCTs)
Intervention: Exercise combined with dietary changes
Leptin Finding: The combined intervention reduced leptin levels significantly more than using either diet or exercise alone.
Adiponectin Finding: The combined intervention raised adiponectin levels more effectively than either strategy by itself.
Wang et al. (2025)
Study Design: Network and dose-response meta-analysis
Intervention: Evaluated all exercise modalities
Leptin Finding: Every exercise modality successfully reduced leptin, but combining training types yielded the best results.
Adiponectin Finding: An exercise volume of 150–300 minutes per week of aerobic activity, paired with resistance training 2–3 times per week, proved optimal for boosting adiponectin.
Balestra et al. (2026)
Study Design: Pilot RCT
Intervention: Very-Low Energy Ketogenic Therapy (VLEKT)
Leptin Finding: The Leptin-to-Adiponectin Ratio (LAR) improved significantly over the course of therapy.
Adiponectin Finding: Adiponectin levels improved, and the reduction in LAR correlated directly with improvements in liver fat content.
Suder et al. (2024)
Study Design: Randomized Controlled Trial (RCT)
Intervention: Aerobic training, resistance training, and calorie restriction
Leptin Finding: Showed a significant reduction in leptin, with the loss of visceral abdominal fat acting as the primary driver.
Adiponectin Finding: Showed a significant increase in adiponectin that correlated directly with a reduction in waist circumference.
Moreira et al. (2025)
Study Design: Comprehensive literature review
Intervention: Exercise combined with dietary changes
Leptin Finding: Reduces systemic oxidative stress, which directly improves cellular leptin signaling sensitivity.
Adiponectin Finding: Improves underlying adipocyte (fat cell) function, expanding the body's overall adiponectin secretion capacity.
Shimizu et al. (2025)
Study Design: Narrative review
Intervention: Yoga and mindfulness practices
Leptin Finding: Successfully improved the Leptin-to-Adiponectin Ratio (LAR) by lowering baseline stress and cortisol production.
Adiponectin Finding: Boosted adiponectin levels by reducing chronic, systemic inflammation.
Aguirre-Cruz et al. (2026)
Study Design: Cross-sectional observational study
Intervention: N/A (Baseline tracking)
Key Finding: Revealed that the Adiponectin-to-Leptin Ratio (ALR) has distinct, sex-specific associations with visceral fat accumulation and adipose tissue dysfunction.
Del Razo-Olvera et al. (2026)
Study Design: Cross-sectional study
Intervention: High-carbohydrate meals vs. high-fat meals
Key Finding: Identified distinct, acute postprandial (after-meal) responses in both leptin and adiponectin based entirely on the macronutrient composition of the consumed meal.
Common Myths and Mistakes
Myth 1: "I Need to Lose a Lot of Weight Before My Hormones Improve"
Wrong. Research consistently shows that exercise improves adiponectin and leptin sensitivity even without significant weight loss. The Khalafi et al. (2023) meta-analysis found meaningful adipokine improvements within 8–12 weeks of lifestyle intervention — often before major weight changes. Quality of lifestyle change matters more than the number on the scale, at least in the early stages.
Myth 2: "Supplements Can Replace Diet and Exercise for Leptin Optimization"
No evidence supports this. While certain compounds — including omega-3 fatty acids, magnesium, and berberine — have modest supportive effects on metabolic markers, no supplement has demonstrated the ability to meaningfully correct leptin resistance or raise adiponectin to the degree that diet and exercise can. Anyone selling a "leptin supplement" that promises dramatic results is marketing ahead of the science.
Myth 3: "Cutting Carbs is the Only Way to Lower Leptin"
Oversimplified. Leptin is primarily regulated by body fat mass, not carbohydrate intake per se. A high-carbohydrate diet built around legumes, whole grains, and vegetables produces very different adipokine effects than the same amount of carbohydrates from ultra-processed foods. Dietary quality and the overall energy balance matter far more than macronutrient ratios for most people.
Myth 4: "More Exercise is Always Better"
Not for adipokine optimization. Wang et al. (2025) clearly showed a dose-response plateau around 300–400 minutes per week. Exceeding this can elevate cortisol and counteract some of the hormonal benefits. Overtraining syndrome is associated with elevated inflammation, worsened insulin sensitivity, and disrupted hormonal balance. Consistency and recovery are as important as volume.
Myth 5: "If My BMI is Normal, My Adipokines Are Fine"
Dangerously wrong. People with "normal" BMI can have elevated visceral fat, low adiponectin, and leptin resistance — sometimes called metabolic obesity or "TOFI" (thin outside, fat inside). Waist circumference and, ideally, direct adipokine measurement are more informative than BMI alone.
Myth 6: "These Hormonal Changes Take Years"
False. The research is remarkably encouraging here. Measurable improvements in adipokine levels begin within 4–8 weeks of consistent lifestyle change, and clinically meaningful changes are typically seen by 12–16 weeks — well within a 3-month program. Patience is required, but the timeline is far shorter than most people assume.
Practical 12-Week Protocol
Use this structured, evidence-based program as your starting blueprint. Adjust based on your current fitness level and health status. Consult your doctor before beginning if you have existing health conditions.
Phase 1: Weeks 1–4 — Foundation Building
Diet:
Begin tracking meals using a food diary (paper or app) to establish baseline and identify ultra-processed food intake
Add one serving of legumes per day (lentil soup, hummus, bean salad)
Replace refined grain at one meal daily with a whole grain alternative
Reduce (not eliminate) added sugar: eliminate sugary drinks, reduce desserts to 2–3 times/week
Exercise:
Walk 30 minutes at a brisk pace, 5 days per week
Begin 2 resistance training sessions per week with bodyweight or light weights (focus on form, not intensity)
Add one 60-minute yoga class or guided yoga video per week
Lifestyle:
Set a consistent sleep schedule (same bedtime and wake time every day)
Begin a 10-minute daily mindfulness or breathing practice
Goal: Build habits, not results. Discomfort should be minimal. Consistency is the only metric that matters this month.
Phase 2: Weeks 5–8 — Progressive Overload
Diet:
Target 30g fiber per day (track it)
Increase vegetables to fill half your plate at every meal
Introduce 2 servings of fatty fish per week (salmon, mackerel, sardines) for omega-3s
Reduce alcohol to 2–3 drinks per week maximum
Exercise:
Progress aerobic to 200–250 minutes/week (mix brisk walking, jogging, cycling, or swimming)
Add progressive load to resistance training (increase weights or difficulty gradually)
Increase yoga or mindfulness movement to 2 sessions per week
Lifestyle:
Address sleep if duration is below 7 hours — implement strict screen-off policy 60 minutes before bed
Begin tracking waist circumference (measure weekly at the navel level, same time of day)
Goal: You should begin noticing changes in energy levels, appetite control, and possibly waist circumference by the end of this phase.
Phase 3: Weeks 9–12 — Optimization and Consolidation
Diet:
Aim for 85–90% of meals from whole, minimally processed foods
Experiment with meal timing: avoid eating within 2–3 hours of bedtime
Add one anti-inflammatory food daily: green tea, turmeric, berries, extra virgin olive oil
Optional: if clinically appropriate, consider 12–16 hour overnight fasting window
Exercise:
Achieve 250–300+ minutes of aerobic activity per week
Resistance training at 70–80% of your one-rep maximum for 8–12 reps
Maintain yoga/mind-body practice 2x per week
Begin adding light HIIT (1 session per week of 20–25 minutes) if well-tolerated
Lifestyle:
Re-evaluate stress levels and adjust time for stress management practices accordingly
Track how you feel: appetite, energy, mood, and hunger are real-world signals of improving leptin sensitivity
Consider discussing a fasting leptin, adiponectin, and LAR measurement with your doctor to objectively assess progress
Goal: By week 12, the research predicts clinically meaningful improvements in your adipokine profile. Maintain these habits — the evidence shows continued improvements for 6–12 months.
12-Week Nutrition Checklist
At least 5 servings of vegetables per day
3–4 servings of legumes per week
100% whole grain starches (zero refined grains)
2 servings of fatty fish per week
Extra virgin olive oil as primary cooking fat
30g+ dietary fiber per day
Zero sugary drinks (including fruit juice)
Alcohol ≤ 2–3 drinks per week
Zero ultra-processed foods
Green tea (2–3 cups daily) as beverage of choice
Frequently Asked Questions
Q: What are normal leptin and adiponectin levels, and should I get tested?
A: Reference ranges vary by laboratory and body composition. In general, for women (who naturally have higher leptin levels due to higher body fat percentage), leptin ranges from 3–18 ng/mL are considered normal for healthy weight; in men, 2–5 ng/mL. Adiponectin ranges from 5–15 μg/mL in healthy adults, with lower levels indicating higher metabolic risk. The leptin/adiponectin ratio (LAR) is increasingly considered a more meaningful biomarker. Testing is most useful for establishing a baseline and tracking treatment response. Ask your doctor if testing is appropriate for you.
Q: How long will it take to see real improvements in my leptin and adiponectin?
A: Based on the Khalafi et al. (2023) meta-analysis and other trial data, measurable improvements in adipokine levels typically begin within 4–8 weeks of consistent lifestyle change. Clinically meaningful, sustained changes — those that translate to reduced disease risk — are generally observed by 12–16 weeks. The full benefit accumulates over 6–12 months of continued adherence.
Q: Can I improve my adipokines without losing weight?
A: Yes, to a meaningful extent. Exercise has been shown to raise adiponectin and improve leptin sensitivity even in the absence of significant weight loss. However, reducing body fat percentage — particularly visceral fat — produces the largest and most durable adipokine improvements. The good news: visceral fat responds relatively quickly to lifestyle changes, often before the scale moves much.
Q: Is a ketogenic diet good or bad for leptin and adiponectin?
A: The evidence is mixed. Very-low-energy ketogenic therapies (VLEKT) — studied by Balestra et al. (2026) — improved the LAR in obese patients with fatty liver disease, suggesting benefits in specific clinical contexts. However, long-term ketogenic dieting may not optimize adiponectin as effectively as plant-rich, fiber-forward diets for most people, given the role of dietary fiber and gut microbiome health in adiponectin regulation. Standard moderate-carbohydrate, high-fiber, whole-food diets have the strongest and most consistent evidence base.
Q: Does intermittent fasting help with leptin and adiponectin?
A: Intermittent fasting (IF) can improve insulin sensitivity and promote fat loss, which indirectly benefits adipokine balance. Some studies show that time-restricted eating improves adiponectin levels and reduces leptin resistance. However, IF's benefits appear to be primarily driven by the caloric restriction it induces, not by the fasting period itself. It is a potentially useful tool, not a magic mechanism.
Q: Are there any supplements that meaningfully improve leptin and adiponectin?
A: Some supplements have modest, supportive evidence: omega-3 fatty acids (EPA/DHA) have anti-inflammatory effects that may modestly support adiponectin; magnesium deficiency is associated with lower adiponectin and correcting deficiency may help; berberine has insulin-sensitizing properties that may improve the adipokine environment. However, no supplement replaces or comes close to the effects of comprehensive lifestyle change. Use supplements, if at all, as adjuncts — not substitutes.
Q: Does the type of exercise matter, or is any movement beneficial?
A: All forms of physical activity improve adipokine balance compared to sedentary behavior. However, combined aerobic plus resistance training produces the best results. Wang et al. (2025) found that exercise modality is less important than total volume and consistency. The best exercise is the one you'll actually do regularly — whether that's yoga, walking, swimming, or weightlifting.
Q: Can stress and poor sleep really affect my metabolic hormones that significantly?
A: Absolutely, and this is often the missing link. Chronic cortisol elevation from psychological stress directly suppresses adiponectin production, promotes visceral fat deposition, and induces leptin resistance. A single night of poor sleep measurably disrupts leptin and ghrelin the very next morning. For people who eat well and exercise but still struggle metabolically, stress and sleep quality are often the overlooked culprits.
Q: Is leptin resistance the same as insulin resistance?
A: They are distinct but closely related conditions. Both involve a hormone being present at normal or elevated levels but failing to produce its intended cellular effect. They share common causes (visceral fat, inflammation, sedentary behavior) and common solutions (the lifestyle interventions described in this article). Many people with one condition also have the other. Insulin resistance is currently better understood and more widely tested, but leptin resistance may be equally clinically important.
Q: Are there differences between men and women in how these hormones work?
A: Yes, significant ones. Women naturally have higher leptin levels than men at any given body fat percentage — likely due to the role of leptin in reproductive function. The 2026 study by Aguirre-Cruz et al. found sex-specific differences in how the adiponectin/leptin ratio (ALR) associates with visceral fat and adipose tissue dysfunction. Postmenopausal women appear particularly vulnerable to adipokine dysregulation due to estrogen withdrawal. This underscores the importance of individualized assessment and the value of discussing your specific hormonal context with your healthcare provider.
Q: What if I have diabetes or heart disease — are these interventions safe?
A: The interventions described — plant-forward diet, moderate exercise, stress management, and improved sleep — are generally beneficial and appropriate for people with type 2 diabetes or established cardiovascular disease. However, the specific targets (caloric deficit, exercise intensity, and timing) need to be personalized, particularly if you take medications (insulin, antihypertensives, etc.) that can interact with significant lifestyle changes. Always work with your healthcare team to implement these changes safely.
Conclusion & Action Steps
Leptin resistance and low adiponectin are not fixed biological fates. They are modifiable metabolic states that respond — often powerfully and relatively quickly — to targeted, consistent lifestyle change.
The science from 2023–2026 delivers a remarkably consistent message:
Combine diet and exercise — the synergy is irreplaceable
Target visceral fat specifically — waist circumference is your most important metric
Go plant-forward — fiber, polyphenols, and whole foods create the ideal environment for adiponectin
Move consistently — 150–300 minutes of moderate aerobic activity weekly plus 2–3 resistance sessions
Don't neglect the mind-body dimension — yoga, sleep, and stress management address the cortisol pathway that conventional exercise misses
Be patient and persistent — 12 weeks of consistent effort produces measurable hormonal improvement; 6–12 months produces transformative change
The emerging evidence on the leptin/adiponectin ratio (LAR) as a clinical biomarker (Balestra et al., 2026; Aguirre-Cruz et al., 2026) also suggests we are moving toward more precise, personalized monitoring of metabolic health — beyond BMI and body weight alone. Ask your doctor whether tracking your LAR makes sense for your situation.
Your action steps for this week:
✅ Add one serving of legumes to your diet daily
✅ Commit to 30 minutes of brisk walking 5 days this week
✅ Set a consistent sleep and wake time and stick to it for 7 days
✅ Replace all sugary drinks with water or unsweetened tea
✅ Attend one yoga class or complete one 30-minute guided yoga session
✅ Talk to your healthcare provider about your metabolic risk and whether adipokine testing is appropriate
Small, consistent changes — not dramatic, unsustainable interventions — are what the research consistently shows to be most effective. You have far more power over your metabolic hormones than you may have realized.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Beyond Glucose: Lipotoxicity as the Central Mechanism of Metabolic Disease | DR T S DIDWAL
Time-Restricted Eating: Metabolic Advantage or Just Fewer Calories? | DR T S DIDWAL
Can You Revitalize Your Immune System? 7 Science-Backed Longevity Strategies | DR T S DIDWAL
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
Light and Longevity: Can Sunlight Slow Cellular Aging? | DR T S DIDWAL
References
Aguirre-Cruz, L., et al. (2026). The adiponectin/leptin ratio as a biomarker of adiposopathy and visceral adipose tissue accumulation: Sex-specific mechanisms. Adipocyte. Advance online publication. https://doi.org/10.1080/21623945.2026.2653961
Aisike, G., Kuerbanjiang, M., Muheyati, D., et al. (2023). Correlation analysis of obesity phenotypes with leptin and adiponectin. Scientific Reports, 13, Article 16202. https://doi.org/10.1038/s41598-023-43550-8
Balestra, F., Donghia, R., De Luca, M., Stabile, D., Coletta, S., Panzetta, G., Palieri, R., Di Chito, M., De Pergola, G., Giannelli, G., Pesole, P. L., & Scavo, M. P. (2026). Leptin/Adiponectin Ratio as a new multidimensional biomarker in obese patients with liver steatosis undergoing VLEKT: Results from a pilot study. Frontiers in Nutrition, 13, Article 1754299. https://doi.org/10.3389/fnut.2026.1754299
Bidulescu, A., Dinh, P. C., Sarwary, S., et al. (2020). Associations of leptin and adiponectin with incident type 2 diabetes and interactions among African Americans: The Jackson Heart Study. BMC Endocrine Disorders, 20, Article 68. https://doi.org/10.1186/s12902-020-0511-z
Boden, G. (2011). Obesity, insulin resistance and free fatty acids. Current Opinion in Endocrinology, Diabetes and Obesity, 18(2), 139–143. https://doi.org/10.1097/MED.0b013e32834445b9
Del Razo-Olvera, F. M., Arias-Marroquín, A. T., Martínez-Fajardo, M., Dávila-Olmedo, W. E., Cruz Bautista, I., Galán-Ramírez, G. A., Juárez-Martínez, L., Gómez-Velasco, D. V., Guillén-Pineda, L. E., López Estrada, A., Otero-Otero, R., Elías-López, D., Martagón-Rosado, A. J., Aguilar-Salinas, C., & Soto-Mota, A. (2026). Postprandial response of leptin and adiponectin to standardized high-carbohydrate and high-fat meals in adults: A cross-sectional study. PLoS ONE, 21(5), Article e0349380. https://doi.org/10.1371/journal.pone.0349380
Fisman, E. Z., & Tenenbaum, A. (2014). Adiponectin: A manifold therapeutic target for metabolic syndrome, diabetes, and coronary disease? Cardiovascular Diabetology, 13, Article 103. https://doi.org/10.1186/1475-2840-13-103
Frühbeck, G., Catalán, V., Rodríguez, A., et al. (2018). Adiponectin-leptin ratio: A promising index to estimate adipose tissue dysfunction. Relation with obesity-associated cardiometabolic risk. Adipocyte, 7(1), 57–62. https://doi.org/10.1080/21623945.2017.1402151
Kazeminasab, F., Fatemi, R., Bagheri, R., Santos, H. O., & Dutheil, F. (2024). Effects of plant-based diets combined with exercise training on leptin and adiponectin levels in adults with or without chronic diseases: A systematic review and meta-analysis of clinical studies. Frontiers in Nutrition, 11, Article 1465378. https://doi.org/10.3389/fnut.2024.1465378
Khalafi, M., Hossein Sakhaei, M., Kheradmand, S., Symonds, M. E., & Rosenkranz, S. K. (2023). The impact of exercise and dietary interventions on circulating leptin and adiponectin in individuals who are overweight and those with obesity: A systematic review and meta-analysis. Advances in Nutrition, 14(1), 128–146. https://doi.org/10.1016/j.advnut.2022.10.001
Koh, K. K., Park, S. M., & Quon, M. J. (2008). Leptin and cardiovascular disease: Response to therapeutic interventions. Circulation, 117(25), 3238–3249. https://doi.org/10.1161/CIRCULATIONAHA.107.741843
Larsen, M. A., Isaksen, V. T., Moen, O. S., et al. (2018). Leptin to adiponectin ratio — A surrogate biomarker for early detection of metabolic disturbances in obesity. Nutrition, Metabolism and Cardiovascular Diseases, 28(11), 1114–1121. https://doi.org/10.1016/j.numecd.2018.06.020
Moreira, R. J., Oliveira, P. F., Spadella, M. A., Ferreira, R., & Alves, M. G. (2025). Do lifestyle interventions mitigate the oxidative damage and inflammation induced by obesity in the testis? Antioxidants, 14(2), Article 150. https://doi.org/10.3390/antiox14020150
Myers, M. G., Leibel, R. L., Seeley, R. J., & Schwartz, M. W. (2010). Obesity and leptin resistance: Distinguishing cause from effect. Trends in Endocrinology and Metabolism, 21(11), 643–651. https://doi.org/10.1016/j.tem.2010.08.002
Ouchi, N., Parker, J. L., Lugus, J. J., & Walsh, K. (2011). Adipokines in inflammation and metabolic disease. Nature Reviews Immunology, 11(2), 85–97. https://doi.org/10.1038/nri2921
Sáinz, N., Barrenetxe, J., Moreno-Aliaga, M. J., & Martínez, J. A. (2015). Leptin resistance and diet-induced obesity: Central and peripheral actions of leptin. Metabolism, 64(1), 35–46. https://doi.org/10.1016/j.metabol.2014.10.015
Shimizu, R., Suzuki, H., Amitani, M., & Amitani, H. (2025). The effects of yoga on key adipocytokines in obesity: A narrative review of leptin and adiponectin. Cureus, 17(1), Article e76792. https://doi.org/10.7759/cureus.76792
Stefan, N., & Cusi, K. (2022). A global view of the interplay between non-alcoholic fatty liver disease and diabetes. The Lancet Diabetes & Endocrinology, 10(4), 284–296. https://doi.org/10.1016/S2213-8587(22)00003-1
Suder, A., Makiel, K., Targosz, A., et al. (2024). Effects of exercise and dietary interventions on asprosin, leptin, and lipid metabolism in males with abdominal obesity: A randomized controlled trial. Scientific Reports, 14, Article 28109. https://doi.org/10.1038/s41598-024-79853-7
Wang, H., Wang, H., Zhan, E., & Liu, X. (2025). Unveiling the perfect workout: Exercise modalities and dosages to ameliorate adipokine dysregulation in individuals with overweight and obesity: A systematic review with pairwise, network, and dose-response meta-analyses. Frontiers in Nutrition, 12, Article 1653449. https://doi.org/10.3389/fnut.2025.1653449
Author: Dr. T.S. Didwal, M.D. | Last Updated: June 2026 | Category: Metabolism, Hormones, Lifestyle Medicine
This article synthesizes evidence from peer-reviewed randomized controlled trials, systematic reviews, and meta-analyses. It is intended for educational purposes and does not constitute individualized medical advice.