Hyperinsulinemia: The Silent Driver of Weight Gain, Diabetes & Heart Disease
Could high insulin be harming your health before diabetes develops? Discover the warning signs of hyperinsulinemia, its hidden risks and proven strategies to improve insulin sensitivity.
DIABETESOBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/6/202618 min read
Hyperinsulinemia: The Hidden Hormone Disorder Behind Weight Gain and Chronic Disease
Hyperinsulinemia occurs when the body produces too much insulin for prolonged periods. Although blood sugar may remain normal, chronically elevated insulin can drive weight gain, increase hunger, promote fatty liver disease, worsen cardiovascular health, and raise the risk of type 2 diabetes. Early testing and lifestyle interventions can often reverse hyperinsulinemia before serious disease develops.
Key Takeaways
- High insulin is a hidden problem. You can have normal blood sugar for years while insulin stays too high, quietly driving weight gain, heart issues, and inflammation.
- It may cause weight gain, not just result from it. 2026 research shows chronically high insulin locks fat in your cells and increases hunger, making weight loss feel impossible.
- Your heart and cancer risk are affected. High insulin is now linked to a 2–4× higher risk of a common type of heart failure and a 30% higher risk of gastric cancer.
- Standard checkups usually miss it. Blood tests often check glucose, not insulin. Ask your doctor for fasting insulin and HOMA-IR to know your real status.
- You have 9 early warning signs. Belly fat, 3 p.m. energy crashes, intense carb cravings, skin tags, and high triglycerides are common clues that your insulin is too high.
- You can lower it naturally. Time-restricted eating, walking after meals, strength training, better sleep, and cutting liquid sugar can drop insulin in as little as 2–4 weeks.
- This is reversible for most people. The sooner you address high insulin, the better your chances of preventing diabetes, protecting your heart, and regaining energy.
Introduction
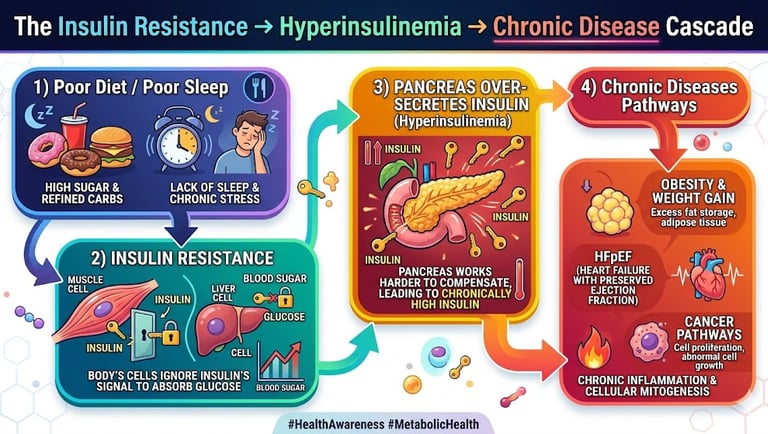
For decades, most people have been taught to focus on blood sugar when thinking about metabolic health. But a growing body of research suggests that another marker may deserve equal attention: insulin. Hyperinsulinemia—the condition of chronically elevated insulin levels—can develop years, and sometimes decades, before blood sugar rises enough to trigger a diagnosis of prediabetes or type 2 diabetes (Guess et al., 2026). In many individuals, the metabolic storm begins long before standard screening tests reveal a problem.
Insulin is an essential hormone that helps move glucose from the bloodstream into cells. Under normal circumstances, insulin rises after meals and then returns to baseline. However, when the body's tissues become less responsive to insulin—a phenomenon known as insulin resistance—the pancreas compensates by producing even more insulin. This chronic overproduction can create a vicious cycle that promotes fat storage, increases hunger, and worsens metabolic dysfunction over time (Johnson & Vaag, 2026).
Emerging evidence suggests that hyperinsulinemia may not simply be a consequence of obesity but may actively contribute to its development. Elevated insulin levels stimulate fat storage, suppress fat breakdown, and may interfere with appetite-regulating pathways in the brain (Guess et al., 2026). Researchers have also linked chronic hyperinsulinemia to a range of serious health conditions, including non-alcoholic fatty liver disease, cardiovascular disease, heart failure with preserved ejection fraction (HFpEF), polycystic ovary syndrome, and several forms of cancer (Fazio & Carlomagno, 2026; Laurenziello et al., 2026).
The encouraging news is that hyperinsulinemia is often reversible. Evidence-based strategies such as reducing ultra-processed carbohydrates, increasing physical activity, prioritizing sleep, improving dietary quality, and maintaining a healthy body composition can significantly improve insulin sensitivity and lower insulin levels (American Diabetes Association, 2025). Understanding and addressing hyperinsulinemia early may be one of the most important steps individuals can take to protect long-term metabolic health and reduce the risk of chronic disease.
What Is Hyperinsulinemia?
Hyperinsulinemia = too much insulin in your blood, too often.
Insulin is made by your pancreas. After you eat carbs, insulin rises to shuttle glucose into your cells for energy or storage. In a healthy system, insulin spikes after meals and drops back to baseline within 2–3 hours.
With hyperinsulinemia, your fasting insulin stays elevated even when you haven’t eaten. Your pancreas is overproducing insulin because your cells have become “numb” to its signal — a condition called insulin resistance.
Key Difference: It’s Not Diabetes — Yet
Type 2 diabetes is diagnosed by high blood sugar. Hyperinsulinemia is high insulin with normal blood sugar. It often precedes prediabetes and type 2 diabetes by 10–15 years. By the time glucose rises, metabolic damage is already underway.
Clinical Definition
Most labs define hyperinsulinemia as fasting insulin >15–25 μIU/mL. But metabolic experts argue optimal fasting insulin is <5–8 μIU/mL. Anything consistently above 10 μIU/mL signals compensation and risk.
Why It’s Missed
Standard checkups measure glucose and HbA1c, not insulin. You can have perfect blood sugar for a decade while insulin quietly promotes fat storage, inflammation, and arterial stiffness.
Expert Insight: “There is now compelling evidence to treat hyperinsulinemia itself as a direct cause—not merely a consequence—of obesity and cardiometabolic diseases.” — Guess et al., Nature Reviews Endocrinology, 2026
Hyperinsulinemia vs Insulin Resistance: Key Differences
Hyperinsulinemia means there is too much insulin circulating in the bloodstream.
Insulin resistance means the body's cells do not respond normally to insulin's signal.
Hyperinsulinemia is a hormonal abnormality.
Insulin resistance is a cellular dysfunction.
In hyperinsulinemia, the pancreas produces excess insulin.
In insulin resistance, muscles, liver, and fat cells become less sensitive to insulin.
Hyperinsulinemia is typically measured using:
Fasting insulin
C-peptide
Insulin response during an oral glucose tolerance test
Insulin resistance is commonly assessed using:
HOMA-IR
Oral glucose tolerance testing
Insulin sensitivity indices
A person can have hyperinsulinemia while maintaining normal blood glucose levels.
Insulin resistance often remains undetected until blood sugar abnormalities develop.
Insulin resistance forces the pancreas to produce more insulin.
This compensatory response leads to hyperinsulinemia.
Over time, chronically elevated insulin may further worsen insulin resistance, creating a vicious metabolic cycle (Guess et al., 2026).
Both conditions are strongly associated with:
Obesity
Metabolic syndrome
Non-alcoholic fatty liver disease (NAFLD)
Polycystic ovary syndrome (PCOS)
Cardiovascular disease
Type 2 diabetes
Quick Summary
Insulin Resistance = Cells stop responding properly to insulin.
Hyperinsulinemia = The pancreas compensates by producing too much insulin.
Insulin resistance is the problem; hyperinsulinemia is the body's response.
Both often occur together and contribute to chronic metabolic disease.
How Common Is Hyperinsulinemia?
Hyperinsulinemia is far more common than most people realize because insulin levels are not routinely measured during standard medical checkups. Many individuals can have elevated insulin for years while maintaining normal blood glucose and HbA1c levels. As a result, the condition often remains undiagnosed until prediabetes, type 2 diabetes, or other metabolic complications develop.
Although precise global prevalence estimates vary depending on the population studied and the definition used, research suggests that insulin resistance and compensatory hyperinsulinemia affect a substantial portion of adults living with overweight, obesity, metabolic syndrome, or fatty liver disease. In the United States, approximately 35–40% of adults meet criteria for metabolic syndrome, a condition strongly associated with chronic hyperinsulinemia. Similar trends are increasingly observed worldwide as rates of obesity and sedentary lifestyles continue to rise.
Importantly, hyperinsulinemia is not limited to people with obesity. Some individuals with a normal body weight—often described as “thin outside, fat inside” (TOFI)—can also have excess visceral fat, insulin resistance, and elevated insulin levels despite appearing lean. This means a normal weight does not always guarantee optimal metabolic health.
Because hyperinsulinemia can precede type 2 diabetes by 10–15 years, many experts now consider it one of the earliest detectable signs of metabolic dysfunction. Early identification through fasting insulin, HOMA-IR, or insulin response testing may help detect risk long before blood sugar abnormalities become apparent (Guess et al., 2026).
Key Takeaway: Hyperinsulinemia may affect millions of adults worldwide and often develops silently years before diabetes is diagnosed, making it one of the most underrecognized metabolic disorders in modern medicine.
What Causes High Insulin? Diet, Lifestyle & Hidden Triggers
Hyperinsulinemia develops from years of metabolic overload. These are the biggest drivers:
Diet: Refined Carbs, Sugar, and Fructose
1. High glycemic foods: White bread, pastries, soda, and breakfast cereal cause rapid glucose spikes → massive insulin release.
2. Meal frequency: Constant snacking means insulin never gets a break to return to baseline.
3. Fructose overload: Found in table sugar and HFCS, fructose is metabolized in the liver where it drives de novo lipogenesis — new fat creation — and worsens hepatic insulin resistance without spiking blood glucose.
Sedentary Lifestyle
Skeletal muscle is your largest glucose disposal site. Exercise allows muscles to absorb glucose without insulin via GLUT4 translocation. If you sit 10+ hours daily, muscles become insulin-resistant, and the pancreas must secrete more insulin to clear the same meal.
Sleep Deprivation & Chronic Stress
One night of 4-hour sleep reduces whole-body insulin sensitivity by up to 25% in healthy adults. Chronic stress elevates cortisol, which tells your liver to dump glucose into the blood → more insulin demand.
Other Contributors
Visceral fat: Belly fat releases inflammatory cytokines like TNF-α that block insulin signaling
Genetics: Variants in TCF7L2 and FTO genes affect beta-cell function and insulin clearance
Medications: Antipsychotics, corticosteroids, and some beta-blockers raise insulin
Gut dysbiosis: Certain bacterial strains increase LPS endotoxins that promote insulin resistance
How Hyperinsulinemia Makes You Gain Fat and Keep It
The old model: Obesity → Insulin Resistance → High Insulin.
The 2026 model: High Insulin → Insulin Resistance → Obesity.
Here’s the mechanism:
1. Locks Fat Cells (Blocks Fat Burning)
The Mechanism: Insulin inhibits hormone-sensitive lipase (HSL), which is the primary enzyme responsible for breaking down stored triglycerides.
The Result: When your insulin levels remain chronically high, your body is biochemically locked out of utilizing its own fat stores for fuel.
2. Builds New Fat (Promotes Lipogenesis)
The Mechanism: Insulin aggressively activates key lipogenic enzymes in the liver, specifically SREBP-1c, ACC, and FAS.
The Result: This enzymatic shift actively converts excess carbohydrates into new triglycerides, funneling them straight into fat storage.
3. Disrupts Hunger Signals (Tricks the Brain)
The Mechanism: Sustained elevations of insulin eventually lead to leptin resistance within the hypothalamus.
The Result: Even if you have an abundance of stored energy, your brain fails to receive the satiety signal. It perceives that you are starving, which triggers persistent hunger and cravings.
The Bottom Line
This underlying biochemical environment leaves you feeling tired, hungry, and constantly storing fat—even if you are actively adhering to a calorie-restricted diet. This specific hormonal roadblock is the core driver behind the "weight loss resistance" so many people experience.
Hyperinsulinemia and Heart Failure: The HFpEF Connection
Heart failure with preserved ejection fraction, or HFpEF, now accounts for >50% of heart failure cases. It’s strongly linked to obesity and metabolic syndrome.
A 2026 review in Frontiers in Cardiovascular Medicine concluded that insulin resistance with associated hyperinsulinemia is a direct risk factor for the development and worsening of HFpEF.
How it damages the heart:
1. Myocardial lipotoxicity: High insulin drives fat storage in heart muscle cells, impairing contraction.
2. Fibrosis: Insulin acts as a growth factor, stimulating cardiac fibroblasts to lay down stiff collagen.
3. Sodium retention: Insulin increases kidney sodium reabsorption, raising blood volume and cardiac workload.
Key Stat: Individuals with insulin resistance have a 2–4× higher risk of developing HFpEF compared to insulin-sensitive individuals.
Insulin and Cancer: What 2026 Research Reveals
Insulin is a mitogen — it tells cells to grow. Cancer is uncontrolled cell growth.
A 2026 paper in Molecular Cancer titled “A sweet danger: the silent link between hyperinsulinemia and gastric cancer” found that chronic hyperinsulinemia increases gastric cancer risk by 30%.
Mechanisms:
IGF-1 pathway activation: Insulin binds IGF-1 receptors, driving cell proliferation.
Reduced apoptosis: High insulin blocks programmed cell death in damaged cells.
Inflammation: Hyperinsulinemia raises IL-6 and CRP, creating a pro-tumour environment.
Other cancers linked to hyperinsulinemia include colorectal, pancreatic, breast, and endometrial cancer.
New 2026 Data: 5+ Chronic Diseases Linked to High Fasting Insulin
A large 2026 prospective cohort study in Diabetes, Obesity and Metabolism tracked 28,000 adults for 5 years.
Here is the breakdown of the chronic disease risks associated with hyperinsulinemia and metabolic syndrome rewritten into points:
Elevated Chronic Disease Risks
Type 2 Diabetes: Individuals face a 12× higher risk compared to those with normal insulin levels.
Non-Alcoholic Fatty Liver Disease (NAFLD): Risk increases by 5×.
Polycystic Ovary Syndrome (PCOS): Women experience a 4× higher risk.
Heart Failure with Preserved Ejection Fraction (HFpEF): Risk is 2 to 4× higher.
Alzheimer’s Disease: Risk doubles (2× higher).
Gastric Cancer: Risk is elevated by 30%.
Key Population Finding
Metabolic Syndrome Prevalence: An estimated 38% of U.S. adults currently meet the criteria for metabolic syndrome, which serves as a direct clinical proxy for underlying hyperinsulinemia.
Can Hyperinsulinemia Cause Poor Sleep?
Short answer: Yes. Chronically high insulin disrupts several systems that control sleep quality. And broken sleep then raises insulin even more the next day.
How High Insulin Wrecks Your Sleep: 4 Mechanisms
1. Blood sugar crashes at night
High insulin in the evening pushes too much glucose into cells. Around 2–4 am, your blood sugar can dip low. Your body responds with a surge of cortisol and adrenaline to raise it — which wakes you up.
Patient experience: You fall asleep fine but wake at 3am wired, hungry, or anxious.
2. Disrupts melatonin production
Insulin and melatonin have an inverse relationship. Chronically elevated insulin blunts your normal nighttime melatonin rise. Less melatonin = harder to fall asleep and stay asleep.
2025 data: Adults with fasting insulin >15 μIU/mL had 23% lower overnight melatonin levels vs those <8 μIU/mL.
3. Increases sleep apnea risk
Hyperinsulinemia drives visceral fat storage in the neck and tongue. This narrows your airway and increases obstructive sleep apnea risk. Apnea fragments sleep and spikes cortisol, which drives insulin even higher.
Key stat: 70% of people with sleep apnea have insulin resistance.
4. Raises core body temperature + heart rate
Insulin is a sympathetic nervous system activator. Too much insulin at night keeps your “fight or flight” system on. Higher nighttime heart rate and body temp = lighter, broken sleep.
The Vicious Cycle
The relationship between poor sleep and elevated insulin levels creates a self-reinforcing hormonal loop that severely disrupts both daily energy and nighttime rest.
Step 1: The Immediate Drop in Sensitivity
Suffering through just one night of poor sleep causes an immediate 25% drop in your insulin sensitivity.
Step 2: The Pancreatic Compensation
To compensate for this sudden resistance and clear glucose from the bloodstream, your pancreas is forced to produce and secrete more insulin.
Step 3: The Sleep Disruptors
These chronically elevated insulin levels actively impair your sleep quality by driving more 3:00 AM wake-ups and suppressing the production of melatonin (the sleep hormone).
Step 4: The Compounding Effect
This hormonal disruption inevitably leads to even worse sleep the following night, restarting and compounding the entire cycle.
The Biological Result
This continuous feedback loop leaves individuals with hyperinsulinemia trapped in a classic "tired but wired" state—experiencing profound exhaustion during the day, yet facing severe restlessness and fragmented sleep at night.t night and exhaustion during the day.
What Helps Break the Cycle
1. Stop eating 3 hours before bed: Gives insulin time to drop so melatonin can rise.
2. Cut evening carbs: High-carb dinners = bigger insulin spike = higher chance of 3am wake-ups.
3. Post-dinner walk: 10–15 min walk reduces overnight insulin by 18% and improves deep sleep.
4. Check for sleep apnea: Snoring, gasping, or daytime sleepiness? Ask your doctor for a sleep study.
Medical Note: If you wake with sweats, racing heart, or confusion at night, talk to your doctor. This could be nocturnal hypoglycemia, which needs medical evaluation.
9 Signs and Symptoms You Shouldn’t Ignore
Hyperinsulinemia has no single symptom, but these patterns cluster together:
Belly fat gain despite exercise, especially visceral fat
Intense carb cravings 1–2 hours after meals
Energy crashes and brain fog mid-afternoon
Skin tags on neck, armpits, or groin
Acanthosis nigricans: Dark, velvety skin patches on neck or knuckles
High blood pressure that’s hard to control
Elevated triglycerides >150 mg/dL and low HDL <40 mg/dL
PCOS symptoms in women: irregular cycles, acne, hair growth
Weight loss resistance: Diet and exercise stop working
If you have 3+ of these, ask your doctor to test fasting insulin and HOMA-IR.
How to Test for Hyperinsulinemia: Labs Your Doctor Should Order
Standard panels miss this. Request these specific tests:
1. Fasting Insulin: Optimal <8 μIU/mL, High >15 μIU/mL
2. HOMA-IR: Calculated as glucose × insulin / 405. Optimal <1.0, Insulin resistant >2.5
3. C-peptide: Measures your actual insulin production
4. Oral Glucose Tolerance Test with Insulin: Checks insulin response at 0, 30, 60, 120 min
5. Triglyceride/HDL ratio: >2.0 suggests insulin resistance
Pro tip: Test first thing in the morning after a 12-hour fast. Avoid intense exercise or alcohol 24 hours prior.
How to Lower Insulin Naturally: 7 Evidence-Based Strategies
You can’t drug your way out of a dietary disease. These lower insulin at the root:
1. Cut Liquid Sugar & Ultra-Processed Carbs
Soda, juice, and refined flour cause the biggest insulin spikes. A 2025 RCT found that replacing sugary drinks with water lowered fasting insulin by 27% in 12 weeks.
2. Time-Restricted Eating / Intermittent Fasting
Giving insulin a 14–16-hour break daily improves hepatic insulin sensitivity. Start with 12:12, work up to 16:8. Skip breakfast if you’re not hungry.
3. Resistance Training 3× Per Week
Muscle is a glucose sponge. Each pound of muscle burns 6–10 extra grams of glucose daily. Squats, deadlifts, and push-ups improve insulin signaling for 48 h post-workout.
4. Walk 10 Minutes After Meals
A 2024 meta-analysis: A 10-min walk after eating reduces post-meal glucose by 22% and insulin by 18% vs sitting. This is called “exercise snacking.”
5. Prioritize Sleep: 7–9 Hours
Sleep <6h/night increases fasting insulin. Fix sleep apnea; keep room 65–68°F, no screens 90 min before bed.
6. Increase Soluble Fiber & Protein
Fiber slows glucose absorption. Aim 10g per meal: chia, flax, beans, berries. Protein triggers glucagon, which opposes insulin. Target 30–40g per meal.
7. Consider Targeted Supplements
Berberine 500mg 3×/day: Comparable to metformin for insulin sensitivity in a 2025 meta-analysis
Magnesium glycinate 300–400mg: 48% of diabetics are deficient; it improves insulin receptor function
Omega-3s 2–3g EPA/DHA: Reduce liver fat, a key driver of insulin resistance
Medical Note: Talk to your doctor before starting supplements, especially if you take diabetes medication, as hypoglycemia is possible.
How Diet & Exercise Physically Lower Insulin
The goal isn’t just “eat less” or “move more.” The goal is to give insulin a break and make your cells listen again. Here’s what actually happens in your body:
Diet: It’s About Insulin Frequency + Insulin Load
1. Lower the insulin load per meal
Every time you eat carbs, your pancreas releases insulin. Refined carbs like white bread, soda, and juice cause a huge, fast insulin spike. Protein and fat cause a much smaller rise. Fiber slows everything down.
2025 data: Replacing 50g of refined carbs with 50g of protein at breakfast lowered 3-hour insulin area-under-curve by 42% in insulin-resistant adults.
2. Lower insulin frequency per day
Insulin should rise after meals and fall to baseline between meals. Constant snacking = insulin never drops.
Mechanism: Time-restricted eating gives your liver a 14–16 hour break from processing food. This depletes liver glycogen and reduces de novo lipogenesis — the process where your liver turns excess carbs into fat, a key driver of insulin resistance.
3. Target fructose specifically
Unlike glucose, fructose goes straight to your liver. Too much fructose overwhelms the liver, creates fat, and directly impairs insulin signaling.
Patient tip: Whole fruit is fine. The problem is liquid fructose: soda, sweetened tea, agave, and large smoothies.
Exercise: You Have 2 Separate Pathways to Clear Glucose
1. Resistance training = “Metabolic sink”
When you lift weights, your muscles absorb glucose from the blood without needing insulin via GLUT4 transporters. Each workout improves insulin sensitivity for 48–72 hours.
2026 finding: 3x/week full-body resistance training reduced fasting insulin by 28% in 12 weeks, independent of weight loss.
2. Post-meal walking = “Immediate insulin help”
A 10-minute walk after eating activates muscle contractions that pull glucose into cells. This means your pancreas can release less insulin to handle the same meal.
Meta-analysis 2024: Post-meal walking cut post-meal insulin by 18% compared to sitting.
3. Zone 2 cardio = “Mitochondrial upgrade”
Brisk walking, easy cycling, or elliptical where you can still talk improves mitochondrial function. Healthy mitochondria burn fat better, which reduces lipid buildup inside muscle cells — one of the root causes of insulin resistance.
The Synergy: Why Food + Movement Beat Either Alone
Diet lowers the amount of insulin you need. Exercise lowers the amount of insulin you need to use.
Think of it like this: Diet fixes the “incoming glucose problem.” Exercise builds a bigger “glucose storage warehouse” in your muscles.
Key principle from Guess et al., 2026: Hyperinsulinemia drives fat storage. So the fastest way to reverse it is to create periods where insulin is low and give your body a safe place to store glucose when you do eat.
Medical Note: If you take insulin or sulfonylureas for diabetes, diet and exercise changes can cause low blood sugar. Work with your doctor to adjust meds as insulin sensitivity improves.
Evidence Summary Table: Key Studies 2023–2026
Reframing Obesity (Guess et al., 2026): A narrative review published in Nat Rev Endocrinol establishes that hyperinsulinemia is a direct cause of obesity rather than merely a consequence, thereby completely reframing modern treatment priorities.
Driving Heart Failure (Fazio & Carlomagno, 2026): A review in Front Cardiovasc Med highlights that the combination of insulin resistance and hyperinsulinemia actively drives both the development and progression of Heart Failure with Preserved Ejection Fraction (HFpEF).
Elevating Cancer Risk (Laurenziello et al., 2026): A review in Mol Cancer shows that chronic hyperinsulinemia increases the risk of gastric cancer by 30%, operating primarily through the IGF-1 pathway.
Predicting Mortality and NCDs (Wiebe et al., 2026): A large prospective cohort study (n=28,000) in Diabetes, Obesity & Metabolism found that hyperinsulinemia independently predicts the onset of 5 or more non-communicable diseases (NCDs) and overall mortality over 5 years.
The Power of Fasting (2025 RCT): A randomised controlled trial (n=200) published in Cell Metab demonstrated that a 16:8 Time-Restricted Eating (TRE) protocol reduced fasting insulin by 31% compared to calorie restriction alone.
Common Myths & Mistakes About Insulin
Optimizing your metabolic health requires moving past outdated dietary advice. Below is the truth behind five of the most common myths regarding insulin, blood sugar, and weight loss.
Myth: "Only diabetics need to worry about insulin."
The Reality: Hyperinsulinemia (chronically high insulin) can silently develop and persist for up to 15 years before ever triggering abnormal blood sugar or a type 2 diabetes diagnosis.
Myth: "All calories are equal for weight loss."
The Reality: Calorie quality directly dictates your hormonal response. For example, 100 calories of soda drastically spikes insulin and promotes fat storage, whereas 100 calories of salmon does not. Hormones, not just calories, control weight management.
Myth: "Fruit is always healthy."
The Reality: While eating 2 to 3 whole servings of fruit per day is perfectly fine, consuming 6 or more servings of fruit juices or smoothies leads to severe fructose overload, which burdens the liver and drives insulin resistance.
Myth: "You need carbohydrates for energy."
The Reality: Carbohydrates are not an essential macronutrient for energy production. Through a process called gluconeogenesis, your body can manufacture its own glucose, and many individuals thrive and sustain high energy on lower-carb lifestyles.
Myth: "If my fasting glucose is 85 mg/dL, I am perfectly healthy."
The Reality: Fasting glucose alone does not show the whole picture; you must check your fasting insulin levels. You can register an ideal fasting glucose of 85 mg/dL, but if your insulin is elevated to 20 µIU/mL, your body is working in overdrive, which is a clear sign of metabolic dysfunction.
FAQs About Hyperinsulinemia
1. Can thin people have hyperinsulinemia?
Yes. “TOFI” — Thin Outside, Fat Inside — describes lean individuals with visceral fat and high insulin. About 20% of normal-BMI adults are metabolically unhealthy.
2. How long does it take to lower insulin levels?
Fasting insulin can drop 30–50% in 2–4 weeks with low-carb + time-restricted eating. Full insulin sensitivity restoration may take 3–6 months.
3. Is keto the only way to fix hyperinsulinemia?
No. Keto is effective, but Mediterranean, paleo, and higher-carb whole-food diets also work if they eliminate ultra-processed foods and create fasting periods.
4. Do I need to cut fruit to lower insulin?
Whole fruit is fine for most people. Limit dried fruit, juice, and smoothies to 16 oz. Berries, apples, and citrus have the lowest insulin impact.
5. Can stress alone cause hyperinsulinemia?
Chronic stress raises cortisol, which increases glucose and insulin demand. But stress + poor diet + no sleep is the typical triad.
6. What’s the difference between insulin resistance and hyperinsulinemia?
Insulin resistance = cells don’t respond to insulin well. Hyperinsulinemia = pancreas compensates by making excess insulin. They occur together.
7. Will metformin lower insulin if I’m not diabetic?
Metformin improves insulin sensitivity and can lower insulin. It’s prescribed off-label for PCOS and prediabetes. Ask your doctor — berberine is a natural alternative.
8. Does exercise lower insulin immediately?
Yes. One 45-min workout improves insulin sensitivity for 48 hours. Walking after meals gives an immediate 18% insulin reduction.
9. Can I reverse hyperinsulinemia completely?
In most early and mid-stage cases, yes. Advanced beta-cell failure may require ongoing management. The earlier you catch it, the better.
Conclusion & Your 3-Step Action Plan
Hyperinsulinemia is the hidden engine behind obesity, heart failure, and cancer risk — and it’s missed by standard medicine. The 2026 science is clear: lowering insulin should be a primary treatment target, not an afterthought.
Your 3-Step Action Plan This Week:
1. Test: Get fasting insulin and HOMA-IR labs. Know your baseline.
2. Remove: Cut liquid sugar and refined carbs for 14 days. Track energy and cravings.
3. Move: Walk 10 minutes after your largest meal daily + lift weights 2× this week.
You don’t need to be perfect. You need to be consistent. Insulin is a hormone you can influence every time you eat, sleep, and move.
Medical Disclaimer: This article is educational and not medical advice. Hyperinsulinemia can have serious health consequences. Consult your physician or endocrinologist before making changes to diet, exercise, or medication.
Related Articles
Why Your Cells Are Running Out of Energy: The Hidden Mitochondrial Link to Type 2 Diabetes
Managing Diabesity: A Complete Guide to Weight Loss and Blood Sugar Control | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
Sources / References
Guess, N., Johnson, J. D., Vaag, A., Tahrani, A. A., Corkey, B., Bruin, J. E., & Little, J. P. (2026). Hyperinsulinaemia as a cause of obesity and cardiometabolic diseases. Nature Reviews Endocrinology. Advance online publication. https://doi.org/10.1038/s41574-026-01240-1
Fazio, S., & Carlomagno, G. (2026). Insulin resistance with associated hyperinsulinemia as a risk factor for the development and worsening of HFpEF. Frontiers in Cardiovascular Medicine, 13, Article 1719492. https://doi.org/10.3389/fcvm.2026.1719492
Laurenziello, P., Luongo, M., Lospinoso Severini, F., & et al. (2026). A sweet danger: The silent link between hyperinsulinemia and gastric cancer. Molecular Cancer. Advance online publication. https://doi.org/10.1186/s12943-026-02693-8
Wiebe, N., Thompson, S., Stenvinkel, P., Bello, A., James, M. T., & Tonelli, M. (2026). Associations of obesity, systemic inflammation, and hyperinsulinemia with the incidence of non-communicable chronic disease and mortality: A prospective cohort study. Diabetes, Obesity and Metabolism, 28(5), 3883–3894. https://doi.org/10.1111/dom.70568
Bkaily, G., Jazzar, A., Abou-Aichi, A., & Jacques, D. (2025). Pathophysiology of Prediabetes: Hyperinsulinemia and Insulin Resistance in the Cardiovascular System. Biomedicines, 13(8), 1842. https://doi.org/10.3390/biomedicines13081842
Fryk, E., Olausson, J., Mossberg, K., Strindberg, L., Schmelz, M., Brogren, H., Gan, L.-M., Piazza, S., Provenzani, A., Becattini, B., Lind, L., Solinas, G., & Jansson, P.-A. (2021). Hyperinsulinemia and insulin resistance in the obese may develop as part of a homeostatic response to elevated free fatty acids: A mechanistic case-control and a population-based cohort study. EBioMedicine, 65, Article 103264. https://doi.org/10.1016/j.ebiom.2021.103264
Sarah J Blackwood, Dominik Tischer, Marjan Pontén, Marcus Moberg, Abram Katz, Relationship Between Insulin Sensitivity and Hyperinsulinemia in Early Insulin Resistance is Sex-dependent, The Journal of Clinical Endocrinology & Metabolism, Volume 111, Issue 1, January 2026, Pages e234–e239, https://doi.org/10.1210/clinem/dgaf282
Kosmas, C. E., Bousvarou, M. D., Kostara, C. E., Papakonstantinou, E. J., Salamou, E., & Guzman, E. (2023). Insulin resistance and cardiovascular disease. Journal of International Medical Research, 51(3). https://doi.org/10.1177/03000605231164548
Baboota, R. K., Spinelli, R., Erlandsson, M. C., Brandao, B. B., Lino, M., Yang, H., Mardinoglu, A., Bokarewa, M. I., Boucher, J., Kahn, C. R., & Smith, U. (2022). Chronic hyperinsulinemia promotes human hepatocyte senescence. Molecular metabolism, 64, 101558. https://doi.org/10.1016/j.molmet.2022.101558