Why Your Cells Are Running Out of Energy: The Hidden Mitochondrial Link to Type 2 Diabetes
Can improving mitochondrial health help prevent diabetes? Explore the emerging science behind metabolism, ATP production, and insulin resistance.
DIABETES
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/17/202614 min read
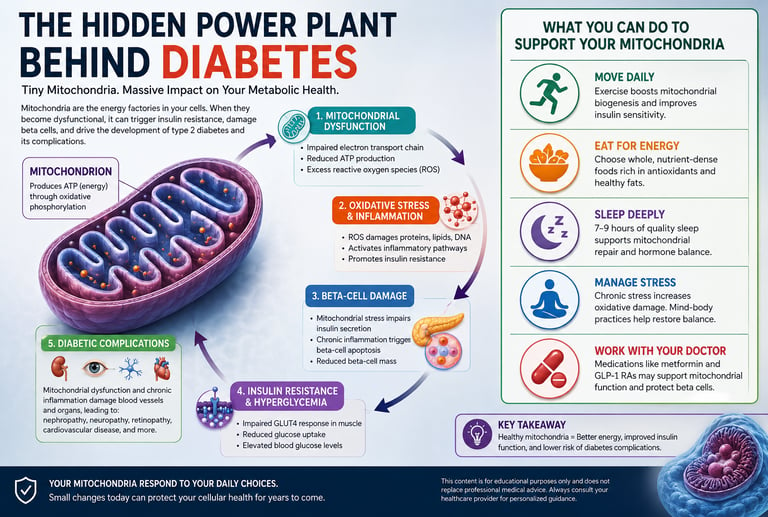
Type 2 diabetes is often described as a disease of high blood sugar. But emerging science suggests that long before glucose levels rise into the diabetic range, a deeper problem may already be unfolding inside your cells: an energy crisis at the mitochondrial level. Mitochondria — the microscopic structures responsible for producing cellular energy — are increasingly being recognized not merely as innocent bystanders in diabetes, but as central drivers of metabolic dysfunction itself (Feng et al., 2025; Ge et al., 2025).
This shift in understanding is transforming how researchers think about the origins of insulin resistance, beta-cell failure, and diabetic complications. Traditionally, type 2 diabetes was viewed primarily as a disorder of excessive calorie intake, obesity, and impaired insulin action. While those factors remain critically important, modern metabolic research now reveals that mitochondrial dysfunction may appear years before overt diabetes develops, silently disrupting how cells process glucose and fat (Darwish et al., 2025).
When mitochondria become inefficient, cells struggle to generate adequate amounts of ATP — the energy currency required for nearly every biological process. In response, harmful reactive oxygen species (ROS) begin to accumulate, triggering oxidative stress, chronic inflammation, and progressive insulin resistance (Yadav et al., 2026). Over time, this metabolic stress damages pancreatic beta cells, impairs insulin secretion, and accelerates the progression toward full-blown diabetes.
What makes this discovery especially important is that mitochondria are highly responsive to lifestyle and environmental signals. Exercise, sleep, nutrition, stress levels, and even meal timing can profoundly influence mitochondrial function and metabolic health (Chen et al., 2025). In other words, the earliest stages of diabetes may begin not simply in the bloodstream, but within the tiny cellular power plants that determine whether your metabolism thrives — or slowly breaks down.
KEY INSIGHT
Mitochondrial dysfunction is not just a symptom of type 2 diabetes — emerging research suggests it is one of its root causes. Understanding this connection opens entirely new avenues for prevention and treatment.
1. What Are Mitochondria — And Why Do They Matter in Diabetes?
To understand how mitochondria contribute to diabetes, it helps to appreciate what they actually do. Mitochondria are responsible for producing adenosine triphosphate (ATP), the molecule your cells use as fuel for virtually every biological process — from muscle contractions to insulin secretion. They accomplish this through a process called oxidative phosphorylation, which uses oxygen and nutrients (primarily glucose and fatty acids) to generate ATP.
In people without diabetes, this energy production system works with extraordinary precision. Glucose from food enters the bloodstream, triggers insulin release from beta cells in the pancreas, and is transported into cells where mitochondria convert it into ATP. The whole system is elegantly coordinated.
In type 2 diabetes, this coordination breaks down. Recent research by Feng et al. (2025), published in Frontiers in Endocrinology, reveals that mitochondrial bioenergetics dysfunction — a failure of the cellular energy-generation process — forms a critical link between oxidative stress and insulin resistance, two hallmarks of T2DM. When mitochondria cannot efficiently produce ATP, cells experience an energy deficit that triggers a cascade of damaging molecular events.
Skeletal muscle mitochondria also play a major role in insulin sensitivity. When mitochondrial fatty acid oxidation becomes impaired, fat-derived metabolites begin accumulating inside muscle cells — a process known as intramyocellular lipid accumulation. These lipid byproducts interfere with insulin signaling and reduce GLUT4 responsiveness, making it harder for muscle cells to absorb glucose from the bloodstream. Over time, this contributes directly to insulin resistance and worsening metabolic dysfunction.
The liver is also highly vulnerable to mitochondrial dysfunction. When hepatic mitochondria become overloaded by excess fat and nutrient influx, fatty acid oxidation declines and de novo lipogenesis increases, promoting fatty liver disease (NAFLD), hepatic insulin resistance, and excessive glucose production — all major drivers of type 2 diabetes progression.
2. The Oxidative Stress Spiral: How Energy Failure Triggers Inflammation
One of the most important discoveries in diabetes research is the concept of the 'oxidative stress spiral.' When mitochondria are dysfunctional, they generate excessive amounts of reactive oxygen species (ROS) — unstable molecules that cause widespread damage to proteins, fats, and DNA. This oxidative stress, in turn, impairs mitochondrial function even further, creating a self-reinforcing cycle of deterioration.
A 2026 study by Yadav and colleagues, published in Molecular Biology Reports, explains this mechanism with striking clarity. The researchers outline how mitochondrial dysfunction-driven inflammation and beta-cell apoptosis (programmed cell death) are central to the progression of T2DM. When pancreatic beta cells — the very cells responsible for producing insulin — are subjected to chronic oxidative stress and inflammatory signaling, they become dysfunctional and eventually die.
The implications are profound. Beta-cell mass, once lost, is extraordinarily difficult to recover. This means that by the time a formal diabetes diagnosis is made, significant and potentially irreversible cellular damage may have already occurred. This makes early detection of mitochondrial dysfunction a genuinely promising frontier in diabetes prevention.
Visceral fat also contributes directly to mitochondrial dysfunction. Unlike subcutaneous fat, visceral adipose tissue releases large amounts of inflammatory cytokines and free fatty acids into the circulation, overwhelming mitochondrial energy metabolism and amplifying oxidative stress, insulin resistance, and chronic inflammation throughout the body.
Beta cells — the insulin-producing cells in your pancreas — are particularly vulnerable to mitochondrial damage. Once lost, they are hard to replace. This is why early intervention matters enormously in managing diabetes risk.
3. Mitochondrial Quality Control: The Body's Own Repair System
The human body is not entirely helpless in the face of mitochondrial damage. Cells have developed a sophisticated system known as mitochondrial quality control (MQC) to identify, repair, and remove damaged mitochondria. This system includes several key processes:
• Mitophagy: The selective degradation and recycling of damaged mitochondria
• Mitochondrial biogenesis: The creation of new, healthy mitochondria
• Mitochondrial dynamics: The continuous fusion and fission (splitting) of mitochondria to maintain quality
• Unfolded protein response: Molecular stress pathways that attempt to restore protein homeostasis
A comprehensive 2025 review by Chen and colleagues, published in Cell Death & Disease, provides a detailed map of how these quality control mechanisms go wrong in diabetes and its complications. The researchers found that in people with T2DM, all major MQC pathways are impaired — mitophagy is insufficient, biogenesis is reduced, and the balance between fusion and fission is disrupted. The result is an accumulation of damaged, dysfunctional mitochondria that perpetuate oxidative stress and inflammation.
Crucially, Chen et al. (2025) also identify MQC pathways as promising therapeutic targets. Pharmacological and lifestyle-based interventions that enhance mitophagy, stimulate biogenesis, or restore mitochondrial dynamics could, in principle, break the cycle of cellular deterioration that underlies diabetes and its complications.
4. Beta-Cell Vulnerability: The Pancreas Under Siege
Of all the cells in the body, pancreatic beta cells are uniquely exposed to mitochondrial stress. This is not coincidental — beta cells rely almost entirely on mitochondrial function to sense blood glucose levels and trigger appropriate insulin secretion. When mitochondria in beta cells falter, so does the entire insulin-release mechanism.
A 2025 paper by Darwish and colleagues in the journal Cells provides a detailed account of the specific mechanisms through which mitochondrial dysfunction undermines beta-cell health. The researchers describe how impaired electron transport chain activity, excessive ROS production, altered calcium signaling, and defective mitophagy all converge to damage beta cells in T2DM patients.
Particularly noteworthy is the role of mitochondria in regulating the precise moment of insulin secretion. When blood glucose rises, mitochondria in beta cells dramatically increase ATP production, which triggers a cascade of molecular events culminating in insulin release. In diabetic patients, this glucose-sensing mechanism is profoundly impaired. The cell sees glucose but cannot respond appropriately, leading to the elevated blood sugar levels that define diabetes.
Darwish et al. (2025) also survey the therapeutic landscape, highlighting several compounds — including GLP-1 receptor agonists and novel mitochondria-targeted antioxidants — that show promise in protecting beta-cell mitochondria and restoring normal function.
5. The Bigger Picture: Mitochondria and Diabetic Complications
Diabetes is not simply about blood sugar. For millions of patients, the real burden of the disease lies in its complications — kidney disease (diabetic nephropathy), nerve damage (neuropathy), eye disease (retinopathy), heart disease, and more. Emerging research suggests that mitochondrial dysfunction plays a central role in driving these complications as well.
A 2025 advance publication by Ge and colleagues in Molecular Aspects of Medicine takes a broad view of mitochondrial involvement in diabetes pathogenesis. The authors document how mitochondrial dysfunction contributes not only to insulin resistance and beta-cell failure, but also to the micro- and macrovascular damage that causes diabetic complications. Oxidative stress, mitochondria-triggered inflammation, and impaired cellular energy metabolism all contribute to vessel wall damage, reduced blood flow, and the multi-organ failure that makes diabetes one of the most serious chronic diseases of our time.
This systems-level view is important for patients and clinicians alike. It suggests that treating diabetes exclusively through blood sugar control, while essential, may not be sufficient to prevent all complications. Addressing the underlying mitochondrial dysfunction may be necessary for truly comprehensive management.
6. Practical Applications: What You Can Do Right Now
The science outlined above may sound abstract, but it carries very concrete implications for everyday health decisions. Here is what current evidence suggests you can do to support your mitochondrial health — and by extension, your metabolic health:
Regular Aerobic Exercise
Exercise is the most potent known stimulus for mitochondrial biogenesis. When you exercise aerobically — walking, cycling, swimming, dancing — your muscles demand more energy, signaling cells to create new mitochondria and improve the efficiency of existing ones. Studies consistently show that even moderate regular exercise (150 minutes per week of brisk walking) significantly improves mitochondrial function and reduces insulin resistance. This is not a minor effect — exercise directly targets the cellular mechanisms described in all five of the research papers cited here.
Dietary Quality and Timing
A diet rich in antioxidants — colourful vegetables, berries, nuts, olive oil — helps neutralize the reactive oxygen species that damage mitochondria. Conversely, a diet high in ultra-processed foods, refined carbohydrates, and added sugars amplifies oxidative stress and accelerates mitochondrial deterioration. Some research also supports the metabolic benefits of time-restricted eating (eating within a 10–12 hour window each day), which may enhance mitophagy — your body's mitochondrial recycling system.
Prioritizing Deep, Restorative Sleep
Sleep deprivation impairs mitochondrial function, increases oxidative stress, and reduces insulin sensitivity — even after just a few nights of poor sleep. Aim for 7–9 hours of quality sleep per night. If you snore or feel tired despite adequate sleep hours, speak with your doctor about screening for sleep apnea, which is strongly associated with metabolic dysfunction.
Stress Management
Chronic psychological stress elevates cortisol levels, which in turn drives oxidative stress and impairs mitochondrial function. Mind-body practices such as yoga, meditation, and deep-breathing exercises have demonstrated measurable benefits for metabolic health markers, likely in part through their effects on stress hormones and inflammatory pathways.
Emerging Pharmacological Approaches
Several drug classes already in clinical use appear to support mitochondrial health. Metformin, a cornerstone medication in T2DM management, modulates mitochondrial complex I activity. GLP-1 receptor agonists (such as semaglutide) show protective effects on beta-cell mitochondria. Researchers are also actively investigating mitochondria-targeted antioxidants (such as MitoQ and SkQ1), AMPK activators, and NAD+ precursors. While these remain largely investigational, the pipeline is genuinely promising. Discuss options with your healthcare provider.
Practical Checklist
Move your body daily (even a 30-minute walk counts). Eat a colorful, whole-food-rich diet. Sleep 7–9 hours per night. Manage stress with mind-body practices. Stay consistent with prescribed medications. Schedule regular metabolic screening if you have risk factors.
Frequently Asked Questions (FAQs)
FAQ 1: Can mitochondrial dysfunction cause type 2 diabetes on its own?
Mitochondrial dysfunction is a major contributing factor to T2DM, but diabetes is a multifactorial condition. Genetic predisposition, lifestyle factors (diet, physical inactivity), chronic inflammation, and hormonal imbalances all interact. However, the five studies reviewed here collectively support the conclusion that mitochondrial dysfunction occupies a central position in diabetes pathogenesis — it is not merely a downstream consequence but an active driver of disease. Addressing it is therefore a scientifically sound therapeutic strategy.
FAQ 2: How do I know if my mitochondria are not working properly?
There is currently no routine clinical test for mitochondrial dysfunction in the primary care setting. However, metabolic markers that suggest poor mitochondrial health include elevated fasting blood glucose, high triglycerides, low HDL cholesterol, insulin resistance (measured by HOMA-IR), and elevated markers of oxidative stress. Fatigue, muscle weakness, and poor exercise tolerance may also be non-specific indicators. If you are concerned, speak with your doctor about comprehensive metabolic testing.
FAQ 3: Are there specific supplements that support mitochondrial health in diabetes?
Several nutraceuticals have shown preliminary promise in supporting mitochondrial function, including CoQ10 (coenzyme Q10), alpha-lipoic acid, magnesium, and NAD+ precursors such as nicotinamide riboside (NR) and NMN. However, the evidence base in humans is still developing, and none of these should be used as a substitute for prescribed medication or lifestyle modification. Always consult your healthcare provider before beginning any supplement regimen, particularly if you are already managing diabetes with medication.
FAQ 4: Does insulin resistance cause mitochondrial dysfunction, or is it the other way around?
This is one of the most debated questions in diabetes research, and the honest answer is: both. The relationship is bidirectional and self-reinforcing. Mitochondrial dysfunction impairs insulin signaling, which worsens insulin resistance. Insulin resistance, in turn, alters fatty acid metabolism and increases oxidative stress, which further damages mitochondria. This feedback loop is precisely why diabetes is so difficult to reverse once established — and why early intervention, before the cycle becomes entrenched, is so important.
FAQ 5: Can lifestyle changes actually reverse mitochondrial dysfunction in diabetes?
Yes, to a meaningful extent. Exercise, in particular, is one of the most potent stimuli for mitochondrial biogenesis known to science. Clinical trials have demonstrated that sustained aerobic exercise programs improve mitochondrial density, efficiency, and function in people with type 2 diabetes. Dietary improvements and weight loss also reduce oxidative stress and improve mitochondrial dynamics. While complete reversal of established damage may not always be possible, significant functional improvements are consistently observed in motivated patients who adopt sustained lifestyle changes.
FAQ 6: How do diabetic complications relate to mitochondrial health?
The complications of diabetes — kidney disease, nerve damage, cardiovascular disease, and eye disease — are not simply the result of high blood sugar directly damaging tissues. Research shows that mitochondrial dysfunction, oxidative stress, and energy depletion in specific organ systems (kidneys, nerves, heart, retina) play major roles in driving these complications. This is why some people with well-controlled blood sugar still develop complications, and why researchers are increasingly focused on targeting mitochondrial pathways as a strategy for complication prevention.
FAQ 7: Are children or younger people affected by mitochondrial dysfunction related to diabetes?
While type 2 diabetes has traditionally been considered an adult disease, its incidence in children and young adults is rising in parallel with global obesity rates. Mitochondrial dysfunction has been documented even in adolescents with obesity and metabolic syndrome, long before a formal diabetes diagnosis. This underscores the importance of early metabolic health education, active lifestyles, and dietary quality in younger age groups. Early mitochondrial protection may be the most effective form of diabetes prevention we have.
Clinical pearls
1. The Bidirectional Energy Trap
Scientific Perspective: The relationship between mitochondrial dysfunction and insulin resistance is an escalating feedback loop, not a linear pathway. Impaired electron transport chain (ETC) activity generates excessive reactive oxygen species (ROS), which structurally damages insulin receptor substrates. Conversely, hyperinsulinemia and lipid oversupply overwhelm the mitochondria, forcing incomplete $\beta$-oxidation and further accelerating cellular energy failure.
Think of your cells like a kitchen with a broken trash disposal. When the disposal stops working, garbage (toxins) builds up, making it harder to cook. The mess makes it even harder to fix the disposal. Breaking this cycle requires lifestyle changes that reduce the workload on your cells while simultaneously giving them the tools to clean up.
2. beta Cell "Sensing" Failure vs. Starvation
Scientific Perspective: Pancreatic beta-cells rely entirely on a surge in the intracellular ATP/ADP ratio generated by mitochondrial oxidative phosphorylation to close K ATP channels, depolarize the membrane, and trigger insulin exocytosis. When mitochondria suffer bioenergetic failure, the glucose-sensing mechanism is severed; the cell registers systemic glucose but is physically incapable of synthesizing the ATP required to secrete insulin.
Your pancreas isn't necessarily "running out" of insulin early on; rather, its internal alarm system is broken. Even though there is plenty of sugar in your blood, the tiny power plants inside your pancreas can't generate the sparks needed to open the doors and release insulin.
3. Mitochondrial Quality Control (MQC) as a Novel Therapeutic Target
Scientific Perspective: T2DM pathology is heavily driven by the systemic failure of Mitochondrial Quality Control (MQC) pathways—specifically the downregulation of Pink1/Parkin-mediated mitophagy (the recycling of defective mitochondria) and PGC-1alpha-mediated biogenesis (the creation of new mitochondria). Therapeutic management must shift from simply lowering blood glucose to actively stimulating these clearance and renewal pathways.
Your body has its own internal recycling program designed to crush and replace old, damaged cell parts with brand-new ones. In diabetes, this recycling system stalls, leaving sluggish, broken power plants taking up space. Treatments are moving toward "restarting" this clean-up crew so your body can naturally manage energy better.
4. The Pathological "Leak" Driving Vascular Complications
Scientific Perspective: Diabetic microvascular and macrovascular complications (nephropathy, retinopathy, and neuropathy) are not caused by glucose toxicity alone. Chronic hyperglycemia forces an oversupply of electrons into the mitochondrial respiratory chain, causing a massive "leak" of superoxide radicals at Complex I and III. This localized oxidative stress activates inflammatory cascades (like NF-kappa) that destroy endothelial cell linings, regardless of tight systemic blood glucose control.
Managing diabetes isn't just about watching the numbers on your blood sugar monitor. High blood sugar causes your cells to "leak" microscopic sparks that irritate and damage your blood vessels from the inside out. This is why protecting your cellular health through diet and exercise is vital to shield your kidneys, eyes, and heart, even if your laboratory numbers look stable.
5. Exercise as a Biogenesis "Prescription"
Scientific Perspective: Mechanical muscle contraction and transient cellular energy depletion, AMP/ATP ratio elevation vigorously activate AMP-activated protein kinase (AMPK). This enzymatic shift triggers immediate mitochondrial biogenesis and restores the delicate balance of mitochondrial fission and fusion. This makes physical movement a direct molecular countermeasure to genetic or metabolic MQC defects.
Exercise isn't just about burning calories or losing weight; it is a direct biological order to your body to build a stronger engine. When you take a brisk 30-minute walk, your muscles panic slightly from the energy drain and immediately start building fresh, highly efficient power plants to handle the workload next time.
6. Metabolic Synchronization and Mitophagy
Scientific Perspective: Nutrient abundance continuously suppresses autophagy and mitophagy via the chronic activation of the mTOR (mechanistic target of rapamycin) pathway. Integrating strategic metabolic pauses—such as consistent sleep-wake cycles and time-restricted eating windows (e.g., 10–12 hours)—allows mTOR to downregulate, facilitating the cellular fasting state required for the selective clearance of dysfunctional, ROS-leaking mitochondria.
Constantly grazing on food keeps your cells in a permanent state of processing, meaning they never get a break to do internal maintenance. By giving your body a predictable, restful window of fasting overnight (like eating all your meals within a 10-hour window) and prioritizing deep sleep, you give your cells the quiet downtime they need to sweep away the cellular debris.
A Clinician’s Perspective: What This Looks Like in Real Life
In clinical practice, mitochondrial dysfunction rarely appears as an isolated laboratory finding. Instead, it often reveals itself through a recognizable metabolic pattern: increasing abdominal obesity, worsening fatigue, rising triglycerides, declining exercise tolerance, elevated fasting glucose, and progressive insulin resistance — sometimes years before overt diabetes is diagnosed.
Consider a typical example. A 46-year-old office worker presents with chronic fatigue, weight gain around the abdomen, poor sleep, and increasing post-meal blood sugar levels. Laboratory testing shows elevated triglycerides, low HDL cholesterol, mildly elevated liver enzymes, and early insulin resistance despite fasting glucose still being technically “normal.” From a traditional perspective, these findings may appear disconnected. But through the lens of mitochondrial medicine, they often represent the same underlying process: impaired cellular energy metabolism.
Inside skeletal muscle and liver cells, mitochondria may already be struggling to efficiently oxidize fatty acids and generate ATP. As energy production declines, intramyocellular lipids accumulate, oxidative stress rises, and insulin signaling becomes progressively impaired. Over time, pancreatic beta cells are forced to compensate by producing larger amounts of insulin, accelerating beta-cell exhaustion and eventual hyperglycemia.
Clinicians increasingly recognize that by the time type 2 diabetes is formally diagnosed, mitochondrial dysfunction and metabolic inflammation may have been evolving silently for years. This is why early intervention matters so profoundly. Improvements in physical activity, sleep quality, dietary composition, visceral fat reduction, and cardiorespiratory fitness can meaningfully improve mitochondrial efficiency long before irreversible beta-cell damage occurs.
From a practical standpoint, treating metabolic disease today is no longer simply about lowering blood sugar. It is increasingly about restoring metabolic flexibility, reducing cellular stress, and protecting the mitochondrial systems that sustain long-term metabolic health.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
Manage Diabetes Naturally: How Beta-Glucans Control Blood Sugar | DR T S DIDWAL
References
Chen, Y., Liu, X., Liu, Y., et al. (2025). Mitochondrial quality control in diabetes mellitus and complications: Molecular mechanisms and therapeutic strategies. Cell Death & Disease, 16, 652. https://doi.org/10.1038/s41419-025-07936-y
Darwish, R., Alcibahy, Y., Abu-Sharia, G., & Butler, A. E. (2025). β-Cell mitochondrial dysfunction: Underlying mechanisms and potential therapeutic strategies. Cells, 14(23), 1861. https://doi.org/10.3390/cells14231861
Feng, Z., Tan, Z., & Lu, D. (2025). Mitochondrial bioenergetics dysfunction in T2DM: Linking oxidative stress to insulin resistance. Frontiers in Endocrinology, 16, 1674477. https://doi.org/10.3389/fendo.2025.1674477
Ge, X., et al. (2025). Advancements in understanding the role and mechanisms of mitochondria in the pathogenesis of diabetes mellitus. Molecular Aspects of Medicine. Advance online publication. https://doi.org/10.1016/j.mam.2025.101203
Yadav, S., Kumar, G., Kumar, S., et al. (2026). Mitochondrial dysfunction–driven inflammation and β-cell apoptosis in type 2 diabetes mellitus: Mechanistic insights and therapeutic implications. Molecular Biology Reports, 53, 662. https://doi.org/10.1007/s11033-026-11851-6