How to Reverse Hepatic Insulin Resistance Naturally (Science-Backed Diet, Exercise & Supplements)
Learn how hepatic insulin resistance drives fatty liver disease, high blood sugar, obesity, and type 2 diabetes — plus evidence-based ways to reverse it naturally.
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/23/202623 min read
Every morning, millions of people wake up believing their metabolism is functioning normally — yet deep inside the liver, a silent metabolic malfunction may already be unfolding. Long before type 2 diabetes is diagnosed, before HbA1c rises dramatically, and even before obvious symptoms appear, the liver can begin losing its ability to respond properly to insulin. This condition, known as hepatic insulin resistance, is now recognized as one of the central drivers of modern metabolic disease, sitting at the crossroads of obesity, fatty liver disease, cardiovascular disease, and type 2 diabetes (Bo et al., 2024).
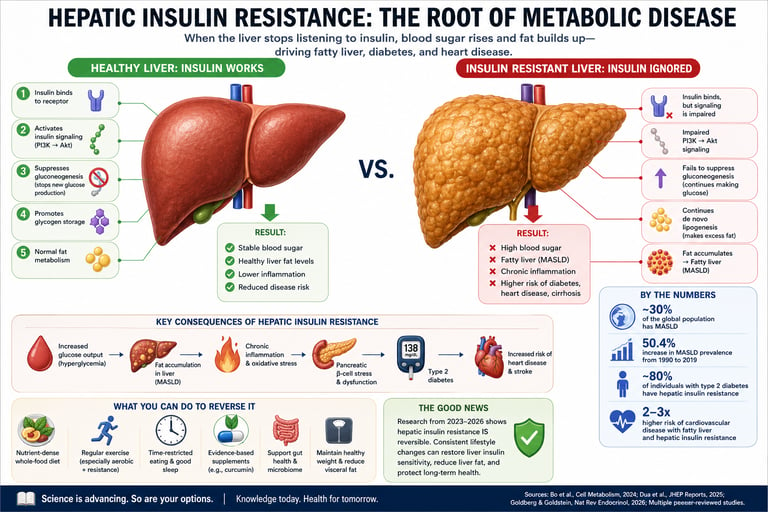
In a healthy body, insulin acts as a precise metabolic signal, telling the liver when to stop producing glucose and when to store energy for later use. But in hepatic insulin resistance, that signal becomes distorted. The liver continues releasing glucose into the bloodstream even when blood sugar is already elevated, while simultaneously converting excess calories into fat through de novo lipogenesis — a dangerous metabolic paradox now termed “selective hepatic insulin resistance” (Bo et al., 2024). The result is a biochemical environment that promotes hyperglycemia, fatty liver accumulation, chronic inflammation, and progressive metabolic dysfunction.
The scale of the problem is staggering. Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD), closely linked to hepatic insulin resistance, now affects an estimated 30% of the global population, with prevalence rising dramatically over recent decades (Dua et al., 2025). Alarmingly, many individuals remain unaware they have liver-related insulin resistance until years of silent damage have already occurred.
Understanding hepatic insulin resistance is no longer optional — it is essential for understanding modern metabolic health itself.
Clinical Pearls on Hepatic Insulin Resistance
1. Selective Hepatic Insulin Resistance is Common
In hepatic insulin resistance, hepatocytes often lose insulin-mediated suppression of gluconeogenesis while retaining (or enhancing) insulin-stimulated de novo lipogenesis via the SREBP-1c pathway. This selective defect simultaneously drives fasting hyperglycemia and hepatic fat accumulation.
2. Strong Bidirectional Link with MASLD and Type 2 Diabetes
Approximately 80% of individuals with type 2 diabetes exhibit significant hepatic insulin resistance. MASLD affects ~30% of the global adult population and frequently represents the earliest manifestation of systemic metabolic dysfunction.
3. Early Detection Relies on Sensitive Biomarkers
Elevated fasting insulin, HOMA-IR >2.5, hypertriglyceridemia, and mildly increased ALT/AST are key indicators that often precede overt hyperglycemia. Early identification through these markers enables timely intervention before progression to advanced fibrosis.
4. Lifestyle Interventions Remain First-Line and Highly Effective
Evidence supports that Mediterranean-pattern diets, combined aerobic and resistance exercise, and time-restricted eating (10–12 hour window) significantly reduce intrahepatic lipid content and improve insulin signaling, frequently independent of substantial weight loss.
5. Mitochondrial Dysfunction and Impaired Mitophagy Play a Central Role
Defective PINK1/Parkin-mediated mitophagy contributes to oxidative stress and disrupted PI3K/Akt insulin signaling in hepatocytes. Targeted support of mitochondrial quality control is an emerging therapeutic focus.
6. Hepatic Insulin Resistance is Largely Reversible
With sustained lifestyle modification — including modest 5–7% body weight reduction, regular physical activity, and optimized sleep — hepatic insulin sensitivity and liver fat content can improve substantially within weeks to months in most patients
1. What Is Hepatic Insulin Resistance?
Hepatic insulin resistance (also called liver insulin resistance) occurs when liver cells (hepatocytes) fail to respond normally to the hormone insulin. In a healthy person, insulin acts like a precise signal that tells the liver: "Glucose is plentiful — stop making more of it, and switch to storing energy instead." In hepatic insulin resistance, the liver ignores this signal, continuing to produce glucose even when blood sugar and insulin levels are already high.
What makes this particularly insidious is a phenomenon researchers call "selective hepatic insulin resistance". A landmark 2024 review published in Cell Metabolism by Bo et al. describes it clearly: in insulin resistance, the liver loses its ability to suppress gluconeogenesis (new glucose production) — yet it paradoxically retains — and even amplifies — insulin's ability to drive de novo lipogenesis (DNL), meaning it keeps making fat. The result is a liver that simultaneously floods the bloodstream with excess glucose and accumulates dangerous fat — a double metabolic insult.
2. How a Healthy Liver Responds to Insulin
To understand what goes wrong in hepatic insulin resistance, you first need to appreciate the elegance of a liver that's working properly.
The Fed State: Insulin in Action
After you eat a carbohydrate-containing meal, blood glucose rises. Your pancreas releases insulin. In the liver, insulin binds to its receptor and activates a signaling cascade: IRS → PI3K → Akt. This has several key downstream effects:
Suppresses gluconeogenesis — the liver stops making new glucose from amino acids and glycerol
Promotes glycogenesis — excess glucose is packaged into glycogen (storage form) in the liver
Activates lipogenesis — small amounts of surplus glucose are converted to fatty acids (normal and appropriate in modest amounts)
Inhibits ketogenesis — ketone body production is switched off when fuel is abundant
The Fasted State: When Insulin Falls
When you fast — even overnight — insulin levels drop, and a coordinated hormonal response kicks in. A comprehensive 2026 review in Nature Reviews Endocrinology by Goldberg and Goldstein details this beautifully: the liver's primary job during fasting is to produce fuel (glucose and ketone bodies) for the brain and other tissues. This is driven by rising levels of glucagon, glucocorticoids, growth hormone, adrenaline, free fatty acids, asprosin, and GP73 — all of which cooperate synergistically to stimulate hepatic glucose and ketone output.
This elegant on/off switch — insulin promoting storage, fasting hormones promoting fuel release — is what hepatic insulin resistance disrupts.
3. The Science: How Hepatic Insulin Resistance Develops
Hepatic insulin resistance doesn't happen overnight. It's the end result of multiple converging biological insults, and researchers have identified several overlapping mechanisms.
Mechanism 1: Mitochondrial Dysfunction and Impaired Mitophagy
The liver is extraordinarily metabolically active, meaning it has an enormous need for healthy mitochondria — the energy-producing organelles inside cells. When mitochondria become damaged and dysfunctional, they produce excess reactive oxygen species (ROS), trigger inflammation, and impair the insulin signaling cascade.
Critically, cells normally clear damaged mitochondria through a process called mitophagy — a selective form of autophagy. A key 2026 study published in Scientific Reports by Guo, Zhang and Kong revealed a compelling new mechanism: hepatic insulin resistance is closely linked to inadequate PINK1/Parkin-mediated mitophagy. When this mitochondrial quality-control pathway breaks down, damaged mitochondria accumulate, disrupting the PI3K/Akt/GLUT4 insulin signaling axis and triggering hepatic fat accumulation.
Lipid Overload / Palmitic Acid → Mitochondrial Damage → ↓ PINK1/Parkin Mitophagy →↓ PI3K/Akt Signaling → Hepatic IR
Mechanism 2: Hepatic Inflammation and the Vicious Cycle
Chronic low-grade inflammation in the liver is both a cause and a consequence of hepatic insulin resistance — creating a self-amplifying loop. A major 2023 review in Frontiers in Endocrinology by Niranjan, Phillips, and Giannoukakis describes this cycle in detail.
Inflammatory cytokines — particularly TNF-α, IL-6, and IL-1β — activate stress kinases such as JNK (c-Jun N-terminal kinase) and IKKβ. These kinases phosphorylate insulin receptor substrate (IRS) proteins at serine residues rather than the normal tyrosine sites, effectively blocking the downstream insulin signal. The liver then fails to suppress gluconeogenesis, driving hyperglycemia, which further promotes inflammation — and the cycle continues.
The same review highlights a critical concept: uncoupling hepatic IR from hepatic inflammation may be the key to breaking this cycle and both restoring insulin sensitivity and halting the progression of fatty liver disease.
Mechanism 3: Ectopic Lipid Accumulation and Lipotoxicity
Excess free fatty acids (FFAs) from an overloaded adipose tissue — particularly in obesity — flood into the liver and trigger several harmful processes:
Diacylglycerol (DAG) accumulation, which activates protein kinase C epsilon (PKCε), a potent inhibitor of insulin receptor signaling
Ceramide synthesis, which activates protein phosphatase 2A (PP2A) and suppresses Akt activity
Endoplasmic reticulum (ER) stress, triggering the unfolded protein response and further impairing insulin signaling
Mechanism 4: The Pathway-Specific Paradox (Selective IR)
Perhaps the most puzzling — and clinically important — aspect of hepatic insulin resistance is the "selective" nature described by Bo et al. (2024) in Cell Metabolism. In MASLD with insulin resistance, a paradox emerges:
The FoxO1 pathway (which suppresses gluconeogenesis) becomes insulin-resistant → blood sugar rises
The SREBP-1c pathway (which drives fat synthesis) remains insulin-sensitive → liver fat increases
This means conventional thinking — "just block insulin action to reduce liver fat" — is dangerously oversimplified. The goal must be to restore normal, balanced insulin signaling rather than broadly suppress it.
4. Fasting Hormones and Their Role in Liver Metabolism
A sophisticated understanding of hepatic insulin resistance requires knowing the full cast of hormonal players — not just insulin. The 2026 Nature Reviews Endocrinology review by Goldberg and Goldstein offers a paradigm-shifting perspective: fasting hormones are not simply "anti-insulin" signals. They cooperate synergistically with each other to fine-tune hepatic fuel production.
Key Fasting Hormones That Drive Hepatic Insulin Resistance
Glucagon
Activates the cAMP/PKA pathway
Stimulates glycogenolysis, gluconeogenesis, and ketogenesis
Chronically elevated glucagon increases hepatic glucose output and worsens fasting hyperglycemia
Cortisol (Glucocorticoids)
Upregulates gluconeogenic enzymes such as PEPCK and G6Pase
Works synergistically with glucagon to increase liver glucose production
Chronic stress and elevated cortisol promote visceral fat accumulation and hepatic insulin resistance
Growth Hormone (GH)
Enhances lipolysis and free fatty acid (FFA) release
Regulates hepatic IGF-1 production
Growth hormone dysregulation and GH resistance are linked to MASLD progression
Adrenaline (Epinephrine)
Rapidly stimulates glycogen breakdown and hepatic fuel mobilization
Chronic stress-induced adrenaline surges contribute to glucose instability and metabolic dysfunction
Free Fatty Acids (FFAs)
Serve as substrates for ketogenesis
Act as regulators of gluconeogenesis
Excess FFAs from visceral fat directly impair hepatic insulin signaling through lipotoxicity
Asprosin
Newly identified fasting hormone that stimulates hepatic glucose release via cAMP signaling
Elevated in obesity and insulin resistance
Emerging therapeutic target in metabolic disease research
Clinical Insight
In hepatic insulin resistance, these fasting hormones often remain abnormally elevated even after meals, keeping the liver locked in a continuous “fuel-production mode.” This contributes to persistent hyperglycemia, fatty liver accumulation, and worsening metabolic dysfunction.
The critical clinical insight: in hepatic insulin resistance, the counter-regulatory hormones (especially glucagon) remain elevated even in the fed state, compounding the liver's failure to suppress glucose output. It is not just an "insulin problem" — it is a global hormonal dysregulation centered on the liver.
5. The Hepatic IR–MASLD–Type 2 Diabetes Triad
[Internal link opportunity: "What Is MASLD?"] If hepatic insulin resistance has a villainous partner, it is MASLD — formerly known as NAFLD (non-alcoholic fatty liver disease). These two conditions are so tightly intertwined that researchers often describe them as a single entity expressed across a spectrum.
How Hepatic IR Causes MASLD
The selective insulin resistance described above directly drives MASLD. The liver keeps producing fat (via the intact SREBP-1c lipogenic pathway) while simultaneously overproducing glucose. Fat accumulates in hepatocytes, triggering oxidative stress and inflammation that further damages the liver. A 2025 review in Frontiers in Medicine by Dua et al. reports that global MASLD prevalence has reached approximately 30% of the world's population, with a staggering 50.4% relative increase between 1990 and 2019 — a timeline that maps almost perfectly onto rising global rates of obesity, processed food consumption, and sedentary behavior.
MASLD Progression: Steatosis → MASH → Fibrosis → Cirrhosis
Left unchecked, hepatic IR drives MASLD along a dangerous trajectory:
Simple steatosis — fat accumulates in >5% of hepatocytes (often asymptomatic)
MASH (Metabolic Dysfunction-Associated Steatohepatitis) — inflammation and hepatocyte damage added to steatosis
Fibrosis — scar tissue begins replacing functional liver cells
Cirrhosis — advanced scarring, lost liver function
Hepatocellular carcinoma (HCC) — liver cancer risk increases substantially
Medical Warning
MASLD and hepatic insulin resistance often progress silently for years. If you have obesity, type 2 diabetes, prediabetes, or metabolic syndrome, ask your healthcare provider about liver function tests, fasting glucose/insulin, and a liver ultrasound. Early intervention dramatically improves outcomes. This article does not replace medical advice.
The Bidirectional Relationship with Type 2 Diabetes
Hepatic insulin resistance and type 2 diabetes reinforce each other in a bidirectional loop. Hepatic IR causes fasting hyperglycemia (the earliest blood sugar abnormality in type 2 diabetes), which drives the pancreas to produce more insulin (compensatory hyperinsulinemia). Over time, the pancreatic beta cells become exhausted, and overt type 2 diabetes emerges. Meanwhile, the hyperglycemia and hyperinsulinemia further worsen hepatic IR and MASLD — a loop that, if not broken, leads to progressive metabolic deterioration.
6. The Gut Microbiome's Hidden Role in Hepatic Insulin Resistance
The gut-liver axis is one of the most exciting frontiers in metabolic medicine. The 2025 Frontiers in Medicine review by Dua et al. dedicates significant attention to how gut microbiome dysbiosis — an imbalance in gut bacterial communities — directly fuels hepatic insulin resistance and MASLD progression.
Three Key Gut-Liver Mechanisms
1. Increased Intestinal Permeability ("Leaky Gut")
Dysbiosis weakens the tight junctions between intestinal cells, allowing bacterial components — particularly lipopolysaccharide (LPS) from Gram-negative bacteria — to enter the portal circulation and reach the liver. LPS activates Toll-like receptor 4 (TLR4) on Kupffer cells (liver immune cells), triggering the same inflammatory cascade that impairs insulin signaling.
2. Altered Short-Chain Fatty Acid (SCFA) Production
Beneficial gut bacteria ferment dietary fiber into SCFAs — especially butyrate, propionate, and acetate — which have direct anti-inflammatory and insulin-sensitizing effects in the liver. Dysbiosis reduces SCFA-producing bacteria (like Faecalibacterium prausnitzii and Roseburia intestinalis), depriving the liver of these protective signals.
3. Bile Acid Dysregulation
The gut microbiome modifies primary bile acids into secondary bile acids, which serve as signaling molecules that activate farnesoid X receptor (FXR) and TGR5 — receptors that regulate hepatic glucose and lipid metabolism. Dysbiosis disrupts this bile acid signaling, further impairing hepatic metabolic control.
Gut Microbiome Changes Linked to MASLD Progression
↓ Akkermansia muciniphila
Associated with early fatty liver (steatosis)
Linked to increased gut permeability (“leaky gut”)
↑ Bacteroides vulgatus
Associated with advanced liver fibrosis
↓ Faecalibacterium prausnitzii
Linked to progression toward MASH and liver inflammation
↑ Gram-negative Proteobacteria (E. coli)
Promote fibrosis through LPS/TLR4 inflammatory pathways
↓ Eubacterium rectale & ↓ Bifidobacterium
Associated with worse insulin resistance and poor glycemic control
7. Causes and Risk Factors for Hepatic Insulin Resistance
Understanding your personal risk is the first step to targeted prevention and reversal.
Primary Causes
Obesity and visceral adiposity — excess fat around organs drives free fatty acid overflow into the liver
High-calorie, high-fructose diet — fructose is metabolized almost exclusively in the liver, promoting DNL and lipid accumulation
Physical inactivity — exercise is one of the most potent drivers of hepatic insulin sensitivity
Chronic sleep deprivation — disrupts circadian regulation of hepatic metabolism and cortisol rhythms
Chronic psychological stress — elevates cortisol and adrenaline, potent stimulators of hepatic glucose production
Gut microbiome dysbiosis — as discussed above, a direct driver via LPS and altered metabolites
Genetic predisposition — variants in PNPLA3, TM6SF2, and MBOAT7 genes increase hepatic fat accumulation susceptibility
Amplifying Risk Factors
Type 2 diabetes (both cause and consequence)
Polycystic ovary syndrome (PCOS)
Hypothyroidism
Certain medications (glucocorticoids, some antipsychotics, highly active antiretroviral therapy)
Excessive alcohol consumption
Rapid weight loss / yo-yo dieting (triggers mobilization of excess fatty acids)
8. Warning Signs and How Hepatic Insulin Resistance Is Diagnosed
Common Warning Signs
Hepatic insulin resistance is often called a "silent" condition because it produces few noticeable symptoms in its early stages. However, certain patterns should prompt investigation:
Persistently elevated fasting blood glucose (100–125 mg/dL suggests prediabetes)
High fasting triglycerides (>150 mg/dL)
Low HDL cholesterol (<40 mg/dL in men, <50 mg/dL in women)
Elevated ALT and AST (liver enzymes) — often the first lab abnormality
High HOMA-IR score (a calculated measure of insulin resistance)
Abdominal obesity (waist circumference >40 inches in men, >35 inches in women)
Fatigue, brain fog, difficulty losing weight despite calorie restriction
Darkened skin patches in neck creases or armpits (acanthosis nigricans) — a sign of chronic hyperinsulinemia
Diagnostic Tests Your Doctor May Order
Fasting glucose and insulin → Calculate HOMA-IR (Fasting Insulin × Fasting Glucose / 405; above 2.5–3.0 suggests IR)
HbA1c — reflects average blood sugar over 2–3 months
Comprehensive liver panel (ALT, AST, GGT, ALP, albumin, bilirubin)
Lipid panel with triglycerides
Liver ultrasound — can detect steatosis (fatty liver)
Fibroscan (transient elastography) — non-invasive assessment of liver stiffness and fat content
FIB-4 score — a calculated index using age, ALT, AST, and platelets to estimate fibrosis risk
Clinical Tip
A HOMA-IR above 2.5, combined with elevated triglycerides and fasting glucose between 100–125 mg/dL, is a strong signal of hepatic insulin resistance even before frank type 2 diabetes develops. Don't wait for a diabetes diagnosis — earlier intervention is dramatically more effective.
9.Diet Strategies to Reverse Hepatic Insulin Resistance
The Mediterranean Diet: Gold Standard Evidence
The Mediterranean diet — centered on vegetables, legumes, whole grains, fish, olive oil, nuts, and moderate red wine — consistently emerges as the most well-studied dietary pattern for improving hepatic insulin sensitivity. Research shows it reduces liver fat, improves insulin signaling markers, favorably shifts gut microbiota composition (increasing Firmicutes, reducing Bacteroidetes), and lowers systemic inflammation. The 2025 Dua et al. review in Frontiers in Medicine specifically notes that Mediterranean-pattern eating is the only human dietary intervention shown to produce favorable, consistent changes in gut microbial signatures associated with MASLD improvement.
Carbohydrate Quality and Quantity: A Critical Variable
Not all carbohydrates affect the liver equally. The evidence strongly indicts fructose — particularly in the form of high-fructose corn syrup in ultra-processed foods and sugar-sweetened beverages — as a primary driver of hepatic lipid accumulation and insulin resistance. Unlike glucose (which is distributed throughout the body), fructose is almost entirely extracted and metabolized by the liver, where it overwhelms normal metabolic pathways and is rapidly converted to fat.
Practical targets:
Eliminate sugar-sweetened beverages (including fruit juices) — the single highest-yield dietary change for hepatic IR
Reduce ultra-processed food intake — high in refined carbohydrates, fructose, and industrial seed oils
Prioritize low-glycemic, fiber-rich carbohydrates — legumes, oats, vegetables, and whole fruit (fiber slows fructose absorption)
Consider time-restricted eating (10–12 hour eating window) — emerging evidence shows benefits for liver fat and insulin sensitivity
Dietary Fats: Type Matters More Than Total Amount
Extra-virgin olive oil — rich in oleocanthal (anti-inflammatory) and monounsaturated fatty acids; directly improves hepatic insulin signaling
Omega-3 fatty acids (EPA/DHA) — from fatty fish; reduce hepatic triglycerides and liver inflammation
Saturated fatty acids (especially palmitic acid) — directly trigger lipotoxic damage in hepatocytes and impair PINK1/Parkin mitophagy (as shown in the Guo et al. 2026 study)
Trans fats — avoid entirely; dramatically worsen hepatic IR and liver inflammation
Protein: The Underappreciated Macronutrient
Adequate protein intake (1.2–1.6 g/kg body weight) supports lean muscle mass, which acts as a metabolic sink for glucose, reducing the burden on the liver. Plant proteins (legumes, soy) appear to have additional benefits over animal proteins for liver fat content, potentially via effects on bile acid metabolism and gut microbiota.
7-Day Hepatic IR Dietary Protocol
Daily Essentials
5+ servings vegetables (emphasize leafy greens, cruciferous)
2–3 tbsp extra-virgin olive oil
Fatty fish 2–3×/week (salmon, mackerel, sardines)
Legumes daily (lentils, chickpeas, beans)
1 handful walnuts or almonds
Strictly Limit
Sugar-sweetened beverages (zero)
Ultra-processed foods
Refined grains (white bread, white rice)
Added sugars <25g/day
Fried foods / trans fats
Meal Timing
Eat within a 10–12 hour window
Largest meal at midday
Avoid eating 2–3 hours before bed
Protein at every meal to stabilize glucose
10. Exercise Protocols That Target the Liver
How Exercise Improves Hepatic Insulin Sensitivity
Reduces hepatic fat content — even without weight loss, aerobic exercise consistently reduces liver fat within 4–12 weeks
Activates AMPK in hepatocytes — a master metabolic regulator that suppresses lipid synthesis and improves insulin signaling
Increases skeletal muscle glucose uptake — reduces the glucose load reaching the liver post-meal
Promotes hepatic mitophagy — exercise is a powerful stimulus for PINK1/Parkin-mediated mitochondrial quality control
Reduces visceral adiposity — decreasing the FFA flux into the liver
Best Exercises to Reverse Hepatic Insulin Resistance
Moderate Aerobic Exercise
Brisk walking, cycling, swimming
Recommended: 150 minutes/week
Helps reduce liver fat, improve HOMA-IR, and lower triglycerides
Strong scientific evidence
High-Intensity Interval Training (HIIT)
Short bursts of intense exercise with recovery periods
Recommended: 20–30 minutes, 3× weekly
Activates AMPK and rapidly improves liver fat metabolism
Strong evidence for improving hepatic insulin sensitivity
Resistance Training
Weight training or bodyweight exercises
Recommended: 2–3 sessions/week
Builds glucose-absorbing muscle and reduces visceral fat
Complements aerobic exercise for metabolic health
Strong evidence
Post-Meal Walking
10–15 minutes after meals
Reduces post-meal glucose spikes and hepatic glucose load
Simple and effective strategy for blood sugar control
Moderate evidence
Clinical Insight
Combining aerobic exercise with resistance training appears most effective for reducing liver fat and improving hepatic insulin resistance — even without major weight loss.
Key insight: A combination of aerobic exercise and resistance training appears synergistically superior to either alone for hepatic fat reduction and insulin sensitivity improvement. Even a single moderate-intensity exercise session can acutely reduce hepatic glucose output by 15–20%.
11. Evidence-Based Supplements: The Curcumin Breakthrough and Beyond
Curcumin: The 2026 Mitophagy Breakthrough
Curcumin — the primary bioactive polyphenol in turmeric (Curcuma longa) — has long been known as an anti-inflammatory compound. But a landmark 2026 study in Scientific Reports by Guo, Zhang and Kong has now revealed a compelling new mechanism of action specifically in the liver.
The researchers induced hepatic insulin resistance in human HepG2 liver cells using palmitic acid (a saturated fatty acid mimicking a high-fat diet), then treated with curcumin. The results were striking: curcumin activated the PINK1/Parkin mitophagy pathway, clearing damaged mitochondria, restoring mitochondrial membrane potential and ATP production, and dramatically improving insulin signaling through the PI3K/Akt pathway — increasing GLUT4 expression and glucose uptake. When PINK1 was blocked (using siRNA), or mitophagy was pharmacologically inhibited, curcumin's benefits were significantly blunted — confirming that mitophagy activation is the central mechanism.
Key Finding (Guo et al., 2026)
Curcumin ameliorates hepatic insulin resistance in liver cells by activating PINK1/Parkin-dependent mitophagy — rescuing mitochondrial function and restoring the PI3K/Akt/GLUT4 insulin signaling axis. This represents a novel and clinically relevant mechanism of action.
Beyond mitophagy, earlier research published in the Journal of Lipid Research showed that curcumin also prevents hepatic insulin resistance by inhibiting adipose tissue lipolysis (via suppression of ER stress), reducing the free fatty acid overflow that reaches the liver and triggers lipotoxic insulin resistance. Together, these studies position curcumin as a uniquely multi-targeted hepatoprotective compound.
Curcumin — Practical Considerations
Bioavailability challenge: Standard curcumin powder is poorly absorbed. Look for formulations with piperine (black pepper extract, 10–20 mg), phospholipid complexes (phytosome), or nanoparticle technologies
Studied dosages: Most clinical trials use 500–1,500 mg/day of curcumin; for HOMA-IR improvements, 12–16 weeks minimum is typical
Food sources: Turmeric spice contains 2–5% curcuminoids — culinary use alone is unlikely to achieve therapeutic levels
Safety: Generally well-tolerated; at high doses, may cause GI discomfort; consult your doctor if on anticoagulant medications
Other Evidence-Supported Supplements for Hepatic IR
Omega-3 (EPA/DHA)
Reduces liver triglycerides and inflammation
Improves adiponectin and metabolic health
Dose: 2–4 g/day
Strong evidence
Berberine
Activates AMPK and lowers hepatic glucose production
Supports gut microbiome health
Dose: 500 mg, 2–3× daily
Strong evidence
Vitamin E
Powerful antioxidant that reduces liver inflammation
FDA-recognized for MASH treatment
Dose: 800 IU/day
Strong evidence
Probiotics / Synbiotics
Improve gut microbiome balance
Reduce endotoxins and improve HOMA-IR
Dose: 10–50 billion CFU/day
Moderate evidence
Magnesium
Supports insulin receptor signaling
Magnesium deficiency worsens insulin resistance
Dose: 200–400 mg/day
Moderate evidence
Silymarin (Milk Thistle)
Hepatoprotective and anti-inflammatory
Helps lower ALT levels in MASLD
Dose: 140–420 mg/day
Moderate evidence
Resveratrol
Activates SIRT1/AMPK pathways
Supports mitochondrial function and reduces liver fat
Dose: 150–500 mg/day
Emerging evidence
⚠️ Important Disclaimer
Supplements are not substitutes for medical treatment. If you have diagnosed type 2 diabetes, MASLD, or advanced hepatic fibrosis, work with your healthcare provider before adding supplements to your regimen. Interactions with medications (particularly blood thinners, metformin, and statins) are possible.
12. Evidence Summary: Key Studies at a Glance
Bo et al. (2024) – Cell Metabolism
Described the “selective hepatic insulin resistance” paradox
Liver fails to suppress glucose production while fat synthesis remains active
Explains simultaneous hyperglycemia and fatty liver development
Goldberg & Goldstein (2026) – Nature Reviews Endocrinology
Showed fasting hormones work cooperatively to regulate hepatic fuel production
Identified glucagon, cortisol, growth hormone, FFAs, and asprosin as key metabolic regulators
Opened new therapeutic targets for hepatic insulin resistance
Guo, Zhang & Kong (2026) – Scientific Reports
Found curcumin improves hepatic insulin resistance via PINK1/Parkin-mediated mitophagy
Restored PI3K/Akt/GLUT4 insulin signaling in liver cells
Supports curcumin as a potential hepatoprotective metabolic therapy
Niranjan, Phillips & Giannoukakis (2023) – Frontiers in Endocrinology
Demonstrated that hepatic inflammation and insulin resistance reinforce each other
Suggested combined anti-inflammatory and insulin-sensitizing therapies may be most effective
Dua et al. (2025) – Frontiers in Medicine
Reported MASLD affects nearly 30% of the global population
Highlighted gut dysbiosis, LPS, bile acids, and SCFAs as major drivers of hepatic insulin resistance
Established the gut microbiome as a key therapeutic target in MASLD and metabolic disease
13. Common Myths & Mistakes About Hepatic Insulin Resistance
❌ Myth 1: "Fatty liver is only a problem for people who drink heavily."
✅ Fact: MASLD — the fatty liver driven by hepatic insulin resistance — occurs in people who drink little or no alcohol. It is now the most common liver disease globally, driven primarily by diet, obesity, and metabolic dysfunction.
❌ Myth 2: If my blood sugar is normal, my liver is fine."
✅ Fact: Hepatic insulin resistance can be present and cause liver fat accumulation for years before blood sugar rises above normal. Liver enzymes, fasting insulin, and HOMA-IR are earlier and more sensitive markers.
❌ Myth 3 :"Just eating less fat will fix a fatty liver."
✅ Fact: Dietary fat type matters more than total fat. The bigger culprit is excess refined carbohydrates and fructose, which directly drive hepatic de novo lipogenesis. A low-fat, high-refined-carb diet can actually worsen hepatic IR.
❌ Myth 4 : "You need to lose a lot of weight to improve hepatic IR."
✅ Fact: Even a 5–7% reduction in body weight produces significant improvements in liver fat and insulin sensitivity. More impressively, regular aerobic exercise reduces liver fat even without any weight loss at all.
❌ Myth 5: "Turmeric in cooking provides enough curcumin to help."
✅ Fact : While culinary turmeric is beneficial as part of an overall diet, the therapeutic doses used in clinical studies (500–1,500 mg curcumin) are far above what cooking provides. Bioavailability-enhanced supplements are needed to achieve mechanistically relevant concentrations.
❌ Myth :"Hepatic insulin resistance is irreversible."
✅ Fact :Hepatic insulin resistance — even in the presence of significant liver fat — is highly reversible with consistent lifestyle intervention. Unlike fibrosis (advanced scarring), simple steatosis and IR-driven liver dysfunction respond remarkably well to diet, exercise, and targeted supplements within months.
14. Frequently Asked Questions
What is the fastest way to reduce hepatic insulin resistance?
The most impactful single change you can make immediately is eliminating sugar-sweetened beverages and ultra-processed foods — this directly reduces the fructose and refined carbohydrate load that drives hepatic fat production. Combined with daily moderate exercise (even 30 minutes of brisk walking), significant improvements in liver fat content and HOMA-IR can be seen within 4–8 weeks. Calorie restriction producing 5–7% weight loss accelerates results further.
Can you have hepatic insulin resistance without being overweight?
Yes — this is known as "lean MASLD" or lean metabolic syndrome, and it is more common than many assume, particularly in Asian populations where it can occur at lower BMI thresholds. Visceral fat (fat around the abdominal organs, not subcutaneous fat) and ectopic liver fat are more relevant than overall body weight. Sedentary behavior, poor diet quality, and genetic factors can drive hepatic IR even in lean individuals.
How is hepatic insulin resistance different from general insulin resistance?
General insulin resistance refers to impaired insulin action across multiple tissues — primarily skeletal muscle, adipose tissue, and liver. Hepatic insulin resistance specifically refers to the liver's failure to suppress glucose production and has unique features: most notably, the "selective" pattern where gluconeogenesis suppression is lost but fat production often increases. This selective defect is central to understanding both fasting hyperglycemia and fatty liver in type 2 diabetes.
Is intermittent fasting beneficial for hepatic insulin resistance?
Emerging evidence supports time-restricted eating (TRE) — eating within a 10–12 hour daily window — as beneficial for hepatic IR and liver fat. During the fasting period, the liver activates autophagy and mitophagy (consistent with the PINK1/Parkin pathway highlighted in 2026 research), clears damaged cellular components, and improves metabolic efficiency. Longer fasting windows (16+ hours) show stronger effects in animal models but may not be sustainable or appropriate for everyone; consult your doctor, especially if you're on glucose-lowering medications.
What blood tests should I ask for to check my liver's insulin sensitivity?
Request fasting glucose, fasting insulin (to calculate HOMA-IR), a full liver function panel (ALT, AST, GGT), triglycerides, HDL cholesterol, and HbA1c. A HOMA-IR above 2.5, elevated ALT, high fasting triglycerides, and low HDL together create a strong clinical picture of hepatic insulin resistance. A liver ultrasound can confirm steatosis. The FIB-4 index (using age, ALT, AST, and platelets) is a useful free online calculator for estimating fibrosis risk.
Does alcohol worsen hepatic insulin resistance?
Yes — alcohol is directly metabolized in the liver, generates oxidative stress, promotes fat accumulation, and impairs mitochondrial function (all mechanisms that worsen hepatic IR). Even moderate alcohol consumption has been shown to worsen liver fat and insulin sensitivity in people with pre-existing metabolic risk. If you have MASLD or hepatic IR, alcohol reduction (or elimination) is recommended by current clinical guidelines.
What medications are used to treat hepatic insulin resistance?
In addition to lifestyle changes, several medications can target hepatic insulin resistance:
Metformin: First-line; reduces hepatic glucose production via AMPK activation.
Pioglitazone: Improves hepatic insulin sensitivity and reduces liver fat in MASH (strong evidence).
GLP-1 receptor agonists (e.g., semaglutide, liraglutide): Promote significant weight loss, reduce liver fat, and improve insulin resistance.
Resmetirom (approved 2024): A thyroid hormone receptor-β agonist specifically approved for MASH with moderate-to-advanced fibrosis.
These should be considered under medical supervision, especially in patients with prediabetes, type 2 diabetes, or progressing MASLD. Medication works best when combined with diet and exercise.
How does sleep affect hepatic insulin resistance?
Sleep deprivation — even a single night of poor sleep — significantly impairs hepatic insulin sensitivity. Circadian disruption dysregulates the cortisol and growth hormone rhythms that control hepatic glucose and lipid metabolism overnight. Chronic sleep restriction (less than 6 hours/night) is independently associated with higher HOMA-IR, elevated liver fat, and worse glycemic control. Prioritizing 7–9 hours of quality sleep is a non-negotiable foundation of any hepatic IR reversal strategy.
Can children develop hepatic insulin resistance?
Yes — pediatric MASLD and hepatic insulin resistance are now recognized as growing epidemics, particularly in children with obesity. The same mechanisms apply: excess refined carbohydrates, sedentary behavior, gut dysbiosis, and visceral fat accumulation. Early intervention in childhood is critical, as pediatric MASLD can progress to significant fibrosis by early adulthood. If your child has obesity, ask their pediatrician about screening for fatty liver and insulin resistance.
How does stress affect the liver's insulin response?
Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, chronically elevating cortisol levels. As the 2026 Goldberg and Goldstein review in Nature Reviews Endocrinology details, cortisol is a potent fasting signal to the liver — it upregulates gluconeogenic enzymes (PEPCK, G6Pase) and cooperates with glucagon to drive hepatic glucose output. Chronically elevated cortisol essentially keeps the liver in a "fasted, fuel-producing" state even when you've just eaten. Stress management — through mindfulness, exercise, adequate sleep, and social connection — is therefore a direct metabolic intervention, not just a nice-to-have.
15. Conclusion and Your Action Plan
Hepatic insulin resistance sits at the intersection of nearly every major metabolic epidemic of the 21st century: type 2 diabetes, fatty liver disease, obesity, cardiovascular disease, and even certain cancers. Yet it is largely invisible in mainstream health conversations — and that needs to change.
The science of 2023–2026 has given us an increasingly precise understanding of exactly what goes wrong in the liver and, critically, how to fix it:
The "selective IR" paradox explains why the liver simultaneously overproduces glucose and fat — and why treatment must restore balanced insulin signaling, not simply suppress it
Fasting hormones are not just "anti-insulin" signals — they cooperate in a sophisticated network that, when dysregulated in IR, continuously drives hepatic glucose overproduction
Curcumin's newly revealed PINK1/Parkin mitophagy mechanism offers a targeted, natural therapeutic approach with multi-layered evidence
The gut-liver axis is a legitimate, modifiable therapeutic target — diet, probiotics, and fiber directly reshape the microbial drivers of hepatic inflammation and insulin resistance
Hepatic insulin resistance is reversible — and the lifestyle tools to do it are in your hands right now
Your 90-Day Hepatic IR Reversal Action Plan
Week 1–4: Foundation
Eliminate SSBs and ultra-processed foods
Start 30 min daily walking
Add 2–3 servings fatty fish/week
Get baseline labs (glucose, insulin, liver panel)
Optimize sleep to 7–9 hours
Week 5–8: Intensify
Add 2× resistance training/week
Implement 10–12 hour eating window
Start bioavailable curcumin (500–1,000 mg/day)
Add omega-3 supplement (2 g EPA+DHA)
Incorporate daily stress-reduction practice
Week 9–12: Optimize
Transition to full Mediterranean dietary pattern
Consider adding berberine (discuss with doctor)
Recheck labs — expect measurable improvements
Maintain exercise consistency
Add prebiotic fiber for gut microbiome support
⚠️ Consult Your Healthcare Provider
This guide is educational and evidence-based, but it is not a substitute for personalized medical advice. If you have or suspect type 2 diabetes, MASLD, liver disease, or significant hepatic insulin resistance, work with your doctor or a registered dietitian to implement these strategies safely — especially if you take medications that affect blood glucose or liver function.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
De Novo Lipogenesis Explained: How Sugar Turns Into Liver Fat and High Triglycerides
Rethinking Dietary Fats: What New Research Reveals About Plant vs. Animal Fats | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
References
Bo, T., Gao, L., Yao, Z., et al. (2024). Hepatic selective insulin resistance at the intersection of insulin signaling and metabolic dysfunction-associated steatotic liver disease. Cell Metabolism, 36(5), 947–968. https://doi.org/10.1016/j.cmet.2024.04.006
Chalasani, N., Younossi, Z., Lavine, J. E., Charlton, M., Cusi, K., Rinella, M., Harrison, S. A., Shushman, G., & Sanyal, A. J. (2018). The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology, 67(1), 328–357. https://doi.org/10.1002/hep.29367
Dua, A., Kumari, R., Singh, M., et al. (2025). Metabolic dysfunction-associated steatotic liver disease (MASLD): The interplay of gut microbiome, insulin resistance, and diabetes. Frontiers in Medicine, 12, Article 1618275. https://doi.org/10.3389/fmed.2025.1618275
Friedman, S. L., Neuschwander-Tetri, B. A., Rinella, M., & Sanyal, A. J. (2018). Mechanisms of NAFLD development and therapeutic strategies. Nature Medicine, 24(7), 908–922. https://doi.org/10.1038/s41591-018-0104-9
Goldberg, D., & Goldstein, I. (2026). Endocrine regulation of the hepatic fasting response: Cues, cooperation and consequences. Nature Reviews Endocrinology, 22, 302–316. https://doi.org/10.1038/s41574-025-01228-3
Groeger, M., et al. (2023). Modeling and therapeutic targeting of inflammation-induced hepatic insulin resistance using human iPSC-derived hepatocytes and macrophages. Nature Communications, 14, Article 39311. https://doi.org/10.1038/s41467-023-39311-w
Guo, Z., Zhang, H., & Kong, Y. (2026). Curcumin ameliorates hepatic insulin resistance by activating PINK1/Parkin-mediated mitophagy. Scientific Reports, 16, Article 47924. https://doi.org/10.1038/s41598-026-47924-6
Hallsworth, K., Thoma, C., Moore, S., Ploetz, T., Anstee, Q. M., Taylor, R., Day, C. P., & Trenell, M. I. (2011). Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut, 60(9), 1278–1283. https://doi.org/10.1136/gut.2011.242073
Jiang, S., et al. (2026). Targeting the PI3K/AKT signaling pathway: An important molecular mechanism of herbal medicine in the treatment of MASLD/MASH. Frontiers in Nutrition, 12, Article 1743899. https://doi.org/10.3389/fnut.2025.1743899
Knowler, W. C., Barrett-Connor, E., Fowler, S. E., Hamman, R. F., Lachin, J. M., Walker, E. A., Nathan, D. M., & Diabetes Prevention Program Research Group. (2002). Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine, 346(6), 393–403. https://doi.org/10.1056/NEJMoa012512
Loomba, R., & Sanyal, A. J. (2013). The global NAFLD epidemic. Nature Reviews Gastroenterology & Hepatology, 10(11), 686–690. https://doi.org/10.1038/nrgastro.2013.171
Miele, L., et al. (2022). Gut microbiota in NAFLD and steatohepatitis. Journal of Hepatology, 77(2), 554–561. https://doi.org/10.1016/j.jhep.2022.02.024
Neeland, I. J., Ross, R., Després, J. P., Matsuzawa, Y., Yamashita, S., Shai, I., Seidell, J., Magni, P., Santos, R. D., Arsenault, B., Richelsen, B., ... & International Atherosclerosis Society; International Chair on Cardiometabolic Risk. (2019). Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. The Lancet Diabetes & Endocrinology, 7(9), 715–725. https://doi.org/10.1016/S2213-8587(19)30084-1
Niranjan, S., Phillips, B. E., & Giannoukakis, N. (2023). Uncoupling hepatic insulin resistance – hepatic inflammation to improve insulin sensitivity and to prevent impaired metabolism-associated fatty liver disease in type 2 diabetes. Frontiers in Endocrinology, 14, Article 1193373. https://doi.org/10.3389/fendo.2023.1193373
Petersen, K. F., Dufour, S., Savage, D. B., Bilz, S., Solomon, G., Yonemitsu, S., Cline, G. W., Befroy, D., Zemany, L., Kahn, B. B., Papademetris, X., Rothman, D. L., & Shulman, G. I. (2007). The role of skeletal muscle insulin resistance in the pathogenesis of the metabolic syndrome. Proceedings of the National Academy of Sciences, 104(31), 12587–12594. https://doi.org/10.1073/pnas.0705408104
Samuel, V. T., & Shulman, G. I. (2018). Nonalcoholic fatty liver disease as a nexus of metabolic and hepatic diseases. Cell Metabolism, 27(1), 22–41. https://doi.org/10.1016/j.cmet.2017.08.002
Sanyal, A. J., Chalasani, N., Kowdley, K. V., McCullough, A., Diehl, A. M., Bass, N. M., Neuschwander-Tetri, B. A., Lavine, J. E., Tonascia, J., Unalp, A., Van Natta, M., Clark, J., Brunt, E. M., Kleiner, D. E., Hoofnagle, J. H., & NASH CRN. (2010). Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. New England Journal of Medicine, 362(18), 1675–1685. https://doi.org/10.1056/NEJMoa0907929
Sun, D. Y., et al. (2026). Advances and perspectives in curcumin regulation of systemic metabolism: A focus on multi-organ mechanisms. Antioxidants, 15(1), Article 109. https://doi.org/10.3390/antiox15010109
Targher, G., Day, C. P., & Bonora E. (2010). Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. New England Journal of Medicine, 363(14), 1341–1350. https://doi.org/10.1056/NEJMra0912063
Titchenell, P. M., Lazar, M. A., & Birnbaum, M. J. (2017). Unraveling the regulation of hepatic metabolism by insulin. Trends in Endocrinology & Metabolism, 28(7), 497–505. https://doi.org/10.1016/j.tem.2017.03.003
Wang, L., Zhang, B., Huang, F., Liu, B., & Xie, Y. (2016). Curcumin inhibits lipolysis via suppression of ER stress in adipose tissue and prevents hepatic insulin resistance. Journal of Lipid Research, 57(7), 1243–1255. https://doi.org/10.1194/jlr.M067397
Younossi, Z. M., Koenig, A. B., Abdelatif, D., Fazel, Y., Henry, L., & Wymer, M. (2016). Global epidemiology of nonalcoholic fatty liver disease — Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology, 64(1), 73–84. https://doi.org/10.1002/hep.28431
[Author Placeholder]. (2016). Curcumin-related research on MASLD/NAFLD. Journal of Agricultural and Food Chemistry. https://doi.org/10.1021/acs.jafc.6c01142 (Note: This partial citation lacked author names in the raw text; please verify and insert specific authors if available).