How Much Exercise Do You Really Need for Heart Health? New Research Reveals the Answer
New studies reveal the exercise dose linked to better heart health. Learn why 150 minutes is a great start—and what additional benefits more activity may provide.
EXERCISEHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/21/202620 min read
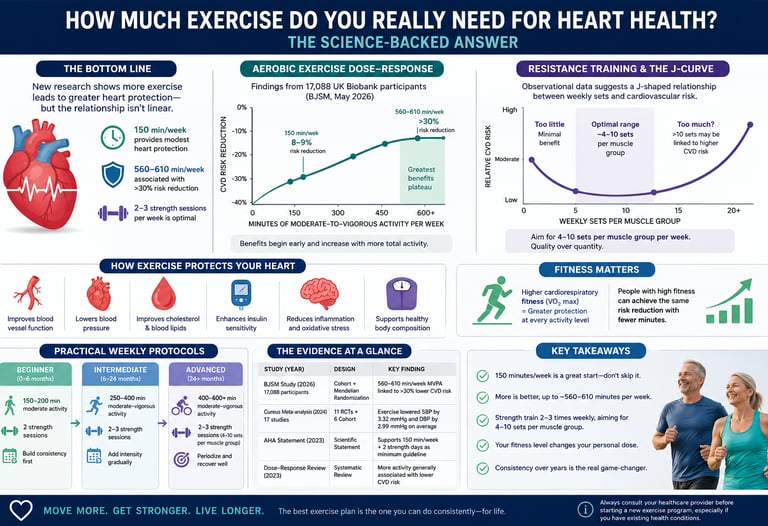
For heart health, aim for at least 150 minutes of moderate aerobic activity plus 2 resistance-training sessions weekly. New research suggests 560–610 minutes weekly may provide greater protection, though benefits begin well before that level.
Key takeaways
1. The 150-min/week floor still matters
150 minutes of moderate-to-vigorous aerobic activity remains a robust, evidence-backed minimum. BJSM 2026 data shows it cuts cardiovascular risk 8–9%. It is not outdated. It is the starting line, not the finish.
2. The high-benefit zone is 3-4x higher
For >30% cardiovascular risk reduction, the new 2026 cohort + Mendelian randomization data points to 560–610 min/week. Only 12% of people hit this. This is an aspirational target, not a mandate. More minutes still help, but with diminishing returns.
3. Resistance training has a J-curve, not a straight line
Cardiovascular benefit from weights peaks at 40–60 min/week total. Beyond that, observational data shows the protection plateaus or attenuates. Proposed reasons: arterial stiffness and unresolved inflammation. This applies to heart health specifically, not strength or hypertrophy goals.
4. Aerobic and resistance work through different pathways
Aerobic training improves endothelial function, autonomic balance, and VO2 max. Resistance training drives insulin sensitivity, body composition, and glucose control. Combined training gives the broadest risk-factor coverage. They are not interchangeable.
5. Your fitness level changes your dose
Low cardiorespiratory fitness means you need 30–50 more minutes/week than highly fit people for the same % risk reduction. But your early gains are also the steepest. Fitness is both a modifier and an outcome.
6. Blood pressure responds fast and measurably
A 2024 meta-analysis of 17 studies found exercise lowers systolic BP by 3.32 mmHg and diastolic by 2.99 mmHg on average. That is clinically meaningful and comparable to some medications. Effect sizes vary, but the direction is consistent.
7. Volume increases must be gradual and recovered
The biggest mistakes are jumping volume too fast and ignoring recovery. Risk of injury, burnout, and blunting the J-curve benefit rises without progression discipline. Cap increases at ~10% per week and prioritize sleep, protein, and rest days.
8. The evidence is strong, but not absolute
Even with Mendelian randomization, these are still observational findings with healthy-volunteer bias. Resistance J-curve mechanisms remain hypothetical. Treat the numbers as population-level guidance, not personal guarantees. Use them to inform your plan with your physician, not replace clinical judgment.
Introduction
If you've ever wondered whether your 20-minute walk is "enough" — or whether you should be lifting heavier, running longer, or doing more of everything for your heart — you're asking the right question, and the answer has actually changed in the last few years.
For decades, the public health message was simple: 150 minutes of moderate aerobic activity per week, plus two days of resistance training. That advice isn't wrong. But a wave of large, methodologically rigorous studies published between 2023 and 2026 has added crucial nuance: more exercise isn't always better, and "enough" depends heavily on your starting fitness level.
In this guide, you'll learn:
The real dose-response relationship between exercise and cardiovascular disease (CVD) risk
Why resistance training appears to follow a J-shaped curve — and what that means for your weekly workout plan
The newest data showing that 560–610 minutes per week of moderate-to-vigorous activity may be needed for "substantial" heart protection — and why that doesn't mean you've been wasting your time at 150 minutes
How cardiorespiratory fitness (VO2 max) changes how much exercise you personally need
Practical, step-by-step protocols you can start this week
The myths, mistakes, and FAQs that trip up even experienced exercisers
This article is built on peer-reviewed studies, systematic reviews, and a Mendelian randomization analysis — a method that gets closer to establishing cause-and-effect than typical observational research. We'll walk through what the data actually shows, where it's strong, and where it's still uncertain, because in cardiovascular health, how you interpret a study matters as much as the headline number.
1. The Big Picture: What the Latest Research Actually Found
Cardiovascular disease remains the leading cause of death worldwide, and exercise is one of the few interventions that reliably moves the needle on multiple risk factors at once — blood pressure, cholesterol, body composition, insulin sensitivity, and vascular function.
A 2024 systematic review and meta-analysis published in Cureus, which pooled 17 studies (11 randomized controlled trials and 6 cohort studies), found that exercise interventions produced a statistically significant average reduction in systolic blood pressure of 3.32 mmHg and diastolic blood pressure of 2.99 mmHg, along with improvements in cholesterol and BMI. People who exercised also showed a trend toward lower stroke and heart attack risk compared with non-exercisers, though the researchers were careful to note substantial heterogeneity across the pooled studies, meaning effect sizes varied a lot from trial to trial depending on the population, exercise type, and duration.
That heterogeneity is not a weakness to gloss over — it's the whole story. It tells us that "exercise reduces CVD risk" is true on average, but the size of your personal benefit depends on dose, modality, baseline fitness, and how long you sustain the habit.
Key takeaway: The relationship between physical activity and heart health is not a simple straight line where every additional minute buys you an equal slice of protection. Two of the most important and recent papers — one on resistance training dosing and one on combined activity-and-fitness dosing — both point to non-linear patterns. That's the central theme of this article.
2. Aerobic Exercise Dose-Response: The 560–610 Minute Study Explained
In May 2026, a large cohort and Mendelian randomization study published in the British Journal of Sports Medicine reshaped how researchers think about exercise "minimums."
What the study did
Researchers analyzed data from 17,088 UK Biobank participants (average age 57, 56% female) who wore wrist-based activity trackers for seven consecutive days and completed a cycle test to estimate VO2 max — the gold-standard proxy for cardiorespiratory fitness. The team then tracked cardiovascular events (atrial fibrillation, myocardial infarction, heart failure, and stroke) over an average follow-up of 7.8 years, during which 1,233 cardiovascular events occurred.
Critically, the researchers didn't stop at observational correlation. They also applied Mendelian randomization, a genetic-epidemiology technique that uses naturally occurring genetic variants associated with physical activity as a proxy for "randomizing" exposure — helping to strengthen the case for causality rather than mere association (a major limitation of most exercise-health observational research).
What they found
People who met the standard guideline of 150 minutes/week of moderate-to-vigorous physical activity (MVPA) saw a modest 8–9% reduction in cardiovascular risk — consistent across fitness levels.
To reach a >30% risk reduction (classified as "substantial" protection), participants needed 560–610 minutes per week — roughly 3 to 4 times the current guideline.
Only 12% of the study population actually achieved that higher volume.
People with lower cardiorespiratory fitness needed more minutes to get the same benefit as fitter people. For a 20% risk reduction, the least-fit group needed about 370 minutes/week, versus 340 minutes/week for the fittest group — a real but modest 30-minute "fitness penalty."
How to interpret this responsibly
This is where clinical relevance and statistical validity diverge from headlines. A few important caveats:
This is still an observational study, even with the genetic-causality reinforcement. The authors themselves state that no firm cause-and-effect conclusion can be drawn, and that the UK Biobank cohort tends to be healthier and more health-conscious than the general population (a phenomenon called the "healthy volunteer" bias).
The 150-minute guideline is not being overturned — the researchers explicitly describe it as "a robust universal minimum." The new finding adds a second, higher target for people who want to maximize benefit, not a replacement floor.
Going from 0 to 150 minutes/week produces the steepest drop in absolute risk. Going from 150 to 600 minutes produces a smaller, though still meaningful, additional drop. This is a classic diminishing-but-still-positive returns curve for aerobic activity — distinct from the J-shaped pattern seen in resistance training (more on that next).
Sedentary time outside of structured exercise wasn't captured, which limits how precisely we can translate "minutes of MVPA" into a real-world daily routine.
Bottom line: 150 minutes a week remains a legitimate, evidence-based floor that meaningfully lowers risk. If you have the time, health status, and joint tolerance to do more — building gradually toward 300–600 minutes a week of brisk walking, cycling, swimming, or similar moderate-intensity activity — the data suggests further, real cardiovascular benefit, especially if your fitness level is currently low.
3. Resistance Exercise and the J-Shaped Curve: Is More Really Worse?
This is the part of the conversation that surprises most people, including many fitness enthusiasts: when it comes to resistance exercise (weight training) specifically, the dose-response relationship doesn't look like aerobic exercise's "more is generally better, with diminishing returns." Instead, it appears J-shaped.
What the research shows
A 2023 narrative review in Current Cardiology Reports by Duck-chul Lee and I-Min Lee — two of the most cited researchers in exercise epidemiology — synthesized recent observational studies on resistance training dose and cardiovascular outcomes. Their central finding:
Resistance training was associated with lower cardiovascular disease risk and lower all-cause mortality up to roughly 40–60 minutes per week.
Beyond that point, the protective association attenuated, flattened, or in some studies reversed, with higher weekly resistance-training volumes associated with less benefit, or even a return toward baseline risk.
The American Heart Association's 2023 scientific statement on resistance training and cardiovascular disease similarly supports resistance training as safe and beneficial for both healthy adults and those with existing CVD — typically recommending 2 or more sessions per week — without specifying an upper time boundary as precisely as the Lee & Lee review.
Why might more resistance training stop helping (or even hurt)?
The review authors propose two plausible — but not yet definitively proven — biological mechanisms:
Increased arterial stiffness. Heavy, high-volume resistance training causes repeated, large spikes in blood pressure during lifts. Some research suggests chronically high training volumes may promote stiffening of the arterial walls over time, which is itself an independent cardiovascular risk factor.
Chronic low-grade inflammation. Without adequate recovery, very high training volumes may trigger a sustained inflammatory load rather than the beneficial, transient inflammatory response seen with moderate exercise.
Why this finding deserves a cautious read
This is exactly the kind of result where validity of data matters more than the soundbite. A few things to weigh:
These are observational associations, not randomized controlled trials. People who lift weights for 5+ hours a week may differ systematically from moderate lifters in ways researchers can't fully control for (occupation, supplement use, undiagnosed conditions, genetics, or even reverse causation — sicker people sometimes can't sustain high training volumes).
"Minutes of resistance exercise" is a crude dose metric. It doesn't capture training intensity, load, recovery quality, or whether the time was spent on compound lifts versus accessory work — all of which plausibly affect cardiovascular strain differently.
The review's authors themselves frame this as filling a knowledge gap, not closing it — they explicitly call for dedicated dose-response trials (one such trial, sponsored by the University of Pittsburgh in collaboration with Harvard and the NHLBI, is currently underway as of 2025–2026 to test this directly).
Bottom line: Current evidence suggests a sweet spot of roughly 40–60 minutes of resistance training per week — easily achieved with two or three 20-minute sessions — captures most of the cardiovascular benefit. This doesn't mean serious lifters training for strength or hypertrophy goals are necessarily harming their hearts; it means the cardiovascular-specific benefit may plateau earlier than people assume, so additional volume should be driven by other goals (strength, muscle, performance) rather than an assumption of ever-increasing heart protection.
4. The Mechanisms: Why Exercise Protects (and Sometimes Stresses) the Heart
Understanding why exercise helps makes the dose-response curves much easier to apply intelligently.
Aerobic exercise mechanisms
Endothelial function and nitric oxide: Aerobic activity increases shear stress on blood vessel walls, which boosts nitric oxide production — a molecule that relaxes blood vessels (vasodilation) and reduces arterial stiffness.
Autonomic balance: Regular aerobic training shifts the body away from sympathetic ("fight or flight") dominance toward greater parasympathetic ("rest and digest") tone, which is linked to lower resting heart rate and blood pressure.
Lipid and inflammatory profile: Exercise lowers triglycerides and LDL cholesterol while raising HDL cholesterol in many studies, and reduces circulating inflammatory markers like C-reactive protein (CRP) — both central players in the atherosclerotic process (plaque buildup in arteries).
Cardiorespiratory fitness itself: Higher VO2 max reflects a more efficient heart, lungs, and vascular system working together — and is one of the single strongest predictors of long-term cardiovascular and all-cause mortality risk in the literature.
Resistance exercise mechanisms
Improved insulin sensitivity and glucose handling: Muscle is metabolically active tissue; building and using it improves how your body manages blood sugar, an upstream driver of cardiometabolic risk.
Favorable body composition: Resistance training helps maintain or build lean mass while reducing visceral fat, which is more metabolically harmful than subcutaneous fat.
Blood pressure adaptation over time: Despite acute blood pressure spikes during a heavy lift, chronic resistance training is associated with modest reductions in resting blood pressure in most moderate-dose studies.
The double-edged sword of volume: As discussed above, very high training volumes may shift this balance, with arterial stiffness and unresolved inflammation potentially offsetting some benefits — the proposed explanation behind the J-curve.
A 2023 state-of-the-art synthesis
A 2023 review in Progress in Cardiovascular Diseases (Isath et al.) reinforced that both aerobic and resistance exercise produce measurable, clinically relevant improvements across traditional cardiovascular risk factors, while also emphasizing that combining both modalities — rather than relying on either alone — tends to produce the most comprehensive risk-factor improvement profile across blood pressure, lipids, glycemic control, and body composition.
5. How Cardiorespiratory Fitness Changes Your Personal "Dose"
One of the most clinically useful insights from the 2026 BJSM study is that cardiorespiratory fitness (CRF) and physical activity have a joint, not independent, effect on cardiovascular risk.
In plain terms: two people doing the exact same number of weekly exercise minutes can have meaningfully different risk profiles depending on their underlying fitness level. The study found that the least-fit participants needed roughly 30–50 more minutes per week than the fittest participants to achieve equivalent cardiovascular risk reduction.
Why this matters practically
If you're just starting out and your fitness is low, don't be discouraged that you "need more" exercise — your relative improvement per minute invested is actually often larger early on, even if your absolute minute target is higher.
A simple way to estimate your own fitness trajectory: track resting heart rate and how you feel completing a fixed test (like a brisk 1-mile walk or the Cooper 12-minute run test) every 4–6 weeks. Improving times or lower heart rate at the same pace indicates rising CRF — and a shrinking "fitness penalty."
This is also a strong argument for combining aerobic and resistance training, since resistance training improves functional capacity and can make sustained aerobic activity easier to tolerate, indirectly supporting higher MVPA volumes over time.
6. Practical Protocols: How to Apply This to Your Week
Here's how to translate the research into an actual weekly plan, organized by where you're starting from.
Step 1: Establish your floor (Weeks 1–4)
Aerobic: 150 minutes/week of moderate activity (e.g., 30 minutes, 5 days/week of brisk walking, cycling, or swimming). This alone produces a real, evidence-backed 8–9% risk reduction.
Resistance: 2 sessions/week, 20–30 minutes each, covering major muscle groups (legs, back, chest, shoulders, core). This lands comfortably within the 40–60 minute "sweet spot" identified in the Lee & Lee review.
Step 2: Build toward the higher-benefit zone (Months 2–6)
Aerobic: Gradually increase toward 300 minutes/week by adding duration or frequency (e.g., 45–60 minutes, 5–6 days/week), or incorporate some vigorous-intensity sessions, which count double toward MVPA minute targets in most guidelines.
Resistance: Hold steady around 40–60 minutes/week total for cardiovascular purposes. If your goals include strength or muscle gain beyond heart health, additional volume can be added for those goals specifically, understood as separate from cardiovascular dosing.
Step 3: Approach the high-protection zone (if appropriate for you)
Aerobic: Working toward 560–600 minutes/week (roughly 80–90 minutes/day) is where the BJSM data showed >30% risk reduction. This is a substantial time commitment and should be built up gradually over months, not weeks, with attention to joint health, recovery, and sustainability.
This level isn't necessary or realistic for everyone — and the data shows even modest increases above 150 minutes continue to add benefit, so there's no cliff where effort below 560 minutes "doesn't count."
A sample weekly framework (intermediate level)
Weekly Fitness Schedule
Monday: Brisk walk or cycling (Moderate) | 45 min
Tuesday: Full-body resistance training (Strength) | 25–30 min
Wednesday: Swimming, rowing, or jogging (Moderate) | 45 min
Thursday: Full-body resistance training (Strength) | 25–30 min
Friday: Cardio session (Moderate-to-Vigorous) | 45–60 min
Saturday: Hike or long ride (Aerobic endurance) | 60–90 min
Sunday: Walk or mobility work (Active recovery) | 20–30 min
Weekly Breakdown & Benefits
Aerobic Total: 260–330 minutes
Resistance Total: 50–60 minutes
The Payoff: Comfortably exceeds basic health guidelines while hitting the resistance sweet spot. This builds a realistic, sustainable path toward optimal aerobic protection over time.Safety checklist before increasing volume or intensity
✅ Get medical clearance if you have known heart disease, uncontrolled blood pressure, or haven't exercised in years and are over 40–45.
✅ Increase volume or intensity gradually — no more than ~10% per week — to reduce injury and overtraining risk.
✅ Prioritize recovery (sleep, protein intake, rest days) especially as resistance training volume rises.
✅ Watch for warning signs during exercise (chest pain, unusual shortness of breath, dizziness, irregular heartbeat) and stop immediately if they occur.
✅ Always consult your doctor before starting a new exercise program, particularly if you have existing cardiovascular risk factors.
7. Evidence Summary
Lee & Lee (2023) | Current Cardiol Rep
Design & Population: Narrative review of observational studies looking at the general adult population.
Key Finding: Discovered a "J-shaped curve" for resistance training. The cardiovascular disease (CVD) and mortality benefits actually peak at just 40–60 minutes per week.
Evidence Strength: Moderate — Synthesizes observational data, though the exact biological mechanisms are still hypothetical.
Design & Population: Cohort study paired with Mendelian randomization (a method using genetic variants to estimate causal relationships) analyzing 17,088 UK Biobank adults (average age 57).
Key Finding: 150 minutes/week of moderate-to-vigorous physical activity (MVPA) yielded an 8–9% risk reduction. Pushing that to 560–610 minutes/week unlocked a greater than 30% risk reduction. Cardiorespiratory fitness directly modifies the required dose.
Evidence Strength: Strong for the association; supportive (but not definitive) for direct causality via the genetic data.
Masmoum et al. (2024) | Cureus
Design & Population: Systematic review and meta-analysis of 17 studies (11 randomized controlled trials and 6 cohorts) focusing on adults 18 and older.
Key Finding: Exercise significantly improved clinical markers, reducing systolic blood pressure by 3.32 mmHg and diastolic by 2.99 mmHg, alongside improvements in cholesterol and BMI.
Evidence Strength: Moderate-to-High for blood pressure improvements; however, there was high heterogeneity (wide variation in data) for specific stroke and heart attack outcomes.
Isath et al. (2023) | Prog Cardiovasc Dis
Design & Population: State-of-the-art narrative review tracking both general and clinical patient populations.
Key Finding: While both aerobic and resistance training independently improve traditional cardiovascular risk factors, combining both training styles yields the optimal health outcome.
Evidence Strength: Moderate — A narrative synthesis built on existing trial and cohort evidence.
AHA Scientific Statement (2023) | Circulation
Design & Population: Multi-author expert consensus statement covering healthy adults and patients with existing cardiovascular disease.
Key Finding: Formally establishes that resistance training is both safe and highly effective for preventing and managing CVD when performed at 2 or more sessions per week.
Evidence Strength: High — Derived from a multi-author expert consensus built on a massive, robust evidence base.
8. Common Myths & Mistakes
Myth 1: "If 150 minutes is good, doubling it must be twice as good." Not necessarily. The dose-response curve for aerobic exercise shows diminishing (but still positive) returns, while resistance training shows an actual J-shaped pattern where benefit can plateau or reverse beyond 40–60 minutes/week.
Myth 2: "Lifting heavy weights is bad for your heart." This is an oversimplification of the J-curve data. Moderate resistance training (2–3 sessions, 40–60 minutes/week total) is consistently linked to lower cardiovascular risk. The concern applies specifically to very high weekly volumes, and even then, the evidence is observational, not proof of harm for any individual lifter.
Myth 3: "If I'm not very fit, exercise won't help me as much." The opposite tends to be true in absolute terms — lower-fitness individuals often see the largest relative improvements when they start. They may need somewhat more total minutes to reach the same percentage risk reduction as a highly fit person, but the benefit curve is steep early on.
Myth 4: "Cardio and weights are interchangeable for heart health." They work through different, complementary mechanisms (vascular/autonomic adaptations vs. metabolic/body composition adaptations). Reviews consistently find combined training produces the broadest risk-factor improvement.
Myth 5: "An observational study with a 30%+ risk reduction proves exercise prevents heart attacks for everyone." Even with Mendelian randomization strengthening the causal case, this remains population-level evidence with documented limitations (healthy volunteer bias, estimated rather than directly measured fitness in some analyses, and incomplete capture of sedentary behavior).
Mistake: Increasing volume too fast. Jumping from 150 to 500+ weekly minutes in a few weeks dramatically raises injury and burnout risk. Gradual progression over months is safer and more sustainable.
Mistake: Ignoring recovery. Especially relevant to the resistance-training J-curve — without adequate rest, higher training volumes may compound inflammatory and cardiovascular strain rather than just adding benefit.
9. Frequently Asked Questions
Q1: What is the minimum amount of exercise needed for heart health? A: Current guidelines and the 2026 BJSM cohort study both support 150 minutes per week of moderate-to-vigorous aerobic activity as an evidence-based minimum, associated with an 8–9% reduction in cardiovascular risk, plus 2 or more resistance training sessions per week.
Q2: Is more exercise always better for your heart? A: For aerobic exercise, more activity (up to at least 560–610 minutes/week in current data) continues to add benefit, though with diminishing returns. For resistance training specifically, evidence suggests benefits may plateau or even reverse beyond roughly 40–60 minutes per week.
Q3: How many minutes of resistance training per week is optimal for the heart? A: A 2023 review in Current Cardiology Reports found the strongest cardiovascular benefit clustered around 40–60 minutes per week, achievable with two or three short sessions.
Q4: Can too much exercise damage your heart? A: Some observational research links very high-volume resistance training to attenuated benefits, possibly via arterial stiffness or chronic inflammation, but this is not the same as proof of heart damage. Separately, extreme endurance training has been associated with increased coronary artery calcification in some athlete studies, though plaque composition in athletes often appears more stable (calcified rather than mixed). This remains an active research area — moderate, well-recovered training is not the concern here.
Q5: What is cardiorespiratory fitness, and why does it matter? A: Cardiorespiratory fitness (CRF) reflects how efficiently your heart, lungs, and muscles deliver and use oxygen, usually estimated via VO2 max. It's one of the strongest known predictors of cardiovascular and all-cause mortality risk, and it modifies how much exercise you specifically need for a given risk reduction.
Q6: Should I do cardio or weights for heart health? A: Both, ideally. They work through different mechanisms — aerobic exercise primarily improves vascular and autonomic function, while resistance training improves insulin sensitivity and body composition. Reviews consistently favor combined training for the broadest cardiovascular benefit.
Q7: How quickly will exercise lower my blood pressure? A: Meta-analysis data (Masmoum et al., 2024) shows average reductions of about 3.3 mmHg systolic and 3.0 mmHg diastolic blood pressure across studied exercise interventions, though individual results vary and most trials measure effects after several weeks to months of consistent training.
Q8: Does walking count toward these exercise minutes? A: Yes, brisk walking that raises your heart rate into the moderate-intensity zone counts fully toward MVPA minute targets used in this research.
Q9: Is the 560–610 minute target realistic for most people? A: Only about 12% of participants in the BJSM study achieved this level, underscoring that it's an aspirational "high-protection" target, not a baseline expectation. The 150-minute guideline remains a legitimate, beneficial floor.
Q10: Do less-fit people need to exercise more than fit people? A: Yes, modestly. The BJSM study found people with the lowest fitness needed roughly 30–50 more minutes per week than the fittest participants to achieve equivalent cardiovascular risk reduction.
Q11: What's the difference between an observational study and a Mendelian randomization study? A: An observational study tracks what people naturally do and measures associated outcomes, which can be confounded by other lifestyle or genetic factors. Mendelian randomization uses genetic variants linked to a behavior (like physical activity) as a natural "randomization" tool, helping researchers get closer to inferring causation — though it still has its own limitations and assumptions.
Q12: Should older adults or people with existing heart disease follow the same targets? A: The American Heart Association's 2023 scientific statement supports resistance training as safe and beneficial for people with existing cardiovascular disease, generally under medical guidance and often with cardiac rehabilitation supervision for higher-risk individuals. Always consult your physician before significantly changing your exercise routine if you have a cardiac history.
10. Conclusion and Action Steps
The science on exercise dosing for cardiovascular health has matured from a single blanket number into a more precise, personalized picture:
150 minutes/week of moderate aerobic activity is a real, evidence-backed floor — don't skip it, and don't discount it just because higher targets exist.
560–610 minutes/week represents a higher-benefit zone worth building toward gradually if your life circumstances and health allow it.
40–60 minutes/week of resistance training appears to capture most of the cardiovascular-specific benefit; more volume should be driven by strength or physique goals, not an assumption of unlimited extra heart protection.
Your personal fitness level shifts your specific "dose" — lower fitness generally means somewhat more minutes needed for equivalent benefit, but also often means a bigger early payoff.
Your next steps this week:
Track your current weekly aerobic and resistance minutes honestly for 7 days.
Compare your numbers to the framework above and identify your next realistic increment — not the end goal.
Schedule resistance sessions like appointments; 40–60 minutes/week is a low time investment for the cardiovascular payoff the data suggests.
If you have any cardiovascular risk factors or existing diagnosis, talk to your doctor before increasing volume or intensity.
This article isn't medical advice — it's a synthesis of the current scientific literature designed to help you have a more informed conversation with your healthcare provider and make smarter training decisions. Cardiovascular health is built through consistent, sustainable habits, not perfect adherence to a single number.
Author's Note: A Clinician's Perspective
As a physician, one of the most common questions I hear from patients is: "Doctor, how much exercise do I really need for my heart?" Many people assume that if they cannot achieve the ideal exercise target, there is little point in trying. The scientific evidence tells a very different story.
What I find most encouraging from the latest research is that the greatest health gains often occur when people move from being inactive to simply becoming moderately active. While newer studies suggest that higher amounts of physical activity may provide additional cardiovascular protection, the benefits begin long before you reach those ambitious targets.
I often think of a 58-year-old patient with high blood pressure, prediabetes, and a sedentary lifestyle. He was convinced that exercise only counted if it involved intense gym workouts. Instead, we started with a simple goal: a 30-minute brisk walk five days per week and two short resistance-training sessions. Six months later, he had lost weight, his blood pressure had improved, his blood sugar levels were lower, and he reported having more energy than he had felt in years. Most importantly, he had built a sustainable habit rather than pursuing a short-lived fitness challenge.
The lesson is that cardiovascular health is rarely determined by a single workout, a specific exercise program, or a perfect weekly target. It is shaped by consistent movement accumulated over months and years. Whether you are currently exercising 30 minutes per week or 300 minutes per week, the next step forward is what matters most.
The best exercise program is not necessarily the one supported by the most impressive statistics—it is the one you can continue doing for the rest of your life.
Always consult your healthcare provider before starting a new exercise program, particularly if you are over 45, previously sedentary, or have a history of cardiovascular disease, hypertension, or diabetes. For individuals with established cardiovascular disease, initiate resistance training within a supervised cardiac rehabilitation program.
Related Articles
How Hard Should You Exercise for Heart Health? New Research Reveals the Answer
Non-Negotiable Health: Why All Women Need Resistance Training, Not Just Cardio | DR T S DIDWAL
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
References
Lee, D., Lee, I.M. (2023). Optimum Dose of Resistance Exercise for Cardiovascular Health and Longevity: Is More Better? Current Cardiology Reports, 25, 1573–1580. https://doi.org/10.1007/s11886-023-01976-6
Liang, Z., Du, S., Zhao, S., Wang, X., Yan, Q., Xu, B., Ng, S., & Ning, Z. (2026). Joint non-linear dose-response associations of device-measured physical activity and cardiorespiratory fitness with cardiovascular disease: a cohort and Mendelian randomisation study. British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2025-111351
Masmoum, M. D., Khan, S., Usmani, W. A., Chaudhry, R., Ray, R., Mahmood, A., Afzal, M., & Mirza, M. S. S. (2024). The Effectiveness of Exercise in Reducing Cardiovascular Risk Factors Among Adults: A Systematic Review and Meta-Analysis. Cureus, 16(9), e68928. https://doi.org/10.7759/cureus.68928
Isath, A., Koziol, K. J., Martinez, M. W., Garber, C. E., Martinez, M. N., Emery, M. S., Baggish, A. L., Naidu, S. S., Lavie, C. J., Arena, R., & Krittanawong, C. (2023). Exercise and cardiovascular health: A state-of-the-art review. Progress in Cardiovascular Diseases, 79, 44–52. https://doi.org/10.1016/j.pcad.2023.04.008
Paluch, A. E., Boyer, W. R., Franklin, B. A., Laddu, D., Lobelo, F., Lee, D., McDermott, M. M., Swift, D. L., Webel, A. R., & Lane, A. (2023). Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. https://doi.org/10.1161/CIR.0000000000001189
World Health Organization. (2024). Cardiovascular diseases (CVDs) fact sheet. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases
Roth, G. A., Mensah, G. A., Johnson, C. O., et al. (2020). Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. Journal of the American College of Cardiology, 76(25), 2982–3021. https://doi.org/10.1016/j.jacc.2020.11.010
University of Pittsburgh / Iowa State University / Harvard School of Public Health / NHLBI. Dose-Response to Resistance Exercise on Cardiovascular Health (ongoing clinical trial). ClinicalTrials.gov NCT06619444.
Guo, L., & Wang, C. (2025). The effect of exercise on cardiovascular disease risk factors in sedentary population: A systematic review and meta-analysis. Frontiers in Public Health, 13, 1470947. https://doi.org/10.3389/fpubh.2025.1470947
Zhuo, C., Zhao, J., Chen, M., & Lu, Y. (2021). Physical Activity and Risks of Cardiovascular Diseases: A Mendelian Randomization Study. Frontiers in Cardiovascular Medicine. https://doi.org/10.3389/fcvm.2021.722154
Sun, Y., & Liu, Y. (2025). Circulating Cytokines Mediate the Protective Effect of Physical Activity on Cardiovascular Diseases: A Mendelian Randomization Mediation Analysis. International Journal of Molecular Sciences. https://doi.org/10.3390/ijms26104615
Aengevaeren, V. L., et al. Exercise and Coronary Atherosclerosis: Observations, Explanations, and Clinical Implications. Circulation. https://doi.org/10.1161/CIRCULATIONAHA.119.044467
American Heart Association/American College of Cardiology. Multisociety guidelines on prevention of cardiovascular disease, hypertension management, and chronic coronary disease management (Class 1 recommendation for physical activity).
Polyak, A., et al. (2026). Physical Activity and Cardiovascular Health. Journal of Diabetes Research. https://doi.org/10.1155/jdr/3341765
Preventive Effects of Physical Activity on the Development of Atherosclerosis: A Narrative Review (2024–2025). PMC11706969.
Physical Activity, Immune System, and the Microbiome in Cardiovascular Disease. PMC6036301.
Exercise, Cardiovascular Health, and Risk Factors for Atherosclerosis: A Narrative Review on These Complex Relationships and Caveats of Literature. PMC7411151.
American College of Sports Medicine. ACSM Guidelines for Exercise Testing and Prescription (current edition) — general aerobic and resistance training dosing recommendations.