How Exercise Lowers LDL and Raises HDL: A Science-Backed Plan for Heart Health
Lower LDL and raise HDL in 12 weeks? Discover the 2025 science behind aerobic exercise, strength training, and HIIT for heart health
EXERCISEMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/12/202621 min read

Can exercise lower cholesterol? Yes. 2025 meta-analyses show structured exercise lowers LDL cholesterol 5–10%, raises HDL 3–9%, and reduces triglycerides up to 20% in 8–12 weeks. Aerobic training clears triglycerides, resistance training raises HDL, and HIIT delivers rapid LDL improvements. Benefits occur even without weight loss.
Key Scientific Points: Exercise and Cholesterol Modulation
1. Multi-Modal Lipid Reductions: Structured aerobic, resistance, and high-intensity interval training (HIIT) elicit mean LDL-C reductions of 5–10%, HDL-C increases of 3–9%, and triglyceride drops of 5–20% based on baseline profiles.
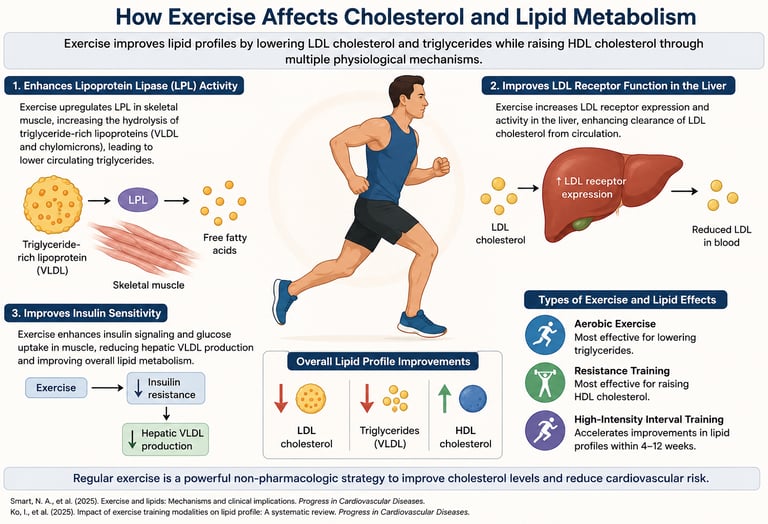
2. Triple Cellular Clearance Pathways: Exercise optimizes your lipid profile via three distinct mechanisms: it upregulates lipoprotein lipase (LPL) for post-meal fat clearance, increases hepatic LDL receptor expression to pull bad cholesterol from the blood, and boosts insulin sensitivity to halt VLDL overproduction.
3. High-Intensity Lifting for Better HDL: Resistance training intensity is a critical driver of "good" cholesterol; heavy lifting protocols (70–85% 1RM) trigger significantly greater HDL-C elevations (5–9%) and LDL-C reductions (5–8%) compared to light-weight training.
4. Rapid Metabolic Benefits via HIIT: High-intensity interval training forces rapid temporal adaptations, driving measurable reductions in LDL-C within just 4–6 weeks and cutting triglycerides by 10–15% through enhanced metabolic flexibility.
5. Weight-Loss Independent Remodeling: In adults with overweight or obesity, aerobic exercise yields a 7–12% drop in LDL-C and a 10–20% drop in triglycerides without requiring body mass reduction, proving that exercise directly remodels liver and muscle tissue.
6. Additive Power of Concurrent Training: You don't have to choose between cardio and weights; combining aerobic and resistance training into a concurrent protocol targets complementary biological pathways to produce superior, comprehensive lipid improvements.
7. Acute vs. Chronic Results Timelines: While a single workout clears triglycerides acutely within hours, true structural adaptations to your total cholesterol and LDL-C require a consistent training stimulus for 8–12 weeks before showing up on laboratory blood tests.
8. The "Exercise Snack" Revolution: Landmark 2026 systematic review data confirms that brief, fragmented, low-to-moderate intensity "exercise snacks" spread throughout the day meaningfully improve lipid and glucose metabolism, officially debunking the myth that workouts must be long to be effective.
Introduction: Exercise Is Cholesterol Medicine — Here Is the Proof
If your doctor handed you a prescription that could lower your LDL (bad) cholesterol by up to 10%, raise your HDL (good) cholesterol by up to 9%, and slash your triglycerides by up to 20% — all without a single side effect — would you take it? That prescription exists. It is called structured exercise.
For decades, cholesterol management has been framed almost exclusively around diet and statins. Yet a rapidly expanding body of high-quality research — including several landmark meta-analyses published in 2025 — now makes one point unmistakably clear: exercise is not merely a lifestyle add-on. It is a direct, powerful modifier of blood lipid metabolism with effects that rival pharmacological interventions in many populations.
This guide explains exactly how different types of exercise change your cholesterol and triglycerides at the molecular level, what the latest 2025 research tells us, and how you can design a practical, week-by-week plan to see measurable improvements in your lipid panel within 8–12 weeks.
In this article, you will learn:
How aerobic exercise, strength training, and HIIT each work through distinct biological pathways to improve your lipid profile
What the most recent 2025 meta-analyses actually found — and what the numbers mean for you
Why people with overweight or obesity often see even greater improvements than lean individuals
A science-backed 12-week exercise prescription, broken down week by week
Common myths that may be sabotaging your progress
Answers to the most frequently searched questions about exercise and cholesterol
What Are Blood Lipids? A Quick Primer
Here is the breakdown of your lipid panel, what the numbers mean, and why they matter for your heart health:
LDL Cholesterol ("Bad" Cholesterol):
Optimal Level: Less than 100 mg/dL
Why It Matters: LDL deposits directly into your artery walls, serving as the primary driver of plaque buildup (atherosclerosis).
The Exercise Advantage: Even a modest exercise-induced LDL reduction of 5–10% translates into a clinically meaningful reduction in atherosclerotic cardiovascular disease (ASCVD) risk.
HDL Cholesterol ("Good" Cholesterol):
Optimal Level: Greater than 60 mg/dL
Why It Matters: HDL acts as a clean-up crew, removing excess cholesterol from your arteries. Small increases in HDL improve "reverse cholesterol transport"—the exact process your body uses to clear plaque-forming cholesterol from artery walls and send it back to the liver.
Triglycerides (Blood Fats):
Optimal Level: Less than 150 mg/dL
Why It Matters: These are the most common type of fat in your body, used for energy. However, chronically elevated levels harden your arteries and significantly raise your overall heart risk.
Total Cholesterol (The Broad Overview):
Optimal Level: Less than 200 mg/dL
Why It Matters: This is the total amount of cholesterol found in your blood, representing the sum of your LDL, HDL, and VLDL fractions. It serves as a broad, high-level indicator of cardiovascular risk.
Non-HDL Cholesterol (The Emerging Marker):
Optimal Level: Less than 130 mg/dL
Why It Matters: Calculated simply as your Total Cholesterol minus your HDL. It accounts for all atherogenic (plaque-forming) particles in your blood, making it more predictive of heart disease than measuring LDL alone.
ApoB (The Particle Count Proxy):
Optimal Level: Less than 90 mg/dL
Why It Matters: Apolipoprotein B (ApoB) measures the actual number of plaque-carrying particles rather than just the amount of cholesterol inside them. Clinical data highlights it as the single best predictor of actual plaque-forming potential.
The Science: How Exercise Changes Your Cholesterol at the Molecular Level
Understanding why exercise works helps you understand why consistency and exercise type both matter. The lipid-improving effects of physical activity operate through three distinct but interconnected biological pathways.
1. Lipoprotein Lipase (LPL) Upregulation — The Clean-Up Crew Effect
Every time you exercise, your skeletal muscles release signals that dramatically increase the activity of an enzyme called Lipoprotein Lipase (LPL). Think of LPL as the janitor of your bloodstream: it sits on the walls of capillaries, intercepts fat-laden particles (called chylomicrons and VLDL) flowing by, and disassembles them — pulling the triglycerides out and channeling them into your muscles to be burned as fuel.
The result? Fewer triglycerides circulate in your blood, and fewer VLDL particles are available to be converted into LDL. This is why aerobic exercise is particularly effective at clearing post-meal fat from the bloodstream. A single 30-minute brisk walk after a high-fat meal can measurably reduce the post-prandial (after-meal) triglyceride spike — one of the fastest cardiovascular benefits available from any lifestyle intervention.
Post-meal triglycerides are acutely sensitive to aerobic activity. A 30-minute walk after dinner accelerates triglyceride clearance and is one of the fastest daily heart-protection strategies available — no equipment required.
2. Hepatic LDL Receptor Sensitivity — The Factory Floor Upgrade
Exercise appears to enhance both the number and efficiency of LDL receptors on liver cells. These receptors act like docking ports: the more functional ones you have, the more efficiently your liver can capture and remove LDL particles from the bloodstream. Even a modest increase in receptor expression can produce a clinically measurable reduction in circulating LDL cholesterol.
This is analogous to adding more checkout lanes at a supermarket — the line (LDL in your blood) clears faster because there are more processing points available.
3. Insulin-Lipid Crosstalk — The Metabolic Feedback Loop
Exercise powerfully improves insulin sensitivity, primarily by increasing GLUT4 transporter activity in muscle cells — meaning your muscles absorb blood glucose more efficiently. This has a direct downstream effect on your liver.
When insulin works effectively, it suppresses the liver's overproduction of Very-Low-Density Lipoprotein (VLDL) — the precursor to LDL. Chronically elevated insulin (common in metabolic syndrome and type 2 diabetes) drives excess VLDL production, flooding the bloodstream with the raw material that becomes LDL. Exercise breaks this cycle by restoring insulin sensitivity, thereby reducing the liver's output of atherogenic particles.
What the 2025 Research Actually Shows
The evidence base has grown substantially in recent years. Here is a summary of the most important studies, what they found, and what those findings mean for your training approach
Smart et al. (2025) — The Gold Standard Meta-Analysis
Published in Sports Medicine, this landmark systematic review of randomized controlled trials (RCTs) serves as the definitive benchmark for exercise and blood lipids:
LDL Cholesterol: Decreased by 5% to 10%, leading to a highly meaningful reduction in overall ASCVD risk.
HDL Cholesterol: Increased by 3% to 7%, actively improving reverse cholesterol transport to clear arterial plaque.
Triglycerides: Decreased by 5% to 15%, effectively shrinking the pool of harmful VLDL precursors.
Total Cholesterol: Dropped by an average of 5%, delivering broad cardiovascular protection.
Chen et al. (2025) — Overweight and Obese Populations
Published in Life, this systematic review examined aerobic exercise in adults with overweight or obesity, completely dismantling the "weight loss first" myth:
Greater Relative Gains: Individuals with overweight or obesity showed greater lipid improvements than normal-weight peers without needing to lose weight first.
The Metrics: LDL dropped 7–12%, triglycerides fell 10–20%, and HDL rose 5–9%.
The Takeaway: Your blood gets healthier before the scale moves. Metabolic adaptations in the liver and muscle tissue happen independently of body weight.
De Oude et al. (2025) — Resistance Training Intensity and Lipids
Published in the European Heart Journal Open, this systematic review proves that how heavy you lift directly dictates your lipid adaptations:
Intensity is King: High-intensity lifting (70–85% of 1RM) produces vastly superior HDL ("good") cholesterol improvements compared to low-intensity regimens.
The Metrics: Consistent lifting yielded a 5–8% reduction in LDL, while triglyceride drops remained modest (3–6%).
The Hybrid Advantage: Combining resistance and aerobic protocols produced additive, complementary health effects rather than redundant ones.
Ko et al. (2025) — High-Intensity Interval Training (HIIT)
Published in the Journal of Cardiovascular Development and Disease, this narrative review analyzed the efficiency of HIIT on heart health:
Rapid Adaptation: HIIT triggers metabolic improvements much faster than traditional, steady-state cardio, showing detectable LDL drops in just 4–6 weeks.
The Metrics: Consistently drives a 10–15% reduction in triglycerides while matching the HDL-boosting benefits of longer cardio sessions in a fraction of the time.
Peng et al. (2026) — Exercise Snacks: Short Bouts, Real Benefits
Published in Frontiers in Physiology, this fresh systematic review evaluated the impact of brief, fragmented movement throughout the day for sedentary adults:
The Takeaway: Short "exercise snacks" (brief, low-to-moderate intensity movements) meaningfully improve both glucose and lipid metabolism.
Mindset Shift: This data firmly destroys the "all-or-nothing" mentality, proving that you do not need long, grueling gym sessions to protect your cardiovascular health.
Summary Master Table: Exercise Type vs. Lipid Outcomes
Aerobic Training (Moderate-Intensity):
Lipid Impact: Lowers LDL by 5–10%, raises HDL by 3–7%, and slashes triglycerides by 10–20%.
Timeline: Expect measurable results in 8–12 weeks.
Resistance Training (Strength):
Lipid Impact: Reduces LDL by 5–8% and cuts triglycerides by 3–6%. Crucially, it boosts HDL by 5–9%, provided you train at a higher intensity (70–85% of your 1-Rep Max).
Timeline: Requires 8–12 weeks of consistent lifting.
HIIT (High-Intensity Interval Training):
Lipid Impact: Drops LDL by 5–10%, increases HDL by 3–7%, and reduces triglycerides by 10–15%.
Timeline: The fastest-acting modality, with adaptations visible in just 4–6 weeks.
Combined / Concurrent Training (Cardio + Weights):
Lipid Impact: The most effective all-around strategy. It yields a 7–12% drop in LDL, a 5–9% increase in HDL, and a 10–20% plunge in triglycerides.
Timeline: Takes 8–12 weeks for full laboratory detection.
Exercise Snacks (Brief, Fragmented Bouts):
Lipid Impact: Delivers meaningful, bite-sized improvements by nudging LDL down by 2–5%, raising HDL by 1–4%, and lowering triglycerides by 5–10%.
Timeline: Cumulative benefits become clear within 6–10 weeks.
⚠️ Note: Individual results vary based on your baseline lipid levels, genetics, diet, and training adherence.
The Three Pillars of Lipid-Lowering Exercise
Pillar 1: Aerobic Exercise — The Triglyceride Terminator
The Focus: Activities like walking, jogging, cycling, swimming, and rowing.
Primary Mechanism: Upregulates lipoprotein lipase (LPL), which accelerates the breakdown and clearance of triglyceride-rich particles from your blood after meals.
Weekly Prescription: 150–300 minutes per week of moderate-intensity activity (roughly 50–70% of your maximum heart rate), which can be broken down into shorter, bite-sized daily sessions.
Target Protocols:
Brisk Walking: Moderate intensity, 30–60 minutes per session, 5 days per week.
Jogging / Running: Moderate-to-vigorous intensity, 20–40 minutes per session, 3–5 days per week.
Cycling (Outdoor/Stationary): Moderate intensity, 30–60 minutes per session, 3–5 days per week.
Swimming: Moderate-to-vigorous intensity, 30–45 minutes per session, 3–4 days per week.
Rowing: Vigorous intensity, 20–30 minutes per session, 3 days per week.
Pillar 2: Resistance Training — The HDL Builder
The Focus: Progressive strength training to optimize "good" HDL cholesterol.
Primary Mechanism: Boosts insulin sensitivity, alters HDL particle composition, and reduces liver VLDL production via superior glucose regulation.
The Intensity Rule (70–85% 1RM): Intensity is critical. You must lift a weight heavy enough to cause muscular fatigue within 8–12 repetitions. If you can easily complete 15–20 reps, the weight is too light to trigger maximum HDL improvements.
Recommended Strength Plan:
Frequency: 2–3 sessions per week, allowing at least 48 hours of recovery for the same muscle groups.
Exercise Selection: Prioritize compound movements that recruit large muscle masses (e.g., squats, deadlifts, bench press, rows, overhead press, lunges).
Volume: Perform 3–4 sets of 8–12 repetitions at 70–85% of your 1-Rep Max (1RM).
Progression: Gradually increase the weight every 1–2 weeks to maintain the required intensity stimulus.
Safety: Always begin with a 5–10 minute warm-up featuring light cardio and dynamic stretching.
Pillar 3: HIIT — The Time-Efficient Lipid Transformer
The Focus: Alternating short bursts of near-maximal effort with brief recovery periods.
Primary Mechanism: Accelerates liver lipid turnover and enhances metabolic flexibility (the body's ability to seamlessly switch between burning carbs and fats), improving VLDL production and LDL particle composition.
The Efficiency Edge: Fastest-acting modality for busy schedules, producing detectable LDL reductions within just 4–6 weeks.
Beginner HIIT Protocol (20–25 Mins Total):
Warm-up: 5 minutes of brisk walking.
Work Interval: 30 seconds of fast jogging or cycling at near-maximal effort.
Rest Interval: 90 seconds of slow walking or complete rest.
Volume: Repeat for 8–10 total cycles.
Cool-down: 5 minutes of slow walking.
Frequency: 2–3 sessions per week on non-consecutive days.
Medical Note: HIIT is not recommended for individuals with uncontrolled cardiovascular disease; always consult a physician before starting.
The Power of Concurrent Training: 1 + 1 = 3
The Strategy: Combining aerobic and resistance training within the same weekly program.
The Additive Effect: Because cardio and weights operate through entirely different, independent biological pathways, their lipid-clearing benefits are complementary rather than redundant.
The Medication Analogy: Think of concurrent training like combination pharmacotherapy—instead of using one drug to hit a single target, you deploy multiple agents to address several cardiovascular mechanisms simultaneously.
The Ultimate Result: Yields a far more comprehensive, all-in-one lipid panel improvement (simultaneously lowering LDL, slashing triglycerides, and elevating HDL) than any single workout modality can achieve on its own.
Your 12-Week Exercise Plan to Improve Cholesterol
This plan integrates all three modalities — aerobic, resistance, and HIIT — in a progressive structure designed to maximize lipid improvements within 12 weeks. It is built for beginners to intermediate exercisers. Always consult your physician before starting a new exercise program, especially if you have known cardiovascular disease, uncontrolled hypertension, or diabetes.
Before You Start: Safety Checklist
Consult your physician if you have cardiovascular disease, uncontrolled high blood pressure, or diabetes
Get a baseline lipid panel before starting — you will want a comparison at Week 12
Invest in a comfortable pair of supportive athletic shoes
Start slower than you think you need to — consistency over the full 12 weeks matters more than intensity in Week 1
Stay hydrated and aim for 7–9 hours of sleep per night to support metabolic adaptatio
Phase 1: Foundation Building (Weeks 1–4)
Primary Goals: Establish a consistent movement habit, build a baseline aerobic foundation, and safely introduce light resistance training.
Weekly Schedule Breakdown:
Monday (Aerobic Foundation): 30 minutes of brisk walking at a moderate intensity (comfortable enough to hold a conversation).
Tuesday (Introductory Strength): Full-body resistance training consisting of 3 sets of 12 repetitions across 5 different exercises, utilizing a light-to-moderate load (60–65% 1RM).
Wednesday (Recovery): Full rest or 20–30 minutes of gentle yoga and light stretching.
Thursday (Active Cardio): 30–40 minutes of brisk walking or light cycling at a steady, moderate pace.
Friday (Strength Consistency): Repeat the full-body resistance training protocol with 3 sets of 12 repetitions across 5 exercises at 60–65% 1RM.
Saturday (Endurance & Recreation): A longer, continuous walk or low-stress recreational activity lasting 45–60 minutes at a light-to-moderate intensity.
Sunday (Rest): Complete rest to allow the body to adapt and recover.
Phase 2: Progressive Overload (Weeks 5–8)
Primary Goals: Increase overall aerobic volume, intentionally raise resistance training intensity to stimulate HDL creation, and safely introduce interval work.
Weekly Schedule Breakdown:
Monday (HIIT Introduction): 20–25 minutes total of running or cycling intervals, pushing to near-maximal effort during the work periods.
Tuesday (Progression Strength): Focused weight training utilizing heavier loads; 4 sets of 10 repetitions across 6 different exercises at 70–75% 1RM.
Wednesday (Steady Cardio): 35–45 minutes of moderate-to-vigorous cycling or swimming to drive metabolic flexibility.
Thursday (Strength Volume): Second weekly weight training session; 4 sets of 10 repetitions across 6 exercises at 70–75% 1RM.
Friday (Hybrid Cardio): 25–30 minutes of high-intensity movement, alternating weekly between a HIIT session and a steady aerobic workout.
Saturday (Extended Aerobic): A dedicated, long aerobic session consisting of 45–60 minutes of continuous cardio at a moderate intensity.
Sunday (Active Recovery): 20–30 minutes of a light walk or deep stretching to flush the muscles.
Phase 3: Lipid Optimization (Weeks 9–12)
Primary Goals: Peak the cumulative training stimulus, consolidate your physiological gains, and maximize cellular changes in preparation for a follow-up lipid blood panel.
Weekly Schedule Breakdown:
Monday (Advanced HIIT): 25–30 minutes of cycling or rowing intervals, aggressively pushing your cardiovascular system to 85–90% of your maximum heart rate during work phases.
Tuesday (Peak Strength): Heavy resistance training optimized for maximum HDL response; 4 sets of 8 repetitions across 6–7 compound exercises at 75–85% 1RM.
Wednesday (Vigorous Cardio): 40–50 minutes of continuous running, swimming, or cycling performed at a challenging, moderate-to-vigorous pace.
Thursday (Peak Strength): Second heavy lifting session of the week; 4 sets of 8 repetitions across 6–7 compound exercises at 75–85% 1RM.
Friday (Tempo Workout): 25–35 minutes of high-intensity interval training or a sustained high-effort tempo cardio session.
Saturday (Max Endurance): A long, sustained aerobic session lasting 50–60 minutes at a steady, moderate pace to empty glycogen stores.
Sunday (Rest): Complete rest or light active recovery to ensure a full system reboot before restarting the weekly cycle.
After Week 12: Retest Your Lipid Panel
Schedule a fasting lipid panel at the end of Week 12 — ideally 48–72 hours after your last exercise session. Compare your LDL, HDL, triglycerides, and total cholesterol to your baseline. Most people see measurable improvements. If you are also on statin therapy, share your results with your physician — some individuals can reduce their medication dose under supervision.
A Critical Truth: You Do Not Need to Lose Weight First
One of the most clinically important — and least widely communicated — findings from recent research is that exercise improves cholesterol independently of body weight changes.
The Chen et al. (2025) study demonstrated that overweight and obese individuals experienced LDL reductions of 7–12% and triglyceride reductions of 10–20% even without significant weight loss. The biological mechanisms — improved hepatic LDL receptor expression, enhanced LPL activity, and better insulin sensitivity — are adaptations within the liver and muscle tissue itself, not consequences of shrinking fat cells.
What does this mean practically? Do not wait until you have "lost enough weight" before prioritizing exercise for heart health. The metabolic remodeling begins with your first workout. Your blood is getting healthier even when the scale refuses to move.
The Scale Is Not the Story
Two patients can have identical body weights with vastly different lipid profiles — because one exercises and one does not. Body composition, metabolic health, and cardiovascular risk are shaped more powerfully by physical activity than by body weight alone. Exercise is metabolic medicine, not just a weight loss tool.
Common Myths and Mistakes That Undermine Your Results
Myth 1: "I need to exercise for at least 45 minutes for it to count."
False. The Peng et al. (2026) meta-analysis found that even short exercise snacks — fragmented bouts of activity throughout the day — meaningfully improve lipid and glucose metabolism in sedentary adults. Ten minutes of brisk walking three times a day produces real cardiovascular benefits. Start where you are.
Myth 2: "Cardio is all I need for cholesterol."
Incomplete. While aerobic exercise is excellent for triglycerides and LDL, resistance training is the superior modality for raising HDL — and higher-intensity lifting produces greater improvements than light loads. For a comprehensive lipid effect, you need both.
Myth 3: "I've been exercising for two weeks, and my labs haven't changed — it's not working."
Too soon. The physiological adaptations that produce measurable changes in LDL and total cholesterol require a minimum of 8–12 weeks of consistent stimulus. Triglycerides respond more quickly (sometimes within hours of a single session), but the full panel takes time. Your body is a large ship — it needs runway to turn.
Myth 4: "If I'm on a statin, exercise won't add much benefit."
Incorrect and potentially harmful to believe. Exercise and statins operate through complementary mechanisms. Statins primarily reduce hepatic cholesterol synthesis; exercise enhances LDL receptor activity, LPL function, and insulin sensitivity. Their effects are additive. Many patients on statins who adopt structured exercise see further improvements in their lipid panels — and some, under physician supervision, have been able to reduce their medication dose.
Myth 5: "HIIT is too intense for someone with high cholesterol."
Not necessarily. For most people without underlying cardiovascular disease, HIIT is safe and highly effective for rapid lipid improvement. However, anyone with known heart disease, uncontrolled hypertension, or significant arrhythmias should undergo a stress test and obtain physician clearance before beginning HIIT.
Myth 6: "Exercise alone will normalize my cholesterol."
It might — or it might not. While exercise produces clinically meaningful lipid improvements, the magnitude depends on your baseline levels, genetics (including familial hypercholesterolaemia), diet quality, and other lifestyle factors. Exercise is a powerful tool, not a guaranteed cure. For individuals with severely elevated LDL (> 190 mg/dL) or established cardiovascular disease, exercise should complement — not replace — pharmacological therapy.
Practical Checklists and Tools
Weekly Exercise Tracking Checklist
1. Log your activity: date, type, duration, and how you felt on a scale of 1–10
2. Check heart rate zones: use a fitness tracker or calculate manually (220 minus your age = estimated max heart rate)
3. Track progressive overload: note the weights used in resistance sessions and aim to increase them every 1–2 weeks
4. Schedule your post-meal 10–30 minute walk at least 3–5 times per week
5. Plan rest days: recovery is when the metabolic adaptations consolidate
6. Retest lipid panel at 12 weeks: fast for 9–12 hours before the blood draw
Nutrition Amplifiers: Enhance Your Exercise Results
Exercise works best when paired with supportive dietary habits. You do not need a perfect diet — but a few evidence-based adjustments can amplify your lipid improvements.
• Increase soluble fiber: Oats, barley, lentils, and beans bind LDL in the gut and reduce its absorption. Target 5–10g of soluble fiber per day.
• Reduce saturated fat: Replace butter, fatty red meat, and full-fat dairy with olive oil, fatty fish, and plant fats where possible. Even modest reductions amplify the LDL-lowering effects of exercise.
• Include omega-3 fatty acids: Salmon, sardines, mackerel, walnuts, and flaxseed reduce triglycerides. Target 2+ servings of fatty fish per week.
• Limit added sugar and refined carbohydrates: These are the primary dietary drivers of elevated triglycerides. Reducing sugar intake synergizes powerfully with exercise-induced triglyceride clearance.
• Stay hydrated: Adequate water intake supports exercise performance and metabolic function.
Frequently Asked Questions
Q: How quickly will I see changes in my cholesterol from exercise?
Triglycerides respond fastest — a single aerobic session can reduce post-meal triglycerides within hours. For LDL and total cholesterol, expect 8–12 weeks of consistent training before seeing laboratory-measurable changes. HDL improvements from resistance training typically appear within 8–10 weeks. Retest your full lipid panel after 12 weeks of consistent exercise for an accurate assessment.
Q: Is one type of exercise better for cholesterol than others?
No single modality dominates. Aerobic exercise best targets triglycerides and supports LDL reduction through LPL upregulation. Resistance training at higher intensities (70–85% of 1RM) most effectively raises HDL. HIIT produces rapid results across multiple markers with shorter time investment. For comprehensive benefits across your entire lipid panel, combine all three — concurrent training is the gold standard.
Q: Can exercise replace my cholesterol medication?
For some individuals with mild-to-moderate dyslipidaemia and no established cardiovascular disease, structured exercise — combined with dietary improvements — may normalize lipid levels without medication. However, never discontinue or reduce medications without explicit guidance from your physician. For individuals with familial hypercholesterolaemia, established atherosclerosis, or very high LDL levels, medication remains essential. Exercise and statins work synergistically — there is rarely a reason to choose one over the other.
Q: I have obesity — will exercise really help my cholesterol?
Absolutely — and possibly more dramatically than for lean individuals. The Chen et al. (2025) systematic review demonstrated LDL reductions of 7–12% and triglyceride reductions of 10–20% in overweight and obese participants — greater improvements than observed in normal-weight groups — and these benefits occurred independently of major weight loss. Start with low-impact aerobic activity (walking, cycling, swimming) and gradually progress.
Q: How much exercise do I need for meaningful cholesterol improvements?
Current evidence supports a minimum of 150 minutes of moderate-intensity aerobic exercise per week, combined with 2 resistance training sessions per week. The Smart et al. (2025) meta-analysis found meaningful lipid improvements with this level of activity. However, more is generally better — up to approximately 300 minutes of moderate aerobic exercise per week — within reason and without causing injury or burnout.
Q: Does walking count, or do I need to do more intense exercise?
Walking absolutely counts. Brisk walking (roughly 3–4 mph, enough to elevate your heart rate and breathing but still allow conversation) has been shown to produce meaningful improvements in triglycerides and modest improvements in LDL and HDL. The Peng et al. (2026) meta-analysis also confirmed that even short exercise snacks — 10-minute walks spread throughout the day — benefit lipid and glucose metabolism. Walking is an excellent starting point, especially after meals.
Q: Is HIIT safe if I have high cholesterol?
For most otherwise healthy adults, HIIT is safe and effective. However, if you have known coronary artery disease, uncontrolled hypertension (blood pressure above 160/100), significant arrhythmias, or have had a recent cardiac event, you should obtain physician clearance and potentially an exercise stress test before beginning HIIT. Start with aerobic base-building for 4–6 weeks before introducing high-intensity intervals.
Q: Will exercise improve my cholesterol if I do not change my diet?
Yes — exercise produces lipid improvements through mechanisms that are independent of diet. However, the combination of exercise and dietary improvement produces substantially greater benefits than either alone. If your diet is high in saturated fat and added sugars, you are working against the improvements exercise is generating. Pairing exercise with modest dietary adjustments (more fiber, less saturated fat, fewer refined carbohydrates) will maximize your lipid panel results.
Q: How long do I need to keep exercising to maintain my improved cholesterol?
The lipid benefits of exercise are not permanent without continued activity. Most studies show that cholesterol returns toward baseline within 4–8 weeks of exercise cessation. Exercise for heart health is a lifelong prescription, not a 12-week course. The good news: once you build the habit and experience the benefits, most people find it far easier to maintain than to start.
Q: Can I exercise too much and worsen my cholesterol?
Overtraining syndrome — which requires extreme volumes of exercise over extended periods — is associated with elevated inflammatory markers and potentially adverse hormonal changes. For the vast majority of people following the exercise volumes described in this guide, more exercise is not harmful to cholesterol. However, inadequate recovery time, poor sleep, and severe caloric restriction combined with high exercise volumes can impair the metabolic adaptations you are trying to achieve. Balance training with adequate rest and nutrition.
Q: Does the time of day I exercise affect cholesterol improvements?
The evidence here is less definitive. Post-meal exercise (within 30–60 minutes of eating) is particularly effective for clearing post-prandial triglycerides — a specific benefit of timing exercise after meals. Beyond this, the total volume and intensity of your training appear more important for long-term lipid changes than the specific time of day. Exercise at the time that best supports your consistency and adherence.
Conclusion: Exercise Is Not Optional for Heart Health
The science is clear and compelling. Structured exercise — when appropriately dosed by type, intensity, and frequency — is one of the most powerful tools available for optimizing your lipid profile and reducing cardiovascular risk. It is not a supplement to medication or a vague lifestyle recommendation. It is metabolic pharmacology.
The 2025 research tells us that:
• Aerobic exercise clears triglycerides and supports LDL reduction through LPL upregulation
• Resistance training at meaningful intensities raises HDL and improves insulin sensitivity
• HIIT produces rapid lipid improvements with time efficiency
• Combining all three modalities — concurrent training — produces additive, comprehensive benefits
• People with overweight or obesity often see the greatest improvements, independent of weight loss
• Measurable changes require 8–12 weeks of consistency — but the biology begins adapting from your very first session
Your action steps are straightforward: get a baseline lipid panel today, begin the 12-week plan outlined in this article, retest in 12 weeks, and work with your physician to interpret the results in the context of your full cardiovascular risk profile.
Exercise is arguably the most under-prescribed therapy in preventive cardiology. You now have the evidence and the plan. The rest is consistency.
Medical Disclaimer
This article is intended for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Patients with cardiovascular disease, diabetes, uncontrolled hypertension, or those currently taking lipid-lowering medications should consult their physician before modifying their exercise program or treatment plan.
Related Articles
Metabolic Plasticity: Epigenetic Adaptations to Calorie Restriction | DR T S DIDWAL
References and Further Reading
1. Smart, N. A., Downes, D., van der Touw, T., Hada, S., Dieberg, G., Pearson, M. J., Wolden, M., King, N., & Goodman, S. P. J. (2025). The effect of exercise training on blood lipids: A systematic review and meta-analysis. Sports Medicine, 55(1), 67–78. https://doi.org/10.1007/s40279-024-02115-z
2. Smart, N. A., Wood, G. N., Pearson, M. J., Dieberg, G., van der Touw, T., & Kostner, K. (2026). Exercise training for the management of dyslipidaemia: A position statement from Exercise and Sports Science Australia (ESSA). Journal of Science and Medicine in Sport, 29(4), 335–341. https://doi.org/10.1016/j.jsams.2025.11.004
3. Chen, Z., Zhou, R., Liu, X., Wang, J., Wang, L., Lv, Y., & Yu, L. (2025). Effects of aerobic exercise on blood lipids in people with overweight or obesity: A systematic review and meta-analysis of randomized controlled trials. Life (Basel), 15(2), 166. https://doi.org/10.3390/life15020166
4. De Oude, K. I., Elbers, R. G., Gerger, H., Maes-Festen, D. A. M., & Oppewal, A. (2025). The effect of different resistance exercise training intensities on cardiovascular risk factors: A systematic review and meta-analysis. European Heart Journal Open, 5(5), oeaf093. https://doi.org/10.1093/ehjopen/oeaf093
5. Ko, J.-M., So, W.-Y., & Park, S.-E. (2025). Narrative review of high-intensity interval training: Positive impacts on cardiovascular health and disease prevention. Journal of Cardiovascular Development and Disease, 12(4), 158. https://doi.org/10.3390/jcdd12040158
6. Peng, Z., Peng, L., Sun, W., Liu, X., Zhou, M., Chen, M., Ren, J., Chen, A., & Guo, C. (2026). Effectiveness of moderate-to-low intensity exercise snacks on glucose and lipid metabolism in sedentary adults: a systematic review and meta-analysis. Frontiers in Physiology, 17, 1805547. https://doi.org/10.3389/fphys.2026.1805547
7. Buzdagli, Y., Tekin, A., Eyipinar, C. D., Oget, F., & Siktar, E. (2022). The effect of different types of exercise on blood lipid profiles: A meta-analysis of randomized controlled studies. Science & Sports, 37(8), 675–687. https://doi.org/10.1016/j.scispo.2022.07.005
8. Mosteoru, S., Gaita, L., & Gaita, D. (2023). Sport as medicine for dyslipidemia (and other risk factors). Current Atherosclerosis Reports, 25, 613–617. https://doi.org/10.1007/s11883-023-01133-y
9. Ozdemir, F., Saglam, M., Uyaroglu, O. A., et al. (2025). Impact of physical activity, health literacy and cognitive health on quality of life in dyslipidemia: an observational study. Scientific Reports, 15, 35586. https://doi.org/10.1038/s41598-025-02223-4
10. Ouda, L. K. (2025). The impact of exercise on blood lipoprotein cholesterol profiles (LDL-HDL): Protecting against atherosclerosis. Journal of Applied Hematology, 16(3), 239–246. https://doi.org/10.4103/joah.joah_77_25
11. American Heart Association. Physical activity and your heart. https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults (external link suggestion)
12. National Lipid Association (2023). Recommendations for patient-centered management of dyslipidemia. Journal of Clinical Lipidology. (external link suggestion)
© Dr. T.S. Didwal, M.D. | Evidence-Based Health & Fitness Science | Updated June 2026