High Homocysteine Levels Explained: Causes, Risks, Symptoms & How to Lower Them
Discover what high homocysteine means for your heart, brain, and blood vessels. Learn the causes, symptoms, optimal levels, and evidence-based ways to lower homocysteine naturally.
NUTRITIONHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/4/202621 min read
High homocysteine (hyperhomocysteinemia) is a blood marker >15 μmol/L linked to increased risk of heart attack, stroke, and cognitive decline. It occurs when your body can’t properly clear homocysteine, usually due to deficiencies in folate (B9), vitamin B12, or B6
Key takeaways
1. Homocysteine is a hidden but modifiable risk to the heart, brain, and kidneys
Elevated levels >15 μmol/L are an independent risk factor for heart attack, stroke, cognitive decline, and vascular damage — even when cholesterol and blood pressure are normal. The damage happens through endothelial dysfunction, oxidative stress, and increased clotting.
2. Optimal is <10 μmol/L, not just “normal”
Lab ranges call 5–15 μmol/L “normal,” but the lowest risk is <7–10 μmol/L.
Mild elevation: 15–30 μmol/L = elevated risk
Moderate: 30–100 μmol/L = high risk
Severe: >100 μmol/L = very high risk, urgent medical care
3. B-vitamin deficiencies are the #1 fixable cause
Your body clears homocysteine using folate (B9), B12, and B6. Deficiency in any one drives levels up. Most powerful combo = methylfolate + methylcobalamin B12 + P5P B6. The 2025 meta-analysis found combined B vitamins beat single nutrients.
4. Your risk profile matters: genetics + age + lifestyle
Highest risk groups: men 65+, vegans/vegetarians, people with the MTHFR C677T gene variant, CKD patients, metformin or PPI users, heavy smokers/drinkers, and postmenopausal women. Men have higher levels than women at all ages.
5. MTHFR gene variants are common but not destiny
Up to 40% of people have reduced MTHFR enzyme function. If you have the C677T variant, standard folic acid may not work well — use methylfolate (5-MTHF) + riboflavin (B2) instead. Genetics + nutrition together determine your levels.
6. Diet + lifestyle changes work within weeks
Top evidence-based moves:
5+ servings of dark leafy greens daily for folate
B12 from meat/fish/eggs or supplements if vegan, 60+, or on metformin
Mediterranean-style diet
Quit smoking, limit alcohol, + excessive coffee
150 min/week aerobic exercise
Levels can drop measurably in 4–6 weeks if deficiency-driven.
7. It affects more than your heart
High homocysteine is linked to stroke + cerebral small vessel disease, dementia/Alzheimer’s, recurrent pregnancy loss + preeclampsia, PCOS, kidney disease progression, bone fractures, and depression via neurotransmitter disruption.
8. Testing and treating should be targeted, not universal
Key nuance: Large trials show lowering homocysteine with B vitamins doesn’t always prevent heart attacks in unselected people. Current consensus = precision approach. Test if you have risk factors, family history of early CVD, recurrent miscarriage, suspected B12 deficiency, CKD, or unexplained cognitive decline. Work with your doctor — don’t self-treat high doses.
Bottom line: Homocysteine is one of the few CV risk markers that’s both predictive and directly modifiable with nutrition. Get tested, know your B-vitamin status, and aim for <10 μmol/L if you have risk factors.
For decades, heart health conversations have focused on cholesterol, blood pressure, blood sugar, and smoking. While these factors remain critically important, researchers have increasingly identified another blood marker that may quietly influence cardiovascular and brain health: homocysteine. Unlike cholesterol, homocysteine is rarely discussed outside specialist clinics, yet growing evidence suggests that elevated levels may contribute to blood vessel damage, stroke, cognitive decline, and other chronic diseases (D'Elia et al., 2025; Smith & Refsum, 2021).
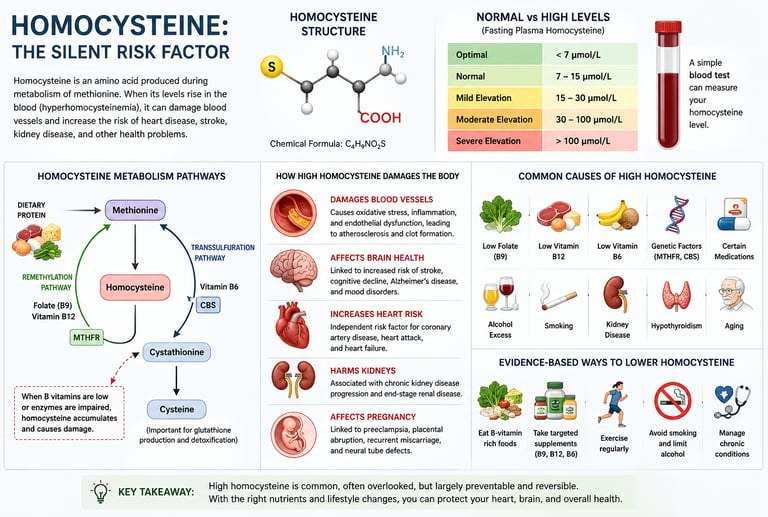
Homocysteine is a naturally occurring amino acid produced when the body metabolizes methionine, a protein-building block found in foods such as meat, eggs, fish, and dairy. Under normal circumstances, the body rapidly recycles homocysteine using vitamins B12, B6, and folate (vitamin B9). However, when this process becomes impaired—because of nutritional deficiencies, genetic variations such as MTHFR mutations, kidney disease, certain medications, or lifestyle factors—homocysteine can accumulate in the bloodstream (Cao et al., 2025).
Why does this matter? Elevated homocysteine has been linked to endothelial dysfunction, oxidative stress, inflammation, and abnormal blood clotting, all of which can accelerate vascular damage and increase the risk of heart attack and stroke (D'Elia et al., 2025; Splaver et al., 2004). Research also suggests that high homocysteine may affect brain health, contributing to cognitive decline, dementia, and cerebral small vessel disease (Huang et al., 2026; Smith & Refsum, 2021).
The encouraging news is that homocysteine is one of the few cardiovascular risk markers that is often measurable, modifiable, and responsive to targeted nutritional interventions. In many individuals, correcting deficiencies of folate, vitamin B12, or vitamin B6 can substantially reduce elevated levels within weeks (Liu et al., 2025).
In this evidence-based guide, you'll learn what homocysteine is, why it rises, how it affects your heart and brain, who is most at risk, and the practical steps you can take to keep your levels in a healthier range.
What Is Homocysteine?
Homocysteine is a sulfur-containing amino acid produced naturally in the body as a byproduct of metabolising methionine — an essential amino acid found in protein-rich foods like meat, eggs, and dairy. Unlike methionine itself, homocysteine does not come from your diet directly. Your body creates it internally every time it processes protein.
Under normal, healthy conditions, homocysteine doesn't stick around for long. Your body rapidly converts it back into useful compounds through two main pathways:
Remethylation pathway: Homocysteine is converted back to methionine, requiring folate (vitamin B9) and vitamin B12 as essential cofactors.
Transsulfuration pathway: Homocysteine is converted to cystathionine and then to cysteine — an antioxidant compound — requiring vitamin B6.
When these pathways work efficiently, homocysteine levels stay low. Problems arise when they don't.
The enzyme methylenetetrahydrofolate reductase (MTHFR) plays a pivotal role here. Mutations in the MTHFR gene — which are surprisingly common, affecting up to 40% of the population to varying degrees — can impair remethylation efficiency, allowing homocysteine to accumulate. A 2025 review in Molecular and Cellular Biochemistry confirmed that mutations in MTHFR and another key enzyme, cystathionine beta synthase (CBS), "underlie the pathogenesis of hyperhomocysteinemia."
Normal vs. High Homocysteine Levels: What the Numbers Mean
A simple blood test — usually a fasting plasma homocysteine measurement — tells you where you stand. Results are reported in micromoles per litre (μmol/L).
Here is the breakdown of the homocysteine classification levels, risk statuses, and required actions:
Optimal
Level: Less than 7 μmol/L
Risk Status: Lowest Risk
Action Needed: Maintain current habits
Normal
Level: 5 to 15 μmol/L
Risk Status: Acceptable
Action Needed: Monitor annually
Mild Elevation
Level: 15 to 30 μmol/L
Risk Status: Elevated Risk
Action Needed: Dietary and lifestyle changes
Moderate Elevation
Level: 30 to 100 μmol/L
Risk Status: High Risk
Action Needed: Medical evaluation and supplementation
Severe (Homocystinuria)
Level: Greater than 100 μmol/L
Risk Status: Very High Risk
Action Needed: Urgent medical managementThe condition of persistently elevated homocysteine — typically defined as levels exceeding 15 μmol/L — is called hyperhomocysteinemia (HHcy). It affects an estimated 5–10% of the general population, though rates are significantly higher in older adults and those with poor nutritional status.
Important Gender & Age Differences
Homocysteine levels are not the same across all people. A large 2020 cross-sectional study of the Chinese general population published in Scientific Reports (Xu et al.) found that:
Men consistently have higher homocysteine levels than women across all age groups
Levels rise significantly with age in both sexes
Postmenopausal women see a notable jump in levels — converging closer to male levels — suggesting a protective role of estrogen
This means that a "normal" reading for a 65-year-old man is not the same as for a 30-year-old woman. Your doctor should interpret your results in this context.
What Causes High Homocysteine? A Comprehensive Look
Homocysteine rises when its normal metabolic clearance is disrupted. The causes span genetics, nutrition, lifestyle, medications, and underlying disease.
Nutritional Deficiencies (The #1 Modifiable Cause)
Because three B vitamins — folate (B9), B12, and B6 — are indispensable cofactors in homocysteine metabolism, deficiencies in any of them can cause levels to climb rapidly. This is the most common and most correctable cause.
Folate deficiency: Most powerfully associated with elevated homocysteine. Found in people with poor vegetable intake or malabsorption disorders.
Vitamin B12 deficiency: Critically important — and frequently overlooked. Vegans, older adults (who produce less intrinsic factor), and those taking metformin or proton pump inhibitors are particularly vulnerable.
Vitamin B6 deficiency: Less common but contributes, especially to post-methionine-load homocysteine elevation.
Riboflavin (B2) deficiency impairs MTHFR enzyme function, especially in those with the MTHFR C677T genetic variant.
Genetic Factors: MTHFR & CBS Mutations
The MTHFR gene variant C677T is the most clinically relevant genetic cause of elevated homocysteine. People who are homozygous for this variant (carrying two copies) may have substantially reduced enzyme activity and higher baseline levels, especially when folate intake is low. A 2025 review in the Journal of Cardiovascular Development and Disease highlights that genetic variants should be evaluated alongside nutritional status — not in isolation — for meaningful clinical interpretation.
Kidney Function
The kidneys play a major role in clearing homocysteine. Chronic kidney disease (CKD) is one of the strongest secondary causes of high homocysteine — nearly all patients with advanced CKD have elevated levels, often dramatically so. Even modest reductions in kidney function can measurably elevate plasma homocysteine.
Medications That Raise Homocysteine
Here is the breakdown of medications that influence folate, B12, or the methionine cycle, along with their mechanisms and clinical management strategies:
Metformin (Diabetes Drug)
Mechanism: Impairs Vitamin B12 absorption.
Clinical Implication: Monitor B12 levels annually.
Proton Pump Inhibitors (PPIs)
Mechanism: Reduce gastric acid production, which leads to Vitamin B12 malabsorption.
Clinical Implication: Consider B12 supplementation if used long-term.
Methotrexate
Mechanism: Acts as a folate antagonist, inhibiting necessary enzyme pathways.
Clinical Implication: Folate supplementation is typically prescribed alongside treatment to mitigate toxicity.
Phenytoin & Carbamazepine
Mechanism: Interfere with hepatic folate metabolism and deplete systemic stores.
Clinical Implication: Monitor plasma homocysteine levels in long-term users.
High-Dose Niacin
Mechanism: Exerts a direct effect on the methionine cycle, increasing consumption of methyl donors.
Clinical Implication: Titrate to the lowest effective dose to prevent elevation of downstream metabolites.Lifestyle Factors
Smoking: Disrupts B-vitamin metabolism and directly elevates homocysteine
Heavy alcohol consumption: Impairs folate absorption and increases folate excretion
Physical inactivity: Associated with modestly higher levels
High protein intake without adequate B vitamins: More methionine means more homocysteine substrate — requires proportionally more B vitamins to clear it
Excessive coffee consumption: Several studies link very high coffee intake (>4 cups/day) to modestly elevated levels
How Elevated Homocysteine Damages Your Body: The Mechanisms
Understanding how homocysteine causes harm is key to understanding why lowering it matters. Research has identified several well-characterised pathological mechanisms.
1. Endothelial Dysfunction
The endothelium — the single-cell lining of every blood vessel — is exceptionally sensitive to homocysteine. Elevated levels reduce the bioavailability of nitric oxide (NO), a critical vasodilator that keeps blood vessels flexible and prevents platelets from clumping. This leads to arterial stiffness, impaired blood flow, and the earliest stages of atherosclerosis.
2. Oxidative Stress
Homocysteine is readily oxidised in plasma, generating reactive oxygen species (ROS) including hydrogen peroxide and superoxide. This oxidative stress damages lipids, proteins, and DNA — contributing to chronic inflammation throughout the cardiovascular system.
3. Prothrombotic Effects
High homocysteine activates platelets and interferes with natural anticoagulant mechanisms, including protein C and thrombomodulin pathways. The net result is a blood environment that clots more readily — dramatically increasing the risk of thrombotic events like heart attacks and strokes.
4. Epigenetic Disruption
Homocysteine interferes with DNA methylation — a fundamental epigenetic process that regulates which genes are expressed. Disrupted methylation patterns can promote inflammation, accelerate cellular ageing, and may contribute to neurodegeneration. This is an emerging area of active research as of 2025–2026.
Homocysteine & Heart Disease: The Evidence
The cardiovascular link is where homocysteine research has the deepest roots. Cardiologist Kilmer McCully first proposed the homocysteine-heart disease connection in 1969 — a theory initially dismissed by the medical establishment, then vindicated by decades of epidemiological data.
2× Increased risk of coronary artery disease at levels >15 μmol/L
25% Rise in cardiovascular risk per 5 μmol/L increase in homocysteine
3–4× Greater stroke risk in patients with moderate-to-severe hyperhomocysteinemia
A 2025 review in the Journal of Cardiovascular Development and Disease synthesised decades of research, confirming that elevated homocysteine is "a reproducible biomarker of cardiovascular risk" and that its pathophysiological mechanisms — endothelial damage, atherosclerosis progression, and prothrombotic effects — are well-supported by both in vitro and animal model evidence.
Homocysteine & Hypertension: A Bidirectional Relationship
A 2025 study in Hypertension Research (Wang et al.) examined plasma homocysteine specifically in patients with essential hypertension and found a significant association between elevated homocysteine and morning blood pressure surge — the dangerous early-morning spike in blood pressure that is strongly predictive of cardiovascular events. Patients with both hypertension and elevated homocysteine (a condition sometimes called "H-type hypertension") face compounded risk.
This combination is particularly common in China, where MTHFR variants are prevalent and folate intake has historically been lower than in Western populations where bread is fortified.
⚠️ Clinical Caution
While the epidemiological link between homocysteine and cardiovascular events is strong, large randomised trials (HOPE-2, SEARCH, VISP) have shown that lowering homocysteine with B vitamins does not always reduce cardiovascular event rates in unselected populations. The current scientific consensus supports a precision medicine approach — targeting high-risk subgroups. Talk to your doctor about your individual risk profile.
Stroke, Brain Health & Cognitive Decline
The brain is exquisitely sensitive to homocysteine's damaging effects. Research linking elevated homocysteine to neurological outcomes has exploded over the past decade, particularly in three areas: stroke, cerebral small vessel disease, and dementia.
Homocysteine & Stroke: 30 Years of Evidence
A landmark 2025 bibliometric analysis in the Journal of Mind and Medical Sciences (Wei et al.) examined 30 years of published research on homocysteine and stroke. Their analysis confirmed that homocysteine research in stroke has accelerated dramatically since 2015, with oxidative stress, inflammation, and thrombosis emerging as the dominant mechanistic themes.
Homocysteine promotes stroke through multiple routes: it stiffens arterial walls, promotes clot formation in cerebral arteries, and may directly damage the blood-brain barrier — allowing neurotoxic substances to reach sensitive brain tissue.
Cerebral Small Vessel Disease in Diabetics
A 2026 study in Frontiers in Endocrinology (Huang et al.) specifically investigated the connection between homocysteine and cerebral small vessel disease (CSVD) burden in patients with type 2 diabetes. Their findings revealed a significant association between higher homocysteine levels and more severe CSVD — a condition characterised by silent white matter lesions, lacunar infarcts, and microbleeds that silently erode cognitive function over years.
This is especially important because people with type 2 diabetes are already at elevated risk for cerebrovascular disease. Elevated homocysteine in this population represents a "double hit" to brain vasculature.
Dementia & Cognitive Decline
Dr. A. David Smith and Professor Helga Refsum — two of the world's foremost homocysteine researchers at Oxford and Oslo universities — published a landmark review in the Journal of Internal Medicine (2021) reviewing decades of evidence. They concluded that elevated homocysteine is "not just a biomarker but a potentially modifiable causal factor" in cognitive decline and Alzheimer's disease — and that B-vitamin interventions in those with elevated levels may meaningfully slow brain atrophy.
Other Conditions Linked to Elevated Homocysteine
Female Reproductive Health
A 2026 narrative review in the European Journal of Medical Research (Yu & Peng) documented emerging evidence connecting elevated homocysteine to a range of female reproductive outcomes, including:
Recurrent pregnancy loss (miscarriage) — possibly via placental vascular damage
Preeclampsia and pregnancy-induced hypertension
Neural tube defects in offspring when folate levels are low
Polycystic ovary syndrome (PCOS) — with homocysteine often elevated in this condition
Impaired IVF success rates
The authors emphasised that pre-conception folate supplementation — widely recommended for neural tube defect prevention — may also help by keeping homocysteine levels in the normal range during early fetal development.
Kidney Disease
Hyperhomocysteinemia is nearly universal in chronic kidney disease and likely contributes to the dramatically elevated cardiovascular mortality seen in CKD patients. The kidneys are both a victim and a cause — reduced kidney function elevates homocysteine, and elevated homocysteine may worsen kidney damage through oxidative stress and endothelial injury.
Bone Health
Several studies link elevated homocysteine to impaired collagen cross-linking in bone tissue, reduced bone mineral density, and increased fracture risk — an association of particular relevance in older adults.
Depression & Mental Health
Homocysteine interferes with neurotransmitter synthesis. Folate and B12 deficiencies — which drive homocysteine up — also impair the production of serotonin, dopamine, and norepinephrine, providing a biochemical link to depressive disorders that several clinical trials are actively investigating.
Who Is Most at Risk for High Homocysteine?
People most at risk for high homocysteine include: older adults (especially men over 65), vegans and vegetarians (B12 deficiency risk), people with MTHFR gene mutations, those with chronic kidney disease, individuals taking metformin or proton pump inhibitors long-term, heavy smokers, and those with diets low in leafy green vegetables.
Older adults (especially men 65+): Age reduces kidney clearance and B12 absorption simultaneously
Vegans and strict vegetarians: Dietary B12 is found exclusively in animal products; deficiency is almost universal without supplementation
MTHFR C677T homozygotes: Reduced enzyme efficiency, especially under low-folate conditions
Chronic kidney disease patients: Impaired renal clearance of homocysteine
Long-term metformin users: Impaired B12 absorption is a well-documented side effect
Heavy smokers: Tobacco disrupts B-vitamin metabolism
Hypothyroid individuals: Thyroid hormone influences homocysteine metabolism
Women with PCOS: Often have elevated homocysteine compared to controls
Pregnant women with poor nutrition: High folate demands during pregnancy
People with malabsorption conditions: Celiac disease, Crohn's disease, gastric bypass surgery
9 Evidence-Based Ways to Lower Homocysteine
The good news: homocysteine levels are highly responsive to targeted intervention. Here are the strategies with the strongest scientific backing, ranked by evidence quality.
1 Optimise Folate (Vitamin B9) Intake
Folate is the single most powerful nutritional lever for reducing homocysteine. Eat at minimum 5 servings of dark leafy greens daily (spinach, kale, broccoli, asparagus, romaine lettuce). For those with MTHFR variants, methylfolate (5-MTHF) — the pre-converted form — may be more effective than standard folic acid. The RDA is 400 mcg/day for adults; 600 mcg/day during pregnancy.
2 Correct Vitamin B12 Deficiency
B12 deficiency is astonishingly common — affecting an estimated 6% of adults under 60 and up to 20% over 60. Dietary sources include meat, fish, eggs, and dairy. If you're vegan, take metformin, use PPIs, or are over 60: get your B12 tested and supplement if indicated. Methylcobalamin or hydroxocobalamin forms have superior retention compared to cyanocobalamin. Sublingual delivery can bypass absorption issues related to intrinsic factor deficiency.
3 Ensure Adequate Vitamin B6
B6 drives the transsulfuration pathway, converting homocysteine to cysteine. Good sources include poultry, fish, potatoes, bananas, and chickpeas. The RDA is 1.3–1.7 mg/day for adults. Supplemental doses used in research typically range from 25–100 mg/day — but long-term high-dose B6 (>200 mg/day) can cause peripheral neuropathy, so stay within safe limits.
4 Use a Targeted B-Complex Supplement
A 2025 systematic review and network meta-analysis in Nutrition Reviews (Liu et al.) evaluated the comparative efficacy of various nutritional supplements for reducing homocysteine in healthy adults. Combined B-vitamin supplementation (folate + B12 + B6) consistently outperformed any single nutrient in lowering plasma homocysteine. Look for supplements providing methylfolate, methylcobalamin, and pyridoxal-5-phosphate (P5P) — the bioactive forms of each vitamin.
5 Build a Homocysteine-Lowering Diet
Beyond B vitamins, the overall dietary pattern matters. A Mediterranean-style diet — rich in vegetables, legumes, fish, whole grains, and olive oil — is associated with lower homocysteine levels across multiple population studies. Particular foods to prioritise include: lentils and beans (folate-rich), salmon and sardines (B12 + omega-3s), leafy greens (folate), eggs (B12 + choline), and whole grains (B vitamins + fibre).
6 Reduce Protein Overconsumption (When Not Matched by B Vitamins)
More dietary protein means more methionine — and more methionine means more homocysteine substrate. Very high-protein diets (typical in bodybuilding contexts) can elevate homocysteine if B-vitamin intake doesn't scale proportionally. This doesn't mean avoiding protein — it means ensuring your B-vitamin status is optimised when protein intake is high.
7 Quit Smoking
Smoking disrupts folate and B12 metabolism at multiple levels. Smokers consistently have higher homocysteine levels than non-smokers in epidemiological studies. Quitting smoking is one of the most powerful, broad-spectrum cardiovascular interventions available — and it will help your homocysteine levels as a bonus.
8 Moderate Alcohol Intake
Alcohol interferes with folate absorption in the small intestine and increases urinary folate excretion, effectively causing functional folate deficiency even in people whose dietary intake appears adequate. Limiting alcohol to no more than one standard drink per day for women and two for men — or abstaining entirely — meaningfully supports healthy homocysteine metabolism.
9 Regular Physical Activity
Aerobic exercise has been associated with modest reductions in homocysteine in several studies, though the effect is smaller than that of nutritional interventions. More importantly, regular exercise improves the endothelial dysfunction that high homocysteine promotes — providing a protective benefit independently of homocysteine levels themselves. Aim for at least 150 minutes of moderate aerobic activity per week.
Supplement Deep-Dive: What the 2025 Network Meta-Analysis Found
The most methodologically rigorous recent analysis of supplements for homocysteine lowering was conducted by Liu et al. (2025) in Nutrition Reviews, covering 83 randomised controlled trials and applying network meta-analysis to compare multiple interventions head-to-head.
Primary Vitamins (Folate & B-Complex)
Folate Alone
Efficacy: High
Key Considerations: The most powerful single agent available. Consider methylfolate (5-MTHF) for individuals with MTHFR polymorphisms to bypass genetic blocks.
Evidence Level: Strong RCT evidence
Vitamin B12 Alone
Efficacy: Moderate
Key Considerations: Efficacy is most pronounced when a baseline B12 deficiency is the primary driver of the elevation.
Evidence Level: Good RCT evidence
Vitamin B6 Alone
Efficacy: Moderate
Key Considerations: Primarily useful for managing post-methionine-load elevations (the transsulfuration pathway).
Evidence Level: Good RCT evidence
Combined Folate + B12 + B6
Efficacy: Highest
Key Considerations: Provides a synergistic effect addressing both the remethylation and transsulfuration pathways simultaneously; yields the most consistent clinical results.
Evidence Level: Strong RCT + meta-analysis evidence
Targeted & Adjunctive Agents
Riboflavin (Vitamin B2)
Efficacy: Moderate
Key Considerations: Serves as a crucial cofactor for the MTHFR enzyme; particularly beneficial for individuals with the MTHFR C677T homozygous genotype.
Evidence Level: Moderate RCT evidence
Betaine (Trimethylglycine / TMG)
Efficacy: High
Key Considerations: Utilizes the alternative, folate-independent BHMT pathway in the liver and kidneys to remethylate homocysteine back to methionine. Highly useful as an adjunct.
Evidence Level: Good RCT evidence
N-Acetyl Cysteine (NAC)
Efficacy: Moderate
Key Considerations: Functions primarily as an antioxidant to mitigate the oxidative vascular endothelial injuries driven by high homocysteine.
Evidence Level: Limited RCT evidence
Omega-3 Fatty Acids
Efficacy: Modest
Key Considerations: Provides indirect cardiovascular benefits via endothelial protection and anti-inflammatory properties rather than acting as a direct homocysteine-lowering agent.
Evidence Level: Mixed evidenceA Practical Supplement Protocol
Based on the current evidence, a reasonable protocol for someone with confirmed elevated homocysteine (under medical supervision) might include:
Methylfolate (5-MTHF): 400–1000 mcg/day (higher if MTHFR homozygous)
Methylcobalamin (B12): 500–1000 mcg/day (sublingual for absorption issues)
Pyridoxal-5-phosphate (B6): 25–50 mg/day
Riboflavin (B2): 10–25 mg/day if MTHFR C677T variant is present
Betaine (TMG): 500–3000 mg/day as an adjunct if needed
⚠️ Always Consult Your Doctor
The protocol above is educational only. High-dose B-vitamin supplementation is generally well-tolerated but can interact with certain medications and conditions. A healthcare provider should confirm your baseline levels, identify the underlying cause of elevation, and monitor your response to treatment. Do not self-diagnose or self-treat based on this article alone.
5 Common Myths & Mistakes About Homocysteine
❌ Myth 1 "If my cholesterol is normal, I don't need to worry about homocysteine."
Homocysteine is an independent risk factor for cardiovascular disease. Research has shown it raises risk even when LDL cholesterol, blood pressure, and other traditional risk markers are within normal ranges. A full cardiovascular risk profile should include both.
❌ Myth 2 "Just take folic acid and you're done."
Standard folic acid (the synthetic form) must be converted by the MTHFR enzyme to be used. People with MTHFR variants can't make this conversion efficiently. For them, methylfolate (5-MTHF) is needed. Additionally, treating high homocysteine with folate alone when B12 is deficient can mask B12 deficiency while allowing neurological damage to progress.
❌ Myth 3: "Lowering homocysteine always prevents heart attacks."
This is the most medically important nuance in this field. While elevated homocysteine is clearly associated with increased cardiovascular risk, large randomised trials in unselected populations have not consistently shown that B-vitamin supplementation reduces heart attack or stroke rates. This doesn't mean homocysteine isn't harmful — it means the relationship is complex, and treatment should be targeted to high-risk individuals.
❌ Myth 4: "Homocysteine testing is only for people who've had heart attacks."
Testing is relevant for a wide range of people: those with a family history of early cardiovascular disease, recurrent pregnancy loss, known MTHFR mutations, type 2 diabetes, chronic kidney disease, long-term medication use, or unexplained cognitive decline. Don't wait for a crisis event.
❌ Myth 5: "High homocysteine is a rare or exotic condition."
Mild hyperhomocysteinemia (15–30 μmol/L) affects millions of people — estimates suggest 5–10% of the general adult population. In older adults, those with poor diets, vegans, and people with MTHFR variants, rates are substantially higher. It's far more common than most people — or their doctors — realise.
Frequently Asked Questions
What is a dangerously high homocysteine level?
Levels above 30 μmol/L are considered moderately elevated and warrant medical investigation and treatment. Levels above 100 μmol/L (seen in the rare genetic condition homocystinuria) are severe and associated with very high rates of early cardiovascular events, lens dislocation, and intellectual disability if untreated. For most adults, a level consistently above 15 μmol/L merits attention and investigation.
How quickly can homocysteine levels be lowered?
In people with nutritional deficiencies as the primary cause, B-vitamin supplementation can produce meaningful reductions in plasma homocysteine within 4–6 weeks. The degree of reduction depends on baseline levels, the severity of the underlying deficiency, and the specific B vitamins supplemented. Levels should be retested 2–3 months after starting an intervention to assess response
.
Should I ask my doctor to test my homocysteine?
Yes, if you have any of the following: a family history of early heart disease, recurrent miscarriages, suspected B12 deficiency (vegan/vegetarian diet, long-term metformin or PPI use), known MTHFR gene mutation, chronic kidney disease, unexplained cognitive decline, or you're simply interested in a comprehensive cardiovascular risk assessment. The test is inexpensive and a simple blood draw.
Can diet alone lower homocysteine to a healthy range?
For people with mild elevations driven purely by dietary deficiencies, a well-planned diet rich in leafy greens, legumes, eggs, and animal proteins (or with appropriate B12 supplementation for vegans) can often normalise levels without additional supplementation. For those with moderate-to-severe elevations, significant MTHFR variants, or poor absorption, targeted supplementation is typically necessary alongside dietary changes.
Does high homocysteine run in families?
Yes, partly. MTHFR gene variants — which predispose to elevated homocysteine — are inherited. If a parent has elevated homocysteine or a confirmed MTHFR variant, children should be tested, especially before conception or if cardiovascular risk factors are present. However, lifestyle and nutritional factors have an equal or greater influence on actual homocysteine levels in most people with these variants.
Is there a link between homocysteine and Alzheimer's disease?
Yes, and it's a compelling area of research. Multiple large population studies have found that elevated plasma homocysteine is a strong, independent predictor of cognitive decline and dementia, including Alzheimer's disease. Researchers Smith and Refsum (2021) have argued that homocysteine may be a partially causal — not just associative — factor, and that B-vitamin intervention in people with elevated levels and mild cognitive impairment may slow brain atrophy. This remains an active area of clinical investigation.
What is the MTHFR mutation and how does it affect homocysteine?
MTHFR (methylenetetrahydrofolate reductase) is an enzyme that converts folate into its active form needed for homocysteine remethylation. The most clinically relevant variant is C677T. Those who are homozygous (two copies of the variant) have up to 70% reduced enzyme activity compared to normal, which significantly impairs the body's ability to clear homocysteine — especially when folate intake is suboptimal. Testing is available through standard genetic panels. The solution often involves using methylfolate instead of folic acid.
Can high homocysteine cause miscarriage?
Research — including a 2026 narrative review in the European Journal of Medical Research — links elevated homocysteine to recurrent pregnancy loss and pregnancy complications including preeclampsia. The proposed mechanism involves vascular damage to the developing placenta. Women with a history of recurrent miscarriage should ask their healthcare provider about homocysteine testing and folate status as part of a comprehensive workup.
Are there medications that can lower homocysteine?
Beyond B-vitamin supplementation, betaine (trimethylglycine) is a pharmacological agent used in homocystinuria management. Some research has explored ACE inhibitors, metformin alternatives, and other approaches in specific populations. For most people, B-vitamin supplementation is the primary therapeutic approach. Addressing underlying conditions (kidney disease, hypothyroidism) also lowers homocysteine secondarily by treating the root cause.
What foods are highest in folate?
The richest dietary sources of folate include: cooked lentils (~358 mcg per cup), cooked spinach (~263 mcg per cup), asparagus (134 mcg per 6 spears), avocado (~122 mcg per cup), black beans (~256 mcg per cup), edamame (~482 mcg per cup), broccoli (~168 mcg per cup cooked), and fortified breakfast cereals. Note that folate is water-soluble and heat-sensitive — steaming or eating greens raw preserves more folate than boiling
.
Conclusion & Your Action Plan
Homocysteine may be one of the most underappreciated markers in preventive medicine. It's measurable, modifiable, and matters — for your heart, your brain, your vascular system, and (for women) your reproductive health.
The science is clear that elevated homocysteine is an independent cardiovascular risk factor, that it contributes to neurodegeneration and cognitive decline, and that it is meaningfully influenced by nutrition and lifestyle. The nuance — which separates good science from oversimplification — is that lowering homocysteine does not automatically translate to preventing events in all people; a precision medicine approach, targeting the right people at the right doses, is where the evidence is most compelling.
Here is your five-step action plan:
Get tested. Ask your doctor for a fasting plasma homocysteine test, especially if you have any of the risk factors described in this article.
Know your B-vitamin status. Request serum B12, red cell folate, and vitamin B6 levels alongside homocysteine.
Optimise your diet. Prioritise dark leafy greens, legumes, eggs, fish, and whole grains. Reduce alcohol and quit smoking.
Consider targeted supplementation. If levels are elevated, work with your doctor on a B-vitamin protocol using bioactive forms (methylfolate, methylcobalamin, P5P). Consider betaine if needed.
Retest in 3 months. Track your response to intervention and adjust accordingly. For those with underlying conditions (CKD, hypothyroidism), treat the root cause simultaneously.
💡 Bottom Line
Homocysteine is one of the few cardiovascular risk markers that is both meaningfully predictive and directly modifiable through nutrition. You don't need to wait for symptoms — a simple blood test gives you actionable information. The goal is optimal levels (under 10 μmol/L), not merely "normal" by conventional lab cutoffs.
Related Articles
Full-Fat Dairy Actually Good for You? The New Science on C15:0 & C17:0 and Heart Health
De Novo Lipogenesis Explained: How Sugar Turns Into Liver Fat and High Triglycerides
Rethinking Dietary Fats: What New Research Reveals About Plant vs. Animal Fats | DR T S DIDWAL
References
Cao, X., Wang, T., Mu, G., et al. (2025). Dysregulated homocysteine metabolism and cardiovascular disease and clinical treatments. Molecular and Cellular Biochemistry, 480(9), 4907–4920. https://doi.org/10.1007/s11010-025-05284-1
D'Elia, S., Morello, M., Titolo, G., et al. (2025). Homocysteine in the cardiovascular setting: What to know, what to do, and what not to do. Journal of Cardiovascular Development and Disease, 12(10), 383. https://doi.org/10.3390/jcdd12100383
Huang, W., Jie, H., Yi, J., Liu, Q., Li, S., Luo, Y., Tang, S., Chi, Z., & Wu, C. (2026). Association between homocysteine and severe cerebral small vessel disease burden in patients with type 2 diabetes mellitus. Frontiers in Endocrinology, 16, Article 1640882. https://doi.org/10.3389/fendo.2025.1640882
Liu, C., Yao, H., & Wang, F. (2025). Effect of nutritional supplements for reducing homocysteine levels in healthy adults: A systematic review and network meta-analysis of randomized trials. Nutrition Reviews, 83(7), e1533–e1543. https://doi.org/10.1093/nutrit/nuae191
Lonn, E., Yusuf, S., Arnold, M. J., et al. (2006). Homocysteine lowering with folic acid and B vitamins in vascular disease (HOPE-2 trial). New England Journal of Medicine, 354(15), 1567–1577. https://doi.org/10.1056/NEJMoa060900
Overview of homocysteine and its role in disease processes. (n.d.). ResearchGate. https://www.researchgate.net/publication/391527750
Refsum, H., Smith, AD., Ueland, P. M., et al. (2004). Facts and recommendations about total homocysteine determinations. Clinical Chemistry, 50(1), 3–32. https://doi.org/10.1373/clinchem.2003.021634
Selhub, J. (1999). Homocysteine metabolism. Annual Review of Nutrition, 19(1), 217–246. https://doi.org/10.1146/annurev.nutr.19.1.217
Smith, A. D., & Refsum, H. (2021). Homocysteine – from disease biomarker to disease prevention. Journal of Internal Medicine, 290(4), 826–854. https://doi.org/10.1111/joim.13279
Splaver, A., Lamas, G. A., & Hennekens, CH. (2004). Homocysteine and cardiovascular disease: Biological mechanisms, observational epidemiology, and the need for randomized trials. American Heart Journal, 148(1), 34–40. https://doi.org/10.1016/j.ahj.2004.03.001
Wang, D., Gao, P., Wang, X., et al. (2025). Association of plasma homocysteine with morning blood pressure in patients with essential hypertension. Hypertension Research, 48, 2243–2254. https://doi.org/10.1038/s41440-025-02235-7
Wei, L. K., Menon, S., & Griffiths, L. R. (2025). Homocysteine and stroke: A 30-year bibliometric study uncovering research trends and future directions. Journal of Mind and Medical Sciences, 12(1), 8. https://doi.org/10.3390/jmms12010008
Xu, R., Huang, F., Wang, Y., et al. (2020). Gender- and age-related differences in homocysteine concentration: A cross-sectional study of the general population of China. Scientific Reports, 10, Article 17401. https://doi.org/10.1038/s41598-020-74596-7
Yu, H., & Peng, L. F. (2026). Homocysteine and female reproductive health: A narrative review. European Journal of Medical Research, 31, Article 598. https://doi.org/10.1186/s40001-026-04229-8
Medical Disclaimer: This article is intended for educational purposes only and does not constitute medical advice. The information presented should not be used to diagnose or treat any medical condition. Always consult a qualified healthcare professional before making changes to your diet, supplement regimen, or medical treatment. Individual results may vary. Statements about supplements have not been evaluated by the Food and Drug Administration.