Exercise Doesn't Just Build Muscle—It Reprograms Aging Cells
Discover how redox regulation drives muscle aging and sarcopenia. Learn why exercise improves mitochondria, reduces oxidative stress, and helps preserve strength as you age.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/23/202618 min read
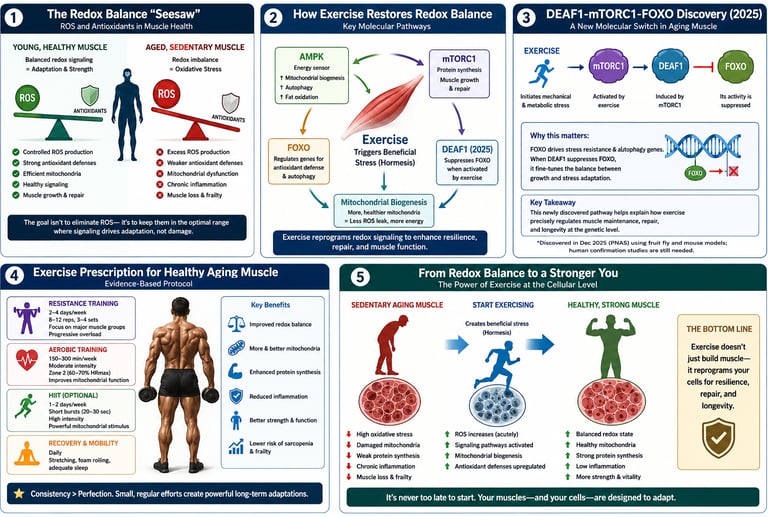

Exercise reverses sarcopenia by restoring redox balance in aging muscle. It acts as controlled “good stress” that activates pathways like FOXO-DEAF1-mTORC1 and AMPK-PGC-1α. This lowers chronic oxidative damage, builds new mitochondria, and improves protein cleanup. Consistent resistance + aerobic training over 8–16 weeks boosts strength, mitochondrial health, and muscle repair capacity.
Key Takeaways:
1. Your muscles don’t just “get old” — their chemistry gets out of balance
As we age, our muscle cells start making more “wear-and-tear” signals called ROS. A little is good. Too much for too long damages mitochondria, proteins, and your ability to rebuild muscle. That imbalance is a root cause of sarcopenia.
2. Exercise is controlled “good stress” that retrains your muscle cells
When you work out, you briefly increase those ROS signals. But that’s the point. Your muscle sees it as a safe drill and responds by building stronger antioxidant defenses and better mitochondria. It’s like a vaccine for your muscles.
3. You need both weights and walking for full protection
Resistance training flips specific switches like FOXO and DEAF1 that clean up damaged proteins. Cardio/aerobic work builds new, efficient mitochondria. Doing only one misses half the benefits. The best plan: lift 2–3x/week + brisk walk/cycle 2–4x/week.
4. It’s never too late, but consistency beats intensity
Studies show people in their 60s, 70s, and beyond can still reverse key signs of muscle aging. But one killer workout won’t do it. The real benefits show up after 8–16 weeks of regular training because you’re training your cells, not just your biceps.
5. “Daily activity” alone isn’t enough to stop muscle loss
Grocery shopping and housework are great. But the 2021 Nature Communications study found older adults still lost mitochondrial function even if they stayed active day-to-day. You need structured exercise that challenges your muscles to get the deep protective effects.
6. Skip the high-dose antioxidant pills — they can backfire
Mega-doses of vitamin C or E can actually block some exercise benefits. Why? Because they mute the ROS signal your muscle needs to adapt. Eat colorful fruits and veggies instead. Let food be your antioxidant, not pills, unless your doctor says otherwise.
7. Sleep + protein are your recovery team
Exercise creates the signal to rebuild. Protein gives your body the bricks. Sleep gives it the construction crew. Without enough of both, you’re asking your muscles to adapt with their hands tied. Spread protein across meals and aim for 7–9 hours of sleep.
8. Sarcopenia is about function, not just size
The newest 2025 research found exercise fixes quality control in muscle — how well it clears junk proteins and repairs itself — not just how big it looks. So track things like grip strength, getting up from a chair easily, and stair speed. That’s real-world aging in reverse.
Your next step, this week:
Pick 2 days for basic resistance work — even bodyweight squats, wall push-ups, and band rows count. Add a 30-minute brisk walk on 2 other days. That’s it. You’re already sending the right signal to your DEAF1-FOXO pathway, even if you can’t pronounce it yet.
Introduction
Somewhere between your 40th and 60th birthday, your muscles start fighting a battle you can't see. It isn't just "getting older." It's a measurable shift in your cells' chemistry — a slow tilt toward oxidative stress that quietly eats away at muscle fibers, mitochondria, and strength.
Scientists call this process redox dysregulation, and it sits at the molecular root of sarcopenia — the age-related loss of muscle mass, strength, and function that affects an estimated 10–27% of adults over 60, depending on the diagnostic criteria used.
Here's the good news, backed by a growing body of 2021–2026 research: exercise is the single most effective modulator of redox balance in aging muscle, and it works through mechanisms far more specific and powerful than "staying active is good for you." Recent studies — including a landmark December 2025 PNAS paper identifying a brand-new molecular switch (DEAF1) and a 2026 Frontiers in Cell and Developmental Biology review — have mapped out exactly how exercise rewires the redox signaling network inside your muscle cells
What Is Redox Regulation? A Plain-Language Primer
"Redox" is shorthand for reduction-oxidation — the constant electron exchange happening inside every cell in your body. Your muscle cells generate reactive oxygen species (ROS), sometimes called free radicals, as a normal byproduct of energy production in the mitochondria.
In a young, healthy muscle cell, ROS aren't villains. At low, controlled levels, they act as signaling molecules — triggering adaptations like new mitochondria, improved insulin sensitivity, and stronger antioxidant defenses. This is called redox signaling.
The problem isn't ROS itself. The problem is imbalance:
Too little ROS → blunted adaptive signaling, weaker stress resilience
Too much ROS, for too long, with too few defenses → oxidative stress, protein damage, mitochondrial dysfunction, and chronic low-grade inflammation
Redox regulation is the body's system for balancing the production of reactive oxygen species (free radicals) against antioxidant defenses, maintaining the right amount of oxidative signaling for healthy cell function without causing cellular damage.
As we age, this balance tips. Antioxidant enzyme activity (superoxide dismutase, catalase, glutathione peroxidase) typically declines, mitochondria become less efficient and leakier, and ROS production rises — a state researchers describe as "inflammaging" combined with chronic oxidative stress.
How Redox Imbalance Drives Sarcopenia and Frailty
Sarcopenia isn't simply "muscle shrinking." It's a multi-system breakdown, and redox imbalance touches nearly every part of it.
1. Protein Quality Control Breaks Down
Muscle fibers constantly need to break down damaged proteins (via autophagy) and build new ones (via protein synthesis). Chronic oxidative stress disrupts this balance, leading to an accumulation of damaged, dysfunctional proteins — a hallmark of aged muscle tissue.
2. Mitochondrial Dysfunction Compounds Itself
Damaged mitochondria leak more ROS than healthy ones, creating a vicious cycle: oxidative damage → mitochondrial dysfunction → more oxidative damage. A 2021 study in Nature Communications found that aging was associated with a clear decline in mitochondrial capacity, exercise capacity and efficiency, gait stability, muscle function, and insulin sensitivity — even in older adults who maintained adequate daily physical activity levels.
3. Satellite Cells (Muscle Stem Cells) Lose Regenerative Capacity
Muscle repair depends on satellite cells, which are highly sensitive to their redox environment. Chronic oxidative stress impairs their ability to activate, proliferate, and differentiate into new muscle fibers — directly limiting regeneration capacity in older adults.
4. Chronic Inflammation Joins the Fight
Oxidative stress and inflammatory signaling are deeply intertwined. Elevated ROS activates inflammatory pathways (like NF-κB), and the resulting cytokines (IL-6, TNF-α) further disrupt muscle protein balance — accelerating both sarcopenia and frailty.
5. The Functional Consequence: Frailty
Clinically, this molecular cascade shows up as frailty syndrome — slow gait speed, weak grip strength, exhaustion, low physical activity, and unintentional weight loss. Frailty and sarcopenia overlap significantly but aren't identical; sarcopenia is a muscle-specific diagnosis, while frailty is a broader vulnerability state.
The Science: How Exercise Rebalances Redox Signaling
This is where the story gets genuinely exciting — and where the newest research adds real precision to what we already knew.
Exercise Is a Controlled Redox Stressor
When you exercise, you transiently increase ROS production in working muscle. This sounds counterintuitive, but it's the key. According to a 2026 review in Frontiers in Cell and Developmental Biology, exercise functions as a key modulator of redox regulation in aging muscle — not by eliminating oxidative stress, but by training the cell's response to it.
This repeated, controlled exposure to exercise-induced ROS triggers what's called a hormetic adaptation: the muscle responds by upregulating its own antioxidant defense systems, becoming more resilient over time. This is fundamentally different from chronic, uncontrolled oxidative stress from sedentary aging — dose and context matter enormously.
Three Major Pathways Exercise Activates
1. Nrf2/Keap1 antioxidant pathway — Exercise activates Nrf2, a master transcription factor that switches on dozens of antioxidant and detoxification genes, boosting the muscle's own defense capacity.
2. AMPK-PGC-1α mitochondrial biogenesis pathway — Exercise-induced energy stress activates AMPK, which in turn activates PGC-1α, the master regulator of mitochondrial biogenesis — literally building new, more efficient mitochondria that produce less ROS leakage per unit of energy generated.
3. FOXO-regulated proteostasis pathway — This is the pathway behind the newest and most significant 2025 discovery, detailed below.
The DEAF1-mTORC1-FOXO Discovery: A 2025 Breakthrough
For years, scientists knew that mTORC1 (mechanistic target of rapamycin complex 1) — a central regulator of cell growth and protein synthesis — becomes paradoxically overactivated in aging muscle, contributing to impaired proteostasis and accelerated sarcopenia. What wasn't clear was why this overactivation happens, or how exercise reverses it.
A December 2025 study published in the Proceedings of the National Academy of Sciences by Choy and colleagues at Duke-NUS Medical School answered this question directly.
What the Researchers Found
Using fruit fly and mouse models, the team identified DEAF1, a transcription factor regulated by the FOXO family of proteins, as a key upstream driver of excessive mTORC1 activity in aged muscle. Increased DEAF1 boosts mTOR expression, driving protein imbalance and muscle decline. As we age, FOXO activity naturally declines, which removes the normal brake on DEAF1 — allowing it to accumulate and push mTORC1 into overdrive.
The clinically important part: exercise reverses this process by suppressing DEAF1 through FOXO activation, while blocking FOXO or elevating DEAF1 prevents exercise benefits. In other words, the researchers experimentally confirmed that FOXO activation is necessary for exercise to produce its muscle-protective effects — when they blocked FOXO or artificially kept DEAF1 levels high, exercise's benefits disappeared entirely.
Lead author Tang Hong-Wen explained the practical implication plainly: physical activity activates proteins that lower DEAF1 levels, bringing the mTORC1 growth pathway back into balance, which restores the muscle's capacity for self-repair.
Why This Matters Clinically
This finding is significant for three reasons that go beyond academic interest:
It identifies a specific, druggable target (DEAF1) for future pharmacological interventions in people who cannot exercise due to illness, injury, or frailty — though no human drug trials exist yet.
It mechanistically explains why long-term, consistent exercise — not a single session — is required: FOXO-DEAF1 suppression appears to depend on a sustained training stimulus, not acute exposure alone.
It validates resistance and endurance training as upstream regulators of protein quality control, not just muscle size — addressing one of the deeper mechanisms behind sarcopenia rather than just symptoms.
Mitochondria, ROS, and Aging Muscle: What the Data Shows
Mitochondria are both the main producers of ROS and the main victims of oxidative damage in aging muscle — making them ground zero for redox-based interventions.
The Maastricht Mitochondrial Capacity Study
One of the most methodologically rigorous studies on this topic comes from Grevendonk and colleagues, published in Nature Communications in 2021. The researchers compared mitochondrial capacity and physical function across young adults, older sedentary adults, and older adults who exercised regularly — all while carefully matching for habitual physical activity levels.
Key findings:
Aging was associated with a decline in mitochondrial capacity, exercise efficiency, gait stability, muscle function, and insulin sensitivity — even in older adults maintaining adequate daily activity.
However, a further increase in physical activity through structured exercise training could largely offset these age-related declines.
Clinical relevance: This study is important because it separates "background daily activity" from "structured exercise training" — and shows that the latter provides protective effects the former alone does not fully deliver. If you're relying on incidental daily movement (errands, light walking) without structured training, you may be missing a meaningful chunk of the mitochondrial protection exercise can offer.
Why Mitochondrial Quality Matters More Than Quantity
Newer research increasingly emphasizes mitochondrial quality control — biogenesis (making new mitochondria), fission/fusion dynamics, and mitophagy (selectively clearing damaged mitochondria) — over simply having more mitochondrial mass. Exercise, particularly a combination of aerobic and resistance training, appears to favorably influence all three processes, reducing the population of "leaky," ROS-generating dysfunctional mitochondria.
Exercise as Hormetic Stress: Why "A Little Damage" Helps
This is one of the most counterintuitive — and most important — concepts in redox biology.
Hormesis describes a biological phenomenon where a low dose of a stressor that would be harmful at high doses instead triggers a beneficial adaptive response. Exercise-induced ROS is a textbook example.
The Mechanistic Logic
Exercise transiently increases ROS production in contracting muscle fibers.
This transient ROS surge activates redox-sensitive signaling pathways (Nrf2, NF-κB at controlled levels, MAPK pathways).
These pathways upregulate the muscle's own antioxidant enzyme production and repair machinery.
Over repeated training sessions, the muscle becomes more resilient to oxidative stress than it was before — a true adaptive overcompensation.
This explains a finding that initially puzzled researchers: high-dose antioxidant supplementation (e.g., very high-dose vitamin C and E) can actually blunt some training adaptations by suppressing the very ROS signal that triggers beneficial adaptation. This doesn't mean antioxidants are bad — dietary antioxidants from whole foods operate very differently from megadose supplements — but it does mean more isn't automatically better (more in the Myths section below).
Acute vs. Chronic Exercise: A Critical Distinction
Factor Acute Exercise (Single Session) Chronic Exercise (Consistent Training) ROS response Transient spike during/after exercise Blunted spike (trained efficiency) Antioxidant defenses Temporarily depleted Progressively upregulated baseline Inflammatory response Short-term, localized rise Lower resting inflammatory markers Net redox effect Short-term oxidative stress Long-term redox resilience Muscle protein balance Temporary breakdown signal Net positive remodeling over time
This table underscores a clinically important point: judging exercise's redox effects from a single session is misleading. The benefits of exercise on redox balance are a training adaptation, observed over weeks to months — not an instant biochemical fix.
Practical Application: An Evidence-Based Exercise Protocol
Translating this mechanistic science into action doesn't require complexity. Here's a structured approach grounded in the research above and broader exercise science consensus for combating sarcopenia.
Step 1: Combine Resistance Training and Aerobic Exercise
Neither modality alone fully replicates the redox and mitochondrial benefits found in the research. A combined approach addresses multiple pathways simultaneously.
Weekly framework (adjust to current fitness level and consult your doctor first):
Resistance training: 2–3 sessions/week, targeting all major muscle groups, progressing gradually in load or repetitions over time
Aerobic/cardiovascular training: 2–4 sessions/week, mixing moderate-intensity steady-state work with occasional higher-intensity intervals
Balance and mobility work: 2–3 sessions/week (can overlap with the above), particularly important for frailty prevention
Step 2: Prioritize Progressive Overload
The FOXO-DEAF1 and mitochondrial biogenesis pathways respond to a sustained training stimulus, not a one-off workout. Gradually increasing resistance, repetitions, or duration over weeks signals to the muscle that adaptation is required.
Step 3: Don't Skip Protein and Recovery
Redox-driven proteostasis repair (clearing damaged proteins, building new ones) requires adequate amino acid availability. General guidance from sarcopenia research supports:
Adequate total daily protein intake spread across meals (specific targets should be personalized with a healthcare provider or registered dietitian, especially for those with kidney conditions)
7–9 hours of sleep, when much of the cellular repair and growth hormone signaling occurs
At least one full rest day between intense resistance sessions for the same muscle group
Step 4: Be Consistent Over Months, Not Days
Because the discussed redox adaptations (Nrf2 upregulation, mitochondrial biogenesis, FOXO-DEAF1 suppression) are training adaptations, expect meaningful physiological shifts over 8–16 weeks of consistent training, with continued gains over years.
Safety note: If you are over 65, have a chronic health condition, take medications affecting balance or heart rate, or have not exercised regularly in years, consult your physician before starting a new training program, and consider an initial assessment with a physical therapist or qualified trainer experienced in older-adult populations.
Evidence Summary Table: Key Studies at a Glance
Choy et al. (2025) — PNAS
Study Design: Mechanistic laboratory investigation utilizing Drosophila (fruit fly) and murine (mouse) models.
Key Finding: Physical exercise suppresses the transcription factor DEAF1 via FOXO activation, which normalizes hyperactive mTORC1 signaling and improves cellular proteostasis (protein homeostasis).
Clinical Relevance: Isolates a distinct, targetable molecular pathway that explains precisely how exercise mitigates and reverses skeletal muscle aging at the cellular level.
Limitations: Exploratory. Restricted to animal and insect models; direct translation to human skeletal muscle biology has not yet been clinically established.
Grevendonk et al. (2021) — Nature Communications
Study Design: Cross-sectional analysis combined with a controlled human exercise training intervention.
Key Finding: Structured exercise training substantially counteracts age-related degradation in mitochondrial capacity and overall physical function.
Clinical Relevance: Differentiates the clinical potency of structured, progressive training from general, incidental physical activity; strongly supports the prescription of dedicated exercise protocols over vague "active lifestyle" recommendations.
Limitations: Moderate. Features a modest sample size typical of deeply phenotype-mapped metabolic physiology trials, necessitating broader replication across diverse patient cohorts.
Cartee et al. (2016) — Cell Metabolism
Study Design: Narrative and mechanistic literature review.
Key Finding: Exercise sustains healthy skeletal muscle aging by stimulating multiple convergent, overlapping molecular pathways.
Clinical Relevance: Establishes a foundational, cross-disciplinary framework that connects physical exertion to baseline muscle aging biology.
Limitations: Qualitative. Serves as a conceptual synthesis of existing primary data rather than introducing novel empirical experiments or data points.
Liu et al. (2023) — Sports Medicine - Open
Study Design: Narrative review.
Key Finding: Exercise actively drives tissue regeneration by modulating diverse mechanistic pathways, including redox status and satellite (stem) cell dynamics.
Clinical Relevance: Expands the regenerative paradigm beyond isolated skeletal muscle tissue to broader, systemic whole-body tissue repair and longevity benefits.
Limitations: Qualitative. Mechanisms are compiled from highly heterogeneous tissue profiles, varying animal species, and disparate study architectures.
Guo et al. (2026) — Frontiers in Cell and Developmental Biology
Study Design: Narrative review.
Key Finding: Positions regular exercise as a primary behavioral modulator of redox regulation (antioxidant/pro-oxidant balance) in preventing sarcopenia (age-related muscle loss) and clinical frailty.
Clinical Relevance: Integrates the complex literature on redox biology, aging, and physical training into a cohesive therapeutic framework for clinicians.
Limitations: Qualitative. Conclusions are entirely dependent on the primary methodologies and data quality of the underlying literature cited.
Common Myths and Mistakes
Myth 1: "More antioxidant supplements means better recovery and less muscle aging."
Reality: High-dose antioxidant supplementation (particularly mega-doses of vitamin C and E) has been shown in some studies to blunt key training adaptations by suppressing the very ROS signaling that drives beneficial change. Whole-food antioxidants as part of a balanced diet are different from concentrated supplement megadoses — but more is not inherently better here.
Myth 2: "If I'm not sore, the workout didn't work."
Reality: Muscle soreness reflects mechanical and inflammatory responses, not a direct measure of redox adaptation or mitochondrial benefit. Many of the most valuable adaptations (mitochondrial biogenesis, FOXO activation) occur without significant soreness.
Myth 3: "Cardio is for the heart, weights are for muscle — pick one."
Reality: As covered above, resistance and aerobic training activate overlapping but distinct redox and mitochondrial pathways. The research consistently favors combined approaches for comprehensive sarcopenia prevention.
Myth 4: "It's too late to reverse muscle aging once you're past 60."
Reality: Multiple studies, including Grevendonk et al., found that structured exercise training in older adults could substantially offset age-related declines — this is a modifiable process well into later decades of life, not a fixed, one-way trajectory.
Myth 5: "A single intense workout 'detoxes' your muscles of oxidative damage."
Reality: Redox adaptation is a training effect built over weeks and months, not a single-session reset. Consistency matters far more than occasional high-intensity efforts.
Myth 6: "Sarcopenia is just about muscle size — building bigger muscles fixes it."
Reality: As the DEAF1 research illustrates, sarcopenia involves deeper issues of protein quality control and cellular repair capacity, not just muscle fiber size. This is why function (strength, balance, mitochondrial efficiency) matters as much as muscle mass in monitoring progress.
Frequently Asked Questions
What is redox regulation in simple terms?
Redox regulation is the body's internal balancing act between producing reactive oxygen species (a normal byproduct of cellular energy use) and neutralizing them with antioxidant defenses, keeping cellular signaling healthy without causing damage.
Does exercise increase or decrease oxidative stress?
Both, depending on the timeframe. A single exercise session transiently increases reactive oxygen species production. Over weeks of consistent training, this triggers the body to build stronger antioxidant defenses, ultimately lowering chronic oxidative stress and improving redox resilience.
What type of exercise is best for sarcopenia?
Current evidence supports combining resistance training (2–3 sessions weekly) with aerobic exercise (2–4 sessions weekly) for the most comprehensive protection against sarcopenia, since each modality activates somewhat different but complementary redox and mitochondrial pathways.
What is DEAF1 and why does it matter for muscle aging?
DEAF1 is a transcription factor that increases in aging muscle and drives excessive activity of mTORC1, a pathway that, when overactivated, impairs the muscle's ability to clear damaged proteins. A 2025 PNAS study found that exercise suppresses DEAF1 through FOXO protein activation, helping restore healthy muscle protein turnover.
Can muscle aging be reversed, or only slowed?
Multiple studies suggest meaningful reversal of specific functional and mitochondrial markers is possible with structured exercise, even in older adults — though full reversal to youthful baseline levels has not been demonstrated, and results vary by individual health status, training consistency, and starting point.
How long does it take to see redox-related benefits from exercise?
Most mechanistic studies suggest meaningful mitochondrial and antioxidant adaptations develop over approximately 8–16 weeks of consistent training, with continued improvements over months and years of sustained activity.
Should I take antioxidant supplements to fight muscle aging?
Be cautious with high-dose antioxidant supplements, as some research suggests they can blunt beneficial exercise-induced redox signaling. A balanced, whole-food diet rich in natural antioxidants (fruits, vegetables, polyphenols) is generally preferred over concentrated supplement megadoses; discuss any supplementation plan with your doctor.
Is walking enough to prevent sarcopenia?
Walking provides valuable cardiovascular and general health benefits, but research like the Grevendonk et al. study suggests that structured exercise training beyond habitual daily activity offers additional, measurable protection against age-related mitochondrial and muscle function decline. Walking is a great foundation, but ideally paired with resistance training.
What's the difference between sarcopenia and frailty?
Sarcopenia specifically refers to age-related loss of muscle mass, strength, and function. Frailty is a broader clinical syndrome involving reduced physiological reserve across multiple systems (including but not limited to muscle), often measured by criteria like slow gait speed, weakness, exhaustion, and unintentional weight loss. They frequently overlap but are distinct diagnoses.
Can resistance training alone fix mitochondrial dysfunction in aging muscle?
Resistance training contributes meaningfully to mitochondrial quality control, but most research suggests combining it with aerobic training produces more comprehensive mitochondrial biogenesis and redox benefits than either modality alone.
At what age should I start worrying about sarcopenia prevention?
Muscle mass and strength typically peak in your 30s and begin a gradual decline afterward, often accelerating after age 60. Most experts recommend incorporating resistance training as a long-term habit well before noticeable declines occur — ideally starting in your 30s or 40s, though it's never too late to begin.
Is the DEAF1 research applicable to humans yet?
Not directly as a treatment target. The 2025 PNAS study was conducted in fruit fly and mouse models, providing strong mechanistic insight into why exercise works, but human drug or supplement interventions targeting DEAF1 have not yet been developed or tested in clinical trials.
Conclusion and Action Steps
Muscle aging isn't a vague, unstoppable decline — it's a specific, increasingly well-mapped biological process involving redox imbalance, mitochondrial dysfunction, and breakdowns in protein quality control. And at every level of that process, from whole-body physical function down to individual transcription factors like DEAF1, exercise is the most consistently validated intervention we have.
The 2025–2026 research summarized here doesn't just confirm "exercise is good for aging muscle" — it explains why, down to the molecular signaling level, while also being honest about what remains unproven, particularly the translation of animal-model mechanisms into confirmed human treatments.
Your action steps, starting today:
Talk to your doctor about starting or adjusting a structured exercise program, especially if you have existing health conditions.
Build a weekly routine combining resistance training (2–3x/week) and aerobic exercise (2–4x/week), using the sample structure above as a starting template.
Commit to at least 8–16 weeks before judging results — redox and mitochondrial adaptations are a training effect, not an instant fix.
Prioritize protein intake and sleep to support the cellular repair processes exercise activates.
Be skeptical of "quick fix" antioxidant supplements and focus on a whole-food, nutrient-dense diet alongside your training.
Always consult your healthcare provider before starting a new exercise program, particularly if you are over 45, previously sedentary, or have a history of cardiovascular disease, hypertension, or diabetes. For individuals with established cardiovascular disease, initiate resistance training within a supervised cardiac rehabilitation program.
Related Articles
Can Exercise Really Prevent Chronic Disease? What the Latest Science Actually Shows
Non-Negotiable Health: Why All Women Need Resistance Training, Not Just Cardio | DR T S DIDWAL
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
References
Guo, H., Jiang, X., Zhiming, W., Gui, Y., & Su, Z. (2026). Redox regulation in aging muscles: exercise as a key modulator to combat sarcopenia and frailty. Frontiers in Cell and Developmental Biology, 14:1772623. https://doi.org/10.3389/fcell.2026.1772623
Liu, C., Wu, X., Vulugundam, G., Gokulnath, P., Li, G., & Xiao, J. (2023). Exercise promotes tissue regeneration: mechanisms involved and therapeutic scope. Sports Medicine - Open, 9(1), 27. https://doi.org/10.1186/s40798-023-00573-9
Choy, S.M., Goh, K.Y., Lee, W.X., Jiang, W., Gou, Q., Gopal Krishnan, P.D., Ong, S.C., Chua, K., Harmston, N., & Tang, H. (2025). Exercise suppresses DEAF1 to normalize mTORC1 activity and reverse muscle aging. Proceedings of the National Academy of Sciences, 122(48), e2508893122. https://doi.org/10.1073/pnas.2508893122
Cartee, G.D., Hepple, R.T., Bamman, M.M., & Zierath, J.R. (2016). Exercise promotes healthy aging of skeletal muscle. Cell Metabolism, 23(6), 1034–1047. https://doi.org/10.1016/j.cmet.2016.05.007
Grevendonk, L., Connell, N.J., McCrum, C., Fealy, C.E., Bilet, L., Bruls, Y.M.H., Mevenkamp, J., Schrauwen-Hinderling, V.B., Jörgensen, J.A., Moonen-Kornips, E., Schaart, G., Havekes, B., de Vogel-van den Bosch, J., Bragt, M.C.E., Meijer, K., Schrauwen, P., & Hoeks, J. (2021). Impact of aging and exercise on skeletal muscle mitochondrial capacity, energy metabolism, and physical function. Nature Communications, 12, 4773. https://doi.org/10.1038/s41467-021-24956-2
Goh, K.Y., et al. (2024). FOXO-regulated DEAF1 controls muscle regeneration through autophagy. Autophagy, 20, 2632–2654.
Gopal Krishnan, P.D., et al. (2025). Transcriptional regulation of autophagy in skeletal muscle stem cells. Disease Models & Mechanisms, 18, DMM052007.
Tang, H., et al. (2019). mTORC1 underlies age-related muscle fiber damage and loss by inducing oxidative stress and catabolism. Aging Cell, 18, e12943.
Nacarelli, T., Azar, A., & Sell, C. (2016). Mitochondrial stress induces cellular senescence in an mTORC1-dependent manner. Free Radical Biology and Medicine, 95, 133–154.
Joseph, G.A., et al. Partial inhibition of mTORC1 in aged rats counteracts the decline in muscle mass and reverses molecular signaling associated with sarcopenia.
Mitochondrial Adaptations in Aging Skeletal Muscle: Implications for Resistance Exercise Training to Treat Sarcopenia. (2024). Biology (Basel), 14(8), 962.
Hood, D.A., Memme, J.M., Oliveira, A.N., & Triolo, M. (2019). Maintenance of skeletal muscle mitochondria in health, exercise, and aging. Annual Review of Physiology, 81, 19–41.
Campos, J.C., Marchesi Bozi, L.H., Krum, B., Grassmann Bechara, L.R., Ferreira, N.D., & Arini, G.S., et al. (2023). Exercise preserves physical fitness during aging through AMPK and mitochondrial dynamics. Proceedings of the National Academy of Sciences, 120(2), e2204750120.
Lanza, I.R., & Nair, K.S. (2010). Mitochondrial function as a determinant of life span. Pflügers Archiv, 459(2), 277–289.
Bishop, D.J., Botella, J., Genders, A.J., Lee, M.J., Saner, N.J., & Kuang, J., et al. (2019). High-intensity exercise and mitochondrial biogenesis: current controversies and future research directions. Physiology, 34(1), 56–70.
Pang, B.P.S., Chan, W.S., & Chan, C.B. (2021). Mitochondria homeostasis and oxidant/antioxidant balance in skeletal muscle—do myokines play a role? Antioxidants, 10(2), 179.
Wan, W., Zhang, L., Lin, Y., Rao, X., Wang, X., & Hua, F., et al. (2023). Mitochondria-derived peptide MOTS-c: effects and mechanisms related to stress, metabolism and aging. Journal of Translational Medicine, 21(1), 36.
Li, J., Wang, Z., Li, C., Song, Y., Wang, Y., & Bo, H., et al. (2022). Impact of exercise and aging on mitochondrial homeostasis in skeletal muscle: roles of ROS and epigenetics.
Fried, L.P., Tangen, C.M., Walston, J., et al. (2001). Frailty in older adults: evidence for a phenotype. Journals of Gerontology Series A.
National Institute on Aging. Sarcopenia: Causes, Symptoms, and Treatment. (NIH publication, accessed via nia.nih.gov).
World Health Organization. Physical Activity Guidelines for Older Adults.
American College of Sports Medicine. Exercise and Physical Activity for Older Adults Position Stand.