Can Exercise Really Prevent Chronic Disease? What the Latest Science Actually Shows
Exercise lowers the risk of heart disease, type 2 diabetes, cancer, and age-related decline. Discover the latest evidence on exercise dose, consistency, exerkines, and long-term health protection.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/25/202617 min read
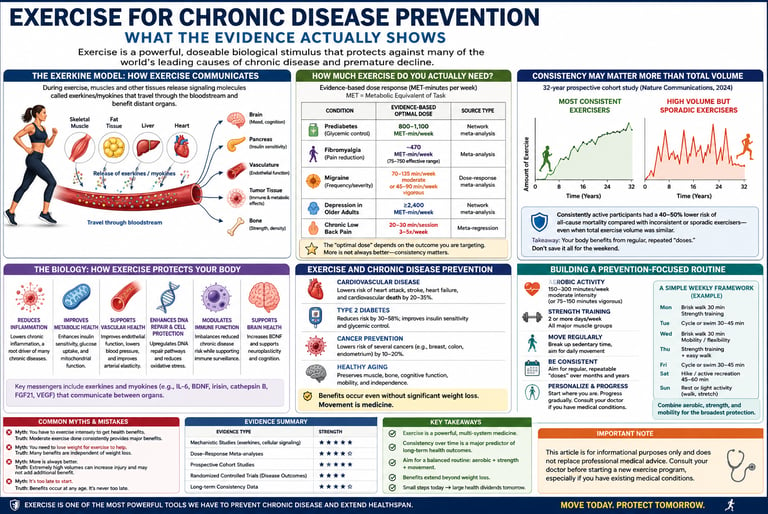
Yes. Research consistently shows that regular exercise lowers the risk of major chronic diseases, including cardiovascular disease, type 2 diabetes, certain cancers, and age-related decline. The strongest evidence supports 150–300 minutes of moderate-intensity activity per week plus strength training at least twice weekly. Studies also suggest that long-term consistency matters more than occasional bursts of intense exercise, with benefits including improved insulin sensitivity, reduced inflammation, enhanced cardiovascular function, and exercise-induced signalling molecules known as exerkines.
Key Takeaways: Exercise for Chronic Disease Prevention
1. Consistency beats intensity over decades
A 32-year study of 231,488 adults found sustained moderate activity cuts chronic disease risk 10–28% after age 60. Total lifetime volume matters less than doing it regularly without long inactive gaps.
2. Exercise is dosed biological signaling, not just calorie burn
Muscle contraction releases exerkines like IL-6, irisin, and BDNF into the bloodstream. These molecules directly influence insulin sensitivity, brain function, inflammation, and DNA repair. The benefits persist even when weight doesn't change.
3. Optimal dose depends on the target, not a universal number
Glycemic control in prediabetes peaks around 880–1,100 MET-min/week. Fibromyalgia pain relief hits at ~470 MET-min/week. Depression in older adults keeps improving up to 2,400+ MET-min/week. One prescription does not fit all outcomes.
4. Mix modalities because pathways differ
In prediabetes, aerobic training lowers post-meal glucose more effectively, whereas resistance training targets fasting glucose more effectively. Across cancer, heart disease, and aging, combined aerobic + strength + balance work covers more biology than any single type.
5. Acute exercise changes your blood’s impact on cells
Post-exercise serum from humans reduced DNA damage and upregulated repair gene PNKP in colon cancer cells within 6 hours. It also shifted gene expression toward mitochondrial metabolism and away from proliferation. Mechanism, not magic.
6. Incidental movement counts, but it’s additive
Light, non-leisure activities like walking and stairs are linked to lower cardiovascular and cancer incidence. Treat it as the foundation under structured exercise, not the replacement for it.
7. More is not always better
Dose-response curves for pain, migraine, and some clinical populations show plateaus or U-shapes. Past a point, additional volume adds little benefit and can backfire without recovery, especially in chronic conditions.
8. Build for durability, not PRs
The data reward a routine you can maintain for years, not months. Protect a "floor" level of activity for bad weeks. If you can only change one habit, pick the one you will still be doing in 2036.
Introduction
If you've ever been told to "exercise more" to protect your health, you've probably wanted a straight answer to a simple question: how much, how often, and does it actually work the way doctors say it does?
This article exists to answer that question properly — not with vague encouragement, but with a clear look at what large-scale studies, mechanistic research, and clinical trials actually show about exercise for chronic disease prevention.
What "Exercise for Disease Prevention" Actually Means
When researchers talk about exercise as a disease-prevention strategy, they're not talking about a single magic mechanism. They're describing a systemic, whole-body signalling response that affects nearly every organ system — and that response is measurably different in people who exercise regularly than in those who don't.
A major 2024 review in Signal Transduction and Targeted Therapy synthesized this idea under a useful umbrella term: exerkines. According to the authors, exerkines are signaling molecules released during exercise by tissues such as skeletal muscle, cardiac muscle, fat, and liver tissue, which mediate the benefits of exercise for preventing and treating disease. These molecules don't stay local — they travel through the bloodstream and act on distant organs, which is part of why a single bout of exercise can influence things as different as insulin sensitivity, brain function, and tumor biology.
This matters for how you should think about "exercise as medicine": it's not just calorie-burning. It's a dosed, repeatable biological stimulus with measurable downstream effects — closer in concept to a drug intervention than to a vague lifestyle habit, which is exactly why researchers increasingly study it with the same rigor (dose-response curves, mechanism studies, RCTs) used for pharmaceuticals.
How Much Exercise Do You Actually Need?
The standard public health benchmark — 150–300 minutes of moderate-intensity aerobic activity per week, or 75–150 minutes of vigorous activity, plus muscle-strengthening activity on 2 or more days — is still the baseline most major health bodies recommend. But the more interesting recent research digs into dose-response curves: does more always mean better, and is there a point of diminishing or even reversed returns?
Here's what dose-response meta-analyses across specific conditions actually show:
Condition Evidence-based optimal dose Source type Prediabetes (glycemic control) ~800–1,100 MET-min/week depending on outcome and exercise type Network meta-analysis Fibromyalgia pain ~470 MET-min/week (effective range 75–750) Meta-analysis Migraine frequency/severity 70–135 min/week moderate, or 45–90 min/week vigorous Dose-response meta-analysis Depression in older adults Risk drops progressively up to ≥2,400 MET-min/week Network meta-analysis Chronic low back pain 20–30 min/session, 3–5x/week Meta-regression
A few things jump out when you look at this table side-by-side instead of one study at a time:
The "optimal dose" is not universal. It depends heavily on the outcome you're targeting. A dose that maximizes glycemic control isn't necessarily the dose that best reduces depressive symptoms.
MET minutes per week is a more precise unit than "minutes of exercise." It accounts for intensity, not just time, which is why two people doing "30 minutes of exercise" can have very different physiological doses.
Several relationships are non-linear — for example, dose-response in chronic conditions sometimes follows a U-shaped or inverted-U curve, meaning more isn't always better past a certain point, particularly in clinical populations.
Why Consistency May Matter More Than Total Volume
Here's where one of the most important recent findings reframes the whole conversation. A 2026 study in Nature Communications followed 231,488 health professionals across three U.S. cohorts for 32 years, tracking physical activity repeatedly over time rather than just once. The goal was to understand long-term patterns — volume, consistency, and trajectory — not just a single snapshot of "how active are you right now."
The findings: maintaining physical activity at the recommended level consistently throughout the follow-up period was associated with a greater reduction in chronic disease risk than engaging in high-volume activity sporadically, interspersed with periods of inactivity. In other words, two people who accumulate the same total lifetime exercise volume may end up with meaningfully different disease outcomes if one was consistent and the other was a "weekend warrior" cycling through bursts of activity and inactivity.
The trajectory analysis was even more specific: being physically active throughout middle adulthood was linked to a 10–28% lower incidence of major chronic diseases after age 60, including type 2 diabetes, major cardiovascular disease, and cancer.
Why this matters for how you think about exercise:
This is one of the largest, longest-running physical activity cohort studies of its kind — 32 years of repeated measurement is rare and valuable.
It directly challenges the common assumption that "total volume is what counts." Pattern and adherence appear to be independent contributors to risk reduction, not just volume's byproduct.
The practical translation: a moderate, sustainable routine you can actually maintain for decades may outperform an intense routine you'll abandon after eight months.
The Biology: How Exercise Talks to Your Cells
This is the section most "exercise is medicine" articles skip — and it's the part that actually explains why the statistics in the sections above exist at all.
Myokines and exerkines: muscle as an endocrine organ
When skeletal muscle contracts repeatedly during exercise, it doesn't just burn fuel — it secretes signaling proteins called myokines, a subset of the broader exerkine family. Recent narrative reviews describe how repeated muscle contraction stimulates the release of myokines — including IL-6, irisin, BDNF, FGF21, and apelin, among others — each acting on different downstream targets.
A few specific, well-studied roles:
IL-6 rises acutely during exercise and, despite being a pro-inflammatory marker in chronic disease contexts, plays an anti-inflammatory and metabolic-regulatory role when released this way — part of why "exercise causes acute inflammation that resolves into a net anti-inflammatory state" is a real and important distinction, not just hype.
Irisin is being studied for roles beyond metabolism — including potential neuroprotective signaling relevant to Parkinson's disease research, an active and still-developing area.
BDNF (brain-derived neurotrophic factor) is one of the most consistently replicated exercise-induced molecules linked to brain health and mood regulation.
Why this matters clinically
The reason this matters isn't academic. If exercise's benefits ran purely through "you burn calories and lose weight," you'd expect any calorie-equivalent intervention to produce identical results. It doesn't. Exercise produces metabolic, anti-inflammatory, and neuroprotective signaling that calorie restriction alone does not reproduce — which is part of why exercise remains protective even in people who don't lose significant weight from it.
Exercise and Cardiovascular Disease
Cardiovascular disease prevention is the area with the deepest evidence base, spanning decades of cohort studies and trials. Current research is refining which kind of activity matters most for which population.
One useful nuance: not all activity needs to be structured "exercise" in the gym sense. Research on incidental physical activity — movement accumulated through daily living rather than dedicated workouts — has found measurable cardiovascular benefit, including findings that light-intensity activity accumulated incidentally is associated with reduced cardiovascular disease and cancer incidence in prospective cohort data.
For people managing diagnosed cardiovascular conditions, structured exercise therapy has an established role — for example, supervised exercise programs are a recognized treatment approach for peripheral artery disease, improving walking distance and symptom burden, not just "general fitness."
Exercise and Type 2 Diabetes / Metabolic Health
For glycemic control, the dose-response research is unusually granular. A 2025 network meta-analysis on people with prediabetes found that aerobic exercise alone produced the largest reductions in 2-hour post-meal blood glucose and HbA1c, with optimal doses identified separately for each outcome — roughly 880 MET-minutes/week for fasting glucose via aerobic or resistance training, and 1,100 MET-minutes/week for post-meal glucose via aerobic exercise specifically.
This level of specificity is genuinely useful, but it comes with a caveat the researchers themselves flag: despite many meta-analyses addressing physical activity's general impact, few have pinpointed the exact optimal type and dose needed to support specific guideline recommendations, leaving real uncertainty about current physical activity guidance.
What this means practically: if you're managing prediabetes, resistance training and aerobic training appear to target different specific glucose markers somewhat differently, which argues for combining modalities rather than choosing one exclusively, consistent with most current clinical guidance to pair both.
Exercise and Cancer Prevention — What the Newest Cellular Research Shows
This is one of the most actively evolving areas in exercise science, and it's worth walking through carefully because the mechanistic detail is genuinely new.
What the colon cancer cell study found
A study published in the International Journal of Cancer investigated a direct biological question: does blood drawn from a person immediately after a bout of exercise have different effects on cancer cells than blood drawn before exercise?
The setup: researchers profiled the serum proteomic response to acute exercise and evaluated the effects of exercise-conditioned human serum on DNA damage kinetics and transcriptomic signatures in colon cancer cells, using blood from people who underwent a maximal cycling test.
The results were specific and measurable:
Compared to pre-exercise serum, post-exercise serum significantly reduced markers of DNA damage at 6 hours post-irradiation and decreased the overall area-under-the-curve measure of damage, indicating accelerated DNA repair in the cancer cells exposed to it.
The post-exercise serum also increased expression of the DNA repair gene PNKP, both with and without irradiation exposure.
At the broader gene-expression level, transcriptomic analysis showed upregulation of mitochondrial energy metabolism pathways and downregulation of cell cycle and proteasome-related pathways — consistent with cells shifting toward a less proliferative, more "housekeeping" metabolic state.
The researchers' own interpretation, as summarized by Newcastle University's press office, is appropriately measured: this offers a potential mechanistic explanation for how exercise might protect against cancer progression by improving how cells repair damaged DNA and use energy, with the explicit framing that future therapies might aim to mimic these effects.
So the honest summary is: this study identifies a plausible, specific molecular mechanism (enhanced DNA repair, metabolic reprogramming) that may help explain a benefit we already see at the population level in epidemiological data — it's a "why," not new proof of the "whether."
Where the broader cancer-exercise evidence stands
Beyond this specific mechanism, exercise's role in cancer prevention and treatment support draws on a wider literature, including evidence on:
Reduced markers of oxidative and inflammatory stress in cancer patients undergoing treatment
Effects on circulating tumor cells and tumor DNA in colorectal cancer patients
Improved outcomes in structured post-treatment exercise programs
Safety note: If you have an active cancer diagnosis or are in treatment, exercise type, intensity, and timing should be guided by your oncology team — some treatments (e.g., certain chemotherapies affecting blood counts or cardiac function) require modified exercise plans, not a generic "more is better" approach.
Exercise and Healthy Aging
Aging-focused exercise research has shifted in recent years from "does exercise help older adults" (clearly yes) toward more specific questions: which modalities address which aging mechanisms, and what's the realistic dose for people with reduced mobility or multiple chronic conditions?
Current overviews of exercise interventions in aging research point to several converging themes:
Resistance training's role in preserving muscle mass and function (countering sarcopenia) is one of the better-established aging-specific benefits, distinct from cardiovascular-focused aerobic recommendations.
Balance and mobility-focused exercise is specifically recommended for older adults with reduced mobility, even when full aerobic guideline minutes aren't achievable — the principle being "be as active as your ability and condition allows," rather than an all-or-nothing threshold.
Depression and mood outcomes show a measurable dose-response relationship in older adults specifically, with risk reduction continuing to improve at higher activity levels in available data.
Practical Application: Building a Prevention-Focused Routine
Translating all of the above into something usable doesn't require perfection — it requires a structure you can sustain, given the strong signal that consistency over years, not intensity over weeks, is what tracks with the biggest risk reductions.
A general framework (confirm specifics with your physician, especially with existing conditions)
1. Anchor on the baseline guideline, then adjust:
150–300 min/week moderate aerobic activity, or 75–150 min/week vigorous, or a combination
Muscle-strengthening activity for major muscle groups on 2+ days/week
Balance-focused work for older adults or anyone with fall risk, 3+ days/week
2. Build in redundancy for bad weeks. Since long-term consistency appears to outperform sporadic high-volume bursts, design your routine assuming some weeks will be lighter — and protect a "floor" level of activity even then, rather than an all-or-nothing approach.
3. Combine modalities rather than picking one. The diabetes dose-response research above found aerobic and resistance training affect different glucose markers differently — a pattern that shows up across multiple conditions. A mixed routine likely covers more biological bases than a single-modality approach.
4. Use incidental activity as a supplement, not a replacement. Walking, taking stairs, and standing more are genuinely associated with benefit in the incidental-activity research above, but they appear to add to — not substitute for — structured activity in most of the literature.
5. Re-evaluate dose if you have a specific condition. The MET-minute targets in the Evidence Summary Table below are starting reference points for the conditions studied — not universal prescriptions. A physical therapist, exercise physiologist, or physician familiar with your condition can individualize this.
Evidence Summary Table
1. The Role of "Exerkines" in Inter-Organ Communication
Study: Walzik et al., 2024 (Signal Transduction and Targeted Therapy)
Source Type: Narrative review
Key Finding: The health benefits of exercise are driven by exerkines—signaling molecules released by the muscles, heart, fat, and liver that enable communication between different organs.
Strength: Provides a strong, comprehensive synthesis of the biological mechanisms behind exercise.
Limitation: It is a review-level paper, meaning it summarizes existing research rather than introducing new primary data.
2. Consistent vs. Sporadic Exercise for Long-Term Health
Study: Fang, Wang, Rosner et al., 2026 (Nature Communications)
Source Type: 32-year prospective cohort ($n=231,488$)
Key Finding: Staying consistently active over time reduces chronic disease risk much more effectively than sporadic bursts of high-volume activity. Sustained exercise during mid-life is linked to a 10% to 28% lower incidence of chronic disease after age 60.
Strength: Exceptionally large sample size tracked over a very long duration.
Limitation: Because it is an observational study, it cannot fully isolate direct cause-and-effect from other confounding lifestyle factors.
3. Exercise-Induced Serum and Cancer Cell Suppression
Study: Orange, Dodd, Nath et al., 2025/2026 (International Journal of Cancer)
Source Type: In-vitro mechanistic study ($n=30$ serum donors)
Key Finding: Blood serum collected immediately after exercise reduced DNA damage and improved repair signaling in colon cancer cells.
Strength: Offers novel, direct mechanistic insights into how exercise might fight cancer at a cellular level.
Limitation: Conducted entirely in a cell-culture model using a small donor sample, so it does not track actual clinical outcomes in patients.
4. Optimal Dosing for Prediabetes Control
Study: Prediabetes Glycemic Control Network Meta-Analysis (2025)
Source Type: Network meta-analysis
Key Finding: Aerobic exercise yields the largest reductions in post-meal glucose and HbA1c, with specific, distinct optimal doses required for each outcome.
Strength: Provides highly granular, specific exercise dosing data.
Limitation: The authors noted persistent uncertainty when trying to perfectly match these specific optimal doses to existing general health guidelines.
5. Benefits of Incidental (Non-Leisure) Activity
Study: Incidental Physical Activity Research (Circulation)
Source Type: Prospective cohort
Key Finding: Light-intensity, non-leisure activity (everyday incidental movement) is still significantly associated with reduced cardiovascular disease and cancer incidence.
Strength: Highly applicable and encouraging for typically sedentary populations who struggle to maintain structured workouts.
Limitation: The protective effect sizes are generally smaller than those achieved through structured, intentional exercise.
Common Myths & Mistakes
Myth: "If I exercise hard a few times a month, it's basically the same as exercising consistently." The 2026 Nature Communications cohort directly challenges this — sporadic high-volume activity mixed with inactivity was associated with smaller risk reduction than maintaining a steady recommended level.
Myth: "More exercise is always better, with no ceiling." Several dose-response analyses above show inverted-U or plateauing patterns for specific outcomes — past a certain point, additional volume may not add proportional benefit, and in some clinical populations, excessive load can be counterproductive without proper recovery.
Myth: "A cell-culture study finding X means I will personally experience X by exercising." The colon cancer serum study is a real and valuable mechanistic finding, but it does not mean "exercise cures cancer" or even that it definitively prevents it in humans at the population level on its own — it explains a plausible mechanism behind benefits already observed separately in human cohort data.
Myth: "Cardio is for your heart, weights are for your muscles — pick one based on your goal." The diabetes dose-response data shows aerobic and resistance training affect different specific metabolic markers differently. For most chronic-disease prevention goals, combining both covers more physiological ground than either alone.
Mistake: Treating MET-minute targets as exact personal prescriptions. These figures come from population-level meta-regressions with real heterogeneity and modest explained variance in some cases — useful as reference points, not as a number to hit exactly regardless of your own response, fitness level, or medical history.
FAQs
1. How much exercise do I need to meaningfully reduce chronic disease risk? The baseline evidence-based target is 150–300 minutes/week of moderate aerobic activity (or 75–150 minutes vigorous), plus strength training 2+ days/week. Specific conditions have more granular optimal doses (see the Evidence Summary Table), but the general guideline is a reasonable starting point for most healthy adults.
2. Is it better to exercise intensely a few times a week or moderately every day? Long-term cohort evidence favors consistency over time more than intensity bursts — sustained moderate activity across years appears to outperform sporadic high-volume activity with the same total lifetime volume.
3. Does walking count as real exercise for disease prevention? Yes, particularly accumulated incidental activity (walking, stairs, daily movement) shows measurable associations with reduced cardiovascular and cancer incidence in prospective research, though structured exercise generally shows larger effects.
4. Can exercise actually affect cancer cells directly, or does it just help with weight and general health? Recent mechanistic research shows exercise-conditioned blood serum can directly influence cancer cell behavior in lab studies — including enhanced DNA repair signaling — suggesting effects beyond weight management alone. This is an active, evolving research area, not a settled clinical claim.
5. What's the difference between aerobic and resistance training for chronic disease prevention? They appear to target overlapping but distinct biological pathways. For example, in prediabetes research, aerobic exercise more strongly affected post-meal glucose, while combined training affected fasting glucose differently — supporting a combined approach rather than choosing one exclusively.
6. Is there an upper limit where more exercise stops helping or becomes harmful? Some condition-specific dose-response curves show plateauing or U-shaped patterns, meaning very high volumes don't always add proportional benefit and, in certain populations or contexts, can be counterproductive without adequate recovery. This varies by condition and individual — discuss your specific situation with a physician if you're training at a high volume.
7. I have an existing chronic condition (diabetes, heart disease, cancer). Should I follow general guidelines or something different? Something individualized. General population guidelines are a reasonable starting reference, but condition-specific factors (medications, current symptoms, treatment stage) should be reviewed with your physician, a physical therapist, or an exercise physiologist before starting or significantly changing a routine.
8. How long does it take to see measurable biological benefits from starting exercise? Acute molecular changes (like the exerkine and serum-signaling effects discussed above) can be measured within hours of a single session. Clinically meaningful risk reduction for chronic disease, however, accumulates over months to years of sustained activity, which is consistent with the long-term cohort findings discussed above.
9. Does exercise help even if I don't lose weight from it? Yes — exercise produces metabolic, anti-inflammatory, and signaling effects (via myokines and exerkines) that are distinct from weight loss itself, which is part of why benefits are observed even in people whose weight doesn't change significantly.
10. What's the single most evidence-backed thing I can do if I can only change one habit? Based on the consistency-focused cohort evidence, building a routine you can sustain for years — even if moderate — appears more valuable than chasing an intense routine that's likely to be abandoned.
Conclusion & Action Steps
The strongest, most consistent theme across this entire body of research isn't a specific exercise type or a specific number of minutes — it's durability. The 32-year cohort data, the dose-response meta-analyses, and the mechanistic cell studies all point toward the same practical conclusion: a sustainable routine you maintain for years will likely do more for your long-term disease risk than an aggressive routine you can't keep up.
Concrete next steps:
Start with the baseline guideline (150–300 min/week moderate aerobic + strength training 2+ days/week) and build from there rather than starting with an ambitious, hard-to-sustain plan.
Protect a "floor" routine for hard weeks rather than treating any gap as a failure — the evidence rewards long-term pattern, not unbroken perfection.
Combine aerobic and resistance training rather than choosing one, since they appear to affect different physiological pathways relevant to chronic disease.
If you have an existing condition, take this article's general findings to your physician or a specialist (cardiologist, endocrinologist, oncologist, or physical therapist as relevant) to individualize dose and modality.
Reassess your routine every few months, not for intensity escalation's own sake, but to confirm it's still something you can sustain for years, not just weeks.
This article is for informational purposes and does not replace personalized medical advice. If you have an existing chronic condition, are pregnant, or are starting exercise after a long period of inactivity, consult your physician before beginning a new program.
Related Articles
Not All Exercise Is Equal: Which Workout Is Best for Diabetes and Heart Health
Non-Negotiable Health: Why All Women Need Resistance Training, Not Just Cardio | DR T S DIDWAL
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
References
Walzik, D., Wences Chirino, T.Y., Zimmer, P., & Joisten, N. (2024). Molecular insights of exercise therapy in disease prevention and treatment. Signal Transduction and Targeted Therapy, 9, 138. https://doi.org/10.1038/s41392-024-01841-0
Jain, A., Johnston, C., Zhang, Y., Oh, J., Tsung, C., Kent, E., & Zhang, H. (2026). An overview of current research on exercise interventions in aging and aging-related disease. Frontiers in Aging, 7:1832962. https://doi.org/10.3389/fragi.2026.1832962
Fang, Z., Wang, P., Rosner, B.A., et al. (2026). Sustained physical activity offers benefits beyond activity volume in chronic disease prevention. Nature Communications, 17, 2730. https://doi.org/10.1038/s41467-026-69552-4
Fairag, M., Alzahrani, S.A., Alshehri, N., et al. (2024). Exercise as a Therapeutic Intervention for Chronic Disease Management: A Comprehensive Review. Cureus, 16(11), e74165. https://doi.org/10.7759/cureus.74165
Orange, S.T., Dodd, E., Nath, S., et al. (2025/2026). Exercise serum promotes DNA damage repair and remodels gene expression in colon cancer cells. International Journal of Cancer, 158(10), 2641–2649. https://doi.org/10.1002/ijc.70271
American Heart Association journal, Circulation — Dose Response of Incidental Physical Activity Against Cardiovascular Events and Mortality. https://doi.org/10.1161/CIRCULATIONAHA.124.072253
Optimal dosage and modality of exercise on glycemic control in people with prediabetes: a systematic review and network meta-analysis (2025). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12066256/
The Optimal Type and Dose of Exercise Interventions on VEGF Levels in Healthy Individuals, Obesity, and Chronic Disease Populations: A Network Meta-Analysis (2025). Biomedicines. https://doi.org/10.3390/biomedicines13102548
Efficacy and optimal dosage of various exercises for migraine: a multilevel network and dose-response meta-analysis (2025). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12548639/
Optimal dose and type of exercise to improve depressive symptoms in older adults: a systematic review and network meta-analysis. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11157862/
Dose-response-relationship of stabilisation exercises in patients with chronic non-specific low back pain: a systematic review with meta-regression. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7547082/
Exercise-Induced Molecular Adaptations in Chronic Non-Communicable Diseases — Narrative Review (2025/2026). International Journal of Molecular Sciences. https://doi.org/10.3390/ijms262412096
Exercise helps fight bowel cancer — Press release, Newcastle University (2025). https://www.ncl.ac.uk/press/articles/latest/2025/12/exercisehelpsfightbowelcancer/
World Health Organization (2020). WHO Guidelines on Physical Activity and Sedentary Behaviour. British Journal of Sports Medicine, 54, 1451–1462.
Bull, F.C., Al-Ansari, S.S., Biddle, S., et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine.
Cross-Platform Transcriptomic Analysis of 40 Human and Rodent Skeletal Muscle Exerkines (2026). Receptors. https://www.mdpi.com/2813-0413/5/1/15
Short-Lived Exercise-Induced Exerkines Modulate Inflammation for Chronic Disease Prevention: A Systematic Review and Meta-Analysis (2025). Biomolecules. https://www.mdpi.com/2218-273X/15/11/1590
Exosomes and microRNAs: Molecular Mediators Linking Obesity, Exercise, and Metabolic Regulation. Current Diabetes Reports. https://doi.org/10.1007/s11892-025-01608-z
Exercise therapy for chronic symptomatic peripheral artery disease. European Heart Journal, 45(15), 1303–1321.
Optimal aerobic exercise dose for pain relief in fibromyalgia syndrome: a systematic review and meta-analysis. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12719272/