Adipokines & Fatty Liver Disease (MASLD): How Leptin, Adiponectin, and Metabolic Signals Shape Liver Health
Discover how adipokines such as leptin and adiponectin influence fatty liver disease (MASLD). Learn the science behind liver inflammation, fibrosis, and proven ways to restore metabolic health. (157 characters)
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/31/202629 min read
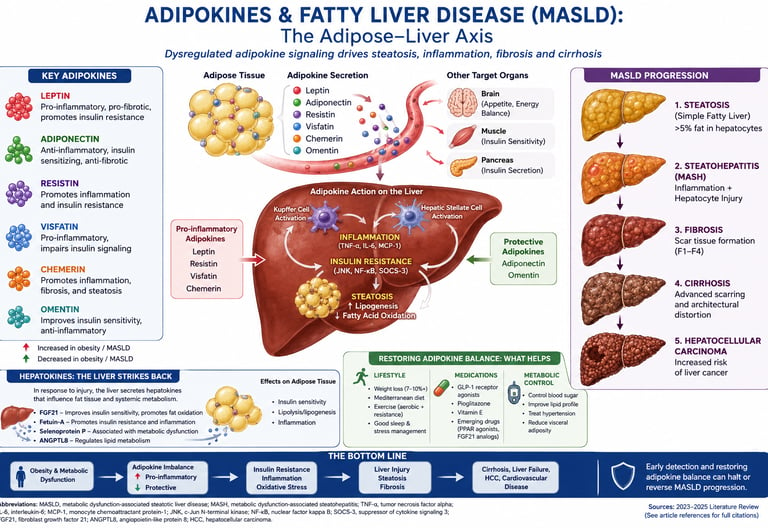
For years, we viewed fat tissue as a passive storage unit. We were wrong. Adipose tissue is a busy endocrine organ, secreting adipokines that directly command liver metabolism (Pezzino et al., 2025). In metabolic dysfunction-associated steatotic liver disease (MASLD), this conversation turns hostile.
Two adipokines dominate the story. Leptin, normally an anti-steatotic signal, becomes a problem when obesity triggers leptin resistance. Circulating levels rise, yet the liver stops listening to leptin's fat-burning message. Meanwhile, leptin keeps activating hepatic stellate cells and Kupffer cells, driving inflammation and fibrosis (Jiménez-Cortegana et al., 2021). A 2024 meta-analysis confirmed that leptin is significantly higher in MASLD patients with fibrosis versus those without (Makri et al., 2024).
At the same time, your liver's best ally goes missing. Adiponectin activates AMPK, burns liver fat, blocks inflammation, and inhibits scarring. But visceral fat expansion suppresses adiponectin secretion (Chen, 2023). The result is a dangerous imbalance: high pro-fibrotic leptin, low hepatoprotective adiponectin. The leptin-to-adiponectin ratio now predicts MASLD severity and liver stiffness independent of age or insulin resistance (Cerabino et al., 2025).
This is not destiny. Losing 7 to 10% body weight through Mediterranean diet and 150 minutes of weekly exercise measurably lowers leptin, raises adiponectin, and can reduce fibrosis (EASL–EASD–EASO, 2024). New drugs like resmetirom and GLP-1 agonists further target these pathways.
The takeaway: MASLD is metabolic cross-talk gone wrong. Restore the adipokine balance, and you give your liver a fighting chance.
Key Points
What are adipokines in MASLD?
Adipokines are hormones released by fat tissue that act on the liver. In MASLD, leptin rises and promotes liver scarring, while protective adiponectin falls, creating a pro-inflammatory, pro-fibrotic environment.
Why is leptin bad for fatty liver disease?
In MASLD, high leptin signals don't curb appetite or burn liver fat due to leptin resistance. Instead, leptin activates liver immune cells and stellate cells, driving inflammation and fibrosis.
What does adiponectin do for the liver?
Adiponectin protects the liver by activating AMPK to burn fat, blocking inflammation, and inhibiting scar tissue formation. MASLD patients have low adiponectin levels, and the drop correlates with disease severity.
What is the leptin-to-adiponectin ratio?
The leptin-to-adiponectin ratio (LAR) reflects adipokine imbalance. A high LAR means elevated pro-fibrotic leptin and low protective adiponectin, and it independently predicts MASLD severity and liver stiffness.
Can you reverse adipokine imbalance in MASLD?
Yes. Losing 7–10% body weight through a Mediterranean diet and regular exercise lowers leptin, raises adiponectin, reduces liver fat, and can even reverse early fibrosis.
Which foods improve adipokines for liver health?
Extra-virgin olive oil, omega-3s, berries, and high-fibre foods raise adiponectin. Added sugar, refined carbs, and excess saturated fat worsen leptin resistance and lower adiponectin.
Do medications help adipokine balance in MASLD?
Resmetirom, GLP-1 agonists, and SGLT-2 inhibitors improve liver fat and insulin sensitivity. They also raise adiponectin levels and are now first-line options for MASH with fibrosis.
1. What Is MASLD? The New Name for Fatty Liver Disease
In 2023, an international consensus of hepatology societies officially renamed non-alcoholic fatty liver disease (NAFLD) to metabolic dysfunction-associated steatotic liver disease (MASLD). The name change was more than semantic — it emphasizes that this is fundamentally a metabolic disease, driven by the same forces behind obesity, type 2 diabetes, and cardiovascular disease.
The Staggering Scale of the Problem
The global burden of MASLD is immense and growing:
1.27 billion people worldwide had MASLD in 2021, according to Global Burden of Disease data
38% of all adults and 7–14% of children currently have MASLD
By 2040, prevalence is projected to exceed 55% of adults
By 2045, an estimated 667 million new cases per year are expected
MASLD has become the top indication for liver transplantation globally
The MASLD Spectrum: From Steatosis to Cirrhosis
MASLD is not a single disease — it is a spectrum:
Simple Steatosis (Fat Accumulation)
What it is: The baseline stage where fat accumulation exceeds 5% of liver cells (hepatocytes), but without active inflammation or cellular damage.
Who it affects: Consistently accounts for ~70–80% of all MASLD patients.
Steatohepatitis (MASH)
What it is: The critical clinical tipping point where hepatic fat is accompanied by cellular ballooning, active tissue inflammation, and ongoing liver cell injury.
Who it affects: Roughly ~20–25% of individuals within the MASLD spectrum.
Progressive Fibrosis (Scarring)
What it is: Chronic inflammation triggers hepatic stellate cells to deposit collagen, creating physical scar tissue across four progressive structural stages (F1 to F3).
Who it affects: Affects an estimated ~10–15% of chronic patients.
Cirrhosis (Advanced Scarring)
What it is: Stage F4 fibrosis, marked by extensive architectural scarring and nodule formation that structurally alters the organ and impairs functional capacity.
Who it affects: Found in ~3–5% of long-term cases.
Hepatocellular Carcinoma (HCC)
What it is: Primary liver cancer that can emerge directly from the hyper-inflammatory, high-turnover environment of cirrhosis or advanced MASH.
Who it affects: A serious, rapidly rising complication worldwide.
What determines who progresses from stage to stage? Increasingly, researchers point to the adipokine imbalance as a critical driver.
2. What Are Adipokines? Fat Tissue as an Endocrine Organ
For decades, adipose (fat) tissue was thought to be inert — just a storage depot for calories. That view was overturned when scientists discovered that fat cells (adipocytes) secrete dozens of biologically active proteins called adipokines (also called adipocytokines).
Adipokines function like hormones — they travel through the bloodstream and regulate:
Appetite and energy expenditure (the brain)
Insulin sensitivity (muscles, liver, fat tissue)
Inflammation (immune cells throughout the body)
Lipid metabolism (fat breakdown and storage)
Liver fibrosis (activation of liver stellate cells)
In a healthy person at a healthy weight, adipokines maintain a careful balance — promoting insulin sensitivity, suppressing inflammation, and protecting the liver from fat overload. In obesity and metabolic disease, this balance collapses. The result is a pro-inflammatory, pro-fibrotic biochemical environment that steadily damages the liver.
Key insight: MASLD is not simply caused by eating too much fat. It is caused by a systemic metabolic dysfunction in which disrupted adipokine signaling creates a hostile environment for the liver.
3. The Six Key Adipokines in MASLD
While over 600 proteins are secreted by adipose tissue, six adipokines have the strongest and best-documented roles in MASLD:
Leptin (↑ Elevated)
Primary Effect on Liver: Drives pro-inflammatory and pro-fibrotic pathways; directly activates Kupffer cells and hepatic stellate cells to deposit scar tissue.
Adiponectin (↓ Decreased)
Primary Effect on Liver: Strongly hepatoprotective and anti-fibrotic; activates AMPK to clear fat out of hepatocytes and dampens inflammatory signaling.
Resistin (↑ Elevated)
Primary Effect on Liver: Accelerates hepatic insulin resistance and fuels local inflammation via the NF-κB cellular pathway.
Visfatin (↑ Elevated)
Primary Effect on Liver: Promotes adipogenesis (fat cell creation) and liver fat accumulation; strongly correlates with advanced fibrosis stages by upregulating TGF-β1.
Chemerin (↑ Elevated)
Primary Effect on Liver: Acts as a potent pro-inflammatory orchestrator, recruiting destructive immune cells directly to liver tissue and driving baseline steatosis.
FGF21 (Context-Dependent / Resistant)
Primary Effect on Liver: Regulates baseline lipid and glucose metabolism; levels rise paradoxically in MASLD due to structural receptor resistance, rendering its protective effects ineffective.The critical insight from 2023–2025 research is that it is not any single adipokine, but the combined imbalance across this network that determines MASLD severity and progression.
4. Leptin: The Double-Edged Sword
Leptin is the most studied adipokine in the context of fatty liver disease — and for good reason. It is one of the most paradoxical molecules in metabolic medicine.
What Leptin Does Normally
In a healthy person, leptin is secreted by fat cells in proportion to how much fat is stored. When fat stores increase, leptin rises, travels to the hypothalamus in the brain, and signals: "Enough — suppress appetite and increase energy expenditure." It acts as a satiety hormone and, importantly, it has anti-steatotic effects on the liver: it promotes fat burning and prevents fat accumulation in hepatocytes.
In people with very little body fat (such as those with rare lipodystrophy conditions), leptin deficiency causes severe liver fat accumulation. Giving these patients leptin as a medication dramatically improves hepatic steatosis — proof of its protective role.
The Leptin Resistance Paradox
Here is where it gets complicated. In obesity and MASLD, leptin levels are chronically elevated, not deficient. Yet the liver and brain stop responding to it — a phenomenon called leptin resistance, directly analogous to insulin resistance.
This creates a tragic paradox:
Leptin levels are high
But the anti-steatotic, appetite-suppressing effects of leptin are lost
Meanwhile, the pro-inflammatory and pro-fibrotic effects of leptin persist and intensify
How Elevated Leptin Damages the Liver
When leptin resistance develops, circulating leptin stops working as a protective signal and starts acting as a driver of liver injury through multiple pathways:
1. Activation of Kupffer Cells (Liver Macrophages) Leptin binds to receptors on Kupffer cells (the liver's resident immune cells) and stimulates them to release tumor necrosis factor-alpha (TNF-α) and other pro-inflammatory cytokines. This creates a sustained inflammatory environment in the liver.
2. Activation of Hepatic Stellate Cells (HSCs) This is perhaps leptin's most dangerous role in MASLD. Leptin directly activates hepatic stellate cells — the main drivers of liver fibrosis — by stimulating them to produce transforming growth factor-beta (TGF-β). TGF-β then triggers a fibrogenic cascade, depositing collagen and scar tissue in the liver.
3. Promotion of Insulin Resistance Elevated leptin amplifies hepatic insulin resistance through JAK2/STAT3 signaling pathways, worsening fat accumulation in the liver.
4. Oxidative Stress Leptin increases reactive oxygen species (ROS) production in liver cells, contributing to cellular damage and progression from simple steatosis to steatohepatitis.
What the Research Shows
A landmark 2024 systematic review and meta-analysis by Makri et al., published in the Journal of Gastroenterology and Hepatology, analyzed 15 studies covering 964 individuals. The findings were striking:
Leptin levels were significantly higher in NAFLD/MASLD patients with liver fibrosis compared to those without fibrosis (SMD: 2.27; 95% CI: 0.81–3.73)
Leptin was also elevated compared to healthy controls without MASLD
The association remained robust across multiple sensitivity analyses
A 2025 cross-sectional FibroScan study by Cerabino et al. published in Nutrients provided real-world confirmation: in 86 overweight and obese patients, each unit increase in leptin was independently associated with increased liver stiffness (β = 0.065; p = 0.038) — a marker of fibrosis — independent of gender, age, and insulin resistance.
Additionally, a 2025 population-based study by Wernly et al. in Endocrine reported that both elevated leptin levels and relative leptin deficiency (low leptin relative to body fat) were associated with steatotic liver disease in the general population, suggesting that the leptin-to-fat-mass ratio may be a more nuanced biomarker than raw leptin levels alone.
Bottom line: In MASLD, leptin is not a helper — it becomes a driver of inflammation and scarring. Normalizing leptin signaling is a key therapeutic goal.
5. Adiponectin: Your Liver's Best Friend
If leptin is the problematic adipokine in MASLD, adiponectin is the protective one — and in obesity and fatty liver disease, it is precisely the one you have too little of.
Adiponectin's Hepatoprotective Actions
Adiponectin is the most abundant adipokine in circulation in healthy individuals. It exerts powerful liver-protective effects through multiple mechanisms:
Anti-steatotic: Adiponectin activates AMPK (AMP-activated protein kinase), the body's master metabolic switch. AMPK activation increases fatty acid oxidation (burning fat for energy), reduces fat synthesis, and directly counteracts hepatic steatosis.
Anti-inflammatory: Adiponectin suppresses TNF-α and IL-6 production, reducing the inflammatory drive toward steatohepatitis.
Anti-fibrotic: Adiponectin inhibits the activation and proliferation of hepatic stellate cells, blocking the fibrotic cascade that leptin promotes.
Insulin-sensitizing: Adiponectin improves insulin signaling in both the liver and peripheral tissues, reducing the hyperinsulinemia that drives fat accumulation.
Why Adiponectin Falls in MASLD
Adiponectin shows an inverse relationship with visceral fat: the more abdominal fat you carry, the lower your adiponectin. This is partly because visceral fat actively suppresses adiponectin secretion through TNF-α and other inflammatory signals.
Clinical studies consistently show that patients with MASLD have low adiponectin, and the reduction is proportional to disease severity. Research published in 2025 confirms that serum adiponectin is negatively correlated with the degree of hepatic steatosis, inflammation, and fibrosis.
The Leptin-to-Adiponectin Ratio: A Critical Biomarker
The leptin-to-adiponectin ratio (LAR) has emerged as a clinically useful tool. In healthy individuals, LAR is low (high adiponectin, modest leptin). In MASLD, LAR rises dramatically as leptin climbs and adiponectin falls.
A rising LAR reflects the convergence of two dangerous forces:
Increasing pro-inflammatory, pro-fibrotic pressure (from leptin)
Decreasing hepatoprotective defense (from falling adiponectin)
Research from 2025 supports LAR as an independent predictor of MASLD severity and metabolic syndrome components, particularly in patients with type 2 diabetes.
Practical note: Ask your doctor about adiponectin and leptin testing if you have MASLD, obesity, or metabolic syndrome. Some specialty labs now offer LAR as a panel.
6. Resistin, Visfatin, Chemerin & More
Beyond the leptin-adiponectin axis, several other adipokines play important and increasingly well-characterized roles in MASLD.
Resistin: The Insulin Resistance Amplifier
What it does: Resistin is a small protein primarily secreted by adipocytes (in rodents) and macrophages (in humans). It directly worsens insulin resistance by increasing glucose production in the liver and reducing insulin sensitivity in peripheral tissues.
In MASLD: Resistin levels are consistently elevated in MASLD patients. A notable study found that resistin had an AUC of 0.997 for predicting MASLD in type 2 diabetes patients — exceptional predictive power — with 96.1% sensitivity and 100% specificity at a specific cut-off. Resistin is also an independent predictor of MASLD by logistic regression analysis.
The mechanism: Resistin activates the NF-κB inflammatory pathway, increasing TNF-α and IL-6 production, fueling the inflammatory cycle that drives steatohepatitis progression.
Visfatin (NAMPT/PBEF): The Fibrosis Promoter
What it does: Visfatin (also known as NAMPT or PBEF) is secreted primarily by visceral fat and is involved in lipid metabolism, immune regulation, and insulin signaling.
In MASLD: Elevated visfatin promotes adipogenesis (creation of new fat cells) and cholesterol accumulation in the liver. It is strongly linked to fibrosis progression — elevated visfatin levels correlate with more advanced fibrosis stages in MASLD patients. Visfatin's pro-fibrotic action is mediated partly through TGF-β1 upregulation.
Chemerin: The Inflammatory Orchestrator
What it does: Chemerin is a chemoattractant protein that recruits immune cells (particularly dendritic cells and macrophages) to adipose tissue and the liver.
In MASLD: Elevated chemerin drives hepatic inflammation by attracting immune cells and activating NF-κB signaling. It correlates with MASLD severity, insulin resistance, and components of metabolic syndrome. Emerging 2024–2025 research suggests chemerin may also modulate the gut microbiome-liver axis.
FGF21 (Fibroblast Growth Factor 21): The Emerging Therapeutic Target
What it does: FGF21 is produced by both the liver (making it a hepatokine) and adipose tissue (making it an adipokine — it bridges both categories). It plays a key role in fatty acid oxidation, ketogenesis, and glucose regulation.
In MASLD: FGF21 levels are paradoxically elevated in MASLD (suggesting FGF21 resistance, similar to leptin and insulin resistance). However, because FGF21 has potent lipid-lowering and anti-inflammatory effects, pharmacological FGF21 analogs are among the most promising drug targets in MASLD treatment, with several in late-stage clinical trials as of 2025.
7. Hepatokines: The Liver Strikes Back
The adipokine story is only half the picture. The liver does not passively receive signals — it sends its own hormone-like proteins back to adipose tissue, the pancreas, muscles, and brain. These are called hepatokines.
In MASLD, the liver's hepatokine output is dysregulated in ways that amplify metabolic dysfunction:
Here is a clean, scannable rewrite of the hepatokine data, organized to highlight how the liver dynamically alters its hormonal output during MASLD:
Dysregulated Hepatokines in MASLD
Fetuin-A (↑ Elevated)
Pathological Effect: Acts as a natural inhibitor of the insulin receptor, directly worsening hepatic and systemic insulin resistance while triggering pro-inflammatory cascades.
FGF21 (↑ Elevated / Resistant)
Pathological Effect: Circulating levels rise paradoxically due to a state of cellular resistance, leading to impaired lipid breakdown and compromised glucose regulation.
Sex Hormone-Binding Globulin / SHBG (↓ Decreased)
Pathological Effect: Production drops sharply as liver fat increases, serving as a reliable systemic biomarker for heightened cardiometabolic and type 2 diabetes risk.
Selenoprotein P (↑ Elevated)
Pathological Effect: Accelerates systemic glucotoxicity by actively driving insulin resistance in both liver tissue and skeletal muscle.
Angiopoietin-like 3 / ANGPTL3 (↑ Elevated)
Pathological Effect: Suppresses lipoprotein lipase activity, which severely impairs peripheral lipid clearance and drives up circulating triglycerides.
LECT2 (↑ Elevated)
Pathological Effect: Secreted heavily by fatty liver tissue, traveling through circulation to selectively block insulin signaling in skeletal muscle tissue.
Clinical Pearl: This dysregulated output creates a destructive cross-talk feedback loop. The fatty liver secretes elevated Fetuin-A and LECT2, which lock down insulin receptors in muscles and fat tissue. This systemic insulin resistance forces peripheral fat stores to break down and flood the portal vein with even more free fatty acids, worsening the liver's fat burden.Fetuin-A: The Hepatokine Villain
Among hepatokines, fetuin-A has attracted the most research attention in MASLD. It acts as a natural inhibitor of the insulin receptor — essentially blocking insulin's ability to signal properly.
Elevated fetuin-A in MASLD:
Worsens hepatic and systemic insulin resistance
Activates toll-like receptor 4 (TLR4), triggering inflammatory cascades
Promotes lipid accumulation through impaired fatty acid signaling
A 2025 bibliometric analysis by Pezzino et al. in Biomedicines confirmed that fetuin-A has become a central research theme in MASLD, clustering alongside insulin resistance, steatosis, and lipodystrophy as one of the core "motor" themes driving the field forward.
The Adipokine-Hepatokine Feedback Loop
This is the key concept that helps explain why MASLD is so hard to reverse once established:
Visceral fat ↑ → leptin ↑, adiponectin ↓ → liver inflammation and insulin resistance ↑ → liver releases fetuin-A, ANGPTL3 → adipose tissue further dysregulated → more leptin, less adiponectin → worse liver injury → cycle repeats
Breaking this cycle at multiple points is what effective MASLD treatment aims to achieve.
8. How Adipokines Drive MASLD Progression Step by Step
Understanding the adipokine-driven progression of MASLD requires seeing the disease as a multi-hit process — not a single insult, but a cascade of metabolic failures that build on each other.
Step 1: The First Hit — Hepatic Steatosis
It begins with excess caloric intake, particularly from refined carbohydrates and saturated fats, combined with physical inactivity. Visceral fat expands. As it does:
Leptin rises but the liver becomes resistant to its anti-steatotic signals
Adiponectin falls, removing AMPK-driven fat oxidation in the liver
Free fatty acid (FFA) flux to the liver increases as adipose tissue lipolysis rises
Insulin resistance causes the liver to produce more fat (de novo lipogenesis)
Fat accumulates in hepatocytes → hepatic steatosis
Step 2: The Second Hit — Inflammation (Steatohepatitis)
With steatosis established, the adipokine imbalance drives the inflammatory "second hit":
Elevated leptin activates Kupffer cells → TNF-α, IL-6, IL-1β production
Elevated resistin and chemerin recruit additional inflammatory immune cells
Falling adiponectin removes its anti-inflammatory brake
Oxidative stress from fatty acid overload generates reactive oxygen species
Result: MASH (metabolic-associated steatohepatitis)
Step 3: Fibrosis — Scar Tissue Replaces Liver Cells
This is the critical juncture. Once hepatic stellate cells (HSCs) are activated, the liver begins to scar:
Leptin directly activates HSCs via TGF-β1 signaling
Visfatin amplifies TGF-β1 production
Falling adiponectin removes its anti-fibrotic inhibition of HSC proliferation
Collagen deposition accelerates → fibrosis, then cirrhosis
Clinical pearl: Leptin's pro-fibrotic effect on hepatic stellate cells may be one of the most important therapeutic targets for preventing liver cirrhosis in MASLD patients.
Step 4: End-Stage Liver Disease
Progressive cirrhosis leads to portal hypertension, liver failure, and — in a proportion of patients — hepatocellular carcinoma (HCC). MASLD is now the fastest-growing cause of HCC globally.
9. Evidence Summary: Key Studies at a Glance
Here is a clean, scannable rewrite of the evidence summary, formatted to highlight the clinical weight and design of each study:
Makri et al. (2024)
Design: Systematic review + meta-analysis
Key Finding: Circulating leptin is significantly higher in MASLD patients with active liver fibrosis compared to non-fibrotic controls (SMD 2.27).
Design: Population-based large cohort study.
Key Finding: Both baseline elevated leptin levels and a state of relative leptin deficiency are independently associated with steatotic liver disease in the general population.
Cerabino et al. (2025)
Design: FibroScan-based cross-sectional study
Key Finding: Each unit increase in circulating leptin is independently associated with a direct increase in liver stiffness a validated marker of tissue fibrosis.
Pezzino et al. (2025)
Design: Large-scale bibliometric analysis.
Key Finding: Identifies the tracking of leptin, adiponectin, and FGF21 as the primary "motor" themes and core research drivers in the metabolic liver disease field.
De la Cruz-Color et al. (2024)
Design: Human tissue extraction and expression study.
Key Finding: Confirms that peripheral leptin resistance localized within omental (visceral) fat and liver tissue directly correlates with MASLD severity.
Alam et al. / Frontiers (2025)
Design: Comprehensive physiological review.
Key Finding: Establishes that the structural leptin-to-adiponectin ratio (LAR) imbalance serves as the central driver for progression from simple fat to active tissue inflammation.
Design: Target cross-sectional cohort study.
Key Finding: Resistin demonstrated exceptional predictive accuracy for MASLD in Type 2 Diabetes patients (AUC 0.997); both low adiponectin and high resistin serve as strong independent predictors.
Chen / Tung's Medical Journal (2023)
Design: Clinical endocrine review.
Key Finding: Maps out how a dysregulated network of peripheral adipokines—specifically leptin, adiponectin, resistin, and visfatin—orchestrates baseline metabolic liver disease.
Jiménez-Cortegana et al. (2021)
Design: Mechanistic molecular review.
Key Finding: Delineates the exact cellular pathways where leptin promotes MASLD via localized Kupffer cell activation, hepatic stellate cell (HSC) stimulation, and downstream TGF-beta fibrotic signaling.
📝 Abbreviation Key: SMD = Standardized Mean Difference; AUC = Area Under the Receiver Operating Characteristic curve; HSC = Hepatic Stellate Cells; T2DM = Type 2 Diabetes Mellitus.Note: SMD = standardized mean difference; AUC = area under the receiver operating characteristic curve; HSC = hepatic stellate cells
10. Diagnosing Adipokine Imbalance: Biomarkers & Tests
Most patients with MASLD are unaware of their adipokine status. Standard liver function tests (ALT, AST) often miss early-stage disease, and even imaging (ultrasound) can be insensitive. Here is what the science says about emerging adipokine-based diagnostics:
Currently Available Tests
Serum leptin: Measurable via standard blood test. Elevated levels in the context of obesity and liver disease suggest leptin resistance. Normal ranges vary by sex (women have higher levels than men due to hormonal differences).
Serum adiponectin: A key protective marker. Low adiponectin (below ~6–7 μg/mL in many references) is associated with insulin resistance, metabolic syndrome, and MASLD. Declining adiponectin with rising BMI is a red flag.
Leptin-to-adiponectin ratio (LAR): An elevated LAR (>1 in many studies, though cut-offs vary) is associated with higher MASLD risk and severity.
Fetuin-A: Increasingly ordered in metabolic research settings. Elevated fetuin-A correlates with insulin resistance and MASLD.
FibroScan (liver elastography): While not an adipokine test itself, FibroScan is now the gold standard non-invasive method for assessing liver stiffness (fibrosis) and controlled attenuation parameter (CAP, for steatosis). The 2025 Cerabino study used FibroScan to directly link leptin levels to liver fibrosis.
Practical Checklist: What to Ask Your Doctor
If you have MASLD, obesity, type 2 diabetes, or metabolic syndrome, consider discussing these tests:
[ ] Fasting serum leptin
[ ] Serum adiponectin (or leptin/adiponectin ratio)
[ ] Fasting insulin + HOMA-IR (insulin resistance score)
[ ] Full liver function panel (ALT, AST, GGT, alkaline phosphatase, bilirubin)
[ ] Lipid panel (especially triglycerides and HDL)
[ ] Liver ultrasound or FibroScan
[ ] HbA1c and fasting glucose
⚠️ Important: These tests should be interpreted by a physician or hepatologist in the context of your full clinical picture. Adipokine testing is not yet routinely standardized across all labs.
11. Lifestyle Interventions That Restore Adipokine Balance
Here is the most empowering part of this guide: the adipokine imbalance in MASLD is not fixed. Diet, exercise, and weight loss have profound and measurable effects on adipokine levels and liver health. You have significant control here.
Weight Loss: The Most Powerful Intervention
Weight loss — particularly loss of visceral fat — is the single most effective way to restore adipokine balance:
5–7% body weight loss: Improves liver steatosis, begins to lower leptin, raises adiponectin
7–10% loss: Significant reduction in liver inflammation (MASH improvement)
>10% loss: Can produce fibrosis regression in some patients
The mechanism is direct: as visceral fat mass decreases, leptin production falls and adiponectin secretion increases. The liver's hostile adipokine environment normalizes.
Dietary Approaches
Mediterranean Diet (strongest evidence):
The Mediterranean diet — rich in olive oil, vegetables, legumes, whole grains, fish, and nuts — consistently reduces liver fat and improves adipokine profiles. It:
Raises adiponectin
Reduces inflammatory cytokines (TNF-α, IL-6)
Improves insulin sensitivity
Reduces hepatic de novo lipogenesis
Key foods for adipokine balance:
Here is a clean, point-by-point rewrite of the dietary components, mapping out exactly how specific foods and eating patterns modulate your systemic adipokine network:
Extra-Virgin Olive Oil
Systemic Effect: Actively drives up protective adiponectin levels while suppressing inflammatory resistin.
Scientific Evidence: Strong. It forms the foundational fat source of the evidence-backed Mediterranean dietary pattern.
Omega-3 Fatty Acids (Fatty Fish, Flaxseed, Walnuts)
Systemic Effect: Promotes an increase in anti-inflammatory adiponectin while lowering excessive, pro-fibrotic circulating leptin.
Scientific Evidence: Moderate-to-Strong. Essential for down-regulating systemic lipid-induced stress.
Berries and Polyphenol-Rich Foods
Systemic Effect: Boosts circulating adiponectin expression and systematically blunts downstream inflammatory cytokines like TNF-$\alpha$.
Scientific Evidence: Moderate. Helps neutralize oxidative stress within hepatocytes.
Refined Carbohydrates & Added Sugars
Systemic Effect: Aggressively fuels peripheral leptin resistance and causes a sharp drop in protective adiponectin.
Scientific Evidence: Strong (Critical to Avoid). Directly drives the hyperinsulinemia that forces the liver to synthesize new fat.
Liquid Fructose (Sugary Drinks, High-Fructose Corn Syrup)
Systemic Effect: Bypasses normal metabolic regulation to directly trigger de novo lipogenesis (the liver creating fat directly from sugar), bypassing protective adipokine brakes.
Scientific Evidence: Strong (Critical to Avoid). One of the fastest clinical drivers of MASH and hepatic fat accumulation.
Excessive Saturated Fats
Systemic Effect: Elevates circulating leptin to pathological levels while driving down baseline adiponectin production.
Scientific Evidence: Moderate (Important to Limit). High intake compromises liver mitochondrial efficiency and worsens insulin resistance.
Soluble and Prebiotic Dietary Fiber
Systemic Effect: Optimizes the short-chain fatty acid profile of the gut microbiome, which indirectly raises adiponectin and repairs the gut-liver axis barrier.
Scientific Evidence: Emerging. A key target of current metabolic and microbiome research.
Practical 7-day eating framework for MASLD:
Breakfast: Greek yogurt with berries + walnuts; or oatmeal with olive oil-drizzled avocado
Lunch: Large salad with olive oil, chickpeas, tuna or salmon, leafy greens
Dinner: Baked salmon or sardines, roasted vegetables, small portion brown rice or quinoa
Snacks: Handful of almonds; hummus with vegetables; a piece of whole fruit
Avoid: Sugary drinks, ultra-processed foods, white bread/pasta in excess, alcohol
⚠️ Alcohol note: Alcohol is explicitly excluded from MASLD by diagnostic criteria (>14 units/week for women, >21 for men). Even moderate alcohol consumption can worsen liver inflammation and fibrosis in susceptible individuals.
Exercise: A Targeted Adipokine Modulator
Exercise is one of the most potent modulators of adipokine balance, independent of weight loss:
Aerobic exercise (walking, cycling, swimming):
Directly increases adiponectin expression in adipose tissue
Reduces leptin levels by improving leptin sensitivity
Decreases liver fat even without major weight change
Resistance training (weights, bodyweight exercise):
Increases muscle mass, which improves glucose disposal and reduces insulin resistance
Reduces visceral fat more effectively than aerobic exercise in some studies
Raises adiponectin levels
Evidence-based exercise prescription for MASLD:
Training Modality (Type)
Recommendation: A deliberate combination of both aerobic cardio and progressive resistance training.
Clinical Rationale: Aerobic exercise excels at clearing intrahepatic fat, while resistance training builds skeletal muscle mass—the body's primary sink for glucose disposal—effectively lowering systemic insulin resistance.
Weekly Frequency
Recommendation: Engage in aerobic training ≥ 5 days per week, coupled with dedicated resistance sessions 2 to 3 days per week.
Clinical Rationale: Frequent physical stimulus keeps insulin receptors highly sensitive and maintains optimal daily fatty acid oxidation (fat burning).
Target Duration
Recommendation: Accumulate 150 to 300 minutes per week of moderate-intensity aerobic exercise.
Clinical Rationale: This volume aligns with international hepatology guidelines to systematically reduce liver volume and visceral fat mass.
Target Intensity
Recommendation: Maintain a baseline Moderate Intensity (60%–70% of your maximum heart rate) at a minimum, stepping up to Vigorous Intensity if clinically tolerated.
Clinical Rationale: Sustaining heart rate within this metabolic window directly optimizes mitochondrial function inside your hepatocytes (liver cells).
Clinical Pearl: The Value of Daily Walking
Key Takeaway: Even a simple 30-minute daily brisk walk significantly reduces liver fat.
Clinical Rationale: You do not need to train like an elite athlete to see results. Consistent, low-impact movement mobilizes visceral fat stores and improves your leptin-to-adiponectin ratio, even if the number on the scale doesn't budge immediately.📊 Insert infographic: Exercise effects on leptin, adiponectin, and liver fat — before vs. after 12 weeks
Sleep and Stress: The Underappreciated Factors
Chronic sleep deprivation and psychological stress both dysregulate adipokines:
Short sleep (<6 hours/night) increases leptin dysregulation, raises cortisol (which drives visceral fat accumulation), and worsens insulin resistance
Chronic psychological stress elevates cortisol → promotes visceral adiposity → worsens adipokine balance
Interventions: Aim for 7–9 hours of quality sleep; consider mindfulness-based stress reduction (MBSR) or cognitive behavioral therapy for chronic stress
12. Medications & Emerging Therapies Targeting Adipokines {#medications}
The field of MASLD pharmacotherapy has advanced rapidly. In 2024, the FDA approved resmetirom (Rezdiffra) — the first drug specifically approved for MASH with fibrosis — and several other agents targeting the adipokine-hepatokine axis are in late-stage trials.
Currently Approved Medications (2025)
Resmetirom (Rezdiffra): A thyroid hormone receptor-beta agonist that activates metabolic pathways in the liver, reducing liver fat and improving fibrosis. It indirectly improves adipokine balance by reducing liver fat burden.
GLP-1 receptor agonists (semaglutide, liraglutide): Though approved primarily for diabetes (semaglutide also for obesity), these drugs substantially reduce liver fat, improve insulin resistance, and have been shown to raise adiponectin levels. Semaglutide is in Phase 3 trials specifically for MASH.
SGLT-2 inhibitors (empagliflozin, dapagliflozin): A 2025 meta-analysis of 16 RCTs (n=11,300) found SGLT-2 inhibitors significantly improved liver stiffness and steatosis in MASLD patients. These drugs also improve adiponectin levels.
Emerging Therapies Targeting the Adipokine Axis
FGF21 Analogs (Phase 2/3 Clinical Trials)
Candidate Agents: Efruxifermin (currently in late-stage Phase 3 trials), Pegbelfermin.
Therapeutic Action: Overcomes systemic FGF21 resistance to lower liver fat, improve insulin sensitivity, and directly blunt the activation of tissue-scarring cells.
Pan-PPAR Agonists (Phase 3 Clinical Trials)
Candidate Agent: Lanifibranor (broadly activating the alpha, delta, and gamma receptors).
Therapeutic Action: Simultaneously targets three critical areas: it clears out baseline liver fat, corrects peripheral fat tissue dysfunction, and directly blocks the pathways that deposit scar tissue in the liver.
Adiponectin Receptor Agonists (Preclinical to Phase 1)
Candidate Agents: Developing small-molecule mimics.
Therapeutic Action: Artificially replaces missing adiponectin levels to restore its anti-inflammatory, fat-burning, and liver-protective benefits.
Anti-Leptin Signaling Agents (Early Research Phase)
Candidate Agents: Experimental monoclonal antibodies and receptor blockers.
Therapeutic Action: Aims to safely block leptin's pro-fibrotic signaling on hepatic stellate cells to halt the progression of advanced liver scarring without disrupting normal metabolic balance.
Chemerin Antagonists (Preclinical Phase)
Candidate Agents: Early-stage small molecules and peptide blockers.
Therapeutic Action: Blocks chemerin receptors to prevent the recruitment of inflammatory immune cells directly into the liver, short-circuiting steatohepatitis progression.⚠️ Consult your doctor before starting any medication. This section is educational only. The right treatment for MASLD depends on your stage of disease, comorbidities, and individual risk profile.
13. Common Myths & Mistakes
Understanding adipokines in MASLD also means recognizing common misconceptions that can lead patients and practitioners astray.
Myth #1: "Fatty liver only happens in people who drink heavily"
False. MASLD, by definition, occurs in people who drink little or no alcohol. It is driven by metabolic factors — diet, obesity, insulin resistance, and adipokine dysregulation — not alcohol consumption. MASLD is now far more prevalent than alcohol-related liver disease globally.
Myth #2: "Leptin supplements can cure fatty liver"
False. While leptin deficiency (an extremely rare condition) does cause liver fat accumulation, the overwhelming majority of MASLD patients have leptin excess with leptin resistance — not deficiency. Taking additional leptin would worsen the situation by increasing inflammation and fibrosis signals.
Myth #3: "If my ALT is normal, my liver is fine"
Dangerous myth. ALT (a liver enzyme commonly tested in blood panels) can be normal even with significant liver fat accumulation or early fibrosis. Many MASLD patients with advanced fibrosis have normal or near-normal ALT. A comprehensive assessment, including imaging and adipokine biomarkers is far more informative.
Myth #4: "Adiponectin supplements can raise my levels"
Largely false. No commercially available supplement reliably raises adiponectin to therapeutic levels. However, certain dietary components (omega-3s, polyphenols from olive oil and berries, magnesium, specific plant extracts) have shown modest effects in some studies. Weight loss and exercise remain the most evidence-backed approaches.
Myth #5: "Once you have MASLD, fibrosis is inevitable"
False. Liver fibrosis can regress with sustained lifestyle change and appropriate medical management. Multiple studies document fibrosis improvement (regression of one or more stages) with significant weight loss (>10%) and disease-modifying medications. Early intervention is critical, but it is never too late to act.
Myth #6: "MASLD is not serious if you feel fine"
Dangerous. MASLD is largely asymptomatic until advanced stages. Most patients with significant fibrosis have no symptoms. The absence of symptoms does not mean the disease is not progressing silently. This is why proactive screening and monitoring are essential in at-risk individuals.
14. FAQs
Q1: What is the difference between MASLD and NAFLD?
MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease) is the new name for NAFLD (Non-Alcoholic Fatty Liver Disease), adopted in 2023 by international hepatology societies. The new term better reflects the metabolic nature of the disease and requires the presence of at least one metabolic risk factor (overweight/obesity, type 2 diabetes, high blood pressure, elevated triglycerides, or low HDL cholesterol) alongside liver fat accumulation. The underlying biology is the same; the name change is designed to reduce stigma and improve diagnostic precision.
Q2: Can a blood test detect adipokine imbalance in MASLD?
Yes, though not all these tests are routinely ordered. Serum leptin, serum adiponectin, and the leptin-to-adiponectin ratio can be measured through specialty blood tests. Elevated leptin combined with low adiponectin — particularly with an elevated LAR — is associated with MASLD severity and liver fibrosis risk. Talk to a hepatologist or metabolic specialist about whether these tests are appropriate for your situation.
Q3: Does losing weight really improve adipokine levels?
Yes — significantly. Even modest weight loss (5–7% of body weight) measurably reduces leptin and raises adiponectin, particularly when the weight lost is from visceral fat stores. Weight loss is the most powerful known intervention for restoring adipokine balance and reducing liver fat. The effects are further amplified by the type of diet used (Mediterranean-style is superior to low-fat diets in head-to-head comparisons for liver outcomes).
Q4: Can children develop adipokine-driven MASLD?
Yes. MASLD affects 7–14% of children and adolescents globally, with higher rates in those with obesity. The same adipokine mechanisms operate in children — elevated leptin with leptin resistance and low adiponectin are observed in pediatric MASLD. This is alarming because early-onset MASLD gives the disease more time to progress. Lifestyle intervention (diet, exercise, reduced screen time) is the primary treatment in pediatric cases.
Q5: Is the leptin-adiponectin ratio tested routinely?
Not yet in most clinical settings, but it is increasingly used in research and by metabolic medicine specialists. Given the evidence linking the LAR to MASLD severity and metabolic risk, some experts advocate for its inclusion in metabolic syndrome screening panels. If you have MASLD or significant metabolic risk factors, it is worth discussing with your doctor.
Q6: Can exercise raise adiponectin levels even without weight loss?
Yes. Multiple studies show that regular aerobic and resistance exercise raises adiponectin levels independently of weight change. The mechanism involves exercise-induced AMPK activation in muscle and adipose tissue, which stimulates adiponectin gene expression. This means even people who do not lose significant weight can benefit liver health through regular physical activity.
Q7: What role does the gut microbiome play in adipokine regulation?
The gut-liver-adipose axis is an emerging frontier in MASLD research. Gut microbiome dysbiosis (reduced diversity and overgrowth of harmful bacteria) directly affects adipokine signaling:
Certain bacteria produce short-chain fatty acids that stimulate adiponectin production
Gut-derived endotoxins (LPS) activate TLR4 on liver cells, amplifying leptin's pro-inflammatory effects
Microbiome diversity correlates inversely with MASLD severity Interventions like Mediterranean diet, probiotics, and prebiotic fiber help restore beneficial microbiome composition, improving adipokine balance indirectly.
Q8: Is MASLD reversible at the fibrosis stage?
Fibrosis (stages F1–F2) can often be reversed with sustained, significant weight loss (>10%) and disease-modifying medications. Even F3 fibrosis regression has been documented with aggressive intervention. Advanced cirrhosis (F4) is generally not reversible but its progression and complications can be slowed. This is why early detection and intervention is critical — fibrosis grade is the strongest predictor of long-term liver-related outcomes.
Q9: Are there genetic factors that affect adipokine levels?
Yes. Several genetic variants influence adipokine levels and MASLD susceptibility. The PNPLA3 I148M variant — the strongest known genetic risk factor for MASLD — affects liver fat metabolism and modifies the response to adipokine signaling. Variants in the adiponectin gene (ADIPOQ) also influence circulating adiponectin levels. Genetic testing for MASLD risk is not yet standard practice but is being studied.
Q10: Can intermittent fasting help MASLD by improving adipokines?
Emerging evidence suggests yes. Time-restricted eating and other forms of intermittent fasting reduce liver fat, improve insulin sensitivity, and have been shown in some studies to raise adiponectin and reduce leptin. However, most studies are short-term and in small populations. Intermittent fasting is not recommended for everyone (e.g., those with diabetes on insulin should consult their physician). The Mediterranean diet with reduced caloric density remains the most evidence-backed dietary approach.
Q11: What is the role of adipokines in the gender difference in MASLD?
MASLD prevalence and severity differ between men and women. Men tend to develop MASLD at lower BMI levels, while women are more protected pre-menopause (due to estrogen's favorable effects on adiponectin). Post-menopausal women show accelerated MASLD risk as estrogen falls and adipokine balance shifts. The gender difference in leptin levels (women naturally have higher leptin than men for the same fat mass) also creates sex-specific diagnostic thresholds.
Q12: How do I know if I'm at risk for MASLD and adipokine imbalance?
You are at higher risk if you have:
Obesity (especially abdominal/visceral fat)
Type 2 diabetes or prediabetes
Metabolic syndrome (combination of high BP, high triglycerides, low HDL, and insulin resistance)
Hypothyroidism
Polycystic ovary syndrome (PCOS)
Family history of liver disease or type 2 diabetes
Sedentary lifestyle with high refined carbohydrate/sugar diet
If two or more of these apply to you, discuss MASLD screening with your physician.
15. Clinical pearls
1. The Visceral Fat "Signal Jammer"
When you carry excess fat around your midsection (visceral fat), it acts like a signal jammer for your liver's health defenses. Visceral fat actively suppresses your body's production of adiponectin—your liver’s premier anti-inflammatory and fat-burning hormone. Think of weight loss not just as shedding pounds, but as turning off the jammer so your liver can finally hear the protective signals it needs to heal.
2. The Leptin Resistance Paradox
Leptin is famously known as the satiety hormone that tells your brain you are full, while simultaneously prompting your liver to burn off excess fat cells. However, in advanced MASLD, leptin levels become chronically elevated to the point where your liver develops leptin resistance. The protective fat-burning signal is entirely lost, but leptin's darker, pro-inflammatory side remains highly active—actively driving liver scarring (fibrosis).
3. Normal Liver Enzymes Can Blindside You
One of the most dangerous traps in hepatology is relying solely on standard blood panels. You can have an entirely normal ALT (alanine aminotransferase) level and still have silent, progressing liver fat accumulation or early-stage tissue scarring. If you have metabolic risk factors like Type 2 diabetes or insulin resistance, demand advanced non-invasive testing like a FibroScan or an adipokine biomarker panel.
4. Sweat Out the Fat, Even Without Weight Loss
If the scale isn't moving, do not lose heart. Clinical data demonstrates that consistent aerobic and resistance exercise significantly improves your leptin-to-adiponectin ratio (LAR) and reduces liver fat even if you don't lose a single pound. Muscle tissue acts as a metabolic sink for circulating sugars and fats, taking immense workload off an overstressed liver.
5. Resistin is the Link Between Your Liver and Diabetes
Resistin is an inflammatory adipokine that acts as a direct molecular bridge between fatty liver disease and Type 2 diabetes. It locks down your liver's insulin receptors, forcing your pancreas to pump out more insulin, which in turn signals the liver to produce even more fat (de novo lipogenesis). Lowering resistin requires cutting down on ultra-processed foods and high-fructose corn syrup, which fuel this vicious loop.
6. Residual Heat: The Golden 10% Weight Loss Threshold
While losing 5% of your body weight is enough to start clearing basic fat accumulation (steatosis) out of liver cells, crossing the 10% weight loss threshold is where the true biological magic happens. At 10%, the systemic adipokine network normalizes deeply enough to trigger fibrosis regression—meaning your body can actually begin dismantling and healing existing scar tissue.
16. Conclusion & Action Steps
MASLD is not simply a disease of eating too much fat. It is a metabolic disease driven by a profound disruption in the hormonal conversation between your fat tissue and your liver. Adipokines — particularly the leptin-adiponectin imbalance — sit at the heart of this disruption, driving fat accumulation, inflammation, and fibrosis in a self-perpetuating cycle.
The good news is that this cycle is not irreversible. Science has given us a clear roadmap:
Your 6-Step Action Plan
Get tested. If you have risk factors (obesity, diabetes, metabolic syndrome), ask your doctor about liver function tests, fasting insulin, HbA1c, and consider adiponectin and leptin testing. A FibroScan may be appropriate.
Target visceral fat. This is the primary source of the leptin-adiponectin imbalance. Even 5–7% body weight loss significantly improves liver health.
Adopt a Mediterranean-style diet. Prioritize olive oil, fish, vegetables, legumes, whole grains, and nuts. Aggressively reduce added sugars, refined carbohydrates, and ultra-processed foods.
Exercise consistently. Aim for 150–300 minutes per week of moderate-intensity aerobic exercise, plus 2–3 sessions of resistance training. This directly raises adiponectin independent of weight loss.
Optimize sleep and manage stress. Both are underappreciated drivers of adipokine dysregulation and visceral fat accumulation.
Work with a specialist. A hepatologist, endocrinologist, or metabolic medicine specialist can guide your care, recommend appropriate medications (if needed), and monitor your disease progression with the right tools.
Remember: MASLD is often silent until late stages. Do not wait for symptoms — act on your risk factors now.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of liver disease or any other medical condition.
Related Articles
How to Reverse Hepatic Insulin Resistance Naturally: Science-Backed Diet, Exercise and Supplements
De Novo Lipogenesis Explained: How Sugar Turns Into Liver Fat and High Triglycerides
Rethinking Dietary Fats: What New Research Reveals About Plant vs. Animal Fats | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
References
Adinolfi, L. E., Marrone, A., Rinaldi, L., Zampino, R., Guerrera, B., & Restivo, L. (2025). Metabolic dysfunction-associated steatotic liver disease (MASLD): A systemic disease with a variable natural history and challenging management. Explore Medicine, 6, Article 1001281. https://doi.org/10.37349/emed.2025.1001281
Alam, M. A., et al. (2025). Metabolic dysfunction associated fatty liver disease and type 2 diabetes: Pathophysiological links, epidemiological trends, and clinical implications. Frontiers in Endocrinology, 16, Article 1669478. https://doi.org/10.3389/fendo.2025.1669478
Casella, G., et al. (2025). Role of perturbated hemostasis in MASLD and its correlation with adipokines. Biomedicines, 13(2), Article 345. https://pmc.ncbi.nlm.nih.gov/articles/PMC10820028/
Cerabino, N., Di Chito, M., Guido, D., Zupo, R., Castellana, F., Lampignano, L., Sardone, R., Giannelli, G., & De Perpetua, G. (2025). Liver fibrosis is positively and independently associated with leptin circulating levels in individuals that are overweight and obese: A FibroScan-based cross-sectional study. Nutrients, 17(11), Article 1908. https://doi.org/10.3390/nu17111908
Chen, C. (2023). The role of adipokines in the disease of metabolic-associated fatty liver disease. Tungs' Medical Journal, 17(2), 49–52. https://doi.org/10.4103/ETMJ.ETMJ-D-23-00015
De la Cruz-Color, L., Dominguez-Rosales, J. A., Maldonado-González, M., et al. (2024). Evidence that peripheral leptin resistance in omental adipose tissue and liver correlates with MASLD in humans. International Journal of Molecular Sciences, 25(12), Article 6420. https://doi.org/10.3390/ijms25126420
Dua, A., Kumari, S., Singh, R., Kumar, A., Pradeep, P., Ojesina, A. I., & Kumar, A. (2025). Metabolic dysfunction-associated steatotic liver disease (MASLD): The interplay of gut microbiome, insulin resistance, and diabetes. Frontiers in Medicine, 12, Article 1618275. https://doi.org/10.3389/fmed.2025.1618275
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), & European Association for the Study of Obesity (EASO). (2024). EASL–EASD–EASO clinical practice guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Journal of Hepatology, 80(4), 782–819. https://doi.org/10.1016/j.jhep.2023.10.035
Jiménez-Cortegana, C., García-Galey, A., Tami, M., Del Pino, P., Carmona, I., López, S., Alba, G., & Sánchez-Margalet, V. (2021). Role of leptin in non-alcoholic fatty liver disease. Biomedicines, 9(7), Article 762. https://doi.org/10.3390/biomedicines9070762
Lee, W. H., Kipp, Z. A., Bates, E. A., et al. (2025). The physiology of MASLD: Molecular pathways between liver and adipose tissues. Clinical Science, 139(18), 1015–1046. https://doi.org/10.1042/CS20257571
Ma, Y., et al. (2025). Metabolic dysfunction-associated steatotic liver disease: Pathogenesis, model and treatment (Review). International Journal of Molecular Medicine, 55(3), Article 45. https://pmc.ncbi.nlm.nih.gov/articles/PMC12549077/
Makri, E. S., Evripidou, K., & Polyzos, S. A. (2024). Circulating leptin in patients with nonalcoholic fatty liver disease-related liver fibrosis: A systematic review and a meta-analysis. Journal of Gastroenterology and Hepatology, 39(5), 806–817. https://doi.org/10.1111/jgh.16480
Pezzino, S., Puleo, S., Luca, T., Castorina, M., & Castorina, S. (2025). Adipokine and hepatokines in metabolic dysfunction-associated steatotic liver disease (MASLD): Current and developing trends. Biomedicines, 13(8), Article 1854. https://doi.org/10.3390/biomedicines13081854
Polyzos, S. A., & Mantzoros, C. S. (2022). Adiponectin as a target for the treatment of nonalcoholic steatohepatitis with thiazolidinediones: A systematic review. Metabolism, 65(9), 1297–1306.
Schoettler, N., et al. (2025). Metabolic dysfunction-associated steatotic liver disease (MASLD) in children with obesity. Obesity Pillars, 14, Article 100167. https://doi.org/10.1016/j.obpill.2025.100167
Wang, Y., et al. (2025). Global burden of MASLD 1990–2021 to 2045: Projections from global burden of disease study data. Annals of Hepatology, 24, Article 101782. https://doi.org/10.1016/j.aohep.2025.101782
Wernly, B., Beghini, M., Semmler, G., et al. (2025). Association of leptin levels and relative leptin deficiency with steatotic liver disease in the general population. Endocrine, 90(3), 1263–1274. https://doi.org/10.1007/s12020-025-04429-y
Younossi, Z. M., et al. (2025). Epidemiology of metabolic dysfunction-associated steatotic liver disease. Clinical and Molecular Hepatology, 31(Suppl. 1), S32–S50. https://doi.org/10.3350/cmh.2024.0431
Zhai, L., et al. (2024). Adipocytokines as predictors of metabolic dysfunction-associated steatotic liver disease (MASLD) in type 2 diabetes mellitus (T2DM). BMC Endocrine Disorders, 24, Article 45. https://pmc.ncbi.nlm.nih.gov/articles/PMC10917643/
Zhang, X., et al. (2025). SGLT-2 inhibitors meta-analysis in MASLD: Effect on liver fibrosis progression: 16 RCTs, n=11,300. Frontiers in Pharmacology, 16, Article 12864. https://pmc.ncbi.nlm.nih.gov/articles/PMC12864471/Last updated: May 2026 | This article will be reviewed and updated as new research is published.
Found this article helpful? Share it with someone managing liver disease or metabolic health. Bookmark it for reference — it will be updated as the science evolves.