Why Strength Training Reduces Inflammation—and May Prevent Most Chronic Diseases
Chronic inflammation drives disease. Learn how resistance training reduces CRP, IL-6, and TNF-α—and why it matters for your health.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/2/202615 min read
Does resistance training reduce inflammation?
Yes. Multiple meta-analyses (2025) show that resistance training significantly lowers inflammatory biomarkers such as CRP, IL-6, and TNF-α, which are linked to cardiovascular disease, diabetes, and cognitive decline.
Resistance training (also called muscle-strengthening activity) refers to exercises that improve muscular strength by working against resistance such as weights, bands, or body weight.Resistance training reduces chronic inflammation, improves metabolic health, and lowers the risk of major diseases—even at just 30–60 minutes per week.
What does the latest research (2022–2025) say about resistance training?
Reduces all-cause mortality by ~10–17%
Lowers risk of heart disease, cancer, and type 2 diabetes
Decreases chronic inflammation (CRP, IL-6, TNF-α)
Improves muscle mass, metabolic health, and brain function
Effective with just 30–60 minutes per week
How Resistance Training Works
Reduces inflammation → lowers disease risk
Increases muscle mass → improves glucose metabolism
Boosts BDNF → enhances brain function
Improves insulin sensitivity → prevents diabetes
Enhances mitochondrial function → supports energy metabolism
Who Should Prioritize Resistance Training?
Adults over 60 (prevent sarcopenia and falls)
People with diabetes or insulin resistance
Individuals with cardiovascular risk
Cancer patients (under supervision)
Sedentary individuals
Limitations of Current Evidence
Observational data cannot prove causality
Response varies by age, intensity, and adherence
Injury risk if unsupervised
Requires long-term consistency
Clinician’s Perspective (Evidence-Based, Practical Takeaways)
Resistance training should be viewed as a core therapeutic intervention, not an adjunct, in preventing and managing non-communicable diseases (CVD, type 2 diabetes, cancer, depression).
Current evidence (2022–2025) supports a minimum effective dose of 30–60 minutes/week, making it highly feasible even for time-constrained patients.
Mechanistically, benefits are mediated through reduction in chronic systemic inflammation (↓ CRP, IL-6, TNF-α), improved insulin sensitivity, and increased lean muscle mass.
In older adults, resistance training is critical for preventing sarcopenia, improving functional capacity, and reducing fall and fracture risk—often more impactful than aerobic exercise alone.
Emerging oncology data suggest resistance training may act as an adjunct therapy, improving inflammatory profiles and potentially influencing treatment outcomes.
Neurocognitive benefits (via BDNF upregulation and reduced neuroinflammation) position resistance training as a promising strategy in cognitive decline and dementia prevention.
Exercise prescriptions should follow individualized, progressive overload principles, similar to pharmacologic titration.
Key barriers include poor adherence, lack of supervision, and fear of injury—these must be proactively addressed.
For patients with chronic disease, referral to physiotherapy or exercise physiology is recommended to ensure safety and efficacy.
Clinicians should routinely incorporate resistance training into lifestyle prescriptions, alongside diet, sleep, and pharmacotherapy.
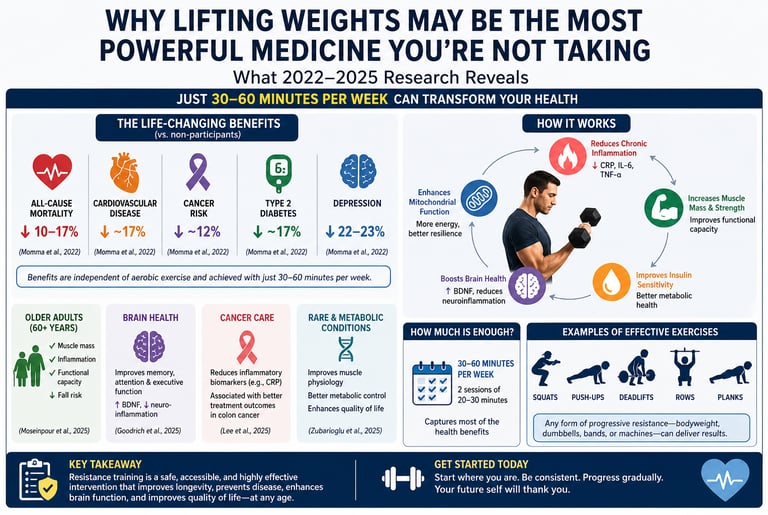
Resistance training—also referred to as muscle-strengthening activity (MSA)—has emerged as a cornerstone intervention in the prevention and management of major non-communicable diseases. A large systematic review and meta-analysis of cohort studies demonstrated that regular participation in resistance training is associated with a 10–17% reduction in all-cause mortality, alongside significant reductions in cardiovascular disease (~17%), cancer (~12%), type 2 diabetes (~17%), and depression (~22–23%) (Momma et al., 2022). Importantly, these benefits are independent of aerobic exercise, underscoring resistance training as a distinct and essential modality.
Mechanistically, resistance training exerts systemic effects by reducing chronic low-grade inflammation, a key driver of cardiometabolic and neurodegenerative diseases. A 2025 meta–meta-analysis confirmed consistent reductions in inflammatory biomarkers such as C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) across diverse populations (Magni et al., 2025). These anti-inflammatory effects are complemented by improvements in insulin sensitivity, body composition, and mitochondrial function, collectively contributing to metabolic resilience.
In older adults, resistance training is particularly impactful. Randomized controlled trial data show significant improvements in muscle mass, functional capacity, and inflammatory profiles, addressing sarcopenia and reducing frailty risk (Hoseinpour et al., 2025). Beyond physical health, resistance training also influences brain function, with evidence linking it to reduced neuroinflammation and increased brain-derived neurotrophic factor (BDNF), a key mediator of neuroplasticity and cognitive performance (Goodrich et al., 2025).
Emerging evidence extends these benefits into clinical populations. In oncology, resistance training has been associated with reduced inflammatory burden and improved treatment outcomes in patients with colon cancer (Lee et al., 2025). Similarly, individualized programs have shown safety and efficacy even in rare metabolic myopathies (Zubarioglu et al., 2025).
Collectively, the evidence supports resistance training as a low-cost, scalable, and high-impact intervention, with meaningful health benefits achievable at just 30–60 minutes per week.
1. The Big Picture: Strength Training and Non-Communicable Diseases
The conversation about physical activity and health has long been dominated by aerobic exercise — running, cycling, swimming. But in 2022, a landmark systematic review and meta-analysis shifted that conversation decisively.
Momma, H., Kawakami, R., Honda, T., & Sawada, S. S. (2022) pooled data from prospective cohort studies worldwide to examine how muscle-strengthening activities (MSA) — including resistance training, weightlifting, bodyweight exercises, and yoga — relate to the incidence and mortality of major non-communicable diseases (NCDs). Published in the British Journal of Sports Medicine, their findings were striking:
All-cause mortality was approximately 10–17% lower among people who regularly performed MSA.
Cardiovascular disease (CVD) incidence was ~17% lower.
Total cancer incidence was ~12% lower.
Type 2 diabetes risk dropped by approximately 17%.
Depression risk fell by an impressive 22–23%.
Crucially, these associations held independently of aerobic exercise. In other words, strength training conferred protective benefits above and beyond what running or cycling already provide. This is not an argument against aerobic exercise — it is an argument for both.
Perhaps the most reassuring finding for time-pressed individuals: most of the risk reduction was captured at just 30–60 minutes of MSA per week — less than 10 minutes a day. Beyond ~60 minutes/week, additional benefits plateaued, suggesting that the barrier to entry is far lower than many assume.
You do not need to spend hours in a gym. Two 20–30 minute strength sessions per week may substantially lower your lifetime risk of heart disease, cancer, diabetes, and depression.
2. Cooling the Fire: How Resistance Training Fights Chronic Inflammation
To understand why strength training protects against so many diseases, we need to talk about chronic systemic inflammation — a low-grade, persistent immune activation that underlies the vast majority of non-communicable diseases, from atherosclerosis and type 2 diabetes to Alzheimer's disease and certain cancers.
Two major 2025 publications directly address the anti-inflammatory power of exercise.
2a. A Meta-Meta-Analysis on Exercise and Inflammation
Magni, O., Arnaoutis, G., & Panagiotakos, D. (2025) conducted what may be the most comprehensive analysis to date: a systematic review of systematic reviews and meta-analyses (a so-called "meta-meta-analysis") on how exercise affects chronic systemic inflammation. Published in Sport Sciences for Health, this study synthesized a vast body of literature to arrive at robust, high-confidence conclusions.
Key findings included significant reductions in canonical pro-inflammatory markers — including C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α) — across multiple exercise modalities. Resistance training, in particular, was identified as a consistently effective strategy for reducing these markers. The breadth of the study's design — pooling findings across dozens of prior meta-analyses — gives these conclusions unusually strong statistical power and generalizability.
This is important clinically: elevated CRP and IL-6 are not abstract laboratory values. They are predictors of heart attack risk, cognitive decline, metabolic dysfunction, and all-cause mortality. Reducing them through exercise is equivalent to reducing disease risk at its root.
Strength training works partly like a natural anti-inflammatory drug — without the side effects of pharmaceuticals.
2b. Resistance Training, Inflammation, and the Cancer Connection
Lee, S., Ma, C., Caan, B. J., et al. (2025) investigated inflammatory biomarkers in a particularly high-stakes population: colon cancer patients undergoing treatment. Published in Cancer, this study found that resistance training not only reduced inflammatory markers in these patients but was also associated with improved treatment outcomes.
Specifically, the study demonstrated that inflammatory biomarkers — including CRP — decreased meaningfully among patients who engaged in resistance training, and these reductions were correlated with better clinical responses. This positions strength training not merely as disease prevention, but as a potential adjunct to cancer treatment — a genuinely remarkable paradigm shift.
Patient-friendly takeaway: If you or someone you love is navigating cancer treatment, ask your oncology team about supervised resistance training. The evidence is growing that it can help, not just with quality of life, but with treatment response.
3. Older Adults Are Not an Exception — They Are the Priority
One of the most persistent myths about resistance training is that it is primarily for young, athletic populations. The 2025 literature destroys this myth emphatically.
Hoseinpour, A. N., et al. (2025) conducted a randomized controlled trial (RCT) — the gold standard of clinical research — specifically examining the effects of resistance training on healthy adults aged 60 years and over. Published in Archives of Gerontology and Geriatrics, the study assessed three pivotal outcome domains:
Inflammatory Biomarkers
Consistent with the broader literature, participants in the resistance training group showed significant reductions in circulating inflammatory markers. For older adults, who carry a disproportionately high burden of chronic low-grade inflammation (sometimes called "inflammaging"), this finding has particular clinical significance.
Body Composition
Resistance training produced meaningful improvements in lean muscle mass and reductions in body fat percentage — even in adults over 60. This matters enormously because sarcopenia (age-related muscle loss) is a primary driver of frailty, falls, metabolic dysfunction, insulin resistance, and loss of independence. Countering sarcopenia is not cosmetic — it is survival.
Functional Capacity
Perhaps most practically, participants demonstrated improved functional capacity: strength, balance, endurance, and the ability to perform activities of daily living. For this age group, functional capacity is the currency of independence.
If you are over 60, resistance training is not just safe — it is arguably the single most important physical activity you can do to preserve your independence, metabolic health, and quality of life.
4. Brain Gains: The Cognitive Connection
The body-brain connection in resistance training is one of the most exciting frontiers in exercise science — and a 2025 review brings it into sharp focus.
Goodrich, J., Tartar, J. L., Banks, J., Leon, F., & Antonio, J. (2025) published a comprehensive review in the Journal of the International Society of Sports Nutrition examining resistance training as a modulator of both inflammation and cognition. This dual framing is conceptually significant: it posits that inflammation is not just a cardiovascular or metabolic concern, but a neurological one — and that resistance training addresses both simultaneously.
Key mechanisms identified in the review include:
Reduction of neuroinflammation: Elevated peripheral inflammatory markers (CRP, IL-6, TNF-α) cross the blood-brain barrier and contribute to neurodegeneration and cognitive decline. Resistance training's anti-inflammatory effects therefore have direct neuroprotective implications.
Upregulation of BDNF: Brain-derived neurotrophic factor — sometimes called "Miracle-Gro for the brain" — promotes neuronal growth, synaptic plasticity, and memory consolidation. Resistance training has been shown to elevate BDNF levels.
Improved executive function: Studies reviewed showed improvements in working memory, processing speed, and attention — domains particularly relevant to aging populations and those at risk for dementia.
This is not a trivial finding. As populations age globally, dementia and cognitive decline represent one of the greatest public health crises of the 21st century. Resistance training, as a low-cost, accessible, and side-effect-free intervention, deserves a central role in cognitive health strategies.
Lifting weights is brain training as much as body training. Protecting your muscles may simultaneously protect your memory.
5. Beyond the Gym: Strength Training in Clinical Settings
Perhaps the most specialized application of resistance training in the 2025 literature comes from a study that examined its effects in patients with metabolic myopathies — a group of rare, inherited disorders affecting muscle energy metabolism.
Zubarioglu, T., Yakal, S., Yegin, F., et al. (2025), publishing in Scientific Reports, demonstrated that individualized and supervised strength training produced meaningful improvements across three domains in these patients:
Muscle physiology: Structural and functional improvements in muscle performance despite the presence of underlying metabolic dysfunction.
Metabolic control: Improved markers of metabolic regulation, suggesting that the benefits of resistance training extend even into pathological states of metabolic impairment.
Quality of life: Patient-reported outcomes showed significant improvements, underscoring that clinical benefit and lived experience are aligned.
What makes this study particularly noteworthy is its population. Metabolic myopathies are conditions where exercise has historically been approached with extreme caution, given concerns about exacerbating muscle damage. That individualized, supervised resistance training not only proved safe but clinically beneficial in this population broadens the scope of who can benefit from strength training — and reinforces the importance of individualization and supervision in clinical exercise prescription.
Even in rare, complex muscle disorders, carefully supervised resistance training can improve function and quality of life. Always work with a qualified professional, but know that "I have a condition" is rarely a reason to avoid movement entirely.
6. Practical Applications: How to Start, Progress, and Sustain
The science is clear. But science alone does not get people to the gym. Here is how to translate the evidence into action — starting from wherever you are right now.
For Beginners (0–3 months)
Frequency: 2 sessions per week (this alone captures most of the mortality-risk reduction per Momma et al., 2022).
Modality: Bodyweight exercises are fully sufficient to start. Squats, push-ups, lunges, glute bridges, and planks require no equipment.
Duration: 20–30 minutes per session.
Progression: Add one repetition or one set per week. Progression, not perfection, is the goal.
Key principle: Consistency over intensity. Showing up irregularly at high intensity is far less effective — and more injurious — than regular moderate sessions.
For Intermediate Practitioners (3–12 months)
Frequency: 2–3 sessions per week.
Modality: Introduce resistance — dumbbells, resistance bands, kettlebells, or machines.
Key compound movements: Squat, hip hinge (deadlift pattern), push (overhead press or bench), pull (rows, lat pulldowns), and carry. These movements recruit the most muscle mass and generate the greatest metabolic and inflammatory benefit.
Tracking: Log your weights and reps. What gets measured gets improved.
For Older Adults (60+)
Priority movements: Lower body strength (squat, step-up, leg press) and balance training to prevent falls.
Starting intensity: Begin with lighter loads and higher repetitions (12–15 reps) to build movement competency safely.
Supervision: Consider working with a certified personal trainer or exercise physiologist, particularly in the early months. As Hoseinpour et al. (2025) demonstrated, supervised training yields robust and measurable results even in this age group.
Rest and recovery: Allow 48 hours between sessions working the same muscle groups. Older adults require, and respond well to, adequate recovery time.
For Individuals With Chronic Conditions
Always consult your healthcare provider before beginning a resistance training program if you have cardiovascular disease, diabetes, osteoporosis, or a metabolic condition.
Evidence from Lee et al. (2025) and Zubarioglu et al. (2025) supports the use of supervised resistance training even in clinical populations — but individualization is essential.
Exercise physiologists and physiotherapists are trained specifically to design safe, effective programs for complex health situations.
Weekly Resistance Training & Activity Template
Monday: Full-Body Resistance Training (30 min)
Focus on compound movements that engage multiple muscle groups (e.g., squats, push-ups, or rows).
This session kicks off the week by stimulating metabolic and anti-inflammatory pathways.
Tuesday: Light Walk or Active Recovery
Engage in low-intensity movement to promote blood flow and muscle repair without adding significant physical stress.
Wednesday: Full-Body Resistance Training (30 min)
Repeat the resistance protocol to meet the evidence-based "60-minute weekly threshold" for maximum longevity benefits.
Thursday: Rest or Yoga/Stretching
Prioritize mobility and flexibility. This helps maintain the joint range of motion necessary for safe lifting.
Friday: Optional Activity (Resistance or Aerobic)
A "flex" day. You can perform a third strength session or opt for moderate-intensity cardio (cycling, jogging) to boost cardiovascular efficiency VO2max).
Saturday: Active Recreation
Engage in enjoyable, functional movement outdoors, such as hiking, swimming, or cycling. This translates gym strength into real-world endurance.
Sunday: Rest
Full recovery day to allow the central nervous system and muscle tissues to fully adapt to the week's stimulus.
Frequently Asked Questions (FAQs)
❓ FAQ 1: How much resistance training do I actually need each week?
According to the meta-analysis by Momma et al. (2022), just 30–60 minutes of muscle-strengthening activity per week is associated with substantial reductions in risk of cardiovascular disease, diabetes, depression, and all-cause mortality. This translates to two sessions of approximately 20–30 minutes each. The WHO recommends at least two sessions per week, and the evidence strongly supports this threshold as clinically meaningful.
❓ FAQ 2: Can resistance training actually reduce inflammation in my body?
Yes — and the evidence is now very strong. The meta-meta-analysis by Magni et al. (2025) demonstrated consistent reductions in key inflammatory biomarkers (CRP, IL-6, TNF-α) through exercise, including resistance training. The RCT by Hoseinpour et al. (2025) confirmed these effects specifically in adults over 60. Chronic inflammation is a root driver of most major diseases, and resistance training addresses it directly.
❓ FAQ 3: Is resistance training safe for older adults, even those with health conditions?
The evidence overwhelmingly says yes — with appropriate individualization and, where needed, supervision. Hoseinpour et al. (2025) demonstrated significant benefits in healthy adults over 60, and Zubarioglu et al. (2025) found meaningful improvements even in patients with rare metabolic muscle disorders. That said, if you have a diagnosed condition, always get clearance from your physician and consider working with a qualified exercise professional.
❓ FAQ 4: Does resistance training help with brain health and memory?
Yes, and the mechanisms are increasingly well understood. Goodrich et al. (2025) reviewed evidence showing that resistance training reduces neuroinflammation, elevates BDNF (a key molecule for brain plasticity and memory), and improves executive function. For aging populations at risk of cognitive decline or dementia, this represents a compelling, low-risk intervention.
❓ FAQ 5: Can resistance training help cancer patients during treatment?
Emerging evidence says yes. Lee et al. (2025) found that resistance training reduced inflammatory biomarkers in colon cancer patients and was associated with improved treatment outcomes. This is an active and rapidly evolving research area. If you or a loved one is undergoing cancer treatment, speak with your oncology team about whether a supervised exercise program — including resistance training — is appropriate for your specific situation.
❓ FAQ 6: I have no gym access. Can I still get the benefits of resistance training?
Absolutely. The studies reviewed in this post do not require gym membership. Bodyweight exercises — push-ups, squats, lunges, planks, glute bridges, pull-ups (if a bar is available) — provide sufficient mechanical loading to stimulate the muscle, metabolic, and anti-inflammatory adaptations documented in the literature. Resistance bands are an inexpensive and highly versatile alternative. What matters is the application of progressive resistance, not the equipment used to achieve it.
❓ FAQ 7: Is resistance training better than cardio, or should I do both?
Both. Momma et al. (2022) specifically found that the protective effects of muscle-strengthening activities were independent of aerobic exercise — meaning each provides unique benefits. The evidence supports a combined approach: aerobic activity for cardiovascular efficiency, stroke volume, and VO2 max; resistance training for muscle mass, metabolic health, bone density, inflammatory control, and functional independence. You do not have to choose.
Clinical pearls
1. Muscle as an Endocrine Organ
Scientific Perspective: Skeletal muscle is a secretory organ that produces and releases "myokines" (e.g., IL-6, irisid) in response to contraction. These signaling molecules exert autocrine, paracrine, and endocrine effects, directly modulating systemic inflammation and glucose metabolism.
Patient-Friendly Perspective: Think of your muscles as a natural pharmacy. Every time you lift weights, your muscles release "chemical messengers" into your bloodstream that travel to your brain, heart, and liver to help them heal and function better.
2. The "30-60 Minute" Mortality Threshold
Scientific Perspective: Meta-analyses show a non-linear dose-response relationship between muscle-strengthening activities (MSA) and all-cause mortality. The maximum risk reduction (10–20%) is achieved at approximately 30–60 minutes per week, after which the mortality benefit plateaus.
Patient-Friendly Perspective: You don't have to live in the gym to live longer. Just one hour of total strength training per week—broken into two short 30-minute sessions—provides nearly all the life-extending benefits of lifting.
3. "Inflammaging" and Sarcopenic Reversal
Scientific Perspective: Resistance training mitigates "inflammaging"—the age-related increase in pro-inflammatory cytokines (CRP, TNF-α). By increasing lean body mass, resistance training reverses sarcopenia, which is a primary driver of metabolic dysfunction in older populations.
Patient-Friendly Perspective: Getting weaker as you age isn't just about your muscles; it’s about "internal rust" (inflammation). Lifting weights acts like an anti-rust treatment, keeping your body’s internal environment clean and your metabolism young.
4. The Neuroprotective "BDNF" Boost
Scientific Perspective: Resistance training is a potent stimulator of Brain-Derived Neurotrophic Factor (BDNF). This protein supports neurogenesis and synaptic plasticity, particularly in the hippocampus, serving as a primary defense against age-related cognitive decline and neurodegenerative disease.
Patient-Friendly Perspective: Lifting weights is a brain workout. It triggers the release of a "brain fertilizer" called BDNF that helps your brain grow new connections, protecting your memory and sharpening your focus as you get older.
5. Independent vs. Synergistic Benefits
Scientific Perspective: The health benefits of resistance training are independent of aerobic physical activity. While cardio improves $VO_{2}$ max and cardiovascular stroke volume, resistance training uniquely improves insulin sensitivity via GLUT4 translocation and bone mineral density through mechanical loading.
Patient-Friendly Perspective: Cardio and strength training are like vitamins and minerals—you need both for a complete "health diet." Running is great for your heart and lungs, but only lifting can build the bone strength and muscle "engines" required to prevent diabetes and frailty.
Author’s Note
This article was written with a clear purpose: to bridge the persistent gap between exercise science and everyday clinical practice. While resistance training has long been associated with athletic performance, the emerging body of evidence from 2022–2025 firmly establishes it as a systemic, disease-modifying intervention with relevance across cardiology, endocrinology, oncology, geriatrics, and neurology.
As a clinician, I have observed that many patients—and even healthcare providers—continue to underestimate the role of muscle health in long-term outcomes. Yet skeletal muscle is not merely a structural tissue; it is a dynamic endocrine organ, influencing inflammation, glucose metabolism, and even brain function. The studies synthesized here reinforce a critical shift in perspective: strength is not just functional—it is metabolic, immunological, and neuroprotective.
Importantly, this article does not advocate replacing pharmacotherapy or established treatments. Instead, it positions resistance training as a foundational therapy—one that works synergistically with medical care to improve outcomes and quality of life. The intention is not to oversimplify complex conditions, but to highlight an intervention that is accessible, scalable, and supported by high-quality evidence.
For clinicians, the challenge moving forward is not whether to recommend resistance training, but how to prescribe it effectively, individualize it for diverse patient populations, and improve long-term adherence.
For patients, the message is equally clear: meaningful health benefits do not require extreme effort—just consistent, structured movement applied over time.
If this article shifts even a small part of the conversation from “exercise as optional” to “exercise as essential medicine,” it has served its purpose.
Disclaimer: This blog post is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before beginning a new exercise program, particularly if you have a pre-existing health condition.
.Related Articles
Just 2 Strength Workouts a Week Can Transform Your Metabolism—Here’s How
The Science of Healthy Brain Aging: Microglia, Metabolism & Cognitive Fitness | DR T S DIDWAL
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
References
Goodrich, J., Tartar, J. L., Banks, J., Leon, F., & Antonio, J. (2025). Resistance training as a modulator of inflammation and cognition. Journal of the International Society of Sports Nutrition, 22(sup2). https://doi.org/10.1080/15502783.2025.2550143
Hoseinpour, A. N., et al. (2025). The influence of resistance training on inflammatory biomarkers, body composition, and functional capacity in healthy adults aged 60 years and over: A randomized controlled trial. Archives of Gerontology and Geriatrics. Advance online publication. https://doi.org/10.1016/j.archger.2024.106060
Lee, S., Ma, C., Caan, B. J., et al. (2025). Impact of resistance training on inflammatory biomarkers and associations with treatment outcomes in colon cancer. Cancer, e35865. https://doi.org/10.1002/cncr.35865
Magni, O., Arnaoutis, G., & Panagiotakos, D. (2025). The impact of exercise on chronic systemic inflammation: A systematic review and meta–meta-analysis. Sport Sciences for Health, 21, 1405–1417. https://doi.org/10.1007/s11332-025-01445-3
Momma, H., Kawakami, R., Honda, T., & Sawada, S. S. (2022). Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: A systematic review and meta-analysis of cohort studies. British Journal of Sports Medicine, 56(13), 755–763. https://doi.org/10.1136/bjsports-2021-105061
Zubarioglu, T., Yakal, S., Yegin, F., et al. (2025). Impact of individualized and supervised strength training on muscle physiology, metabolic control and quality of life in metabolic myopathies. Scientific Reports, 15, 26125. https://doi.org/10.1038/s41598-025-11361-8